Prescribing Physical Activity in Parks to Improve Health and Wellbeing: Protocol of the Park Prescription Randomized Controlled Trial

Abstract
:1. Introduction
1.1. Study Objectives
- improving participants’ total volume of physical activity per week, reflecting average acceleration peroin gravitational units (mg); the amount of light physical activity in minutes per week, the amount of sedentary behavior in hours per week (all assessed via accelerometer);
- improving participants’ self-reported health behaviors including time spent in parks, physical activity time in parks, recreational physical activity and sedentary behavior;
- promoting participants’ self-reported mental well-being; and,
- improving participants’ objectively measured physical health.
2. Materials and Methods
2.1. Study Design
2.2. Trial Setting
2.3. Eligibility Criteria
- Singapore citizen or Permanent Resident;
- aged 40–65 years;
- self-reported weekly exercise of <150 min per week;
- blood pressure of ≤139 mmHG (systolic) over ≤89 mmHG (diastolic);
- fasting glucose level of ≤6.0 mmol/L;
- pass the adapted Physical Activity Readiness Questionnaire (PAR-Q) [21];
- able to write and read in English or Chinese; and,
- provide written informed consent.
2.4. Intervention
2.4.1. Group 1—Park Prescription Trial (PPT) Intervention
2.4.2. Group 2—Control
2.5. Outcomes
2.5.1. Primary Outcome
2.5.2. Secondary Outcomes
2.6. Sample Size Calculation
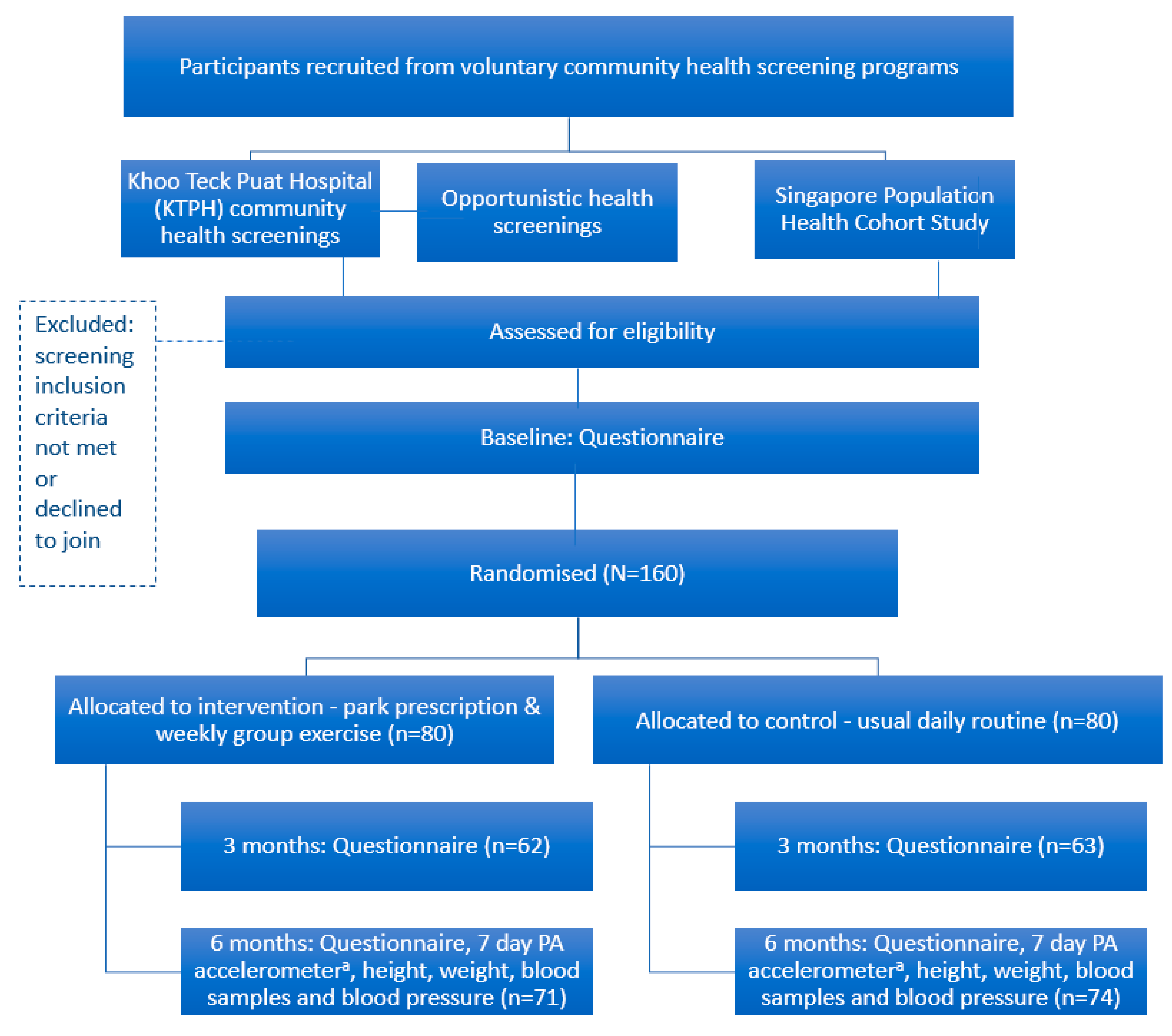
2.7. Recruitment
2.7.1. Main Recruitment Mechanism: KTPH Community Screening Program
2.8. Participant Timeline
2.9. Assignment of Interventions
2.10. Data Collection and Analysis
2.10.1. Data Collection
2.10.2. Data Management
2.10.3. Statistical Analysis
2.11. Ethics and Dissemination
2.11.1. Research Ethics Approval
2.11.2. Declaration of Interests
2.11.3. Dissemination Policy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Trial Registration
References
- Kohl, H.W., 3rd; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S. The pandemic of physical inactivity: Global action for public health. Lancet 2012, 380, 294–305. [Google Scholar] [CrossRef]
- Yoon, K.-H.; Lee, J.-H.; Kim, J.-W.; Cho, J.H.; Choi, Y.-H.; Ko, S.-H.; Zimmet, P.; Son, H.-Y. Epidemic obesity and type 2 diabetes in Asia. Lancet 2006, 368, 1681–1688. [Google Scholar] [CrossRef]
- Diabetes: The War Continues. Available online: https://www.moh.gov.sg/content/moh_web/home/pressRoom/pressRoomItemRelease/2017/diabetes--the-war-continues.html (accessed on 20 October 2017).
