How Does Low Socioeconomic Status Increase Blood Lead Levels in Korean Children?

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
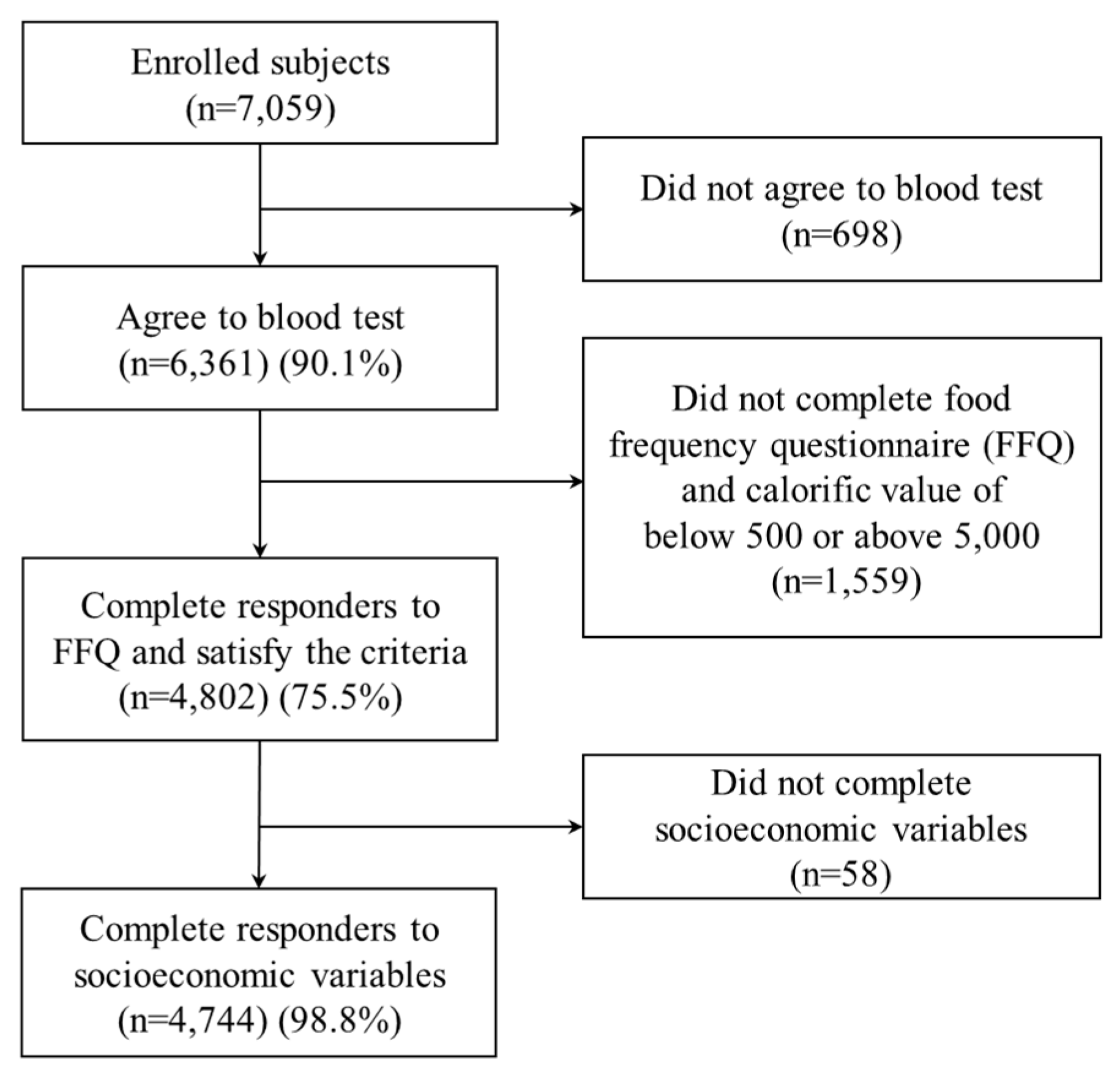
2.1. Data Collection and Processing
2.2. Measures
2.2.1. BLLs
2.2.2. SES
2.2.3. Lead in the Air and Total Length of Every Road within a 200-m Radius of the House
2.2.4. Agriculture and Playing outside on Weekdays
2.2.5. Dietary Assessment
2.3. Statistical Analyses
3. Results
3.1. Descriptive Statistics and Generalized Linear Models
3.2. Measurement Modeling
3.3. SEM: Blood Lead Exposure Pathways
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Flora, G.; Gupta, D.; Tiwari, A. Toxicity of Lead: A Review with Recent Updates. Interdiscip. Toxicol. 2012, 5, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Mason, L.H.; Harp, J.P.; Han, D.Y. Pb Neurotoxicity: Neuropsychological Effects of Lead Toxicity. Biomed. Res. Int. 2014, 2014, 840547. [Google Scholar] [CrossRef] [PubMed]
- Bello, O.; Naidu, R.; Rahman, M.M.; Liu, Y.; Dong, Z. Lead Concentration in the Blood of the General Population Living Near a Lead–Zinc Mine Site, Nigeria: Exposure Pathways. Sci. Total Environ. 2016, 542, 908–914. [Google Scholar] [CrossRef] [PubMed]
- White, P.D.; Van Leeuwen, P.; Davis, B.D.; Maddaloni, M.; Hogan, K.A.; Marcus, A.H.; Elias, R.W. The Conceptual Structure of the Integrated Exposure Uptake Biokinetic Model for Lead in Children. Environ. Health Perspect. 1998, 106 (Suppl. 6), 1513–1530. [Google Scholar] [CrossRef] [PubMed]
