A Cross-Sectional Study of Smoking Behaviors and Attitudes of Parents in Pediatric Primary Care Settings



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Settings
2.2. Procedures
2.3. Data Collection
2.4. Analyses
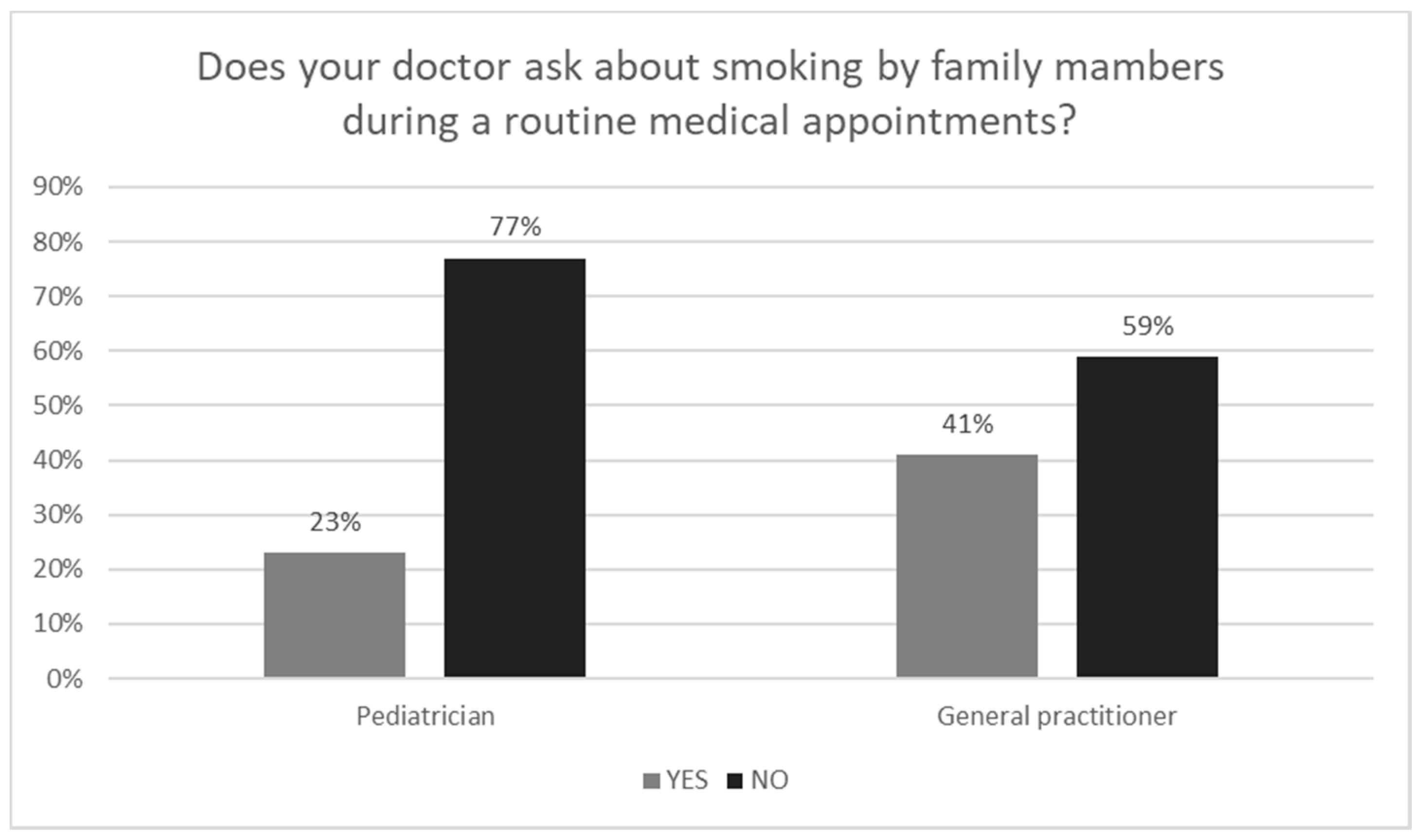
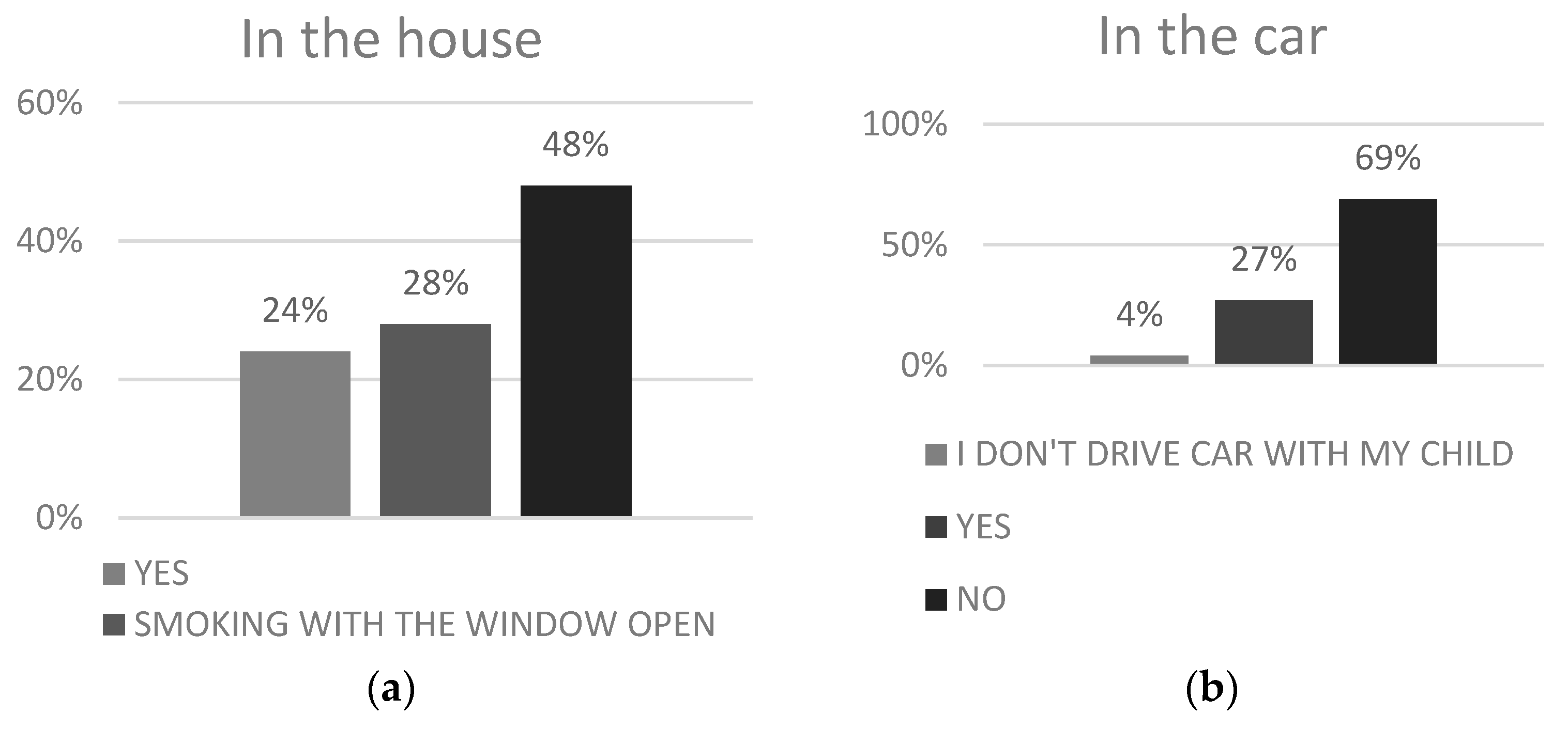
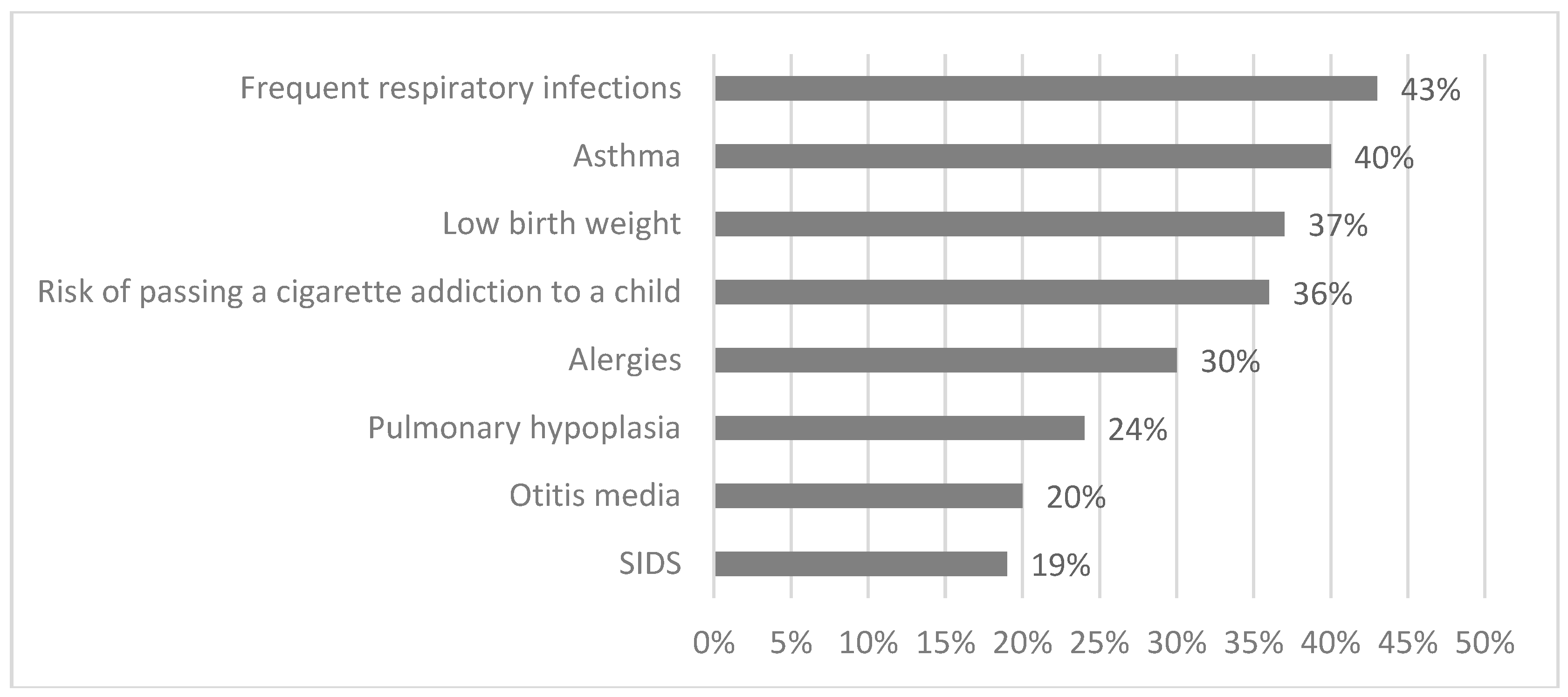
