A Rapid Public Health Needs Assessment Framework for after Major Earthquakes Using High-Resolution Satellite Imagery

 ,
,  ,
,
Abstract
:1. Introduction
2. Framework of Rapid Public Health Needs Assessment
3. Materials and Methods
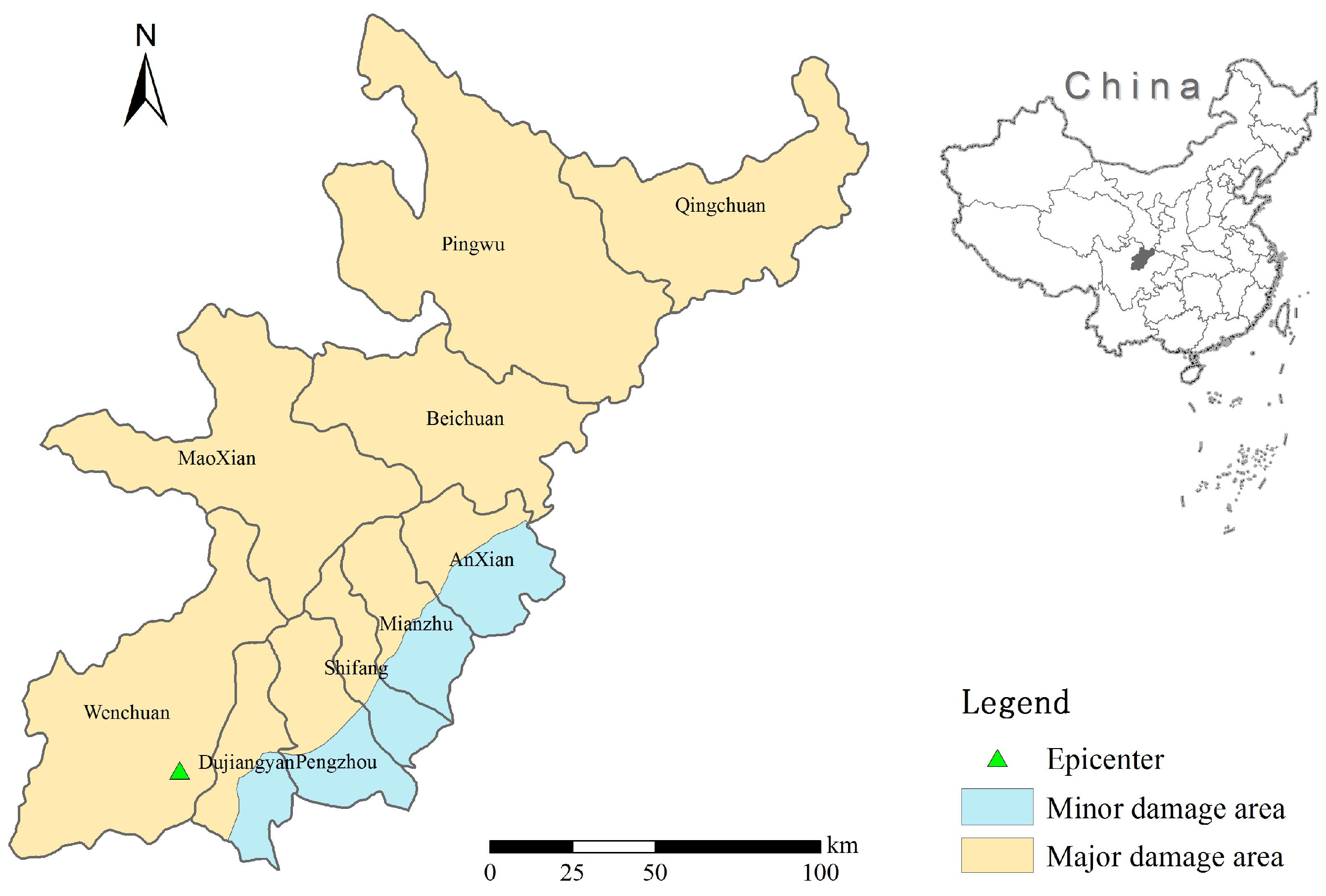
3.1. Study Area
3.2. Data Collection and Processing
3.2.1. Satellite Data
3.2.2. Infectious Disease Incidence Data
3.2.3. Population Data
3.2.4. Geographic Information Data
3.3. Estimating Earthquake Casualties and Injures
- (1)
- Type A are a multi-storey reinforced concrete houses that have steel and reinforced concrete structures, such as high-rise steel and reinforced concrete frame shear wall structures, reinforced concrete shear wall structures, high-rise and multi-storey reinforced concrete frame structures, etc. This kind of structure has the best seismic performance of all structures;
- (2)
- Type B are multi-storey masonry buildings. They include brick structures, industrial buildings, public buildings, etc. This kind of structure is the most abundant in cities and their seismic performance is inferior to that of A class buildings.
