A US/Mexico Study of Joint Associations of Physical Activity and Sedentary Behavior on Anthropometric Indicators, Migration Status, Country of Birth and Country of Residence

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Characteristics of the Population Study
2.1.1. National Health and Nutrition Examination Survey
2.1.2. National Health and Nutrition Examination Survey from Mexico
2.2. Measurement
2.2.1. Anthropometrics Measurements
2.2.2. Physical Activity Levels and Sedentary Behavior
2.2.3. Categories of Physical Activity and Sedentary Behavior
2.2.4. Measurement of Migration Status, Country of Birth and Country of Residence
2.2.5. Covariates
2.3. Statistical Analyses
3. Results
3.1. Sociodemographic Characteristics and Categories of Physical Activity and Sedentary Behavior
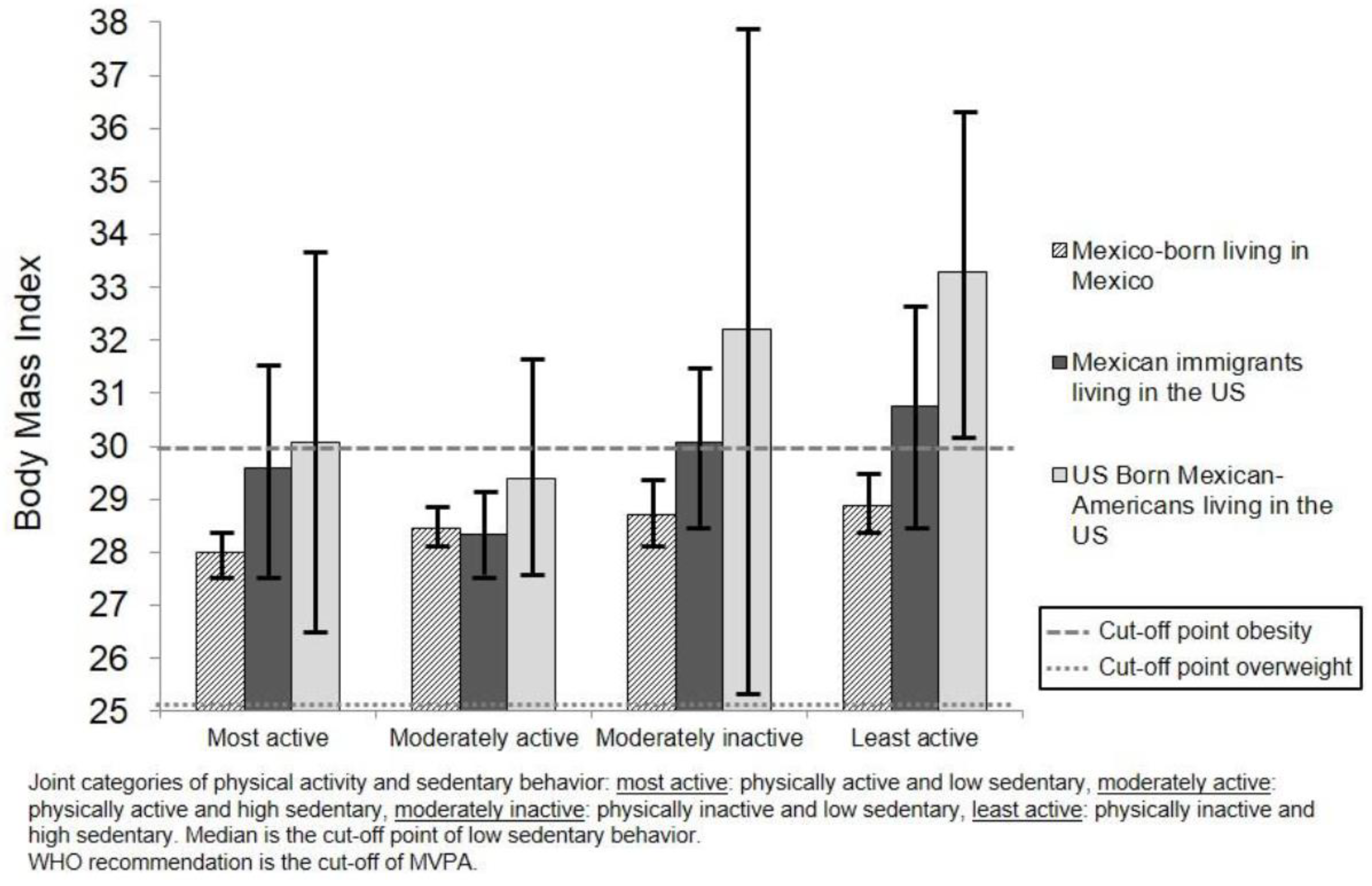
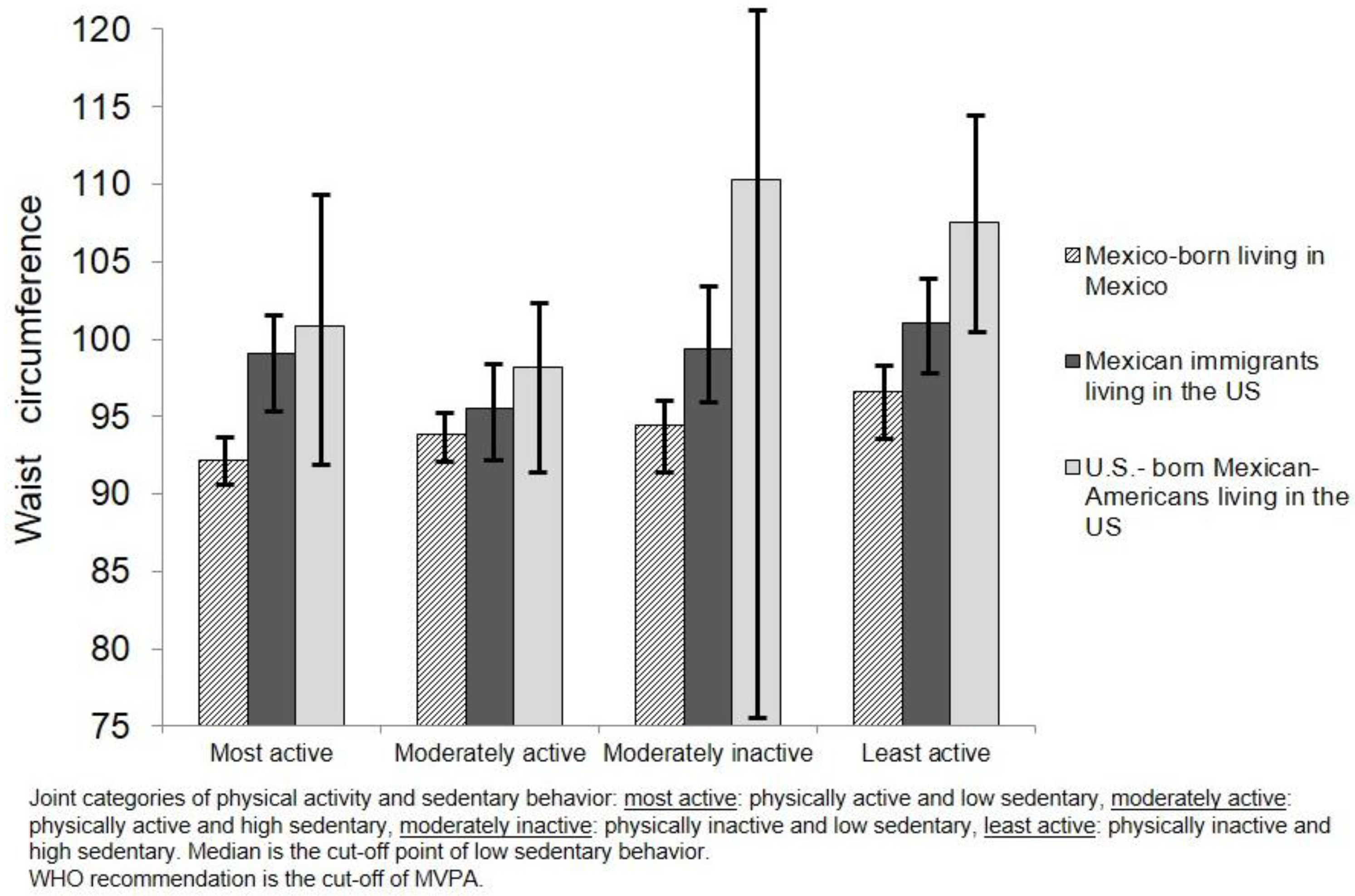
3.2. Associations between Categories of Physical Activity and Sedentary Behavior on BMI and Waist Circumference by Migration Status, Country of Birth and Country of Residence
4. Discussion
Limitations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Hunt, L.M.; Schneider, S.; Comer, B. Should “acculturation” be a variable in health research? A critical review of research on U.S. Hispanics. Soc. Sci. Med. 2004, 5, 973–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, J.W. Immigration, Acculturation, and Adaptation. Appl. Psychol. 1997, 46, 5–34. [Google Scholar] [CrossRef]
- Park, Y.; Neckerman, K.; Quinn, J.; Weiss, C.; Jacobson, J.; Rundle, A. Neighborhood immigrant acculturation and diet among Hispanic female residents of New York City. Public Health Nutr. 2011, 14, 1593–1600. [Google Scholar] [CrossRef] [PubMed]
- Abraido-Lanza, A.F.; Echeverria, S.E.; Florez, K.R. Latino immigrants, acculturation, and health: Promising new direction in research. Annu. Rev. Pub. Health 2016, 37, 219–236. [Google Scholar] [CrossRef] [PubMed]
