Differences of Four Work-Related Behavior and Experience Patterns in Work Ability and Other Work-Related Perceptions in a Finance Company


Abstract
:1. Introduction
1.1. Work-Related Behavior and Experience Patterns: The AVEM
1.2. Work-Related Behavior and Experience Patterns and Work Ability
1.3. Work-Related Behavior and Experience Patterns and Job Engagement, Job Satisfaction, Presenteeism, and Turnover Intention
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Work-Related Behavior and Experience Pattern (AVEM)
2.3.2. Work Ability Index (WAI)
2.3.3. Work Ability Survey-R (WAS-R)
2.3.4. Job Satisfaction
2.3.5. Turnover Intention
2.3.6. Work Engagement
2.3.7. Presenteeism
3. Results
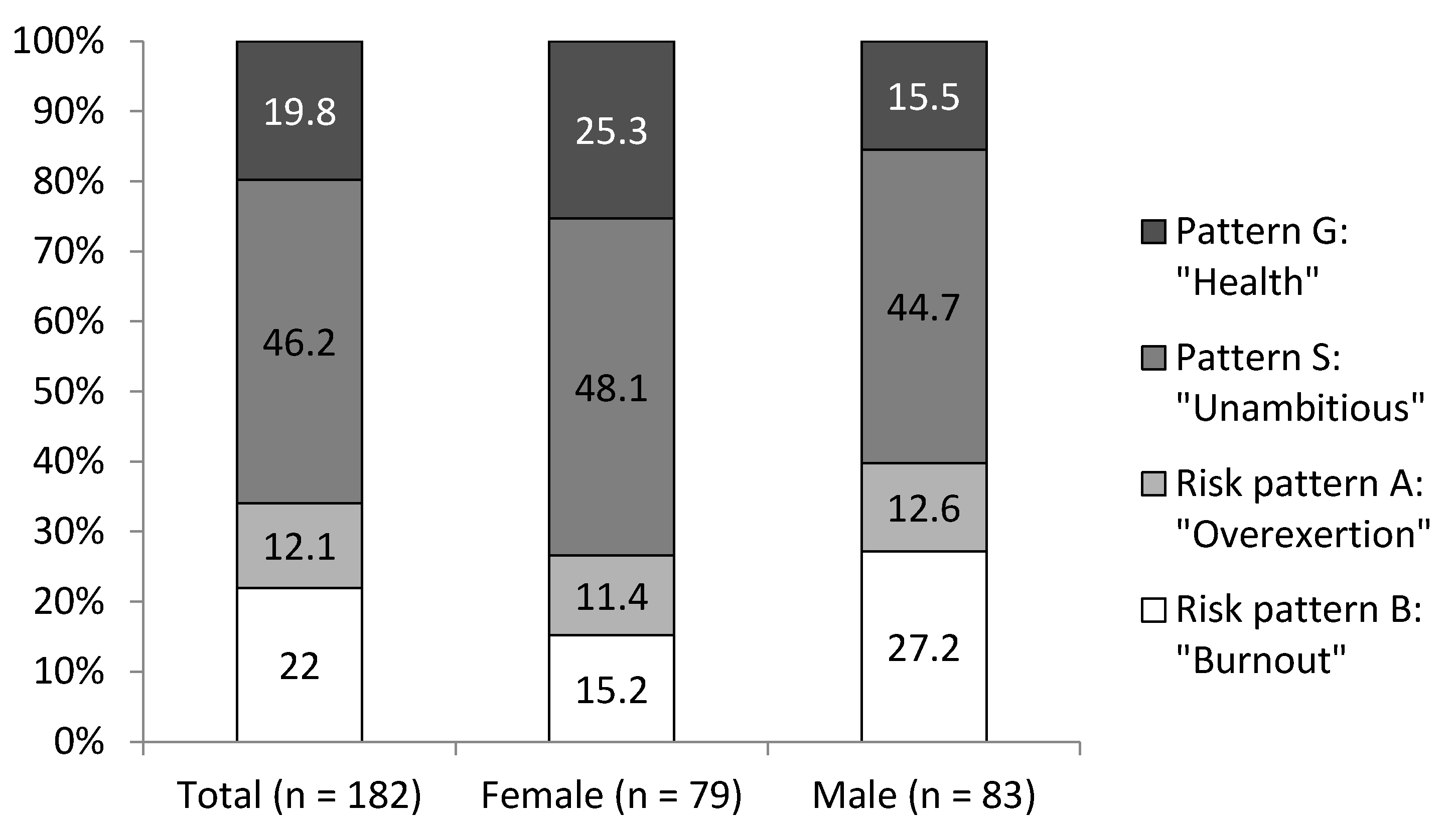
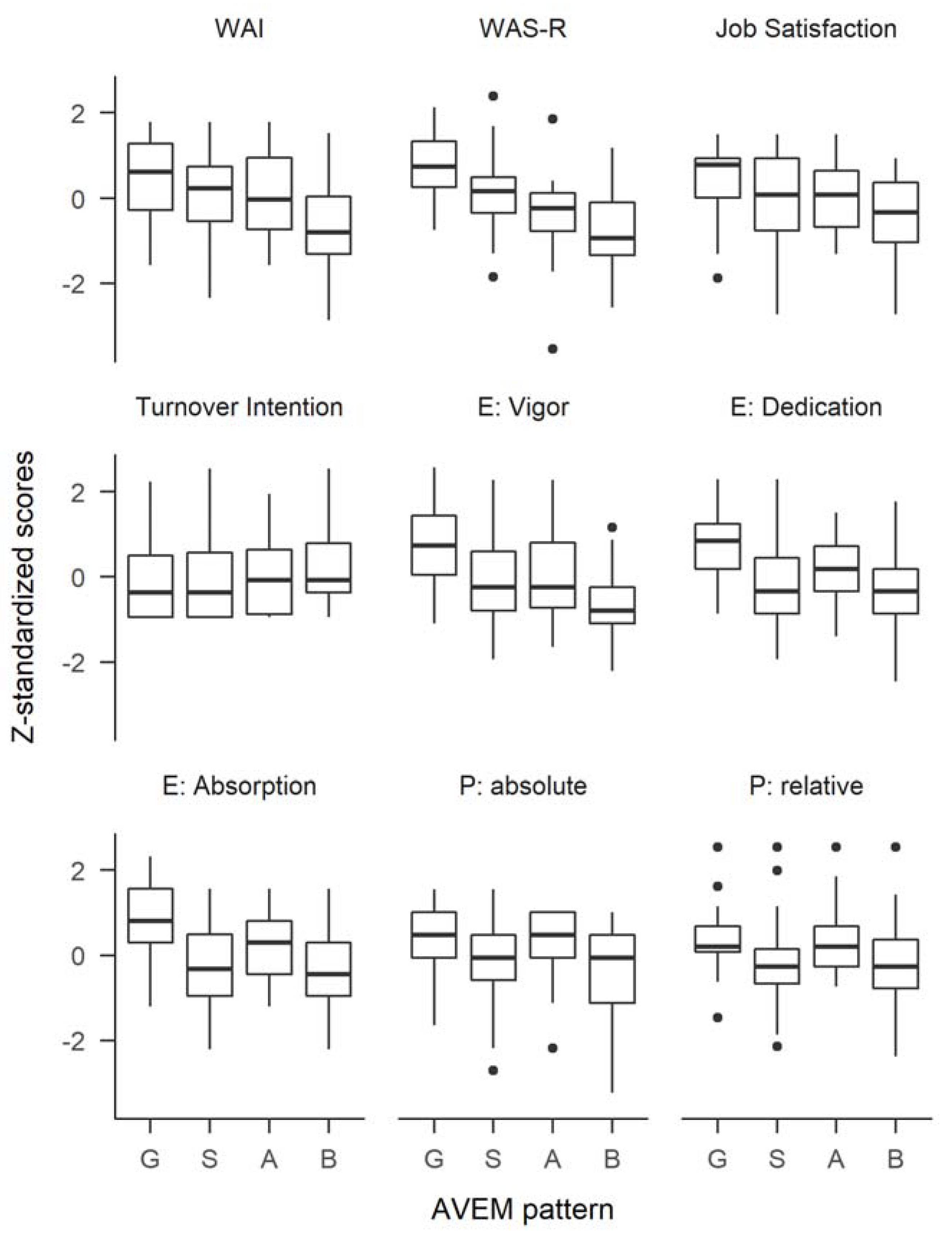
Differences in AVEM Patterns
4. Discussion
4.1. Hypothesized Differences in Work-Related Behavior and Experience Patterns and Hypothesized Work Outcome Differences
4.2. Further Results on Work-Related Behavior and Experience Patterns and Work Outcome Differences
4.3. Implications for Health Promotion
- Different situations, environments, and individuals call for different interventions to promote health and wellbeing at work. In our study, a substantial proportion of participants indicated a rather unambitious attitude towards work or even a burnout-related risk pattern. These individuals are in part strongly differing from those participants with a healthier pattern in terms of perception of and behavior at work. Applying a “one-size-fits-all” intervention will, at a minimum, waste resources on one of the groups but, in the worst case, could also have harmful effects on one of the groups, while being beneficial to the other. Studies show that more tailored approaches could tackle workplace health challenges more effectively [9,101]. Based on results in rehabilitation patients [75] and teachers [102], a health-training program has been developed that addresses the specific needs of the respective risk patterns [102]. Starting with the AVEM as a diagnostic of the four work-related behavior and experience patterns, accompanied by additional general measures of work organization and stress management (e.g., problem-solving training, time- and self-management, training of communication and social competence, goal setting), specific recommendations for clients with risk patterns A and B are made. Both have in common an inability to distance oneself from work and to relax. In clients with risk pattern A, this is mainly self-imposed. There is still energy to change behavior and circumstances. Emphasis on training in self- and time-management as well as relaxation techniques could be helpful. Clients with risk pattern B often feel like victims of circumstances and lack the energy for change. Therefore, emotional stabilization and support in goal setting and proactive coping are needed. For those employees with unambitious pattern S, the main challenge is to foster work motivation and engagement. Measures of human resource development like job enrichment or job enlargement may be appropriate steps to overcome the unambitious attitude.