- (3)
- Type C are single homes; these structures mainly include the lime mortar masonry brick buildings, the 24 cm thick brick structures of empty houses and classrooms, hollow brick wall structures, etc.
- (4)
- Type D are buildings with adobe, earth-rock structure. These includes the raw soil structures often found in the countryside, such as adobe, adobe caves, rock structures. The seismic performance of these is the worst type of all types of structure.
3.4. Rapid Medical Resource Damage Assessment
3.5. Public Health Needs Assessment After an Earthquake
3.5.1. Water Supply Assessment
3.5.2. Risk Assessment of Infectious Disease
3.5.3. Settlement Selection after an Earthquake
- (1)
- It should be within 50–500 m of the damaged residential areas to facilitate the transport of the wounded;
- (2)
- In order to ensure the smooth access of medical supplies and relief workers to the rescue point, a road traffic area should be selected and be within 200 m of the highway.
- (3)
- To prevent the secondary hazards such as landslides, debris flows, lake threats to personnel, the selected area should be 100 m away from a river system, and any landslide area should be 200 m away from the secondary disaster risk area;
- (4)
- To avoid high slopes, and the vegetation that is rich in mountains, the emergency rescue area that refers to the smallest size square hospital, the emergency rescue point location area shall be no less than 2500 m2.
4. Results
4.1. Earthquake Casualties and Injuries Estimation
4.2. Rapid Medical Resource Damage Assessment
4.3. Public Health Needs Assessment after Earthquake
4.3.1. Water Supply Assessment
4.3.2. Risk Assessment of Infectious Disease
4.3.3. Settlement Selection after an Earthquake
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zhang, L.; Liu, X.; Li, Y.; Liu, Z.; Lin, J.; Shen, J.; Tang, X.; Zhang, Y.; Liang, W. Emergency medical rescue efforts after a major earthquake: Lessons from the 2008 Wenchuan earthquake. Lancet 2012, 379, 853–861. [Google Scholar] [CrossRef]
- Liang, Y. Satisfaction with economic and social rights and quality of life in a post-disaster zone in China: Evidence from earthquake-prone Sichuan. Disaster Med. Public Health Prep. 2015, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Burchfiel, B.C.; Royden, L.H.; Van der Hilst, R.D.; Hager, B.H. A geological and geophysical context for the Wenchuan earthquake of 12 May 2008, Sichuan, People’s Republic of China. GSA Today 2008, 18, 4–11. [Google Scholar] [CrossRef]
- Ni, S.; Wang, W.; Li, L. The April 14th, 2010 Yushu earthquake, a devastating earthquake with foreshocks. Sci. China Earth Sci. 2010, 53, 791–793. [Google Scholar] [CrossRef]
- Tang, B.; Zhang, L. Ya’an earthquake. Lancet 2013, 381, 1984–1985. [Google Scholar] [CrossRef]
- Russo, F.; Rindone, C.; Trecozzi, M.R. The role of training in evacuation. WIT Trans. Inf. Commun. Technol. 2012, 44, 491–502. [Google Scholar]
- Lillibridge, S.; Niji, E.; Burkle, F. Disaster assessment: The emergency health evaluation of a population affected by a disaster. Ann. Emerg. Med. 1993, 22, 1715–1720. [Google Scholar] [CrossRef]
- Ranjbar, H.R.; Ardalan, A.A.; Dehghani, H.; Saradjian, M.R. Using high-resolution satellite imagery to provide a relief priority map after earthquake. Natl. Hazards 2017, 90, 1087–1113. [Google Scholar] [CrossRef]