- Lauderdale, D.S.; Rathouz, P.J. Body mass index in a U.S. national sample of Asian Americans: Effects of nativity, years since immigration and socioeconomic status. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- Wen, M.; Kowaleski-Jones, L.; Fan, J.X. Ethnic-immigrant disparities in total and abdominal obesity in the U.S. Am. J. Health Behav. 2013, 37, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Rtveladze, K.; Marsh, T.; Barquera, S.; Sanchez Romero, L.M.; Levy, D.; Melendez, G. Obesity prevalence in Mexico: Impact on health and economic burden. Public Health Nutr. 2014, 17, 233–239. [Google Scholar] [CrossRef] [PubMed]
- OECD/EU. Obesity Update 2017, OECD Publishing, Paris, 2017. Available online: http://www.oecd.org/els/health-systems/Obesity-Update-2017.pdf (accessed on 17 May 2018).
- National Center for Health Statistics. Health, United States, 2016: With Chartbook on Long-term Trends in Health. Hyattsville, MD. 2017. Available online: https://www.cdc.gov/nchs/data/hus/hus16.pdf#058 (accessed on 18 May 2018).
- Albretch, S.S.; Diez Roux, A.V.; Aiello, A.E.; Schulz, A.J.; Abraido-Lanza, A.F. Secular trends in the association between nativity/length of U.S. residence with body mass index, and waist circumference among Mexican-Americans, 1998–2008. Int. J. Public Health 2013, 58, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Delavari, M.; Sønderlund, A.L.; Swinburn, B.; Mellor, D.; Renzaho, A. Acculturation and obesity among migrant populations in high income countries –A systematic review. BMC Public Health 2013, 13, 458. [Google Scholar] [CrossRef] [PubMed]