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
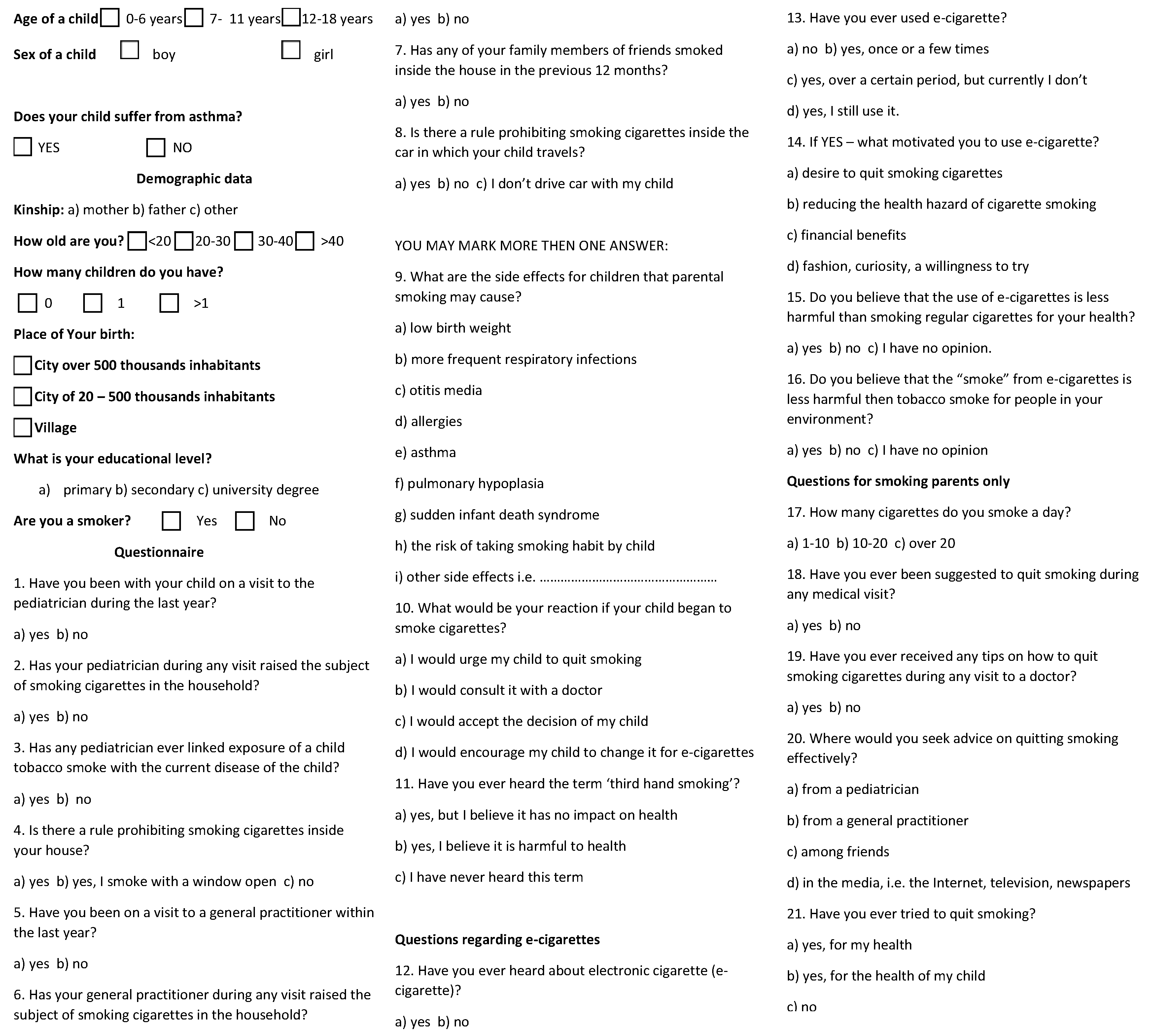
Appendix A

References
- Oberg, M.; Jaakkola, S.; Woodward, A.; Peruga, A.; Pruss-Ustun, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet 2011, 377, 139–146. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; Rockville, M.D., Ed.; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2006.
- World Health Organization. WHO Report Second-Hand Gender, Women, and the Tobacco Epidemic: 5. Second-Hand Smoke, Women, and Children; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Samet, J.M.; Yang, G. Passive Smoking, Women and Children. In Women and the Tobacco Epidemic. Challenges for the 21st Century; Samet, J.M., Yoon, S.Y., Eds.; WHO in Collaboration with the Institute for Global; Tobacco Control and the Johns Hopkins School of Public Health: Geneva, Switzerland, 2001; Available online: www.who.int/tobacco/media/en/WomenMonograph.pdf (accessed on 23 March 2011).