- Feng, T.; Hong, Z.; Fu, Q.; Tong, X. Application and prospect of a high-resolution remote sensing and geo-information system in estimating earthquake casualties. Natl. Hazards Earth Syst. Sci. 2014, 14, 2165. [Google Scholar] [CrossRef]
- Ranjbar, H.R.; Dehghani, H.; Ardalan, A.R.A.; Saradjian, M.R. A GIS-based approach for earthquake loss estimation based on the immediate extraction of damaged buildings. Geomat. Natl. Hazards Risk 2017, 8, 772–791. [Google Scholar] [CrossRef]
- Kenny, C. Disaster risk reduction in developing countries: Costs, benefits and institutions. Disasters 2012, 36, 559–588. [Google Scholar] [CrossRef] [PubMed]
- Rij, E. An approach to the disaster profile of People’s Republic of China 1980–2013. Emerg. Disaster Rep. 2016, 3, 3–48. [Google Scholar]
- Zhang, Y.; Hao, Y. Hazards and Strategies for Infectious Diseases Prevention and Control after Catastrophic Disaster of Earthquake. J. Sun Yat-Sen Univ. (Med. Sci.) 2008, 29, 375–378. (In Chinese) [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, Y.; Liu, X.; Lin, L.; Liu, Y.; Peng, Z. Disease surveillance and risk evaluation on the transmission of infectious disease in emergent status after earthquake. South China J. Prev. Med. 2008, 34, 9–12. (In Chinese) [Google Scholar] [CrossRef]
- Malilay, J.; Flanders, W.D.; Brogan, D. A modified cluster sampling method for post-disaster rapid assessment of needs. Bull. World Health Organ. 1996, 74, 399–405. [Google Scholar] [PubMed]
- Akbari, M.E.; Farshad, A.A.; Asadi-Lari, M. The devastation of Bam: An overview of health issues 1 month after the earthquake. Public Health 2004, 118, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Ye, F.; Guo, E.; Liu, J. Seismic damage investigation and analysis of water supply system in Lushan earthquake. World Earthq. Eng. 2013, 29, 52–58. (In Chinese) [Google Scholar]
- Watson, J.T.; Michelle, G.; Maire, A.C. Epidemics after natural disasters. Emerg. Infect. Dis. 2007, 13, 1. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Chen, X.; Li, Q.; Chen, J. The temporal hierarchy of shelters: A hierarchical location model for earthquake-shelter planning. Int. J. Geogr. Inf. Sci. 2013, 27, 1612–1630. [Google Scholar] [CrossRef]
- Wagner, R.M.; Jones, N.P.; Smith, G.S. Risk factors for casualty in earthquakes: The application of epidemiologic principles to structural engineering. Struct. Saf. 1994, 13, 177–200. [Google Scholar] [CrossRef]
- Beck, L.R.; Lobitz, B.M.; Wood, B.L. Remote sensing and human health: New sensors and new opportunities. Emerg. Infect. Dis. 2000, 6, 217. [Google Scholar] [CrossRef] [PubMed]
- Hay, S.; Noor, A.; Nelson, A.; Tatem, A. The accuracy of human population maps for public health application. Trop. Med. Int. Health 2005, 10, 1073–1086. [Google Scholar] [CrossRef] [PubMed]
- Aubrecht, C.; Freire, S.; Neuhold, C.; Curtis, A.; Steinnocher, K. Introducing a temporal component in spatial vulnerability analysis. Disaster Adv. 2012, 5, 48–53. [Google Scholar]
- Freire, S.; Aubrecht, C. Integrating population dynamics into mapping human exposure to seismic hazard. Nat. Hazards Earth Syst. Sci. 2012, 12, 3533–3543. [Google Scholar] [CrossRef] [Green Version]