- Block, J.P.; He, Y.; Zaslavsky, A.M.; Ding, L.; Ayanian, J.Z. Psychosocial stress and change in weight among U.S. adults. Am. J. Epidemiol. 2009, 170, 181–192. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R.; Jastreboff, A.M. Stress as a common risk factor for obesity and addiction. Biol. Psychiatry 2013, 73, 827–835. [Google Scholar] [CrossRef] [PubMed]
- Pampel, F.C.; Denney, J.T.; Krueger, P.M. Obesity, SES, and economic development: A test of the reversal hypothesis. Soc. Sci. Med. 2012, 74, 1073–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, M.; Robertson, W.; Oyebode, O. Obesity in International Populations. Curr. Obes. Rep. 2017, 6, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, J.R.; Johnson, C.M.; Dean, W.R. Nativity is associated with sugar-sweetened beverage and fast-food meal consumption among Mexican-origin women in Texas border colonias. Nutr. J. 2011, 10, 101. [Google Scholar] [CrossRef] [PubMed]
- Batis, C.; Hernández-Barrera, L.; Barquera, S.; Rivera, J.A.; Popkin, B.M. Food acculturation drives dietary differences among Mexicans, Mexican Americans, and non-Hispanic whites. J. Nutr. 2011, 141, 1898–1906. [Google Scholar] [CrossRef] [PubMed]
- Langellier, B.A.; Brookmeyer, R.; Wang, M.C.; Glik, D. Language use affects food behaviors and food values among Mexican-origin adults in the U.S.A. Public Health Nutr. 2015, 18, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Murillo, R.; Albrecht, S.S.; Daviglus, M.L.; Kershaw, K.N. The role of physical activity and sedentary behaviors in explaining the association between acculturation and obesity among Mexican-American adults. Am. J. Health Promot. 2015, 30, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet. 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Pew Research Center. Available online: http://www.pewhispanic.org/2015/05/12/statistical-portrait-of-hispanics-in-the-united-states-2013-key-charts (accessed on 1 May 2017).
