Trial to Encourage Adoption and Maintenance of a Mediterranean Diet (TEAM-MED): Protocol for a Randomised Feasibility Trial of a Peer Support Intervention for Dietary Behaviour Change in Adults at High Cardiovascular Disease Risk

 , , , ,
, , , ,
Abstract
:1. Introduction
1.1. The Cardioprotective Benefits of a Mediterranean Diet
1.2. Peer Support as a Potential Strategy to Encourage Dietary Behaviour Change
1.3. Development of a Tailored Peer Support Intervention
1.4. Aim
2. Materials and Methods
2.1. TEAM-MED Objectives
- Estimate and compare the variability of Mediterranean Diet Score (MDS) from baseline to 6 months and from 6 months to 12 months between the peer support intervention and other intervention groups
- Estimate and compare the variability of biochemical markers of nutritional status and health markers over the course of the intervention, as for MDS, between the peer support intervention and other intervention groups
- Test recruitment strategies, retention, attrition rates
- Estimate the sample size for a large-scale trial
- Test the validity of the theoretical model underpinning the peer support intervention
- Evaluate the training and support provided to peer supporters to deliver the intervention
- Determine fidelity of implementation and acceptability of the intervention
- Assess outcome data collection processes within the pilot trial, including those to explore mediators and moderators of MD adherence and cost-effectiveness
- Explore reasons for withdrawal for study participants and peer supporters recruited to deliver the peer support intervention
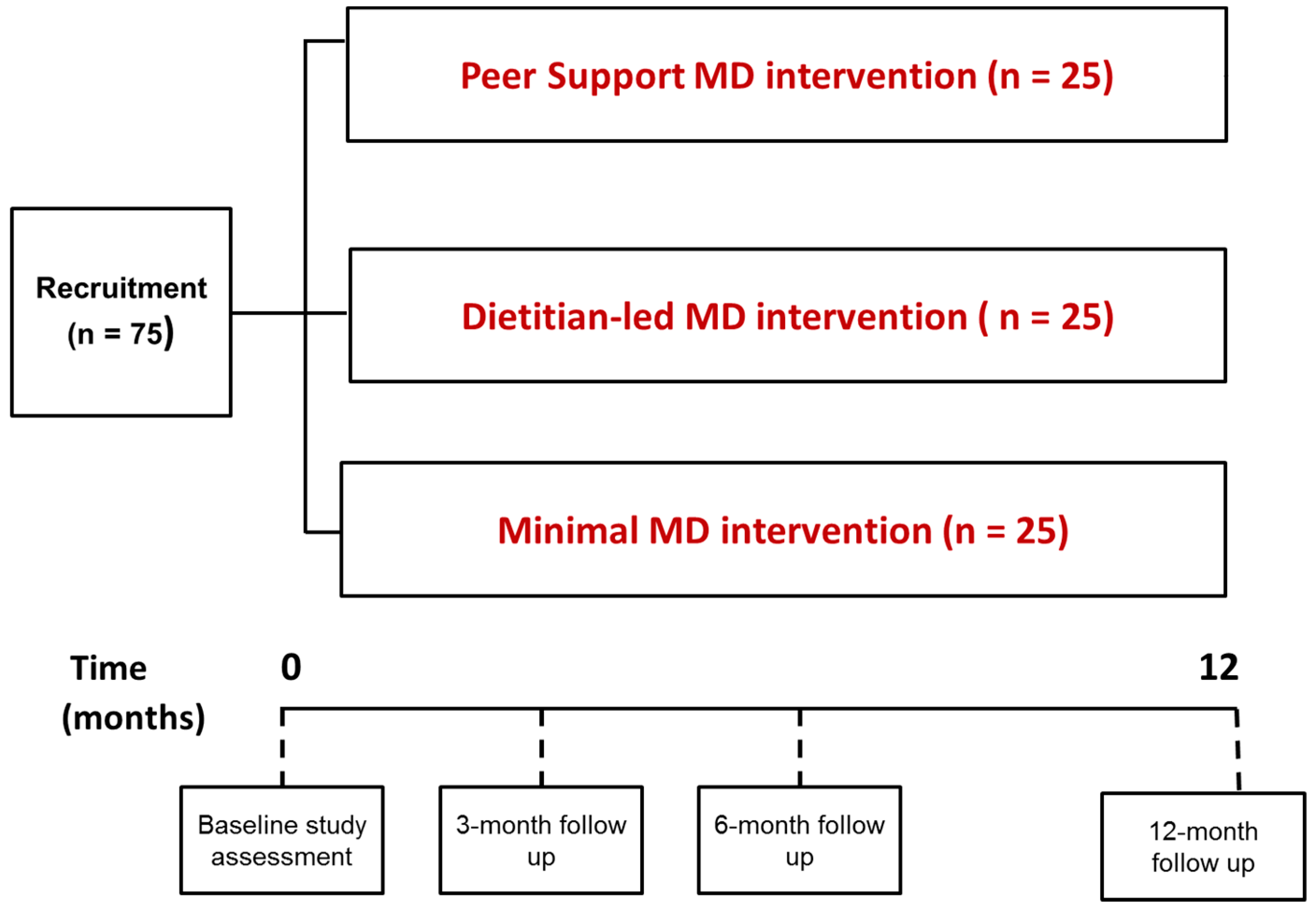
2.2. Design
2.3. Study Participants
2.3.1. Participant Recruitment
2.3.2. Inclusion Criteria
2.3.3. Exclusion Criteria
2.3.4. Peer Supporters
2.3.5. Peer Supporter Training
2.3.6. Peer Supporter Support
2.4. TEAM-MED Intervention Groups
2.4.1. Group 1: Peer Support (n = 25)
2.4.2. Group 2: Dietitian-Led Support (n = 25)
- 50 mL extra virgin olive oil (EVOO) or,
- 30 g nuts (15 g walnuts, 7.5 g almonds and 7.5 g hazelnuts) or,
- Combination of both (25 mL EVOO plus 15 g nuts (8 g walnuts, 3.5 g almonds and 3.5 g hazelnuts))
2.4.3. Group 3: Minimal Support (Control) (n = 25)
3. Results
3.1. Outcomes
3.2. Study Measures
3.2.1. Primary Outcome—MD Behaviour Change
3.2.2. Clinical Measures
3.2.3. Biochemical Measures
3.2.4. Mediators of MD Behaviour Change
3.2.5. Intervention Moderators
3.2.6. Evaluation of Recruitment and Study Attrition Rates
3.3. Power and Sample Size