- Taskin, G.; Ersoy, O.K.; Kamasak, M.E. Earthquake-induced damage classification from postearthquake satellite image using spectral and spatial features with support vector selection and adaptation. J. Appl. Remote Sens. 2015, 9, 096017. [Google Scholar] [CrossRef]
- Eguchi, R.T.; Mansouri, B. Use of remote sensing technologies for building damage assessment after the 2003 Bam, Iran, earthquake—Preface to remote sensing papers. Earthq. Spectra 2005, 21, 207–212. [Google Scholar] [CrossRef]
- Wang, F.; Wang, S.; Zhou, Y.; Wang, L.; Yan, F.; Li, W.; Liu, X. High Resolution Remote Sensing Monitoring and Assessment of Secondary Geological Disasters Triggered by the Lushan Earthquake. Spectrosc. Spectr. Anal. 2016, 36, 181–185. (In Chinese) [Google Scholar] [CrossRef]
- Cao, C.; Chang, C.; Xu, M.; Zhao, J.; Gao, M.; Zhang, H.; Guo, J.; Guo, J.; Dong, L.; He, Q.; et al. Epidemic risk analysis after the Wenchuan Earthquake using remote sensing. Int. J. Remote Sens. 2010, 31, 3631–3642. [Google Scholar] [CrossRef]
- Feng, T.; Hong, Z.; Wu, H.; Fu, Q.; Wang, C.; Jiang, C.; Tong, X. Estimation of earthquake casualties using high-resolution remote sensing: A case study of Dujiangyan city in the May 2008 Wenchuan earthquake. Natl. Hazards 2013, 69, 1577–1595. [Google Scholar] [CrossRef]
- Huang, T.; Zhao, T.; Qu, J.; Wang, S.; Huang, M.; Wang, S. The advantages of space information technology in serving Wenchuan earthquake relief decisions. Remote Sens. Technol. Appl. 2008, 23, 486–492. (In Chinese) [Google Scholar]
- Hu, S.Q. Research into “Information Lonely Island” in natural disasters with 5.12 Wenchuan earthquake as an example. J. Nanchang Coll. 2008, 5, 163–165. (In Chinese) [Google Scholar]
- Brown, D.; Saito, K.; Liu, M.; Spence, R.; So, E.; Ramage, M. The use of remotely sensed data and ground survey tools to assess damage and monitor early recovery following the 12.5. 2008 Wenchuan earthquake in China. Bull. Earthq. Eng. 2012, 10, 741–764. [Google Scholar] [CrossRef]
- Zhang, L.L.; Liu, Y.; Liu, X.; Zhang, Y. Rescue efforts management and characteristics of casualties of the Wenchuan earthquake in China. Emerg. Med. J. 2011, 28, 618–622. [Google Scholar] [CrossRef] [PubMed]
- Zhong, B.; Chen, L.; Liu, Y.; Wu, Z.S.; Zhu, H.Q.; Lu, D.; Xu, L.; Zhang, Y.; Wang, C.F.; Xie, M.K.; et al. Risk assessment of schistosomiasis transmission in earthquake-stricken areas after the Lushan Earthquake in Sichuan Province on April 20, 2013. Chin. J. Schistosomiasis Control 2013, 25, 226–231. (In Chinese) [Google Scholar]
- Yang, X.; Jiang, D.; Wang, N.; Liu, H. Method of pixelizing population data. J. Geogr. Sci. 2002, 57, 70–75. [Google Scholar]
- Rabus, B.; Eineder, M.; Roth, A.; Bamler, R. The shuttle radar topography mission—A new class of digital elevation models acquired by spaceborne radar. ISPRS J. Photogram. Remote Sens. 2003, 57, 241–262. [Google Scholar] [CrossRef]
- Wei, B.; Nie, G.; Su, G.; Sun, L.; Bai, X.; Qi, W. Risk assessment of people trapped in earthquake based on km grid: A case study of the 2014 Ludian earthquake, China. Geomat. Natl. Hazards Risk 2017, 8, 1289–1305. [Google Scholar] [CrossRef]
- Jaiswal, K.; Wald, D.; Earle, P.; Porter, K.A.; Hearne, M. Earthquake casualty models within the USGS Prompt Assessment of Global Earthquakes for Response (PAGER) system. In Human Casualties in Earthquakes; Springer: Dordrecht, The Netherlands, 2011; pp. 83–94. [Google Scholar]