- Dunton, G.F.; Berrigan, D.; Ballard-Barbash, R.; Graubard, B.; Atienza, A.A. Joint associations of physical activity and sedentary bahaviors with body mass index: Results from a time survey of U.S. adults. Int. J. Obes. 2009, 33, 1427–1436. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Healy, G.N.; Dunstan, D.W.; Salmon, J.; Owen, N. Joint associations of multiple leisure-time sedentary behaviours and physical activity with obesity in Australian adults. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunstan, D.W.; Salmon, J.; Owen, N.; Armstrong, T.; Zimmet, P.Z.; Welborn, T.A. Associations of TV viewing and physical activitywith the metabolic syndrome in Australian adults. Diabetologia 2005, 48, 2254–2261. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Television time and continuous metabolic risk in physically active adults. Med. Sci. Sports Exer. 2008, 40, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Dunstan, D.W.; Thorp, A.A.; Healy, G.N. Prolonged sitting: Is it a distinct coronary heart disease risk factor? Curr. Opin. Cardiol. 2011, 26, 412–419. [Google Scholar] [CrossRef] [PubMed]
- van der Ploeg, H.P.; Chey, T.; Korda, R.J.; Banks, E.; Bauman, A. Sitting time and all-cause mortality risk in 222 497 Australian adults. Arch. Intern. Med. 2012, 172, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S. Standardized use of the terms ‘‘sedentary’’ and ‘‘sedentary behaviours’’. Appl. Physiol. Nutr. Metab. 2012, 37, 540–542. [Google Scholar]
- Maher, C.; Olds, T.; Mire, E.; Katzmarzyk, P.T. Reconsidering the sedentary behavior paradigm. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Matthews, C.E.; Dunstan, D.W.; Winkler, E.A.H.; Owen, N. Sedentary time and cardio-metabolic biomarkers in U.S. adults: NHANES 2003–2006. Eur. Heart J. 2011, 32, 590–597. [Google Scholar]
- Henson, J.; Yates, T.; Biddle, S.J.; Edwarson, C.L.; Khunti, K.; Wilmot, E.G. Associations of objectively measured sedentary time and physical activity with markers of cardiometabolic health. Diabetologia 2013, 56, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Stamatakis, E.; Hammer, M.; Tilling, K.; Lawlor, D.A. Sedentary time in relation to cardio-metabolic risk factors: Differential associations for self-report vs. accelerometry in working age adults. Int. J. Epidemiol. 2012, 41, 1328–1337. [Google Scholar] [CrossRef] [PubMed]
- Bakrania, K.; Edwardson, C.L.; Bodicoat, D.H.; Esliger, D.W.; Gill, J.M.; Kazi, A. Associations of mutually exclusive categories of physical activity and sedentary time with markers of cardio-metabolic health in English adults: A cross-sectional analysis of the Health Survey for England. BMC Public Health 2016, 12, 16–25. [Google Scholar]
- Centers for Disease Control and Prevention. National Health and Nutrition Survey. Available online: http//:www.cdc.gov/nchs/nhanes/nhanes2011–2012 (accessed on 20 August 2016).