- Rodgman, A.; Perfetti, T.A. The Chemical Components of Tobacco and Tobacco Smoke; CRC Press, Taylor & Francis Group: Boca Raton, FL, USA, 2009; ISBN 9781466515482. [Google Scholar]
- U.S. Environmental Protection Agency. Respiratory health effects of Passive Smoking: Lung Cancer and Other Disorders; U.S. Environmental Protection Agency: Washington, DC, USA, 1992.
- Vitoria, P.D.; Machado, J.C.; Racara, S.B.; Araujo, A.C.; Samorinha, C.; Antunes, H.; Rosas, M.; Becona, E.; Precioso, J. Portuguese children’s exposure to second-hand tobacco smoke in the family car. Gac. Sanit. 2015, 29, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Feleszko, W.; Ruszczyński, M.; Jaworska, J.; Strzelak, A.; Zalewski, B.M.; Kulus, M. Environmental tobacco smoke exposure and risk of allergic sensitisation in children: A systematic review and meta-analysis. Arch. Dis. Child. 2014, 99, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Oberg, M.; Jaakkola, M.S.; Pruss-Ustun, A.; Schweizer, C.; Woodward, A. Second-Hand Smoke—Assessing the Burden of Disease at National and Local Levels; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Feleszko, W.; Rurarz, A.; Ratajczak, K. Pediatricians Do Not Ask Routinely About Parental Smoking Habits. Iran. J. Pediatr. 2017, 2, e9992. [Google Scholar] [CrossRef]
- Rosen, L.; Kostjukovsky, I. Parental Risk Perceptions of Child Exposure to Tobacco Smoke. BMC Public Health 2015, 15, 90. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics, Committee on Substance Abuse. Tobacco’s toll: Implications for the pediatrician. Pediatrics 2001, 107, 794–798. [Google Scholar]
- American Academy of Family Physicians. Summary of Policy Recommendations for Periodic Health Examination; American Academy of Family Physicians: Kansas City, MO, USA, 1998. [Google Scholar]
- Moss, D.; Cluss, P.A.; Mesiano, M.; Kip, K.E. Accessing adult smokers in the pediatric setting: What do parents think? Nicotine Tob. Res. 2006, 8, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Sharif, I.; Oruwariye, T.; Waldman, G.; Ozuah, P.O. Smoking cessation counseling by pediatricians in an inner-city setting. J. Natl. Med. Assoc. 2002, 94, 841. [Google Scholar] [PubMed]
- Glover, M.; Kira, A.; Johnston, V.; Walker, N.; Brown, N.; Thomas, D. Australian and New Zealand Indigenous mothers’ report respect for smoking bans in homes. Women Birth 2015, 28, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Moore, G.F. Prevalence of smoking restrictions and child exposure to secondhand smoke in cars and homes: A repeated crosssectional survey of children aged 10–11 years in Wales. BMJ Open 2015, 5, e006914. [Google Scholar] [CrossRef] [PubMed]
- Murphy-Hoefer, R.; Madden, P.; Maines, D.; Coles, C. Prevalence of smoke-free car and home rules in Maine before and after passage of a Smoke-Free Vehicle Law, 2007–2010. Prev. Chronic Dis. 2014, 11, 130132. [Google Scholar] [CrossRef] [PubMed]
- Claire, A.W.; Amato, M.S.; Boyle, R.G.; Rode, P.; Kinney, A.M. Secondhand Smoke Exposure 7 Years After an Indoor Smoke-Free Law. Am. J. Health Promot. 2016, 32, 131–134. [Google Scholar] [CrossRef] [PubMed]
- ASH Scotland. Secondhand Smoke in Cars; ASH Scotland: Edinburgh, UK, 2011. [Google Scholar]
- Soliman, S.; Pollack, H.; Warner, K. Decrease in the prevalence of environmental tobacco smoke exposure in the home during the 1990s in families with children. Am. J. Public Health 2004, 2, 314–320. [Google Scholar] [CrossRef]
- Hyland, A.; Higbee, C.; Hassan, L.; Fong, G.T.; Borland, R.; Cummings, K.M.; Hastings, G. Does smoke-free Ireland have more smoking inside the home and less in pubs than the United Kingdom? Findings from the international tobacco control policy evaluation project. Eur. J. Public Health 2008, 1, 63–65. [Google Scholar] [CrossRef] [PubMed]
- O’Dowd, A. Smoking ban in public places also cuts smoking at home. BMJ Clin. Res. Ed. 2005, 7509, 129. [Google Scholar] [CrossRef] [PubMed]
- Borland, R.; Mullins, R.; Trotter, L.; White, V. Trends in environmental tobacco smoke restrictions in the home in Victoria, Australia. Tob. Control 1999, 3, 266–271. [Google Scholar] [CrossRef]
- Action on Smoking and Health Research Report Secondhand Smoke: The Impact on Children. 2014. Available online: http://ash.org.uk/information-and-resources/secondhand-smoke/ash-research-report-secondhand-smoke/ (accessed on 28 March 2014).
