Changes in Risk Perception of the Health Effects of Radiation and Mental Health Status: The Fukushima Health Management Survey

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
2.3. Study Population
2.4. Assessments
2.5. Analysis
3. Results
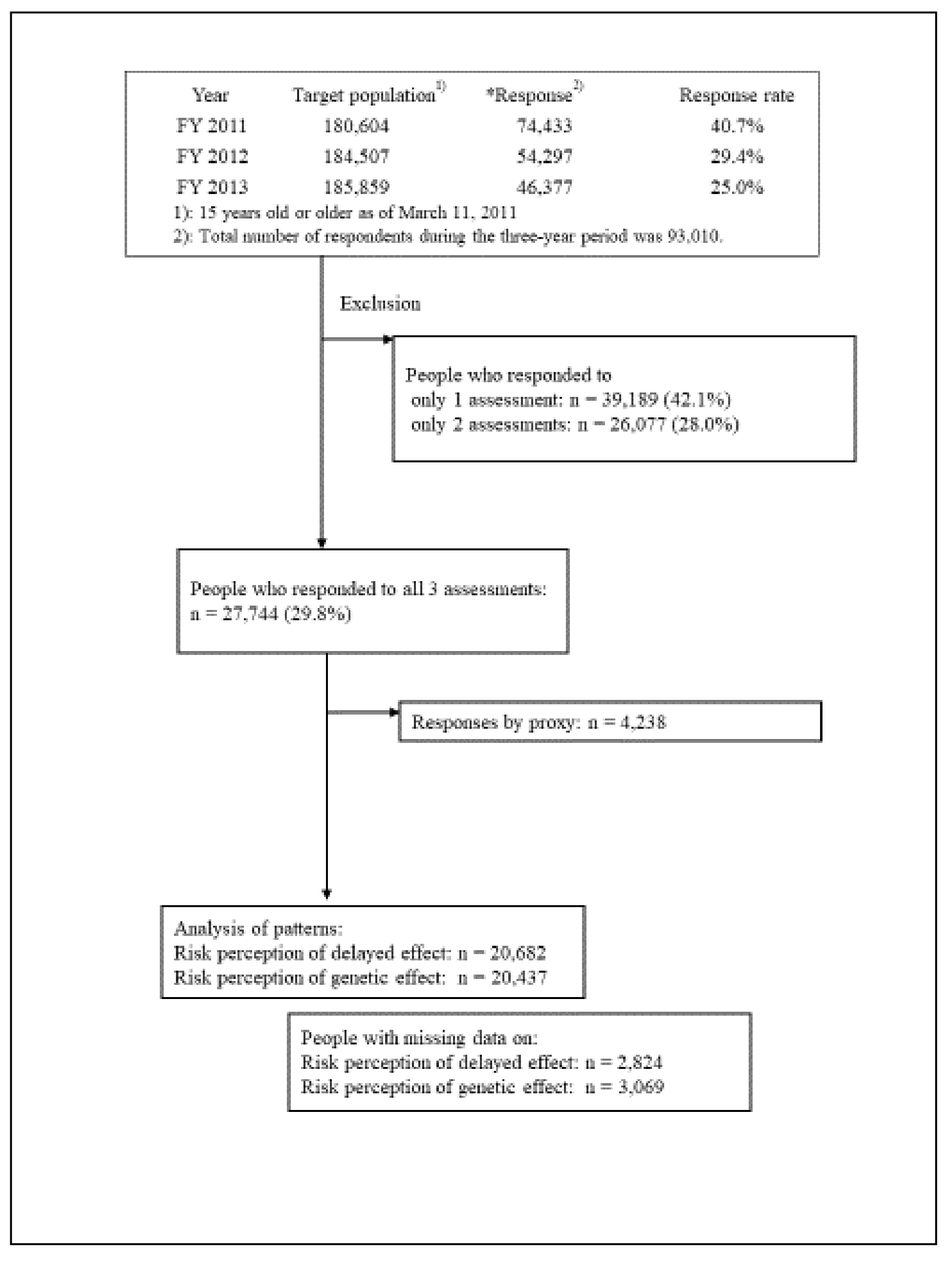
3.1. Participants
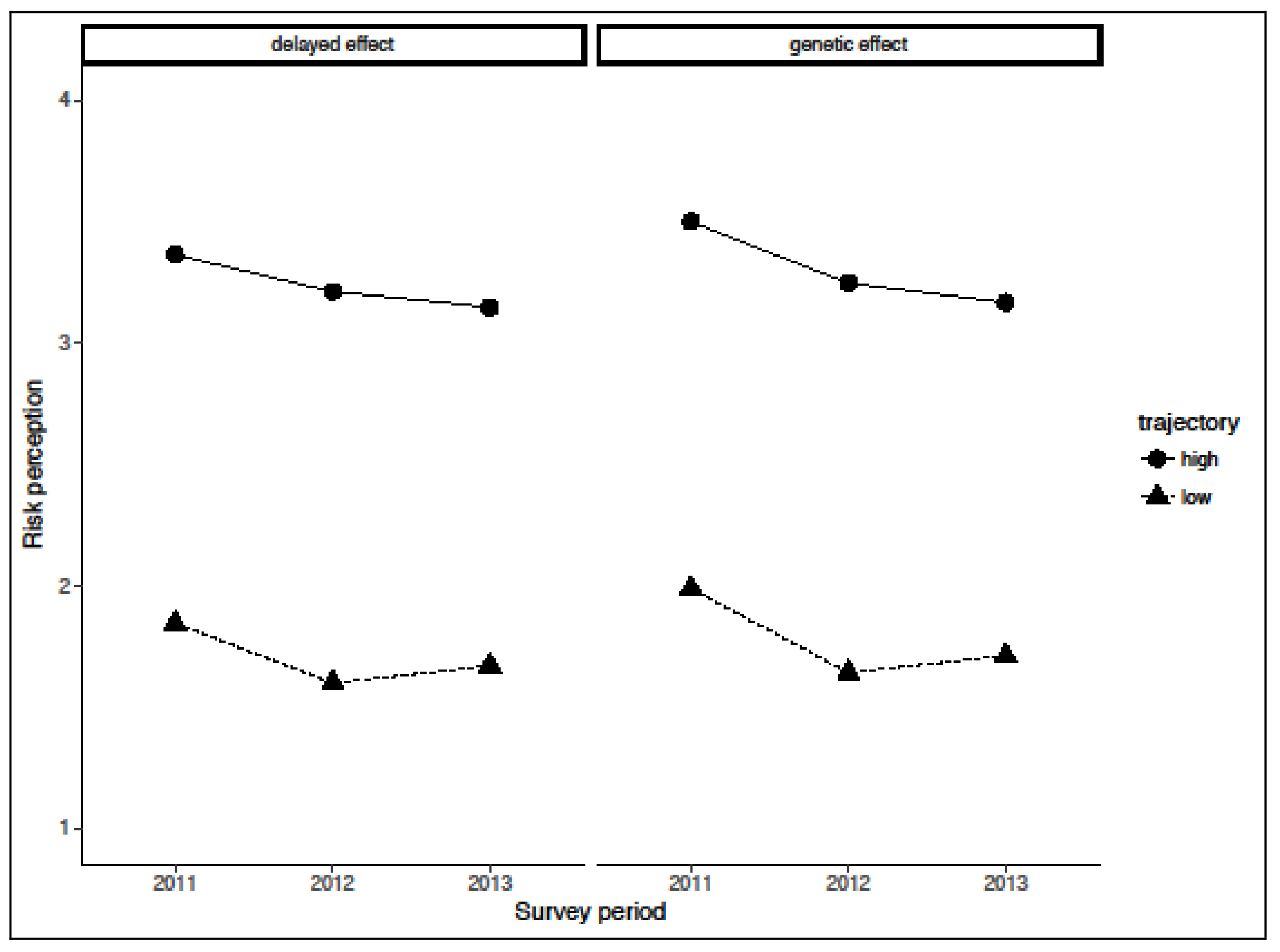
3.2. Trajectory Analysis
3.3. Logistic Regression Analysis for Predicting High-Risk Perception
4. Discussion
4.1. Trajectories
4.2. Impact of Traumatic Reaction on Change in Risk Perception
4.3. Associated Factors of Risk Perception Pattern
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- United Nations Scientific Committee on the Effects of Atomic Radiation. Chapter III. Scientific finding. In Sources, Effects and Risks of Ionizing Radiation; UNSCEAR 2013 Reports to the General Assembly with Scientific Annexes; United Nations: New York, NY, USA, 2014; ISBN 978-92-1-142291-7. [Google Scholar]
- Suzuki, Y.; Yabe, H.; Yasumura, S.; Ohira, T.; Niwa, S.; Ohtsuru, A.; Mashiko, H.; Maeda, M.; Abe, M. Psychological distress and the perception of radiation risks: The Fukushima health management survey. Bull World Health Organ 2015, 93, 598–605. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Chapter 6 Non-cancer and non-thyroid health effects. In Health Effects of the Chernobyl Accident and Special Health Care Programmes. Report of the UN Chernobyl Forum Expert Group; World Health Organization: Geneva, Switzerland, 2006; pp. 69–97. ISBN 92-4-159417-9. [Google Scholar]
- Kahan, D.M.; Braman, D.; Gastil, J.; Slovic, P.; Mertz, C.K. Culture and identity-protective cognition: Explaining the white-male effect in risk perception. J. Empir. Legal Stud. 2008, 5, 645. [Google Scholar] [CrossRef]
- Slovic, P. Perception of risk. Science 1987, 236, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Orita, M.; Hayashida, N.; Urata, H.; Shinkawa, T.; Endo, Y.; Takamura, N. Determinants of the return to hometowns after the accident at Fukushima Dai-Ichi Nuclear Power Plant: A case study for the village of Kawauchi. Radiat. Prot. Dosim. 2013, 156, 383–385. [Google Scholar] [CrossRef] [PubMed]
- Orita, M.; Hayashida, N.; Nakayama, Y.; Shinkawa, T.; Urata, H.; Fukushima, Y.; Endo, Y.; Yamashita, S.; Takamura, N. Bipolarization of risk perception about the health effects of radiation in residents after the accident at Fukushima Nuclear Power Plant. PLoS ONE 2015, 10, e0129227. [Google Scholar] [CrossRef] [PubMed]