- Kolossa-Gehring, M.; Becker, K.; Conrad, A.; Lüdecke, A.; Riedel, S.; Seiwert, M.; Schulz, C.; Szewzyk, R. German Environmental Survey for Children (GerES IV)–first Results. Int. J. Hyg. Environ. Health 2007, 210, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Burm, E.; Song, I.; Ha, M.; Kim, Y.; Lee, K.J.; Kim, H.; Lim, S.; Kim, S.; Lee, C.; Kim, S.Y. Representative Levels of Blood Lead, Mercury, and Urinary Cadmium in Youth: Korean Environmental Health Survey in Children and Adolescents (KorEHS-C), 2012–2014. Int. J. Hyg. Environ. Health 2016, 219, 412–418. [Google Scholar] [CrossRef] [PubMed]
- CDC. Fourth National Report on Human Exposure to Environmental Chemicals, Updated Tables of National Health and Nutritional Examination Survey (NHANES) IV; CDC: Atlanta, GA, USA, 2015.
- Health Canada. Report on Human Biomonitoring of Environmental Chemicals in Canada, Results of the Canadian Health Measure Survey Cycle 1 (2007–2009); CHMS: Ottawa, ON, Canada, 2010.
- Zahran, S.; Laidlaw, M.A.; McElmurry, S.P.; Filippelli, G.M.; Taylor, M. Linking Source and Effect: Resuspended Soil Lead, Air Lead, and Children’s Blood Lead Levels in Detroit, Michigan. Environ. Sci. Technol. 2013, 47, 2839–2845. [Google Scholar] [CrossRef] [PubMed]
- Hwang, Y.; Chang, C.; Chao, K.; Hsiao, F.; Chang, H.; Han, H. Using Structural Equation Model to Explore Occupational Lead Exposure Pathways. Sci. Total Environ. 2002, 284, 95–108. [Google Scholar] [CrossRef]
- ATSDR. Toxicological Profile for Lead. Book Toxicological Profile for Lead City; US Department of Health and Human Services, Public Health Service, Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2007.