3.4. Statistical Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Willett, W.C. The Mediterranean diet: Science and practice. Public Health Nutr. 2006, 9, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Mente, A.; de Koning, L.; Shannon, H.S.; Anand, S.S. A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch. Intern. Med. 2009, 169, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Rexrode, K.M.; Mantzoros, C.S.; Manson, J.E.; Willet, W.C.; Hu, F.B. Mediterranean diet and incidence of and mortality from coronary heart disease and stroke in women. Circulation 2009, 119, 1093–1100. [Google Scholar] [CrossRef] [PubMed]
- Knoops, K.T.; de Groot, L.C.; Kromhout, D.; Perrin, A.E.; Moreiras-Varela, O.; Menotti, A.; van Staveren, W.A. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European Men and Women: The HALE project. JAMA 2004, 292, 1433–1439. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; García-López, M.; Bes-Rastrollo, M.; Toledo, E.; Martínez-Lapiscina, E.H.; Delgado-Rodriguez, M.; Vazquez, Z.; Benito, S.; Beunza, J.J. Mediterranean diet and the incidence of cardiovascular disease: A Spanish cohort. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing evidence on benefits of adherence to the Mediterranean diet on health: An updated systematic review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- De Lorgeril, M.; Salen, P.; Martin, J.L.; Monjaud, I.; Delaye, J.; Mamelle, N. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: Final report of the Lyon Diet Heart Study. Circulation 1999, 99, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvado, J.; Covas, M.I.; Corella, D.; Aros, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of Cardiovascular disease with a Mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The effect of Mediterranean diet on metabolic syndrome and its Components: A meta-analysis of 50 studies and 534,906 individuals. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Salas-Salvadó, J.; Estruch, R.; Corella, D.; Fitó, M.; Ros, E. PREDIMED Investigators. Benefits of the Mediterranean Diet: Insights from the PREDIMED Study. Prog. Cardiovasc. Dis. 2015, 58, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvadó, J.; Bulló, M.; Estruch, R.; Ros, E.; Covas, M.I.; Ibarrola-Jurado, N.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; et al. Prevention of diabetes with Mediterranean diets: A subgroup analysis of a randomized trial. Ann. Intern. Med. 2014, 160, 1–10. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed.; U.S. Department of Health and Human Services and U.S. Department of Agriculture: Washington, DC, USA, December 2015. Available online: https://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 17 April 2018).