- Takeda, S.; Orita, M.; Fukushima, Y.; Kudo, T.; Takamura, N. Determinants of intention to leave among non-medical employees after a nuclear disaster: A cross-sectional study. BMJ Open 2016, 6, e011930. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, M.; Sutterlin, B. Human and nature-caused hazards: The affect heuristic causes biased decisions. Risk Anal. 2014, 34, 1482–1494. [Google Scholar] [CrossRef] [PubMed]
- Page, L.A.; Petrie, K.J.; Wessely, S.C. Psychosocial responses to environmental incidents: A review and a proposed typology. J. Psychosom. Res. 2006, 60, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Petrie, K.J.; Sivertsen, B.; Hysing, M.; Broadbent, E.; Moss-Morris, R.; Eriksen, H.R.; Ursin, H. Thoroughly modern worries: The relationship of worries about modernity to reported symptoms, health and medical care utilization. J. Psychosom. Res. 2001, 51, 395–401. [Google Scholar] [CrossRef]
- MacGregor, D.G.; Fleming, R. Risk perception and symptom reporting. Risk Anal. 1996, 16, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M.; Nakatani, J.; Oki, T. Evaluation of risk perception and risk-comparison information regarding dietary radionuclides after the 2011 Fukushima Nuclear Power Plant accident. PLoS ONE 2016, 11, e0165594. [Google Scholar] [CrossRef] [PubMed]
- Miura, I.; Nagai, M.; Maeda, M.; Harigane, M.; Fujii, S.; Oe, M.; Yage, H.; Suzuki, Y.; Takahashi, H.; Ohira, T.; et al. Perception of radiation risk as a predictor of mid-term mental health after a nuclear disaster: The Fukushima Health Management Survey. Int J. Environ. Res. Public Health 2017, 14, 1067. [Google Scholar] [CrossRef] [PubMed]
- Oe, M.; Takahashi, H.; Maeda, M.; Harigane, M.; Fujii, S.; Miura, I.; Nagai, M.; Yabe, H.; Ohira, T.; Suzuki, Y.; et al. Changes of posttraumatic stress responses in evacuated residents and their related factors. Asia Pac. J. Public Health 2017, 29, 182S–192S. [Google Scholar] [CrossRef] [PubMed]
- Lima, M.L. On the influence of risk perception on mental health: Living near an incinerator. J. Environ. Psychol. 2004, 24, 71–84. [Google Scholar] [CrossRef]