- Lanphear, B.P.; Roghmann, K.J. Pathways of Lead Exposure in Urban Children. Environ. Res. 1997, 74, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.S.; Kang, S.K.; Park, I.J.; Rhee, K.Y.; Moon, Y.H.; Sohn, D.H. Lead Concentrations in Blood among the General Population of Korea. Int. Arch. Occup. Environ. Health 1996, 68, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Huang, L.; Yan, B.; Li, H.; Sun, H.; Bi, J. Effect of Lead Pollution Control on Environmental and Childhood Blood Lead Level in Nantong, China: An Interventional Study. Environ. Sci. Technol. 2014, 48, 12930–12936. [Google Scholar] [CrossRef] [PubMed]
- Ahamed, M.; Verma, S.; Kumar, A.; Siddiqui, M. Environmental Exposure to Lead and its Correlation with Biochemical Indices in Children. Sci. Total Environ. 2005, 346, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Lanphear, B.P.; Weitzman, M.; Eberly, S. Racial Differences in Urban Children’s Environmental Exposures to Lead. Am. J. Public Health 1996, 86, 1460–1463. [Google Scholar] [CrossRef] [PubMed]
- Bellinger, D.C. Lead Neurotoxicity and Socioeconomic Status: Conceptual and Analytical Issues. Neurotoxicology 2008, 29, 828–832. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Ai, Y.; McCauley, L.; Pinto-Martin, J.; Yan, C.; Shen, X.; Needleman, H. Blood Lead Levels and Associated Sociodemographic Factors among Preschool Children in the South Eastern Region of China. Paediatr. Perinat. Epidemiol. 2012, 26, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Naicker, N.; Norris, S.A.; Mathee, A.; von Schirnding, Y.E.; Richter, L. Prenatal and Adolescent Blood Lead Levels in South Africa: Child, Maternal and Household Risk Factors in the Birth to Twenty Cohort. Environ. Res. 2010, 110, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Bannon, D.I.; Portnoy, M.E.; Olivi, L.; Lees, P.S.; Culotta, V.C.; Bressler, J.P. Uptake of Lead and Iron by Divalent Metal Transporter 1 in Yeast and Mammalian Cells. Biochem. Biophys. Res. Commun. 2002, 295, 978–984. [Google Scholar] [CrossRef]
- Wright, R.O.; Tsaih, S.; Schwartz, J.; Wright, R.J.; Hu, H. Association between Iron Deficiency and Blood Lead Level in a Longitudinal Analysis of Children Followed in an Urban Primary Care Clinic. J. Pediatr. 2003, 142, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Schell, L.M.; Denham, M.; Stark, A.D.; Ravenscroft, J.; Parsons, P.; Schulte, E. Relationship between Blood Lead Concentration and Dietary Intakes of Infants from 3 to 12 Months of Age. Environ. Res. 2004, 96, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Shahar, D.; Shai, I.; Vardi, H.; Shahar, A.; Fraser, D. Diet and Eating Habits in High and Low Socioeconomic Groups. Nutrition 2005, 21, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Kordas, K.; Lönnerdal, B.; Stoltzfus, R.J. Interactions between Nutrition and Environmental Exposures: Effects on Health Outcomes in Women and Children. J. Nutr. 2007, 137, 2794–2797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marmot, M. Multilevel Approaches to Understanding Social Determinants. In Social Epidemiology; Oxford University Press: New York, NY, USA, 2000; pp. 349–367. [Google Scholar]
- Ha, M.; Kwon, H.; Lim, M.; Jee, Y.; Hong, Y.; Leem, J.; Sakong, J.; Bae, J.; Hong, S.; Roh, Y. Low Blood Levels of Lead and Mercury and Symptoms of Attention Deficit Hyperactivity in Children: A Report of the Children’s Health and Environment Research (CHEER). Neurotoxicology 2009, 30, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Gwiazda, R.; Campbell, C.; Smith, D. A Noninvasive Isotopic Approach to Estimate the Bone Lead Contribution to Blood in Children: Implications for Assessing the Efficacy of Lead Abatement. Environ. Health Perspect. 2005, 113, 104–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Childs, C. Interpolating Surfaces in ArcGIS Spatial Analyst. ArcUser 2004, 32–35. [Google Scholar]