- Mozaffarian, D. Dietary and Policy Priorities for Cardiovascular Disease, Diabetes, and Obesity: A Comprehensive Review. Circulation 2016, 33, 187–225. [Google Scholar] [CrossRef] [PubMed]
- Logan, K.J.; Woodside, J.V.; Young, I.S.; McKinley, M.C.; Perkins-Porras, L.; McKeown, P.P. Adoption and maintenance of a Mediterranean diet in patients with coronary heart disease from a Northern European population: A pilot randomised trial of different methods of delivering Mediterranean diet advice. J. Hum. Nutr. Diet. 2010, 23, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Toobert, D.J.; Glasgow, R.E.; Strycker, L.A.; Barrera, M., Jr.; Ritzwoller, D.P.; Weidner, G. Long-term effects of the Mediterranean lifestyle Program: A randomized clinical trial for postmenopausal Women with type 2 diabetes. Int. J. Behav. Nutr. Phys. Act. 2007, 17. [Google Scholar] [CrossRef]
- Heisler, M. Overview of Peer Support Models to Improve Diabetes Self-Management and Clinical Outcomes. Diabetes Spectr. 2007, 20, 214–221. [Google Scholar] [CrossRef]
- Dennis, C.L. Peer support within a health care Context: A concept analysis. Int. J. Nurs. Stud. 2003, 40, 321–332. [Google Scholar] [CrossRef]
- Cohen, S.; Gottlieb, B.; Underwood, L. Social relationships and health. In Social Support Measurement and Intervention; Cohen, S., Underwood, L., Gottlieb, B., Eds.; Oxford University Press: New York, NY, USA, 2000; pp. 3–28. [Google Scholar]
- Toobert, D.J.; Stryker, L.A.; Glasgow, R.E.; Barrera, M., Jr.; Angell, K. Effects of the Mediterranean Lifestyle Program on multiple risk behaviours and psychosocial outcomes among women at risk for heart disease. Ann. Behav. Med. 2005, 29, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Keyserling, T.C.; Samuel Hodge, C.D.; Jilcott, S.B.; Johnston, L.F.; Garcia, B.A.; Gizlice, Z.; Gross, M.D.; Saviñon, C.E.; Bangdiwala, S.I.; Will, J.C.; et al. Randomized trial of a clinic-based; community-supported, lifestyle intervention to improve physical activity and diet: The North Carolina enhanced WISEWOMAN project. Prev. Med. 2008, 46, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Lorig, K.; Ritter, P.L.; Villa, F.J.; Armas, J. Community-based peer-led diabetes self-management: A randomized trial. Diabetes Educ. 2009, 35, 641–651. [Google Scholar] [CrossRef] [PubMed]
- Garrett, N.; Hageman, C.M.; Sibley, S.D.; Davern, M.; Berger, M.; Brunzell, C.; Malecha, K.; Richards, S.W. The effectiveness of an interactive small group diabetes intervention in improving knowledge, feeling of control, and behaviour. Health Promot. Pract. 2005, 6, 320–328. [Google Scholar] [CrossRef] [PubMed]
- Robinson-Whelen, S.; Hughes, R.B.; Taylor, H.B.; Colvard, M.; Mastel-Smith, B.; Nosek, M.A. Improving the health and health behaviours of women aging with physical disabilities: A peer-led health promotion program. Womens Health Issues 2006, 16, 334–345. [Google Scholar] [CrossRef] [PubMed]
- Gary, T.L.; Bone, L.R.; Hill, M.N.; Levine, D.M.; McGuire, M.; Saudek, C.; Brancati, F.L. Randomized controlled trial of the effects of nurse case manager and community health worker interventions on risk factors for diabetes-related complications in Urban African Americans. Prev. Med. 2003, 37, 23–32. [Google Scholar] [CrossRef]
- Corkery, E.; Palmer, C.; Foley, M.E.; Schechter, C.B.; Frisher, L.; Roman, S.H. Effect of a bicultural community health worker on completion of diabetes education in a Hispanic population. Diabetes Care 1997, 20, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Dale, J.R.; Williams, S.M.; Bowyer, V. What is the effect of peer support on diabetes outcomes in adults? A systematic review. Diabet. Med. 2012, 29, 1361–1377. [Google Scholar] [CrossRef] [PubMed]
- Parry, M.; Watt-Watson, J. Peer support intervention trials for individuals with heart disease: A systematic review. Eur. J. Cardiovasc. Nurs. 2010, 9, 57–67. [Google Scholar] [CrossRef] [PubMed]
- NICE. Behaviour Change: General Approaches. Public Health Guideline. 2007. Available online: http://nice.org.uk/guidance/ph6 (accessed on 22 July 2017).