- Yasumura, S.; Hosoya, M.; Yamashita, S.; Kamiya, K.; Abe, M.; Akashi, M.; Kodama, K.; Ozasa, K.; Fukushima Health Management Survey Group. Study protocol for the Fukushima Health Management Survey. J. Epidemiol. 2012, 22, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Lindell, M.K.; Barnes, V.E. Protective response to technological emergency: Risk perception and behavioral intention. Nucl. Saf. 1986, 27, 457–467. [Google Scholar] [CrossRef]
- Weathers, F.W.; Litz, B.T.; Herman, D.S.; Hushka, J.A.; Keane, T.M. The PTSD Checklist (PCL), Reliability, Validity, and Diagnostic Utility; The Annual Meeting of International Society for Traumatic Stress Studies: San Antonio, TX, USA, 1993. [Google Scholar]
- Iwasa, H.; Suzuki, Y.; Shiga, T.; Maeda, M.; Yabe, H.; Yasumura, S. Psychometric evaluation of the Japanese version of the posttraumatic stress disorder checklist in community dwellers following the Fukushima Daiichi Nuclear Power Plant incident-The Fukushima Health Management Survey. SAGE Open 2016, 6, 1–11. [Google Scholar] [CrossRef]
- McDonald, S.D.; Calhoun, P.S. The diagnostic accuracy of the PTSD checklist: A critical review. Clin. Psychol. Rev. 2010, 30, 976–987. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Yabe, H.; Horikoshi, N.; Yasumura, S.; Kawakami, N.; Ohtsuru, A.; Mashiko, H.; Maeda, M. Mental health group of the Fukushima Health Management Survey. Diagnostic accuracy of Japanese posttraumatic stress measures after a complex disaster: The Fukushima Health Management Survey. Asia Pac. Psychiatry 2017, 9, e12248. [Google Scholar] [CrossRef]
- Sexual and Reproductive Health. Infertility Definitions and Terminology. Available online: http://www.who.int/reproductivehealth/topics/infertility/definitions/en/ (accessed on 9 March 2018).
- Genolini, C.; Alacoque, X.; Sentenac, M.; Arnaud, C. kml and kml3d: R packages to cluster longitudinal data. J. Stat. Softw. 2015, 65, 1–34. [Google Scholar] [CrossRef]
- Fox, J.; Weisberg, S. An R Companion to Applied Regression, 2nd ed.; Sage: Thousand Oaks, CA, USA, 2011; ISBN 978-1412975148. [Google Scholar]
- Peters, E.M.; Burraston, B.; Mertz, C.K. An emotion-based model of risk perception and stigma susceptibility: Cognitive appraisals of emotion, affective reactivity, worldviews, and risk perceptions in the generation of technological stigma. Risk Anal. 2004, 24, 1349–1367. [Google Scholar] [CrossRef] [PubMed]
- Rehani, M.M. Radiation effects and risks: Overview and a new risk perception index. Radiat. Prot. Dosim. 2015, 165, 7–9. [Google Scholar] [CrossRef] [PubMed]