- Ahamed, M.; Singh, S.; Behari, J.; Kumar, A.; Siddiqui, M. Interaction of Lead with some Essential Trace Metals in the Blood of Anemic Children from Lucknow, India. Clin. Chim. Acta 2007, 377, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Hou, S.; Yuan, L.; Jin, P.; Ding, B.; Qin, N.; Li, L.; Liu, X.; Wu, Z.; Zhao, G.; Deng, Y. A Clinical Study of the Effects of Lead Poisoning on the Intelligence and Neurobehavioral Abilities of Children. Theor. Biol. Med. Model. 2013, 10, 13. [Google Scholar] [CrossRef] [PubMed]
- Téllez-Rojo, M.M.; Hernández-Avila, M.; Lamadrid-Figueroa, H.; Smith, D.; Hernández-Cadena, L.; Mercado, A.; Aro, A.; Schwartz, J.; Hu, H. Impact of Bone Lead and Bone Resorption on Plasma and Whole Blood Lead Levels during Pregnancy. Am. J. Epidemiol. 2004, 160, 668–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Kim, Y.; Ahn, Y.; Paik, H.; Aim, Y.; Tokudome, Y.; Hamajima, N.; Inouc, M.; Tajima, K. Development of a Food Frequency Questionnaire in Koreans. Asia Pac. J. Clin. Nutr. 2003, 12, 243–250. [Google Scholar] [PubMed]
- Willett, W. Nutritional Epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Czink, N.; Cera, P.; Salo, J.; Bonek, E.; Nuutinen, J.; Ylitalo, J. Improving Clustering Performance using Multipath Component Distance. Electron. Lett. 2006, 42, 33–35. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating Structural Equation Models with Unobservable Variables and Measurement Error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis, 6th ed.; Pearson Education: Upper Saddle River, NJ, USA, 2006. [Google Scholar]
- Kim, H.; Lim, Y.; Kim, S.; Yeo, I.; Shin, D.; Yang, J. Health Risk Assessment for Artificial Turf Playgrounds in School Athletic Facilities: Multi-Route Exposure Estimation for use Patterns. Asian J. Atmos. Environ. 2012, 6, 206–221. [Google Scholar] [CrossRef]
- Mielke, H.W.; Gonzales, C.R.; Powell, E.; Jartun, M.; Mielke, P.W. Nonlinear Association between Soil Lead and Blood Lead of Children in Metropolitan New Orleans, Louisiana: 2000–2005. Sci. Total Environ. 2007, 388, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Pizzol, M.; Thomsen, M.; Andersen, M.S. Long-Term Human Exposure to Lead from Different Media and Intake Pathways. Sci. Total Environ. 2010, 408, 5478–5488. [Google Scholar] [CrossRef] [PubMed]
- NHMRC. Revision of the Australian Guidelines for Lead in Blood and Lead in Ambient Air; Report of the 115th Session of the NHMRC (National Health and Medical Research Council); NHMRC: Canberra, Australia, 1993.
- NHMRC. Blood Lead Level for Australians; NHMRC Information Paper; NHMRC: Canberra, Australia, 2009.
- Yang, J.; Kim, J.; Jang, J.; Lee, G.; Kim, S.; Shin, D.; Lim, Y. Exposure and Toxicity Assessment of Ultrafine Particles from Nearby Traffic in Urban Air in Seoul, Korea. Environ. Health Toxicol. 2013, 28, e2013007. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Fenske, R.A.; Simcox, N.J.; Kalman, D. Pesticide Exposure of Children in an Agricultural Community: Evidence of Household Proximity to Farmland and Take Home Exposure Pathways. Environ. Res. 2000, 84, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Karadžinska-Bislimovska, J.; Minov, J.; Stoleski, S.; Mijakoski, D.; Risteska-Kuc, S.; Milkovska, S. Environmental and Occupational Health Risks among Agricultural Workers Living in a Rural Community Near Petroleum Refinery and Motorway in Skopje Region. Arch. Ind. Hyg. Toxicol. 