- Yin, Z. Earthquake Hazard and Loss Prediction; Seismological Press: Beijing, China, 1995. (In Chinese) [Google Scholar]
- Ma, Y.; Xie, L. Methodologies for assessment of earthquake casualty. Earthq. Eng. Eng. Vib. 2000, 20, 140–147. (In Chinese) [Google Scholar]
- Fan, S.; Hu, Y.; Liu, Z. Research of information extraction of city building based on a new object-oriented method. J. South China Norm. Univ. 2015, 47, 91–97. (In Chinese) [Google Scholar]
- Greaney, P.; Pfiffner, S.; David, W.D. Humanitarian Charter and Minimum Standards in Humanitarian Response; The Sphere Project: Southampton, UK, 2011. [Google Scholar]
- Zhang, B.; Wang, F.; Zhao, Y.; Geng, H. A probe into the transitional allocation plan after the earthquake: A case study on the allocation plan of Daguan town. New Archit. 2008, 6, 69–71. (In Chinese) [Google Scholar] [CrossRef]
- Song, X. Selections of locations, environmental protections and fire research for settlements of victims in the Wenchuan earthquake. Fire Sci. Technol. 2009, 28, 505–507. (In Chinese) [Google Scholar] [CrossRef]
- Chinese Center for Disease Control and Prevention. Preliminary Risk Assessment of Major Infectious Diseases in Disaster Area after Sichuan Earthquake. 2008. Available online: http://www.chinacdc.cn/n272442/n272530/n273736/n342415/n3866878/n3867602/appendix/Preliminary%20Report%20on%20Communicable%20Diseases%20Risk%20Assessment%20and%20Interventions%20after%20Sichuan%20Earthquake_China%20CDC.doc (accessed on 17 December 2017).
- Kouadio, I.K.; Aljunid, S.; Kamigaki, T.; Hammad, K.; Oshitani, H. Infectious diseases following natural disasters: Prevention and control measures. Expert Rev. Anti-Infect. Ther. 2012, 10, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Petal, M. Earthquake casualties research and public education. In Human Casualties in Earthquakes; Springer: Dordrecht, The Netherlands, 2011; pp. 25–50. [Google Scholar]
- Chen, Z.; Nie, Z.; Ma, X.; Wang, J.; Chen, Z.; Liu, C.; Zhong, Y.; Sun, Y.; Zhang, H.; Li, J. Water quality monitoring and safety evaluation of Yingxiu town, the epicenter of the “5.12” Wenchuan earthquake. Bull. Acad. Mil. Med. Sci. 2008, 32, 367–369. (In Chinese) [Google Scholar]
- Lemonick, D.M. Epidemics after natural disasters. Am. J. Clin. Med. 2011, 8, 144–152. [Google Scholar]
- World Health Organization. Acute water diarrhea outbreak. In Weekly Morbidity and Mortality Report; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- World Health Organization. Acute jaundice syndrome. In Weekly Morbidity and Mortality Report; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Schneider, E.; Hajjeh, R.A.; Spiegel, R.A.; Jibson, R.W.; Harp, E.L.; Marshall, G.A.; Gunn, R.A.; McNeil, M.M.; Pinner, R.W.; Baron, R.C.; et al. A coccidiomycosis outbreak following the Northridge, Calif, earthquake. JAMA 1997, 277, 904–908. [Google Scholar] [CrossRef] [PubMed]
- Logue, J.N. Disasters, the environment, and public health: Improving our response. Am. J. Public Health 1996, 86, 1207–1210. [Google Scholar] [CrossRef] [PubMed]
- Nathalie, F.; Viel, J.F.; Mauny, F.J.; Hoen, B.; Piarroux, R. Negligible risk for epidemics after geophysical disasters. Emerg. Infect. Dis. 2006, 12, 543. [Google Scholar]