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Medical Research Council Guidance. Developing and evaluating complex interventions: The new Medical Research Council guidance. Br. Med. J. 2008, 337, 1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.E.; McEvoy, C.T.; McKinley, M.C.; Woodside, J.V. The effectiveness of peer support in encouraging dietary behaviour change in adults: A systematic review. Proc. Nutr. Soc. 2017, 76, E111. [Google Scholar] [CrossRef]
- McEvoy, C.T.; McAuley, E.; Moore, S.E.; Cupples, M.E.; Kee, F.; Young, I.S.; McKinley, M.C.; Woodside, J.V. A systematic review and meta-analysis of the effectiveness of peer support to reduce cardiovascular risk. Proc. Nutr. Soc. 2017, 76, E117. [Google Scholar] [CrossRef]
- Moore, S.E.; McEvoy, C.T.; Prior, L.; Lawton, J.; Patterson, C.C.; Kee, F.; Cupples, M.; Young, I.S.; Appleton, K.; McKinley, M.C.; et al. Barriers to adopting a Mediterranean diet in Northern European adults at high risk of developing cardiovascular disease. J. Hum. Nutr. Diet. 2017. [Google Scholar] [CrossRef] [PubMed]
- Erwin, C.M.; McEvoy, C.T.; Moore, S.E.; Prior, L.; Lawton, J.; Kee, F.; Cupples, M.; Young, I.S.; Appleton, K.; McKinley, M.C.; et al. A qualitative analysis Exploring preferred methods of peer support approaches to encourage adherence of a Mediterranean diet in a Northern European population at high risk of cardiovascular disease. BMC Public Health 2018, 18, 213. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behaviour change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behaviour change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef] [PubMed]
- Siero, F.W.; Broer, J.; Bemelmans, W.J.; Meyboom-de Jong, B.M. Impact of group nutrition education and surplus value of Prochaska-based stage-matched information on health-related cognitions and on Mediterranean nutrition behaviour. Health Educ. Res. 2000, 15, 635–647. [Google Scholar] [CrossRef] [PubMed]
- British Cardiac Society; British Hypertension Society; Diabetes UK; HEART UK; Primary Care Cardiovascular Society; The Stroke Association. JBS 2: Joint British Societies’ guidelines on prevention of cardiovascular disease in clinical practice. Heart 2005, 91, v1–v52. [Google Scholar] [CrossRef]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [PubMed]
- McCall, D.O.; McGartland, C.P.; McKinley, M.C.; Patterson, C.C.; Sharpe, P.; McCance, D.R.; Young, I.S.; Woodside, J.V. Dietary intake of fruits and vegetables improves microvascular function in hypertensive subjects in a dose-dependent manner. Circulation 2009, 119, 2153–2160. [Google Scholar] [CrossRef] [PubMed]
- Craft, N.E.; Wise, S.A.; Soares, J.H. Optimisation of an isocratic high performance liquid chromatography separation of carotenoids. J. Chromatogr. 1992, 589, 171–176. [Google Scholar] [CrossRef]
- Vuillemier, J.P.; Keck, E. Fluorometric assay of vitamin C in biological materials using a centrifugal analyser with fluorescence attachment. J. Micronutr. Anal. 1989, 5, 25–34. [Google Scholar]
- Morrison, W.R.; Smith, L.M. Preparation of fatty acid methyl esters and dimethylacetals from Lipids with Boron Trifluoride methanol. J. Lipid Res. 1964, 5, 600–608. [Google Scholar] [PubMed]
- Folch, J.; Lees, M.; Sloane Stanley, G.H. A simple method for the isolation and purification of total Lipides from animal tissues. J. Biol. Chem. 1957, 226, 497–509. [Google Scholar] [PubMed]
- Barrera, M., Jr.; Toobert, D.J.; Angell, K.L.; Glasgow, R.E.; Mackinnon, D.P. Social support and social-ecological resources as mediators of lifestyle intervention effects for type 2 diabetes. J. Health Psychol. 2006, 11, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Parmenter, K.; Wardle, J. Development of a general nutrition knowledge questionnaire for adults. Eur. J. Clin. Nutr. 1999, 53, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Calfas, K.J.; Sallis, J.F.; Zabinski, M.F.; Wilfley, D.E.; Rupp, J.; Prochaska, J.J.; Thompson, S.; Pratt, M.; Patrick, K. Preliminary evaluation of a multicomponent program for nutrition and physical activity change in primary care: PACE+ for Adults. Prev. Med. 2002, 34, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Wareham, N.J.; Jakes, R.W.; Rennie, K.L.; Mitchell, J.; Hennings, S.; Day, N.E. Validity and repeatability of the EPIC-Norfolk Physical Activity Questionnaire. Int. J. Epidemiol. 2002, 31, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Golubic, R.; May, A.M.; Benjaminsen Borch, K.; Overvad, K.; Charles, M.A.; Diaz, M.J.; Amiano, P.; Palli, D.; Valanou, E.; Vigl, M.; et al. Validity of electronically administered Recent Physical Activity Questionnaire (RPAQ) in ten European countries. PLoS ONE 2014, 9, e92829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glanz, K.; Rimer, B.K.; Lewis, F.M. Health Behaviour and Health Education: Theory; Research and Practice, 3rd ed.; Wiley & Sons: San Fransisco, CA, USA, 2002. [Google Scholar]