- Daly, J.B.; Mackenzie, L.J.; Freund, M.; Wolfenden, L.; Roseby, R.; Wiggers, J.H. Interventions by Health Care Professionals Who Provide Routine Child Health Care to Reduce Tabacco Smoke Exposure in Children. A Review and Meta-analysis. JAMA Pediatr. 2016, 2, 138–147. [Google Scholar] [CrossRef] [PubMed]
- Wasowicz, A.; Feleszko, W.; Goniewicz, M.L. E-Cigarette use among children and young people: The need for regulation. Expert Rev. Respir. Med. 2015, 5, 507–509. [Google Scholar] [CrossRef] [PubMed]
- Protano, C.; Vitali, M. The New Danger of Thirdhand Smoke: Why Passive Smoking Does Not Stop at Secondhand Smoke. Environ. Health Perspect. 2011, 119, a422. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, G.; Simoni, M.; Cibella, F.; Ferrara, F.; Liotta, G.; Malizia, V.; Corsello, G.; Viegi, G.; La Grutta, S. Third-hand smoke exposure and health hazards in children. Monaldi Arch. Chest Dis. 2013, 79, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Caraballo, R.S.; Giovino, G.A.; Pechacek, T.F.; Mowery, P.D. Factors associated with discrepancies between self-reports on cigarette smoking and measured serum cotinine levels among persons aged 17 years or older: Third National Health and Nutrition Examination Survey, 1988–1994. Am. J. Epidemiol. 2001, 153, 807–814. [Google Scholar] [CrossRef] [PubMed]



© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ratajczak, A.; Ratajczak, K.; Feleszko, W. A Cross-Sectional Study of Smoking Behaviors and Attitudes of Parents in Pediatric Primary Care Settings. Int. J. Environ. Res. Public Health 2018, 15, 1384. https://doi.org/10.3390/ijerph15071384
Ratajczak A, Ratajczak K, Feleszko W. A Cross-Sectional Study of Smoking Behaviors and Attitudes of Parents in Pediatric Primary Care Settings. International Journal of Environmental Research and Public Health. 2018; 15(7):1384. https://doi.org/10.3390/ijerph15071384
Chicago/Turabian StyleRatajczak, Aleksandra, Karol Ratajczak, and Wojciech Feleszko. 2018. "A Cross-Sectional Study of Smoking Behaviors and Attitudes of Parents in Pediatric Primary Care Settings" International Journal of Environmental Research and Public Health 15, no. 7: 1384. https://doi.org/10.3390/ijerph15071384
APA StyleRatajczak, A., Ratajczak, K., & Feleszko, W. (2018). A Cross-Sectional Study of Smoking Behaviors and Attitudes of Parents in Pediatric Primary Care Settings. International Journal of Environmental Research and Public Health, 15(7), 1384. https://doi.org/10.3390/ijerph15071384