- Johnson, C.L.; Dohrmann, S.M.; Burt, V.L.; Mohadjer, L.K. National Health and Nutrition Examination Survey: Sample design, 2011–2014. National Center for Health Statistics. Vital Health Stat. 2014, 2, 162. [Google Scholar]
- Romero-Martínez, M. Metodología. In Encuesta Nacional de Salud y Nutrición 2012, Resultados Nacionales; Gutiérrez, J.P., Rivera-Dommarco, J., Shamah-Levy, T., Villalpando-Hernández, S., Franco, A., Cuevas-Nasu, L., Eds.; Instituto Nacional de Salud Pública: México, México, 2012; pp. 19–27, ICBN:24626712. [Google Scholar]
- National Health and Nutrition Examination Survey (NHANES) 2011. Anthropometry Procedures Manual. Available online: www.cdc.gov/nchs/data/nhanes/nhanes _11_12/Anthropometry_Procedures_Manual.pdf (accessed on 6 June 2017).
- Habicht, J. Standardization of anthropometric methods in the field. PAHO Bull 1974, 76, 375–384. [Google Scholar]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics: Champaign, IL, USA, 1988; ISBN 9780873221214. [Google Scholar]
- World Health Organization. Global Physical Activity Questionnaire (GPAQ). Analysis Guide. Geneva. Switzerland: World Health Organization. 2001. Available online: http//:www.cdc.gov/nchs/nhanes/nhanes2011–2012 (accessed on 16 November 2015).
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E. International physical activity questionnaire: 12 Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, S.D.; Heumann, K.J.; Der Ananian, C.A.; Ainsworth, B.E. Validity and reliability of the Global Physical Activity Questionnaire (GPAQ). Meas. Phys. Educ. Exerc. Sci. 2013, 17, 221–225. [Google Scholar] [CrossRef]
- Medina, C.; Barquera, S.; Janssen, I. Validity and reliability of the International Physical Activity Questionnaire among adults in Mexico. Rev. Panam. Salud. Publica. 2013, 34, 21–28. [Google Scholar] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health. 2011. Available online: http://www.who.int/rpc/guidelines/9789241599979/en/ (accessed on 5 June 2016).
- Tremblay, M.S.; LeBlanc, A.G.; Kho, M.E.; Saunders, T.J.; Larouche, R.; Colley, R.C. Systematic review of sedentary behavior and health indicators in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 98. [Google Scholar] [CrossRef] [PubMed]
- Berrigan, D.; Dodd, K.; Troiano, R.P.; Reeve, B.B.; Ballard-Barbash, R. Physical activity and acculturation among adults Hispanics in the United States. Res. Q. Exerc. Sport. 2006, 77, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Larsen, B.A.; Noble, M.L.; Murray, K.E.; Marcus, B.H. Physical activity in Latino men and women: Facilitators, barriers, and interventions. Am. J. Lifestyle Med. 2015, 9, 4–30. [Google Scholar] [CrossRef]
- Crespo, C.J.; Smit, E.; Carter-Pokras, O.; Andersen, R. Acculturation and leisure-time physical activity in Mexican-American adults: Results from NHANES III, 1988–1994. Am. J. Public Health 2001, 91, 1254–1257. [Google Scholar] [CrossRef] [PubMed]