- As these recommendations primarily addressed personal behavior, and while addressing only physical health factors can already improve health and wellbeing [101,103,104], a systemic approach that addresses also the organizational and even the societal level (i.e., integrated programs of occupation health management) delivered more promising results [105,106,107,108]. After a diagnostic approach (sick leave analysis, employee survey, work process analysis), these programs usually comprise measures of work process and equipment optimization (e.g., shift schedules, office chair and desk, prohibition of smoking) at the workplace, in addition to measures that address the identified specific health risk behaviors (e.g., stress management training, preventive back and spine exercise courses). Great emphasis must be placed on the participation of employees in the development of measures and an evaluation of the results. Moreover, emphasis should also be placed on the supervisor and leadership style: supervisor behavior not only has a direct impact on health [109], but studies also suggest indirect effects via working conditions and personality of the worker [110], and supervisors not only act as occupational role models, but also as role models on the border between occupational and nonoccupational life [111]. However, according to surveys of the German insurance branch, a preliminary diagnostic step or an evaluation of effects was seldom used, and measures of individual health promotion dominated. Integration in an occupational health and human resource management program increased the likelihood and number of performed measures [112,113]. Within the participating company in our study, the study results must be seen as only the first step to derive and develop measures to tackle occupational health from both an individual perspective and a company perspective. Further research evaluating the impact of organizational culture, supervisor and leadership style, and societal factors is needed.
4.4. Limitations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Digitale Arbeit—Digitale Gesundheit. BKK Gesundheitsreport 2017 [Digital Work—DIGITAL health: BKK Health Report 2017]; Knieps, F.; Pfaff, H. (Eds.) Medizinisch Wissenschaftliche Verlagsgesellschaft: Berlin, Germany, 2017. [Google Scholar]
- Nöllenheidt, C. Arbeitswelt im Wandel. Zahlen-Daten-Fakten (Changing World of Work: Facts and Figures); Federal Institute for Occupational Safety and Health: Dortmund, Germany, 2013. [Google Scholar]
- Fuchs, J. Demografie und Fachkräftemangel: Die künftigen arbeitsmarktpolitischen Herausforderungen (Demography and labor shortage. Future challenges of labor market policy). Bundesgesundheitsbla 2013, 56, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Bußmann, S.; Seyda, S. Fachkräfteengpässe in Unternehmen [Shortage of skilled workers]. Die Altersstruktur in Engpassberufen (The Age Distribution in Bottleneck Jobs); Institut der deutschen Wirtschaft Köln e.V.: Köln, Germany, 2014. [Google Scholar]
- Leon, D.A. Trends in European life expectancy: A salutary view. Int. J. Epidemiol. 2011, 40, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Bloom, D.E.; Canning, D.; Mansfield, R.K.; Moore, M. Demographic change, social security systems, and savings. J. Monet. Econ. 2007, 54, 92–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong-Stassen, M. Organisational practices and the post-retirement employment experience of older workers. Hum. Resour. Manag. J. 2008, 18, 36–53. [Google Scholar] [CrossRef]
- Wöhrmann, A.M.; Deller, J.; Wang, M. Postretirement career planning: Testing a model based on social cognitive career theory. J. Career Dev. 2014, 41, 363–381. [Google Scholar] [CrossRef]
- Truxillo, D.M.; Cadiz, D.M.; Hammer, L.B. Supporting the aging workforce: A review and recommendations for workplace intervention research. Annu. Rev. Organ. Psychol. Organ. Behav. 2015, 2, 351–381. [Google Scholar] [CrossRef]