- Bhalla, V.; Fong, C.W.; Chew, S.K.; Satku, K. Changes in the levels of major cardiovascular risk factors in the multi-ethnic population in Singapore after 12 years of a national non-communicable disease intervention program. Singap. Med. J. 2006, 47, 841–850. [Google Scholar]
- Goh, L.; Pang, J. Obesity in Singapore, prevention and control. Singap. Fam. Phys. 2012, 38, 8–13. [Google Scholar]
- Toh, C.M.; Chew, S.K.; Tan, C.C. Prevention and control of non-communicable diseases in Singapore: A review of national health promotion programs. Singap. Med. J. 2002, 43, 333–339. [Google Scholar]
- Sallis, J.F.; Bull, F.; Guthold, R.; Heath, G.W.; Inoue, S.; Kelly, P.; Oyeyemi, A.L.; Perez, L.G.; Richards, J.; Hallal, P.C. Progress in physical activity over the Olympic quadrennium. Lancet 2016, 388, 1325–1336. [Google Scholar] [CrossRef]
- Win, A.M.; Yen, L.W.; Tan, K.H.; Lim, R.B.T.; Chia, K.S.; Mueller-Riemenschneider, F. Patterns of physical activity and sedentary behavior in a representative sample of a multi-ethnic South-East Asian population: A cross-sectional study. BMC Public Health 2015, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-J.; Huang, Y.-H.; Lu, F.-H.; Wu, J.-S.; Lin, L.L.; Chang, C.-J.; Yang, Y.-C. The correlates of leisure time physical activity among an adults population from southern Taiwan. BMC Public Health 2011, 11, 427. [Google Scholar] [CrossRef] [PubMed]
- Egorov, A.I.; Mudu, P.; Braubach, M.; Martuzzi, M. Urban Green Spaces and Health; WHO Regional Office for Europe: Copenhagen, Denmark, 2016. [Google Scholar]
- Fong, K.C.; Hart, J.E.; James, P. A review of epidemiologic studies on greenness and health: Updated literature through 2017. Curr. Environ. Health Rep. 2018, 5, 77–87. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Banay, R.F.; Hart, J.E.; Laden, F. A Review of the Health Benefits of Greenness. Curr. Epidemiol. Rep. 2015, 2, 131–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, R.F.; Christian, H.; Veitch, J.; Astell-Burt, T.; Hipp, J.A.; Schipperijn, J. The impact of interventions to promote physical activity in urban green space: A systematic review and recommendations for future research. Soc. Sci. Med. 2015, 124, 246–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- PARKRx Park Prescription Programs San Francisco: Golden Gate National Parks Conservancy. Available online: http://www.parkrx.org/park-prescription-programs (accessed on 31 May 2018).