- Ting, L.; Wang, F.; Wen, J.; Ping, Y. Rapid assessment of health needs after disasters: A systematic review. Chin. J. Emerg. Med. 2011, 11, 605–612. (In Chinese) [Google Scholar]
- Jin, Q.; Chen, K.H.; Huang, Y. How to carry out health and disease prevention work in Aba after Wenchuan earthquake. Chin. Evid. Based Med. 2008, 8, 685–691. (In Chinese) [Google Scholar]
- Zhao, L.; Rodriguez-Llanes, J.M.; Wu, Q.; van den Oever, B.; Westman, L.; Albela, M.; Pan, L.; Chen, G.; Zhang, D.; Hughes, M.; et al. Multiple injuries after earthquakes: A retrospective analysis on 1871 injured patients from the 2008 Wenchuan earthquake. Crit. Care 2012, 16, R87. [Google Scholar]
- Peng, H. China’s Health Challenges after the Yushu Earthquake. Prehosp. Disaster Med. 2011, 26, 135–136. [Google Scholar] [CrossRef] [PubMed]
- Liu, T. The significance of emergency preparedness highlighted by Yushu earthquake once again. J. Saf. Sci. Technol. 2010, 2, 5–7. [Google Scholar]
- Ye, S.; Zhai, G.; Hu, J. Damages and Lessons from the Wenchuan Earthquake in China. Hum. Ecol. Risk Assess. Int. J. 2011, 17, 598–612. [Google Scholar] [CrossRef]
- Teng, A.M.; Blakely, T.; Ivory, V.; Kingham, S.; Cameron, V. Living in areas with different levels of earthquake damage and association with risk of cardiovascular disease: A cohort-linkage study. Lancet Planet. Health 2017, 1, e242–e253. [Google Scholar] [CrossRef]
- Liu, M.; Wang, L.; Shi, Z.; Zhang, Z.; Zhang, K.; Shen, J. Mental health problems among children one-year after Sichuan earthquake in China: A follow-up study. PLoS ONE 2011, 6, e14706. [Google Scholar] [CrossRef] [PubMed]
- Giovanna, C.; Giuseppe, M.; Antonio, P.; Corrado, R.; Francesco, R.; Antonino, V. Transport models and intelligent transportation system to support urban evacuation planning process. IET Intell. Transp. Syst. 2016, 10, 279–286. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The Damage Matrix of Type C Structures (%) | |||||
| MMI | Undamaged | Slight | Middle | Severe | Destroyed |
| VI | 49 | 27.15 | 15.05 | 6.76 | 1.82 |
| VII | 28 | 21.29 | 22.07 | 20.27 | 8.36 |
| VIII | 12 | 16.33 | 23.09 | 30.22 | 18.28 |
| IX | 8 | 10.53 | 17.66 | 26.08 | 37.67 |
| X | 2.2 | 4.81 | 11.91 | 17.21 | 63.84 |
| The Damage Matrix of Type D Structures (%) | |||||
| MMI | Undamaged | Slight | Middle | Severe | Destroyed |
| VI | 32.5 | 26.5 | 22.5 | 16.5 | 2.5 |
| VII | 16.5 | 18.5 | 20 | 26 | 19 |
| VIII | 7 | 12 | 16.5 | 27 | 37.5 |
| IX | 2.5 | 8.5 | 14 | 25 | 50 |
| X | 0 | 1.5 | 7.5 | 17.5 | 73.5 |
| Population Denstiy (Person/km2) | Less than 50 | 50~200 | 200~500 | More than 500 |
|---|---|---|---|---|
| 0.8 | 1.0 | 1.1 | 1.2 |
| MMI | VI | VII | VIII | IX | X |
|---|---|---|---|---|---|
| 17 | 8 | 4 | 2 | 1.5 |
| Principle | Indicator | Calculation |
|---|---|---|
| Nearest principle | Distance to the damaged residential area | Within 50–500 m |
| Safety Principle | Slope | Less than 15° |
| Distance to river | 100 m away | |
| Distance to landslide area | 200 m away | |
| Convenient transportation | Distance to road | Within 200 m |
| Size limitation | Minimum Size | 2500 m2 |
| County | 2008 Population | 2000 Gridded Population | Estimated Casualties | Estimated Injuries | Major Damage Area (Percentage) | Minor Damage Area (Percentage) | Medical Institutions (Number) | Damaged Medical Institutions (Number) | Water Supply Needs (L) |