- Loprinzi, P.D. Joint associations of objectively-measured sedentary behavior and physical activity with health-related quality of life. Prev. Med. Rep. 2015, 14, 959–961. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.; Palarea-Albaladejo, J.; Dontje, M.L.; Skelton, D.A. Combined effects of time spent in physical activity, sedentary behaviors and sleep on obesity and cardio-metabolic health markers: A novel compositional data analysis approach. PLoS One 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Troiano, R.P.; Berrigan, D.; Dood, K.W.; Masse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States Measured by Accelerometer. Med. Sci. Sports. Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Norman, P.; Boyle, P.; Rees, P. Selective migration, health and deprivation: A longitudinal analysis. Soc. Sci. Med. 2005, 60, 2755–2771. [Google Scholar] [CrossRef] [PubMed]
- Ruvalcaba, L.N.; Teruel, G.M.; Thomas, D.; Goldman, N. The healthy migrant effect: New findings from the Mexican Family Life Survey. Am. J. Public Health 2008, 1, 78–84. [Google Scholar]
- Castañeda, H.; Holmes, S.M.; Madrigal, D.S.; Young, M.E.; Beyeler, N.; Quesada, J. Immigration as a social determinant of health. Annu. Rev. Public Health 2015, 18, 375–392. [Google Scholar] [CrossRef] [PubMed]
- Cantero, P.J.; Richardson, J.L.; Baezconde-Garbanati, L.; Marks, G. The association between acculturation and health practices among middle-aged and elderly Latinas. Ethn. Dis. 1999, 9, 166–180. [Google Scholar] [PubMed]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Connor Gorber, S.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2008, 5. [Google Scholar] [CrossRef] [PubMed]
- Hacker, K.; Anies, M.; Folb, B.L.; Zallman, L. Barriers to healthcare for undocumented immigrants: A literature review. Risk Manag. Healthc. Policy 2015, 8, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Fernández, A.; Rodriguez, R.A. Undocumented Immigrants and Access to Health Care. JAMA Intern. Med. 2017, 177, 536–537. [Google Scholar] [CrossRef] [PubMed]
- Stimpson, J.P.; Wilson, F.A.; Zallman, L. ED visits and spending by unauthorized immigrants compared with legal immigrants and U.S. natives. Am. J. Emerg. Med. 2014, 32, 679–680. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Mexico-Born Living in Mexico | Mexican Immigrants Living in the US | US-Born Mexican-Americans Living in the US | Mexico-Born Living in Mexico | Mexican Immigrants Living in the US | US-Born Mexican-Americans Living in the US |
|---|---|---|---|---|---|---|
| Most active | Moderately active | |||||
| (N = 21,272,889) (n = 3944) | (N = 2,104,861) (n = 67) | (N = 889,926) (n = 26) | (N = 26,469,663) (n = 4127) | (N = 2,919,679) (n = 88) | (N = 3,399,165) (n = 91) | |
| % (C.I. 95%) | % (C.I. 95%) | % (C.I. 95%) | % (C.I. 95%) | % (C.I. 95%) | % (C.I. 95%) | |
| Age (in years) * | 41.3 (40.4, 42.1) | 39 (35, 43) | 39.6 (32.5, 46.6) | 38.5 (37.7, 39.4) | 39.4 (36.3, 42.6) | 34.3 (31.9, 36.7) |
| Sex % (95% C.I.) | ||||||
| Male | 41.5 (38.6, 44.4) | 53.9 (38.6, 69.1) | 66.7 (38.2, 95.3) | 49.4 (46.6, 52.2) | 62.9 (49.7, 76.1) | 53.9 (42.4, 65.4) |
| Female | 58.4 (55.5, 61.3) | 46.1 (30.8, 61.4) | 33.2 (4.7, 61.8) | 50.5 (47.7, 53.3) | 37.1 (23.9, 50.2) | 46.1 (34.6, 57.6) |
| Education level % (95% C.I.) | ||||||