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PN, USA, 2013. [Google Scholar]
- Orrow, G.; Kinmonth, A.-L.; Sanderson, S.; Sutton, S. Effectiveness of physical activity promotion based in primary care: Systematic review and meta-analysis of randomized controlled trials. BMJ 2012, 344, e1389. [Google Scholar] [CrossRef] [PubMed]
- Sims, J.; Huang, N.; Pietsch, J.; Naccarella, L. The Victorian Active Script Program: Promising signs for general practitioners, population health and the promotion of physical activity. Br. J. Sports Med. 2004, 38, 19–25. [Google Scholar] [CrossRef]
- Messiah, S.E.; Kardys, J.; Forster, L. Reducing Childhood Obesity Through Pediatrician and Park Partnerships. J. Public Health Manag. Pract. 2017, 23, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Zarr, R.; Cottrell, L.; Merrill, C. Park Prescription (DC Park Rx): A New Strategy to Combat Chronic Disease in Children. J. Phys. Act. Health 2017, 14, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, A.-W.; Tetzlaff, J.M.; Gøtzsche, P.C.; Altman, D.G.; Mann, H.; Berlin, J.A.; Dickersin, K.; Hróbjartsson, A.; Schulz, K.F.; Parulekar, W.R. SPIRIT 2013 explanation and elaboration: Guidance for protocols of clinical trials. BMJ 2013, 346, e7586. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Reading, J.; Shephard, R.J. Revision of the Physical Activity Readiness Questionnaire (PAR-Q). Can. J. Sport Sci. 1992, 17, 338–345. [Google Scholar] [PubMed]
- Chu, A.H.; Ng, S.H.; Koh, D.; Müller-Riemenschneider, F. Reliability and validity of the self-and interviewer-administered versions of the Global Physical Activity Questionnaire (GPAQ). PLoS ONE 2015, 10, e0136944. [Google Scholar] [CrossRef] [PubMed]
- IPAQ Internaional Physical Activity Questionnaire. Available online: https://sites.google.com/site/theipaq/ (accessed on 7 February 2018).
- Group, W. Development of the WHOQOL: Rationale and current status. Int. J. Mental Health 1994, 23, 24–56. [Google Scholar] [CrossRef]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.-L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef] [PubMed]
- Sach, T.; Barton, G.; Doherty, M.; Muir, K.; Jenkinson, C.; Avery, A. The relationship between body mass index and health-related quality of life: Comparing the EQ-5D, EuroQol VAS and SF-6D. Int. J. Obes. 2007, 31, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- van Hees, V.T.; Gorzelniak, L.; Dean Leon, E.C.; Eder, M.; Pias, M.; Taherian, S.; Ekelund, U.; Renstrom, F.; Franks, P.W.; Horsch, A.; et al. Separating movement and gravity components in an acceleration signal and implications for the assessment of human daily physical activity. PLoS ONE 2013, 8, e61691. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, A.V.; Yates, T.; Davies, M.; Khunti, K.; Edwardson, C.L. Raw Accelerometer Data Analysis with GGIR R-package: Does Accelerometer Brand Matter? Med. Sci. Sports Exerc. 2016, 48, 1935–1941. [Google Scholar] [CrossRef] [PubMed]
- Elley, C.R.; Kerse, N.; Arroll, B.; Robinson, E. Effectiveness of counselling patients on physical activity in general practice: Cluster randomized controlled trial. BMJ 2003, 326, 793. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata: Release 12. Statistical Sotware; StataCorp LP: College Station, TX, USA, 2011. [Google Scholar]
- Maas, J.; Verheij, R.A.; de Vries, S.; Spreeuwenberg, P.; Schellevis, F.G.; Groenewegen, P.P. Morbidity is related to a green living environment. J. Epidemiol. Community Health 2009, 63, 967–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, D.A.; Han, B.; Derose, K.P.; Williamson, S.; Marsh, T.; McKenzie, T.L. Physical activity in parks: A randomized controlled trial using community engagement. Am. J. Prev. Med. 2013, 45, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Reis, R.S.; Salvo, D.; Ogilvie, D.; Lambert, E.V.; Goenka, S.; Brownson, R.C. Scaling up physical activity interventions worldwide: Stepping up to larger and smarter approaches to get people moving. Lancet 2016, 388, 1337–1348. [Google Scholar] [CrossRef]