- Schaarschmidt, U.; Fischer, A.W. Arbeitsbezogenes Verhaltens- und Erlebensmuster (Work-Related Behavior and Experience Pattern). AVEM (Standardform [Standard form]): AVEM-44 (Kurzform [Short form]): Manual; 3., überarb. und erw. Aufl.; Pearson: Frankfurt, Germany, 2008. [Google Scholar]
- Schaufeli, W.B.; Taris, T.W. A critical review of the Job Demands-Resources Model: Implications for improving work and health. In Bridging Occupational, Organizational and Public Health; Bauer, G.F., Hämmig, O., Eds.; Springer: Dordrecht, The Netherlands, 2014; pp. 43–68. [Google Scholar]
- Hobfoll, S.E. Conservation of resources: A new attempt at conceptualizing stress. Am. Psychol. 1989, 44, 513–524. [Google Scholar] [CrossRef] [PubMed]
- Armstrong-Stassen, M.; Schlosser, F.; Zinni, D. Seeking resources: Predicting retirees’ return to their workplace. J. Manag. Psychol. 2012, 27, 615–635. [Google Scholar] [CrossRef]
- Ilmarinen, J.; Tuomi, K.; Eskelinen, L.; Nygård, C.-H.; Huuhtanen, P.; Klockars, M. Background and objectives of the Finnish research project on aging workers in municipal occupations. Scand. J. Work Environ. Health 1991, 17, 7–11. [Google Scholar] [PubMed]
- Roelen, C.A.M.; van Rhenen, W.; Groothoff, J.W.; van der Klink, J.J.L.; Twisk, J.W.R.; Heymans, M.W. Work ability as prognostic risk marker of disability pension: Single-item work ability score versus multi-item work ability index. Scand. J. Work Environ. Health 2014, 40, 428–431. [Google Scholar] [CrossRef] [PubMed]
- Roelen, C.A.M.; Heymans, M.W.; Twisk, J.W.R.; van der Klink, J.J.L.; Groothoff, J.W.; van Rhenen, W. Work Ability Index as tool to identify workers at risk of premature work exit. J. Occup. Rehabil. 2014, 24, 747–754. [Google Scholar] [CrossRef] [PubMed]
- Schaufeli, W.B.; Bakker, A.B. Job demands, job resources, and their relationship with burnout and engagement: A multi-sample study. J. Organ. Behav. 2004, 25, 293–315. [Google Scholar] [CrossRef]
- Demerouti, E.; Bakker, A.B. The Job Demands–Resources model: Challenges for future research. SA J. Ind. Psychol. 2011, 37. [Google Scholar] [CrossRef]
- Kaschka, W.P.; Korczak, D.; Broich, K. Modediagnose Burn-out (Trend diagnosis burnout). Deutsch. Ärztebl. 2011, 108, 781–787. [Google Scholar]
- Schaufeli, W.B.; Enzmann, D. The Burnout Companion to Study and Practice. A Critical Analysis; Taylor & Francis: London, UK, 1998. [Google Scholar]
- Demerouti, E.; Bakker, A.B.; Leiter, M.P. Burnout and job performance: The moderating role of selection, optimization, and compensation strategies. J. Occup. Health Psychol. 2014, 19, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1986. [Google Scholar]
- Siegrist, J.; Starke, D.; Chandola, T.; Godin, I.; Marmot, M.; Niedhammer, I.; Peter, R. The measurement of effort–reward imbalance at work: European comparisons. Soc. Sci. Med. 2004, 58, 1483–1499. [Google Scholar] [CrossRef]
- Steptoe, A.; Siegrist, J.; Kirschbaum, C.; Marmot, M. Effort-reward imbalance, overcommitment, and measures of cortisol and blood pressure over the working day. Psychosom. Med. 2004, 66, 323–329. [Google Scholar] [PubMed]
- Siegrist, J. Adverse health effects of high-effort/low-reward conditions. J. Occup. Health Psychol. 1996, 1, 27–41. [Google Scholar] [CrossRef] [PubMed]
- Kivimäki, M.; Virtanen, M.; Elovainio, M.; Kouvonen, A.; Väänänen, A.; Vahtera, J. Work stress in the etiology of coronary heart disease: A meta-analysis. Scand. J. Work Environ. Health 2006, 32, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Sonnentag, S.; Binnewies, C.; Mojza, E.J. Staying well and engaged when demands are high: The role of psychological detachment. J. Appl. Psychol. 2010, 95, 965–976. [Google Scholar] [CrossRef] [PubMed]