- Apolone, G.; Mosconi, P. The Italian SF-36 Health Survey: Translation, validation and norming. J. Clin. Epidemiol. 1998, 51, 1025–1036. [Google Scholar] [CrossRef]
- EuroQol Group. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar]
- Corle, D.K.; Sharbaugh, C.; Mateski, D.J.; Coyne, T.; Paskett, E.D.; Cahill, J.; Daston, C.; Lanza, E.; Schatzkin, A. PPT Study Group. Polyp Prevention Trial. Self-Related Quality of Life Measures: Effect of change to a Low-Fat, High-Fibre, Fruit and Vegetable Enriched Diet. Ann. Behav. Med. 2001, 23, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1998, 54, 1063–1070. [Google Scholar] [CrossRef]
- Rosenberg, F. Global self-esteem and specific self-esteem: Different concepts, different outcomes. Am. Sociol. Rev. 1995, 60, 141–156. [Google Scholar] [CrossRef]
- Davis, C.R.; Hodgson, J.M.; Woodman, R.; Bryan, J.; Wilson, C.; Murphy, K.J. A Mediterranean diet lowers blood pressure and improves endothelial function: Results from the MedLey randomized intervention trial. Am. J. Clin. Nutr. 2017, 105, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Davis, C.R.; Bryan, J.; Hodgson, J.M.; Woodman, R.; Murphy, K.J. A Mediterranean Diet Reduces F2-Isoprostanes and Triglycerides among Older Australian Men and Women after 6 Months. J. Nutr. 2017, 147, 1348–1355. [Google Scholar] [CrossRef] [PubMed]
- Murphy, K.J.; Parletta, N. Implementing a Mediterranean-Style Diet outside the Mediterranean Region. Curr. Atheroscler. Rep. 2018, 20, 28. [Google Scholar] [CrossRef] [PubMed]
- Marteau, T.; Dieppe, P.; Foy, R.; Kinmonth, A.L.; Schneiderman, N. Behavioural medicine: Changing our behaviour. Br. Med. J. 2006, 332, 437–438. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| TEAM-MED Intervention Groups | BCTs (n) | BCT Label (from BCT Taxonomy 1 or CALO-RE 2) | BCT Definition | Example of BCT Delivery in the Intervention Groups |
|---|---|---|---|---|
| Group 1: Peer support | 18 | Provide information on consequences of behaviour in general 2 | Information about the relationship between the behaviour and its possible or likely consequences in the general case, usually based on epidemiological data, and not personalised for the individual | Peer supporters show a short video clip to group members demonstrating the health effects of a MD |
| Provide normative behaviour about others’ behaviour 2 | Involves providing information about what other people are doing i.e., indicates that a particular behaviour or sequence of behaviours is common or uncommon amongst the population or amongst a specified group—presentation of case studies of a few others is not normative information. | Peer supporters provide information about current MD adherence in Northern European populations | ||
| Goal setting (Behaviour) 1,2 | Set or agree on a goal defined in terms of the behaviour to be achieved | Peer supporters support members to set MD goals at each group session based on the session topic | ||
| Goal setting (outcome) 1,2 | Set or agree on a goal defined in terms of a positive outcome of wanted behaviour | Group members are encouraged within their personal planners to define what they want to achieve by taking part in the peer support groups, e.g., target weight loss, or decreasing to target blood pressure level etc. | ||
| Action planning 1,2 | Prompt detailed planning of performance of the behaviour | Peer supporters support members to set MD goals that are easy to measure, something that can be achieved, small and meaningful (i.e., SMART goals) at each group session | ||
| Barrier identification/problem solving 1,2 | Analyse, or prompt the person to analyse, factors influencing the behaviour and generate or select strategies that include overcoming barriers and/or increasing facilitators | Peer supporters facilitate group discussion to identify barriers/challenges in achieving personal MD goals and assist members to select the best strategies to overcome these | ||
| Set graded tasks 1,2 | Set easy-to-perform tasks, making them increasingly difficult, but achievable, until behaviour is performed | Increasing adherence to a MD is broken down into smaller tasks within written materials, e.g., food swaps are listed separately for each major MD component | ||
| Prompt review of behavioural goals 2 | Involves a review or analysis of the extent to which previously set behavioural goals were achieved | Each group session will provide an opportunity for general progress review in terms of behaviour | ||