- Rychetnik, L.; Bauman, A.; Laws, R.; King, L.; Rissel, C.; Nutbeam, D.; Colagiuri, S.; Caterson, I. Translating research for evidence-based public health: Key concepts and future directions. J. Epidemiol. Community Health 2012. [Google Scholar] [CrossRef] [PubMed]
- Green, L.; Kreuter, M. The precede–proceed model. In Health Promotion Planning: An Educational Approach, 3rd ed.; Mayfield Publishing Company: Mountain View, CA, USA, 1999; pp. 32–43. [Google Scholar]


{kind=link}
| Component | Description | Delivery Timing |
|---|---|---|
| Counselling | Face-to-face physical activity and park use counselling. | Commencement |
| Park Prescription | Participants completed a sheet with a trained study team member. The prescription section of the participant’s sheet outlined a goal they committed to which specified the frequency, intensity, time and location of exercise in parks. The study team retained a separate sheet with an assessment of the participant’s baseline activity level—low, moderate or active. | Commencement |
| Materials | Participants received two brochures: one developed for the Trial provided information on the main parks in the northern part of Singapore and their features, including walking trails (with time needed to complete them) and fitness corners. The other was a general brochure from the Singapore National Parks Board containing a map and information on the Northern Explorer Loop (a series of parks in Singapore’s north connected by a network of walking and cycling paths). A planning sheet, where participants filled in the types of activities they aimed to do each week over the trial period, also included information and examples. | Commencement |
| Follow-up counselling | Brief phone call counselling by a trained study team member. The counselling assessed progress towards set goals and included modification of those goals if necessary. | Three months |
| Group exercise | Structured exercise program delivered in parks by a trained group exercise instructor. To encourage attendance, participants received mobile text message reminders prior to each weekly exercise session. | Weekly over six months. |
| Primary Outcome | Measurement | Instrument | V0 | V1 | V2 |
|---|---|---|---|---|---|
| MVPA | Time spent in activity of moderate to vigorous intensity | Accelerometer | X | ||
| Secondary outcome | |||||
| Physical activity | Total physical activity volume a | Accelerometer | X | ||
| Light and sedentary activity | Time spent in light and sedentary activity | Accelerometer | X | ||
| Physical activity | Frequency, intensity, time and type | Self-administered questionnaire—GPAQ | X | X | X |
| Sedentary activity | Time spent sitting | Self-administered questionnaire—IPAQ | X | X | X |
| Park usage | Time spent in parks last month, physical activity time in parks on a typical month. | Self-administered questionnaire | X | X | X |
| Mental wellbeing | Wellness | Self-administered questionnaire—SF-12, K10, WHO5, WHOQoL-BREF b | X | X | |
| Anthropometry | BMI c—weight in kilograms divided by height in meters squared | BMI machine | X | X | |
| Biochemistry | Blood lipids, fasting blood glucose | Blood samples | X | X | |
| Blood pressure | Systolic and diastolic | Dinamap blood pressure monitor | X | X | |
| Process indicator d | |||||
| Motivation to exercise | Social support for physical activity, reasons to engage, physical activity knowledge | Self-administered questionnaire—BREQ-2 | X | ||
| Attitudes and behaviors | Perceived changes in participants’ attitudes and behaviors towards physical activity and park use, intention to continue group exercise | Self-administered questionnaire. | X | ||
| Satisfaction with and quality of program | Satisfaction with and quality of prescription sheet and parks brochure | Self-administered questionnaire | X | ||
| Satisfaction with and quality of physical activity planning sheet | Self-administered questionnaire | X | |||