2010, 61, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Meza-Montenegro, M.M.; Valenzuela-Quintanar, A.I.; Balderas-Cortés, J.J.; Yanez-Estrada, L.; Gutiérrez-Coronado, M.L.; Cuevas-Robles, A.; Gandolfi, A.J. Exposure Assessment of Organochlorine Pesticides, Arsenic, and Lead in Children from the Major Agricultural Areas in Sonora, Mexico. Arch. Environ. Contam. Toxicol. 2013, 64, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Carrel, M.; Zahrieh, D.; Young, S.G.; Oleson, J.; Ryckman, K.K.; Wels, B.; Simmons, D.L.; Saftlas, A. High Prevalence of Elevated Blood Lead Levels in both Rural and Urban Iowa Newborns: Spatial Patterns and Area-Level Covariates. PLoS ONE 2017, 12, e0177930. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.C.; Gerbing, D.W. Structural Equation Modeling in Practice: A Review and Recommended Two-Step Approach. Psychol. Bull. 1988, 103, 411. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | n = 4744 | Mean ± SD(μg/dL) | p-Value * | Variables | n = 4744 | Mean ± SD(μg/dL) | p-Value * |
|---|---|---|---|---|---|---|---|
| Sex | Age | ||||||
| Boy | 2425 | 1.89 ± 1.06 | <0.0001 | <8 year | 2831 | 1.83 ± 1.05 | 0.0003 |
| Girl | 2319 | 1.68 ± 0.83 | ≥8 year | 1913 | 1.73 ± 0.81 | ||
| Paternal education | Maternal education | ||||||
| <12 year | 179 | 2.09 ± 1.11 | <0.0001 | <12 year | 179 | 2.00 ± 1.06 | <0.0001 |
| 12 year | 1846 | 1.86 ± 0.91 | 12 year | 2342 | 1.83 ± 1.02 | ||
| >12 year | 2234 | 1.71 ± 0.99 | >12 year | 1691 | 1.69 ± 0.86 | ||
| Unknown | 485 | 1.76 ± 0.91 | Unknown | 532 | 1.83 ± 0.95 | ||
| Household income (103 KRW/month) † | Playing outside on weekdays | ||||||
| <$1000 | 304 | 1.90 ± 0.89 | 0.0001 | <1 h | 2968 | 1.72 ± 0.99 | <0.0001 |
| $1000–<$2000 | 1004 | 1.88 ± 1.24 | 1 h–<3 h | 1520 | 1.89 ± 0.88 | ||
| $2000–<$3000 | 1600 | 1.77 ± 0.88 | 3 h–<5 h | 131 | 2.14 ± 0.95 | ||
| $3000–<$5000 | 1357 | 1.74 ± 0.88 | ≥5 h | 24 | 2.53 ± 1.74 | ||
| ≥$5000 | 442 | 1.68 ± 0.76 | Unknown | 101 | 1.72 ± 0.79 | ||
| Unknown | 37 | 1.80 ± 1.05 | |||||
| Lead in the air | Total length of every road within a 200-m radius of the house | ||||||
| <0.054μg/m3 | 2352 | 1.74 ± 0.98 | 0.001 | <200 m | 3257 | 1.77 ± 0.86 | 0.25 |
| ≥0.054 μg/m3 | 2392 | 1.83 ± 0.93 | ≥200 m | 1340 | 1.80 ± 0.96 | ||
| Unknown | 147 | 2.11 ± 2.23 | |||||
| Farmer’s children | Pesticides use in agriculture | ||||||
| No | 3704 | 1.77 ± 0.90 | 0.01 | No | 3843 | 1.78 ± 0.90 | 0.01 |
| Yes | 463 | 1.93 ± 1.39 | Yes | 334 | 1.99 ± 1.56 | ||
| Unknown | 577 | 1.75 ± 0.90 | Unknown | 567 | 1.75 ± 0.90 | ||
| Nutrition (%) | |||||||
| High | 1752 | 1.72 ± 0.87 | <0.0001 | ||||
| Low | 2992 | 1.83 ± 1.01 | |||||
| Iron ‡ | Protein ‡ | ||||||
| High | 4272 | 1.77 ± 0.97 | 0.003 | High | 3558 | 1.76 ± 0.98 | 0.0002 |
| Low | 472 | 1.90 ± 0.83 | Low | 1186 | 1.87 ± 0.88 | ||
| Calcium ‡ | Zinc ‡ | ||||||
| High | 1186 | 1.73 ± 0.87 | 0.009 | High | 1183 | 1.72 ± 0.85 | 0.002 |
| Low | 3558 | 1.81 ± 0.99 | Low | 3561 | 1.81 ± 0.99 | ||
| Variables | β | (95% CI) | p-Value * | P for Trends * | ≥2 μg/dL n (%) | p-Value † |
|---|---|---|---|---|---|---|
| Socioeconomic status (%) | 0.001 | |||||
| High | Referent | 517 (28.2) | <0.0001 | |||
| Middle | 0.052 | (−0.03, 0.14) | 0.23 | 194 (31.1) | ||
| Middle-Low | 0.138 | (0.06, 0.21) | <0.0001 | 327 (34.2) | ||
| Low | 0.224 | (0.14, 0.31) | <0.0001 | 290 (39.0) | ||
| Playing outside on weekdays | 0.012 | |||||
| <1 h | Referent | 850 (28.6) | <0.0001 | |||