- Richter, P.; Hille, B.; Rudolf, M. Gesundheitsrelevante Bewältigung von Arbeitsanforderungen (Health relevant coping with job demands). Z. Differ. Diagn. Psychol. 1999, 20, 25–38. [Google Scholar] [CrossRef]
- Bakker, A.B.; Schaufeli, W.B.; Leiter, M.P.; Taris, T.W. Work engagement: An emerging concept in occupational health psychology. Work Stress 2008, 22, 187–200. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Salanova, M.; González-romá, V.; Bakker, A.B. The measurement of engagement and burnout: A two sample confirmatory factor analytic approach. J. Happiness Stud. 2002, 3, 71–92. [Google Scholar] [CrossRef]
- Folkman, S.; Lazarus, R.S. The relationship between coping and emotion: Implications for theory and research. Soc. Sci. Med. 1988, 26, 309–317. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Antonovsky, A. Unraveling the Mystery of Health. How People Manage Stress and Stay Well, 1st ed.; 2. print; Jossey-Bass: San Francisco, CA, USA, 1988. [Google Scholar]
- Moak, Z.B.; Agrawal, A. The association between perceived interpersonal social support and physical and mental health: Results from the National Epidemiological Survey on Alcohol and Related Conditions. J. Public Health 2010, 32, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Prins, J.T.; Hoekstra-Weebers, J.E.H.M.; Gazendam-Donofrio, S.M.; van de Wiel, H.B.M.; Sprangers, F.; Jaspers, F.C.A.; van der Heijden, F.M.M.A. The role of social support in burnout among Dutch medical residents. Psychol. Health Med. 2007, 12, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Tyssen, R.; Dolatowski, F.C.; Røvik, J.O.; Thorkildsen, R.F.; Ekeberg, O.; Hem, E.; Gude, T.; Grønvold, N.T.; Vaglum, P. Personality traits and types predict medical school stress: A six-year longitudinal and nationwide study. Med. Educ. 2007, 41, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Ogińska-Bulik, N. Occupational stress and its consequences in healthcare professionals: The role of type D personality. Int. J. Occup. Med. Environ. Health 2006, 19. [Google Scholar] [CrossRef]
- Francis, L.J.; Craig, C.L.; Whinney, M.; Tilley, D.; Slater, P. Psychological typology of Anglican clergy in England: Diversity, strengths, and weaknesses in ministry. Int. J. Pract. Theol. 2007, 11. [Google Scholar] [CrossRef]
- Asendorpf, J.B.; Borkenau, P.; Ostendorf, F.; van Aken, M.A.G. Carving personality description at its joints: Confirmation of three replicable personality prototypes for both children and adults. Eur. J. Pers. 2001, 15, 169–198. [Google Scholar] [CrossRef]
- Kieschke, U.; Schaarschmidt, U. Professional commitment and health among teachers in Germany: A typological approach. Learn. Instr. 2008, 18, 429–437. [Google Scholar] [CrossRef]
- Voltmer, J.-B.; Deller, J. Measuring work ability with its antecedents: Evaluation of the Work Ability Survey. J. Occup. Rehabil. 2017. [Google Scholar] [CrossRef] [PubMed]
- Lederer, V.; Loisel, P.; Rivard, M.; Champagne, F. Exploring the diversity of conceptualizations of work (dis)ability: A scoping review of published definitions. J. Occup. Rehabil. 2014, 24, 242–267. [Google Scholar] [CrossRef] [PubMed]
- Tuomi, K.; Ilmarinen, J.; Eskelinen, L.; Järvinen, E.; Toikkanen, J.; Klockars, M. Prevalence and incidence rates of diseases and work ability in different work categories of municipal occupations. Scand. J. Work Environ. Health 1991, 17, 67–74. [Google Scholar] [PubMed]
- Ilmarinen, J.; Tuomi, K.; Klockars, M. Changes in the work ability of active employees over an 11-year period. Scand. J. Work Environ. Health 1997, 23, 49–57. [Google Scholar] [PubMed]
- Dimensions of Work Ability. Results of the Health 2000 Survey; Gould, R.; Ilmarinen, J.; Järvisalo, J.; Koskinen, S. (Eds.) Finnish Centre for Pensions: Helsinki, Finland, 2008. [Google Scholar]