| Prompt self-monitoring of behaviour 2 | The person is asked to keep a record of specified behaviour(s) as a method for changing behaviour. | Group members are given personal planners to monitor their daily/weekly progress in achieving set MD goals and to allow them to record any barriers/challenges they experience | ||
| Prompt self-monitoring of behavioural outcome 2 | The person is asked to keep a record of specified measures expected to be influenced by the behaviour change | Group members are encouraged to log and monitor their weight, blood pressure etc. in personal planners | ||
| Provide information on when and where to perform the behaviour 2 | Involves telling the person about when and where they might be able to perform the behaviour | Recipe books and written information provide information regarding different meals, and also eating out as well as eating in the home | ||
| Provide instruction on how to perform behaviour 1,2 | Involves telling the person how to perform behaviours, either verbally or in written form. | Peer supporters provide group members with a booklet and a visual guide (MD food pyramid) to provide instruction on the types and proportions of food components in a MD | ||
| Model/demonstrate the behaviour 1,2 | Provide an observable sample of the performance of the behaviour, directly in person or indirectly | Peer supporters show a short video clip to group members demonstrating preparation and consumption of a MD on a budget and food tasting sessions form part of peer group meetings | ||
| Use of follow-up prompts 2 | Intervention components are gradually reduced in intensity, duration and frequency over time, e.g., letters or telephone calls instead of face-to-face and/or provided at longer time intervals | Group sessions decrease in frequency after six months | ||
| Plan social support/social change 2 | Involves prompting the person to plan how to elicit social support from other people to help him/her achieve their target behaviour/outcome. | Group members are encouraged to support and contact each other between group sessions | ||
| Relapse prevention/coping planning 2 | This relates to planning how to maintain behaviour that has been changed. The person is prompted to identify in advance situations in which the changed behaviour may not be maintained and develop strategies to avoid or manage those situations | One group session (session nine) is dedicated to maintenance of dietary change and relapse prevention | ||
| Biofeedback 1 | Provide feedback about the body using an external monitoring device as part of a behaviour change strategy | Peer supporters offer individual feedback on blood pressure and weight measurements at each group session | ||
| Social support 1 | Advise on, arrange or provide social support or non-contingent praise or reward for performance of the behaviour | Peer supporters and group members provide positive encouragement and support to each-other to adopt new MD behaviours | ||
| Group 2: Dietitian-led support | 20 | Motivational interviewing 2,* | This is a clinical method including a specific set of techniques involving prompting the person to engage in change talk in order to minimise resistance and resolve ambivalence to change | Participants attend individual motivational interviewing delivered by a trained dietitian |
| Provide information on consequences of behaviour in general 2 | Information about the relationship between the behaviour and its possible or likely consequences in the general case, usually based on epidemiological data, and not personalised for the individual | Dietitian shows a short video clip demonstrating the health effects of a MD within the structured group education sessionHealth consequences of MD also detailed in educational material | ||
| Provide information on consequences of behaviour to the individual 2 | Information about the benefits and costs of action or inaction to the individual or tailored to a relevant group based on that individual’s characteristics | Discussion of dietary change to encourage adherence to a MD occurs specifically based on individual’s current level of adherence, and with knowledge of their CVD risk score | ||
| Provide normative behaviour about others’ behaviour 2 | Involves providing information about what other people are doing i.e., indicates that a particular behaviour or sequence of behaviours is common or uncommon amongst the population or amongst a specified group—presentation of case studies of a few others is not normative information. | Dietitian provides information about current MD adherence in Northern European populations | ||
| Goal setting (Behaviour) 1,2 | Set or agree on a goal defined in terms of the behaviour to be achieved | Discussed during motivational interview with dietitian | ||