- Kanda, R.; Tsuji, S.; Yonehara, H. Perceived risk of nuclear power and other risks during the last 25 years in Japan. Health Phys. 2012, 102, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Fukushima Revitalization Station. Available online: http://www.pref.fukushima.lg.jp/site/portal-english/ (accessed on 9 March 2018).
- National Institute for Health and Clinical Excellence. Post-Traumatic Stress Disorder: The Management of PTSD in Adults and Children in Primary and Secondary Care; National Collaborating Centre for Mental Health (UK); Gaskell: Leicester, UK, 2005. [Google Scholar]
- Murakami, M.; Sato, A.; Matsui, S.; Goto, A.; Kumagai, A.; Tsubokura, M.; Orita, M.; Takamura, N.; Kuroda, Y.; Ochi, S. Communicating with residents about risks following the Fukushima nuclear accident. Asia Pac. J. Public Health 2017, 29, 74S–89S. [Google Scholar] [CrossRef] [PubMed]
- Vyncke, B.; Perko, T.; Van Gorp, B. Information sources as explanatory variables for the Belgian health-related risk perception of the Fukushima nuclear accident. Risk Anal. 2017, 37, 570–582. [Google Scholar] [CrossRef] [PubMed]
- Turcanu, C.O.; El Jammal, M.H.; Perko, T.; Baumont, G.; Latre, E.; Choffel de Witte, I. Satisfaction with information about ionising radiation: A comparative study in Belgium and France. J. Radiol. Prot. 2016, 36, S122–S1242. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Delayed Effect | Genetic Effect | |||||||
|---|---|---|---|---|---|---|---|---|
| Traumatic reaction (ref: 17–49 on PCL-S) | ||||||||
| FY2011 | OR | 95% CI | OR | 95% CI | ||||
| ≥50 | 2.05 | 1.82 | 2.31 | 2.18 | 1.92 | 2.48 | ||
| FY2012 | ||||||||
| ≥50 | 1.86 | 1.61 | 2.15 | 2.05 | 1.75 | 2.40 | ||
| FY2013 | ||||||||
| ≥50 | 1.88 | 1.62 | 2.17 | 1.82 | 1.55 | 2.15 | ||
| Basic characteristics (FY2011) | ||||||||
| Gender (ref: Men) | ||||||||
| Women | 1.27 | 1.18 | 1.36 | 1.30 | 1.22 | 1.40 | ||
| Age (Ref: 50–64) | ||||||||
| 15–49 | 1.52 | 1.40 | 1.65 | 1.12 | 1.03 | 1.21 | ||
| ≥65 | 0.97 | 0.88 | 1.06 | 1.08 | 0.99 | 1.18 | ||
| Education (ref: High school) | ||||||||
| Junior high school | 1.11 | 1.00 | 1.23 | 1.11 | 1.01 | 1.23 | ||
| College or higher | 0.88 | 0.81 | 0.95 | 0.82 | 0.76 | 0.89 | ||
| Exposure to the disaster (FY2011) | ||||||||
| Tsunami (ref: No) | ||||||||
| Yes | 0.99 | 0.91 | 1.08 | 1.03 | 0.95 | 1.12 | ||