|---|---|---|---|---|---|---|---|---|---|
| Anxian | 476,072 | 497,308 | 12,275 | 36,825 | 44.2 | 55.8 | 24 | 15 | 5,239,637 |
| Beichuan | 157,341 | 159,098 | 9615 | 28,845 | 100 | 0 | 22 | 22 | 2,386,470 |
| Dujiangyan | 611,430 | 583,556 | 14,285 | 42,855 | 63.8 | 36.2 | 42 | 31 | 7,063,362 |
| Maoxian | 105,909 | 102,098 | 4399 | 13,197 | 100 | 0 | 25 | 25 | 1,531,470 |
| Mianzhu | 501,794 | 511,245 | 13,769 | 41,307 | 54 | 46 | 40 | 27 | 5,787,293 |
| Pengzhou | 754,925 | 773,772 | 9616 | 28,848 | 53.4 | 46.6 | 34 | 23 | 8,721,958 |
| Pingwu | 185,666 | 188,041 | 8557 | 25,671 | 0 | 0 | 27 | 27 | 2,820,615 |
| Qingchuan | 251,417 | 250,284 | 11,682 | 35,046 | 100 | 0 | 39 | 39 | 3,754,260 |
| Shifang | 420,225 | 400,650 | 6151 | 18,453 | 57.8 | 42.2 | 26 | 18 | 4,657,156 |
| Wenchuan | 114,138 | 109,523 | 5797 | 17,391 | 100 | 0 | 15 | 15 | 1,642,845 |
| Total | 3,578,917 | 3,575,575 | 96,146 | 288,438 | 294 | 242 | 43,605,066 |
| Diseases | Risk ☆ | Diseases | Risk ☆ |
|---|---|---|---|
| Bacillary dysentery | ++++ | Visceral Leishmaniasis | ++ |
| Other infectious diarrhea | ++++ | Hemorrhagic fever with renal syndrome | ++ |
| Cholera | +++ | Tetanus | ++ |
| Hepatitis A | +++ | Malaria | +~++ |
| Typhoid and paratyphoid | +++ | Plague | + |
| Tuberculosis | +++ | Hepatitis B | + |
| Acute upper respiratory tract infections | +++ | Japanese Encephalitis | + |
| Rubella | +++ | Leptospirosis | + |
| Mumps | +++ | Dengue | + |
| Acute hemorrhagic conjunctivitis | +++ | Rabies | + |
| Chicken Pox | +++ | Schistosomiasis | + |
| Measles | ++ | Streptococcus suis | + |
| Meningococcal meningitis | ++ | Avian influenza/H5N1 | + |
| Hand-foot-and-mouth disease | ++ | Syphilis/gonorrhea | + |
| Anthrax | ++ | SARS (Severe Acute Respiratory Syndromes) | -~+ |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, J.; Ding, F.; Wang, Z.; Ren, J.; Zhao, J.; Wang, Y.; Tang, X.; Wang, Y.; Yao, J.; Li, Q. A Rapid Public Health Needs Assessment Framework for after Major Earthquakes Using High-Resolution Satellite Imagery. Int. J. Environ. Res. Public Health 2018, 15, 1111. https://doi.org/10.3390/ijerph15061111
Zhao J, Ding F, Wang Z, Ren J, Zhao J, Wang Y, Tang X, Wang Y, Yao J, Li Q. A Rapid Public Health Needs Assessment Framework for after Major Earthquakes Using High-Resolution Satellite Imagery. International Journal of Environmental Research and Public Health. 2018; 15(6):1111. https://doi.org/10.3390/ijerph15061111
Chicago/Turabian StyleZhao, Jian, Fan Ding, Zhe Wang, Jinghuan Ren, Jing Zhao, Yeping Wang, Xuefeng Tang, Yong Wang, Jianyi Yao, and Qun Li. 2018. "A Rapid Public Health Needs Assessment Framework for after Major Earthquakes Using High-Resolution Satellite Imagery" International Journal of Environmental Research and Public Health 15, no. 6: 1111. https://doi.org/10.3390/ijerph15061111
APA StyleZhao, J., Ding, F., Wang, Z., Ren, J., Zhao, J., Wang, Y., Tang, X., Wang, Y., Yao, J., & Li, Q. (2018). A Rapid Public Health Needs Assessment Framework for after Major Earthquakes Using High-Resolution Satellite Imagery. International Journal of Environmental Research and Public Health, 15(6), 1111. https://doi.org/10.3390/ijerph15061111