| Goal setting (outcome) 1,2 | Set or agree on a goal defined in terms of a positive outcome of wanted behaviour | Discussed during motivational interview with dietitian | ||
| Action planning 1,2 | Prompt detailed planning of performance of the behaviour | Discussed during motivational interview with dietitian | ||
| Set graded tasks 1,2 | Set easy-to-perform tasks, making them increasingly difficult, but achievable, until behaviour is performed | Increasing adherence to a MD is broken down into smaller tasks within educational materials, e.g., food swaps are listed separately for each major MD component Reinforced by dietitian in group education session and in individual session | ||
| Provide information on when and where to perform the behaviour 2 | Involves telling the person about when and where they might be able to perform the behaviour | Recipe books and written information provide information regarding different meals, and also eating out as well as eating in the home | ||
| Provide instruction on how to perform behaviour 1,2 | Involves telling the person how to perform behaviours, either verbally or in written form. | Practical support around shopping lists, recipes, food storage and preparation given within educational material | ||
| Barrier identification/problem solving 1,2 | Analyse, or prompt the person to analyse, factors influencing the behaviour and generate or select strategies that include overcoming barriers and/or increasing facilitators | Discussion about challenges in meeting dietary goals and developing strategies to overcome these in group education session | ||
| Prompt review of behavioural goals 2 | Involves a review or analysis of the extent to which previously set behavioural goals were achieved | Individual progress review and feedback provided at end of group education session | ||
| Prompt self-monitoring of behaviour 2 | The person is asked to keep a record of specified behaviour(s) as a method for changing behaviour | Plan to monitor progress in achieving goals developed during motivational interview | ||
| Provide feedback on performance 2 | This involves providing the participant with data about their own recorded behaviour | Individual progress review and feedback provided at end of group education session | ||
| Model/demonstrate the behaviour 1,2 | Provide an observable sample of the performance of the behaviour, directly in person or indirectly | Video clip demonstrating preparation and consumption of a MD on a budget shown in group education session | ||
| Plan social support/social change 2 | Involves prompting the person to plan how to elicit social support from other people to help him/her achieve their target behaviour/outcome. | Discussion of support around family structure and food purchasing/preparation included in motivational interview and individual progress review. Social support encouraged through participation in group education session with other participants. | ||
| Relapse prevention/coping planning 2 | This relates to planning how to maintain behaviour that has been changed. The person is prompted to identify in advance situations in which the changed behaviour may not be maintained and develop strategies to avoid or manage those situations. | Challenging situations discussed during both motivational interview and group education session | ||
| Commitment 1 | Ask the person to affirm or reaffirm statements indicating commitment to change the behaviour | Affirmation of personal dietary goals sought during motivational interview | ||
| Credible source 1 | Present verbal or visual communication from a credible source in favour of or against the behaviour | Both motivational interview and group education session delivered by trained dietitian | ||
| Adding objects to the environment 1 | Add objects to the environment in order to facilitate performance of the behaviour | Key foods delivered to participants | ||
| Group 3: Minimal support | 4 | Provide information on consequences of behaviour in general 2 | Information about the relationship between the behaviour and its possible or likely consequences in the general case, usually based on epidemiological data, and not personalised for the individual | Health consequences of MD detailed in educational material |
| Set graded tasks 1,2 | Set easy-to-perform tasks, making them increasingly difficult, but achievable, until behaviour is performed | Increasing adherence to a MD is broken down into smaller tasks within written materials, e.g., food swaps are listed separately for each major MD component | ||
| Provide information on when and where to perform the behaviour 2 | Involves telling the person about when and where they might be able to perform the behaviour | Recipe books and written information provide information regarding different meals, and also eating out as well as eating in the home | ||