| Satisfaction with and quality of phone counselling | Self-administered questionnaire | X | |||
| Satisfaction with and quality of program overall | Self-administered questionnaire | X | |||
| Outcome | Hypothesis | Definition | Analysis |
|---|---|---|---|
| (1) Primary | |||
| Time spent on MVPA a—objective measure | Improvement in MVPA in intervention group as compared to control group at six months | Time spent on MVPA in minutes per week as measured by the accelerometer | t-test. Linear regression |
| (2) Secondary | |||
| a. Health behaviors | Improvement in health behaviors in intervention group as compared to control group at six months | ||
| Total volume of physical activity | Total activity volume as measured by the accelerometer b | t-test. Linear regression | |
| Time spent on light and sedentary activity | Time spent per week on light and sedentary physical activity as measured by the accelerometer | t-test. Linear regression | |
| Time spent on MVPA—subjective measure | Self-reported time (minutes) per week spent on MVPA as recorded in questionnaire | t-test. Linear regression | |
| Time spent in parks; time spent being physically active in parks | Self-reported time (minutes) in parks in the past month; and time spent engaging in physical activity in parks in a typical month as recorded in the questionnaire | t-test. Linear regression | |
| Recreational MVPA time | Self-reported time (minutes) per week spent on recreational activity as measured by GPAQa | t-test. Linear regression | |
| Sitting time | Self-reported time (minutes) per week spent sitting as measured by IPAQ a | t-test. Linear regression | |
| b. Mental wellbeing | Improvement in mental wellbeing in intervention group as compared to control group at six months | ||
| Mental wellbeing | Self-reported mental wellbeing as measured by SF-12 (1-item, general health), K-10, WHO5 and WHOQOL-BREFa | t-test. Linear regression. Logistic regression | |
| c. Physical health | Improvement in physical health in intervention group as compared to control group at six months | ||
| Body Mass Index (BMI) | Weight in kg divided by height squared in m measured by BMI machine. | t-test. Linear regression | |
| Fasting blood glucose | Fasting blood glucose in mmol/L. Laboratory assessment | t-test. Linear regression | |
| Systolic and diastolic blood pressure | Systolic and diastolic blood pressure in mmHG measured by a Dinamap blood pressure monitor | t-test. Linear regression |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Müller-Riemenschneider, F.; Petrunoff, N.; Sia, A.; Ramiah, A.; Ng, A.; Han, J.; Wong, M.; Choo, T.B.; Uijtdewilligen, L. Prescribing Physical Activity in Parks to Improve Health and Wellbeing: Protocol of the Park Prescription Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2018, 15, 1154. https://doi.org/10.3390/ijerph15061154
Müller-Riemenschneider F, Petrunoff N, Sia A, Ramiah A, Ng A, Han J, Wong M, Choo TB, Uijtdewilligen L. Prescribing Physical Activity in Parks to Improve Health and Wellbeing: Protocol of the Park Prescription Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2018; 15(6):1154. https://doi.org/10.3390/ijerph15061154
Chicago/Turabian StyleMüller-Riemenschneider, Falk, Nick Petrunoff, Angelia Sia, Anbumalar Ramiah, Alwyn Ng, Jane Han, Michael Wong, Tai Bee Choo, and Léonie Uijtdewilligen. 2018. "Prescribing Physical Activity in Parks to Improve Health and Wellbeing: Protocol of the Park Prescription Randomized Controlled Trial" International Journal of Environmental Research and Public Health 15, no. 6: 1154. https://doi.org/10.3390/ijerph15061154
APA StyleMüller-Riemenschneider, F., Petrunoff, N., Sia, A., Ramiah, A., Ng, A., Han, J., Wong, M., Choo, T. B., & Uijtdewilligen, L. (2018). Prescribing Physical Activity in Parks to Improve Health and Wellbeing: Protocol of the Park Prescription Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 15(6), 1154. https://doi.org/10.3390/ijerph15061154