| 1 h–< 3 h | 0.140 | (0.08, 0.20) | <0.0001 | 548 (36.1) | ||
| 3 h–< 5 h | 0.374 | (0.21, 0.54) | <0.0001 | 67 (51.2) | ||
| ≥5 h | 0.719 | (0.34, 1.10) | <0.0001 | 14 (58.3) | ||
| Lead in the air | ||||||
| <0.054 μg/m3 | Referent | 699 (29.7) | 0.001 | |||
| ≥0.054 μg/m3 | 0.110 | (0.06, 0.17) | <0.0001 | 814 (34.0) | ||
| Farmer’s children | ||||||
| No | Referent | 1167 (31.5) | 0.003 | |||
| Yes | 0.171 | (0.08, 0.26) | <0.0001 | 178 (38.4) | ||
| Nutrition (%) | ||||||
| High | Referent | 507 (28.9) | 0.001 | |||
| Low | 0.098 | (0.04, 0.15) | 0.001 | 1006 (33.6) | ||
| Sex | ||||||
| Girl | Referent | 634 (27.3) | <0.0001 | |||
| Boy | 0.201 | (0.15, 0.25) | <0.0001 | 879 (36.3) | ||
| Age | ||||||
| <8 year | Referent | 960 (33.9) | <0.0001 | |||
| ≥8 year | −0.128 | (−0.19, −0.07) | <0.0001 | 553 (28.9) | ||
| Intercept | 1.454 | (1.38, 1.53) | <0.0001 | |||
| Alternative Hypothesis | Standard Coefficient | Z | p-Value | Acceptance and Rejection of Alternative Hypothesis |
|---|---|---|---|---|
| Socioeconomic status | ||||
| Blood lead (direct) | −0.111 | −6.09 | <0.001 | Acceptance |
| Blood lead (indirect) | −0.020 | −2.89 | 0.004 | Acceptance |
| Blood lead (total) | −0.132 | −7.79 | <0.001 | Acceptance |
| Playing outside | ||||
| Blood lead (direct) | 0.113 | 7.69 | <0.001 | Acceptance |
| Nutrition | ||||
| Blood lead (direct) | −0.062 | −3.72 | <0.001 | Acceptance |
| Lead in the air and total length of road | ||||
| Blood lead (direct) | 0.068 | 2.82 | 0.005 | Acceptance |
| Agriculture | ||||
| Blood lead (direct) | 0.059 | 3.23 | 0.001 | Acceptance |
| Blood lead (indirect) | −0.021 | −7.72 | <0.001 | Acceptance |
| Blood lead (total) | 0.038 | 2.11 | 0.035 | Acceptance |
| Agriculture | ||||
| Lead in the air and total length of road (direct) | −0.306 | −7.72 | <0.001 | Acceptance |
| Socioeconomic status | ||||
| Lead in the air and total length of road (direct) | 0.188 | 7.11 | <0.001 | Acceptance |
| Lead in the air and total length of road (indirect) | 0.058 | 6.28 | <0.001 | Acceptance |
| Lead in the air and total length of road (total) | 0.246 | 8.41 | <0.001 | Acceptance |
| Socioeconomic status | ||||
| Nutrition (direct) | 0.133 | 6.66 | <0.001 | Acceptance |
| Socioeconomic status | ||||
| Playing outside (direct) | −0.153 | −8.98 | <0.001 | Acceptance |
| Socioeconomic status | ||||
| Agriculture (direct) | −0.190 | −10.12 | <0.001 | Acceptance |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, E.; Kwon, H.-j.; Ha, M.; Lim, J.-A.; Lim, M.H.; Yoo, S.-J.; Paik, K.C. How Does Low Socioeconomic Status Increase Blood Lead Levels in Korean Children? Int. J. Environ. Res. Public Health 2018, 15, 1488. https://doi.org/10.3390/ijerph15071488
Kim E, Kwon H-j, Ha M, Lim J-A, Lim MH, Yoo S-J, Paik KC. How Does Low Socioeconomic Status Increase Blood Lead Levels in Korean Children? International Journal of Environmental Research and Public Health. 2018; 15(7):1488. https://doi.org/10.3390/ijerph15071488
Chicago/Turabian StyleKim, Eunjung, Ho-jang Kwon, Mina Ha, Ji-Ae Lim, Myung Ho Lim, Seung-Jin Yoo, and Ki Chung Paik. 2018. "How Does Low Socioeconomic Status Increase Blood Lead Levels in Korean Children?" International Journal of Environmental Research and Public Health 15, no. 7: 1488. https://doi.org/10.3390/ijerph15071488
APA StyleKim, E., Kwon, H. -j., Ha, M., Lim, J. -A., Lim, M. H., Yoo, S. -J., & Paik, K. C. (2018). How Does Low Socioeconomic Status Increase Blood Lead Levels in Korean Children? International Journal of Environmental Research and Public Health, 15(7), 1488. https://doi.org/10.3390/ijerph15071488