| Less than high school | 83.8 (81.6, 86) | 67.9 (46.9, 88.8) | 35.2 (−6.01, 76.5) | 63.8 (60.7, 66.9) | 55.8 (43.2, 68.4) | 19.1 (12.4, 25.8) |
| High school graduate and more | 16.2 (13.9, 18.3) | 32.1 (11.1, 53) | 64.7 (23.49, 106) | 36.1 (33.1, 39.2) | 44.2 (31.5, 56.7) | 80.1 (74.2, 87.6) |
| Occupation % (95% C.I.) | ||||||
| Employment | 53.1 (50.1, 56.1) | 75.6 (61.6, 98.7) | 64.5 (32.8, 96.2) | 57.4 (54.3, 60.5) | 76.4 (64.2, 83) | 70.7 (60.4, 80.9) |
| Unemployment | 46.8 (43.8, 49.8) | 24.3 (10.2, 38.4) | 35.5 (3.8, 67.2) | 42.6 (39.5, 45.7) | 26.4 (16.9, 35.7) | 29.3 (19.1, 39.6) |
| Health risk conditions % (95% C.I.) | ||||||
| Diabetes | 8.4 (6.6, 10) | 10.3 (0.001, 20.7) | 13.7 (−0.72, 28.2) | 7.4 (6, 8.8) | 7.9 (8.5, 15.1) | 3.5 (−2.2, 9.3) |
| High blood pressure | 14.7 (12.7, 16.8) | 15.2 (3.9, 26.4) | 36.1 (−1.2, 73.4) | 13.6 (11.6, 15.7) | 13.9 (6.3, 21.5) | 21.8 (10.6, 33.1) |
| High cholesterol | 12.7 (10.5, 14.8) | 19 (7.6, 30.3) | 29.2 (9.3, 49.2) | 13.7 (11.8, 15.7) | 20 (12.4, 27.6) | 18.7 (7.4, 29.9) |
| MVPA (minutes/day) * | 159.4 (153.2, 165.5) | 196.8 (136.1, 257.5) | 190.3 (105.2, 275.3) | 147.1 (140.8, 153.5) | 178.4 (133.2, 223.5) | 152.7 (121, 184.5) |
| Sedentary time (minutes/day) * | 117.3 (114.3, 120.3) | 84.5 (70.5, 98.5) | 96.2 (77.2, 115.3) | 378.8 (368.6, 389) | 268. (1 (239.4, 296.9) | 355 (300.2, 411.4) |
| Moderately inactive | Least active | |||||
| (N = 3,410,936) (n = 707) | (N = 1,220,304) (n = 39) | (N = 278,715) (n = 11) | (N = 5,684,364) (n = 924) | (N = 2,475,596) (n = 81) | (N = 1,505,528) (n = 46) | |
| Age (in years) * | 41.5 (40, 42.9) | 40.9 (36.2, 45.6) | 47.3 ( −11.9, 106.5) | 40.1 (38.5, 41.7) | 40.3 (38.1, 42.5) | 37.6 (32.5, 42.6) |
| Sex % (95% C.I.) | ||||||
| Male | 33.5 (27.3, 39.6) | 38.4 (16.3, 60.5) | 31.4 (−1.5, 2.1) | 50.1 (44, 56.2) | 48.2 (31.7, 64.7) | 34.2 (22.4, 46) |
| Female | 66.4 (60.3, 72.6) | 61.5 (39.5, 83.7) | 68.6 (−1.1, 2.5) | 49.8 (43.7, 55.9) | 51.8 (35.3, 68.3) | 65.8 (53.9, 77.6) |
| Education level % (95% C.I.) | ||||||
| Less than high school | 82.5 (77.8, 87.2) | 83.1 (66.7, 99.3) | 34.7 (−2.44, 3.14) | 61.7 (56.1, 67.3) | 65.6 (54.4, 76.9) | 31 (8.7, 53.3) |
| High school graduate and more | 17.4 (12.7, 22.1) | 16.9 (6.1, 33.2) | 65.2 (−2.14, 3.44) | 38.3 (32.7, 43.8) | 34.3 (23, 45.6) | 68.9 (46.6, 91.2) |
| Occupation % (95% C.I.) | ||||||
| Employment | 41.3 (35.4, 47.3) | 54 (32.7, 75.3) | 46.1 (−3.26, 4.19) | 60.2 (54.7, 65.7) | 63.3 (42.8, 83.8) | 70.1 (47.7, 92.5) |
| Unemployment | 58.6 (52.6, 64.6) | 45.9 (24.7, 67.2) | 53.9 (−3.19, 4.26) | 39.8 (34.2, 45.3) | 36.7 (16.2, 57.2) | 29.9 (7.5, 52.3) |
| Health risk conditions % (95% C.I.) | ||||||
| Diabetes | 10.6 (7, 14.3) | 11.8 (−0.9, 24.4) | 22.8 (−2.05, 2.51) | 13.7 (9.8, 17.6) | 10.4 (1.37, 19.37) | 9.4 (5.8, 13.1) |
| High blood pressure | 15.4 (11.6, 19.2) | 21.5 (4.8, 38.1) | 49.3 (−1.29, 2.27) | 15.5 (12.3, 18.8) | 18.7 (6.4, 31) | 22.8 (7.4, 38.2) |
| High cholesterol | 13.6 (9.5, 17.6) | 14.9 (2.1, 27.7) | 13.2 (−54.7, 81.2) | 13.5 (10.1, 16.9) | 25.4 (17.2, 33.6) | 20.7 (8.1, 33.3) |