| Provide instruction on how to perform behaviour 1,2 | Involves telling the person how to perform behaviours, either verbally or in written form. | Practical support around shopping lists, recipes, food storage and preparation given within educational material |
| Day | Training Components |
|---|---|
| One (7 h) | Mediterranean Diet food components, health benefits and pyramid model Role of a peer supporter Group intervention format, content and introduction to resources Practical dietary advice to overcome barriers to eating a Mediterranean diet Weight and blood pressure measurement workshop including provision of feedback Maintaining study documentation for group sessions |
| Two (7 h) | Social support in a group setting to encourage dietary change Group facilitation skills Delivering group resources Handling difficult group situations |
| Outcome | Domain to Be Measured | Data Collection Method(s) | Baseline | 3 Months | 6 Months | 12 Months |
|---|---|---|---|---|---|---|
| Diet | MD adherence | 14-item MDS questionnaire [8] 2 | √ | √ | √ | √ |
| Dietary intake | Food record (4-day) | √ | √ | √ | √ | |
| Clinical & biomarker | Nutritional biomarkers | Venepuncture (fasting blood sample) OGTT | √ | √ | √ | √ |
| Impaired glucose tolerance | √ | √ | √ | √ | ||
| HbA1C | √ | √ | √ | √ | ||
| Blood pressure | Clinic measured [41] | √ | √ | √ | √ | |
| Nutrition and CVD markers | Urine sample (spot fasting sample) | √ | √ | √ | √ | |
| Weight | Digital scales | √ | √ | √ | √ | |
| Height | Stadiometer | √ | √ | √ | √ | |
| Waist circumference | Flexible tape | √ | √ | √ | √ | |
| Mediators of diet behaviour change | MD knowledge | Nutrition knowledge questionnaire [47] 2 | √ | √ | √ | √ |
| Readiness to change | Stage of dietary change questionnaire [38] | √ | √ | √ | √ | |
| Perceived barriers to MD | Eating habits questionnaire 1 | √ | √ | √ | √ | |
| Self-efficacy | Questionnaire [48] | √ | √ | √ | √ | |
| Social support | Questionnaire [46] 2 | √ | × | √ | √ | |
| Problem solving ability | Questionnaire [20] 2 | √ | √ | √ | √ | |
| Intervention Moderators | Physical activity | RPAQ questionnaire [49,50] | √ | √ | √ | √ |
| Smoking, alcohol, medication use | Questionnaire 1 | √ | √ | √ | √ | |
| Health beliefs | Health belief questionnaire [51] 2 | √ | √ | √ | √ | |
| Health-related Quality of Life | SF-36 [52]; EQ-5D-3L [53] | √ | √ | √ | √ | |
| Diet-related Quality of life | Questionnaire [54] 2 | √ | √ | √ | √ | |
| Mood | Questionnaire [55] | √ | √ | √ | √ | |
| Self-esteem | Self-esteem questionnaire [56] | √ | √ | √ | √ |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McEvoy, C.T.; Moore, S.E.; Appleton, K.M.; Cupples, M.E.; Erwin, C.M.; Hunter, S.J.; Kee, F.; McCance, D.; Patterson, C.C.; Young, I.S.; et al. Trial to Encourage Adoption and Maintenance of a Mediterranean Diet (TEAM-MED): Protocol for a Randomised Feasibility Trial of a Peer Support Intervention for Dietary Behaviour Change in Adults at High Cardiovascular Disease Risk. Int. J. Environ. Res. Public Health 2018, 15, 1130. https://doi.org/10.3390/ijerph15061130
McEvoy CT, Moore SE, Appleton KM, Cupples ME, Erwin CM, Hunter SJ, Kee F, McCance D, Patterson CC, Young IS, et al. Trial to Encourage Adoption and Maintenance of a Mediterranean Diet (TEAM-MED): Protocol for a Randomised Feasibility Trial of a Peer Support Intervention for Dietary Behaviour Change in Adults at High Cardiovascular Disease Risk. International Journal of Environmental Research and Public Health. 2018; 15(6):1130. https://doi.org/10.3390/ijerph15061130
Chicago/Turabian StyleMcEvoy, Claire T., Sarah E. Moore, Katherine M. Appleton, Margaret E. Cupples, Christina M. Erwin, Steven J. Hunter, Frank Kee, David McCance, Christopher C. Patterson, Ian S. Young, and et al. 2018. "Trial to Encourage Adoption and Maintenance of a Mediterranean Diet (TEAM-MED): Protocol for a Randomised Feasibility Trial of a Peer Support Intervention for Dietary Behaviour Change in Adults at High Cardiovascular Disease Risk" International Journal of Environmental Research and Public Health 15, no. 6: 1130. https://doi.org/10.3390/ijerph15061130
APA StyleMcEvoy, C. T., Moore, S. E., Appleton, K. M., Cupples, M. E., Erwin, C. M., Hunter, S. J., Kee, F., McCance, D., Patterson, C. C., Young, I. S., McKinley, M. C., & Woodside, J. V. (2018). Trial to Encourage Adoption and Maintenance of a Mediterranean Diet (TEAM-MED): Protocol for a Randomised Feasibility Trial of a Peer Support Intervention for Dietary Behaviour Change in Adults at High Cardiovascular Disease Risk. International Journal of Environmental Research and Public Health, 15(6), 1130. https://doi.org/10.3390/ijerph15061130