| NPP accident (ref: No) | ||||||||
| Yes | 1.30 | 1.21 | 1.40 | 1.35 | 1.26 | 1.45 | ||
| Bereavement (ref: No) | ||||||||
| Yes | 1.26 | 1.16 | 1.37 | 1.24 | 1.14 | 1.35 | ||
| Secondary stressors (FY2013) | ||||||||
| Living in other prefecture (ref: No) | ||||||||
| Yes | 1.03 | 0.94 | 1.13 | 0.92 | 0.84 | 1.01 | ||
| Family separation (ref: No) | ||||||||
| FY2012 or FY2013 | 1.21 | 1.08 | 1.35 | 1.21 | 1.08 | 1.36 | ||
| FY2012 & FY2013 | 1.11 | 1.03 | 1.20 | 1.16 | 1.08 | 1.26 | ||
| Number of relocations (ref: 0–2) | ||||||||
| 3–4 | 1.07 | 0.98 | 1.17 | 1.08 | 0.99 | 1.17 | ||
| ≥5 | 1.19 | 1.09 | 1.30 | 1.20 | 1.10 | 1.31 | ||
| Living circumstances | ||||||||
| (ref: well off/relatively well-off/normal) | ||||||||
| Poor/relatively poor | 1.85 | 1.72 | 1.98 | 1.84 | 1.71 | 1.97 | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, Y.; Takebayashi, Y.; Yasumura, S.; Murakami, M.; Harigane, M.; Yabe, H.; Ohira, T.; Ohtsuru, A.; Nakajima, S.; Maeda, M. Changes in Risk Perception of the Health Effects of Radiation and Mental Health Status: The Fukushima Health Management Survey. Int. J. Environ. Res. Public Health 2018, 15, 1219. https://doi.org/10.3390/ijerph15061219
Suzuki Y, Takebayashi Y, Yasumura S, Murakami M, Harigane M, Yabe H, Ohira T, Ohtsuru A, Nakajima S, Maeda M. Changes in Risk Perception of the Health Effects of Radiation and Mental Health Status: The Fukushima Health Management Survey. International Journal of Environmental Research and Public Health. 2018; 15(6):1219. https://doi.org/10.3390/ijerph15061219
Chicago/Turabian StyleSuzuki, Yuriko, Yoshitake Takebayashi, Seiji Yasumura, Michio Murakami, Mayumi Harigane, Hirooki Yabe, Tetsuya Ohira, Akira Ohtsuru, Satomi Nakajima, and Masaharu Maeda. 2018. "Changes in Risk Perception of the Health Effects of Radiation and Mental Health Status: The Fukushima Health Management Survey" International Journal of Environmental Research and Public Health 15, no. 6: 1219. https://doi.org/10.3390/ijerph15061219
APA StyleSuzuki, Y., Takebayashi, Y., Yasumura, S., Murakami, M., Harigane, M., Yabe, H., Ohira, T., Ohtsuru, A., Nakajima, S., & Maeda, M. (2018). Changes in Risk Perception of the Health Effects of Radiation and Mental Health Status: The Fukushima Health Management Survey. International Journal of Environmental Research and Public Health, 15(6), 1219. https://doi.org/10.3390/ijerph15061219