| MVPA (minutes/ day) * | 8.2 (7.3, 9.1) | 3.8 (1.27, 6.4) | 7.3 (−27.6, 42.3) | 7.8 (7.1, 8.6) | 4.7 (3.1, 6.3) | 4.3 (1.1, 7.49) |
| Sedentary time (minutes/day) * | 107.3 (100.4, 114.2) | 87.7 (67.8, 107.6) | 81.7 (−99.8, 263.3) | 481.1 (437.6, 524.7) | 334 (284.8, 383.2) | 485.2 (386, 584.4) |
| Joint Categories of Physical Activity and Sedentary Behavior | Body Mass Index | Waist Circumference | ||||||
|---|---|---|---|---|---|---|---|---|
| Mexican Immigrants Living in the US | US-Born Mexican-Americans Living in the US | Mexican Immigrants Living in the US | US-Born Mexican-Americans Living in the US | |||||
| Non-adjusted ¥ | Adjusted § | Non-adjusted ¥ | Adjusted § | Non-adjusted ¥ | Adjusted § | Non-adjusted ¥ | Adjusted § | |
| β (95% C.I.) | β (95% C.I.) | β (95% C.I.) | β (95% C.I.) | β (95% C.I.) | β (95% C.I.) | β (95% C.I.) | β (95% C.I.) | |
| Most active | 1.32 (0.1, 2.7) * | 1.3 (0.02, 2.6) * | 1.5 (−0.5, 3.6) | 1.28 (−0.73, 3.3) | 6.85 (1.5, 12.1) ** | 4.54 (−0.5, 9.5) | 11.3 (2.9, 19.5) ** | 6.85 (−1.1, 14.7) |
| Moderately active | −0.54 (−1.7, 0.6) | −0.43(−1.5, 0.69) | 0.64 (−0.5, 1.8) | 0.88 (−0.2, 1.9) | 3.72 (−0.8, 8.3) | 0.8 (−3.5, 5.1) | 7.65 (3.2, 12.1) ** | 6.86 (2.6, 11.1) ** |
| Moderately inactive | 0.57 (−1.4, 2.5) | 0.02 (−1.8, 1.9) | 3.4 (0.05,6.8) | 3.1 (−0.1, 6.4) | 11 (1.35, 20.7) * | 5.76 (−3, 14.5) | 12.3 (−4.4, 29) | 5.3 (−10.1, 20.7) |
| Least active | 1.26 (−0.1, 2.7) | 1.01 (−0.4, 2.3) | 4.6 (2.8, 6.4) ** | 4.1 (2.4, 5.8) ** | 9.6 (3.2, 15.9) * | 5.6 (−0.3, 11.5) | 15.3 (7.6, 23.1) * | 14.4 (7.2, 21.7) * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallegos-Carrillo, K.; Belcher, B.R.; Dunton, G.F.; Samet, J.M.; Baezconde-Garbanati, L. A US/Mexico Study of Joint Associations of Physical Activity and Sedentary Behavior on Anthropometric Indicators, Migration Status, Country of Birth and Country of Residence. Int. J. Environ. Res. Public Health 2018, 15, 1283. https://doi.org/10.3390/ijerph15061283
Gallegos-Carrillo K, Belcher BR, Dunton GF, Samet JM, Baezconde-Garbanati L. A US/Mexico Study of Joint Associations of Physical Activity and Sedentary Behavior on Anthropometric Indicators, Migration Status, Country of Birth and Country of Residence. International Journal of Environmental Research and Public Health. 2018; 15(6):1283. https://doi.org/10.3390/ijerph15061283
Chicago/Turabian StyleGallegos-Carrillo, Katia, Britni R. Belcher, Genevieve F. Dunton, Jonathan M. Samet, and Lourdes Baezconde-Garbanati. 2018. "A US/Mexico Study of Joint Associations of Physical Activity and Sedentary Behavior on Anthropometric Indicators, Migration Status, Country of Birth and Country of Residence" International Journal of Environmental Research and Public Health 15, no. 6: 1283. https://doi.org/10.3390/ijerph15061283
APA StyleGallegos-Carrillo, K., Belcher, B. R., Dunton, G. F., Samet, J. M., & Baezconde-Garbanati, L. (2018). A US/Mexico Study of Joint Associations of Physical Activity and Sedentary Behavior on Anthropometric Indicators, Migration Status, Country of Birth and Country of Residence. International Journal of Environmental Research and Public Health, 15(6), 1283. https://doi.org/10.3390/ijerph15061283