- Alavinia, S.M.; van den Berg, T.I.J.; van Duivenbooden, J.C.; Elders, L.A.M.; Burdorf, A. Impact of work-related factors, lifestyle, and work ability on sickness absence among Dutch construction workers. Scand. J. Work Environ. Health 2009, 35, 325–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Berg, T.I.J.; Robroek, S.J.W.; Plat, J.F.; Koopmanschap, M.A.; Burdorf, A. The importance of job control for workers with decreased work ability to remain productive at work. Int. Arch. Occup. Environ. Health 2011, 84, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Ahlstrom, L.; Grimby-Ekman, A.; Hagberg, M.; Dellve, L. The Work Ability Index and single-item question: Associations with sick leave, symptoms, and health. A prospective study of women on long-term sick leave. Scand. J. Work Environ. Health 2010, 36, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Feldt, T.; Hyvönen, K.; Mäkikangas, A.; Kinnunen, U.; Kokko, K. Development trajectories of Finnish managers’ work ability over a 10-year follow-up period. Scand. J. Work Environ. Health 2009, 35, 37–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilmarinen, J. Work ability: A comprehensive concept for occupational health research and prevention. Scand. J. Work Environ. Health 2009, 35, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Noone, J.H.; Mackey, M.G.; Bohle, P. Work Ability in Australia—Pilot Study; Safe Work Australia: Canberra, Australia, 2014. Available online: http://www.safeworkaustralia.gov.au/sites/SWA/about/Publications/Documents/868/Work-Ability-in-Australia-July-2014.pdf (accessed on 17 July 2018).
- McLoughlin, C.; Taylor, P. Australian Work Ability Pilot Survey; Safe Work Australia: Melbourne, Australia, 2012. [Google Scholar]
- Judge, T.A.; Parker, S.K.; Colbert, A.E.; Heller, D.; Ilies, R. Job satisfaction: A cross-cultural review. In Handbook of Industrial, Work & Organizational Psychology: Volume 2 Organizational Psychology; Anderson, N., Ones, D.S., Sinangil, H.K., Eds.; Sage: London, UK, 2001; pp. 25–48. [Google Scholar]
- Locke, E.A. What is job satisfaction? Org. Behav. Hum. Perform. 1969, 4, 309–336. [Google Scholar] [CrossRef]
- Tett, R.P.; Meyer, J.P. Job satisfaction, organizational commitment, turnover intention, and turnover: Path analyses based on meta-analytic findings. Pers. Psychol. 1993, 46, 259–293. [Google Scholar] [CrossRef]
- Egan, T.M.; Yang, B.; Bartlett, K.R. The effects of organizational learning culture and job satisfaction on motivation to transfer learning and turnover intention. Hum. Resour. Dev. Q. 2004, 15, 279–301. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B.; Salanova, M. The measurement of work engagement with a short questionnaire: A cross-national study. Educ. Psychol. Meas. 2006, 66, 701–716. [Google Scholar] [CrossRef]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed]
- Csikszentmihalyi, M.; Csikszentmihalyi, I. Beyond Boredom and Anxiety, 1st ed.; [Nachdr.]; Jossey-Bass Publ.: San Francisco, CA, USA, 1977. [Google Scholar]
- Bakker, A.B.; Oerlemans, W.; Demerouti, E.; Slot, B.B.; Ali, D.K. Flow and performance: A study among talented Dutch soccer players. Psychol. Sport Exerc. 2011, 12, 442–450. [Google Scholar] [CrossRef]
- Quinn, R.W. Flow in knowledge work: High performance experience in the design of national security technology. Admin. Sci. Q. 2005, 50, 610–641. [Google Scholar] [CrossRef]
- Bergstrom, G.; Bodin, L.; Hagberg, J.; Aronsson, G.; Josephson, M. Sickness presenteeism today, sickness absenteeism tomorrow? A prospective study on sickness presenteeism and future sickness absenteeism. J. Occup. Environ. Med. 2009, 51, 629–638. [Google Scholar] [CrossRef] [PubMed]
- Taloyan, M.; Aronsson, G.; Leineweber, C.; Hanson, L.M.; Alexanderson, K.; Westerlund, H. Sickness presenteeism predicts suboptimal self-rated health and sickness absence: A nationally representative study of the Swedish working population. PLoS ONE 2012, 7, e44721. [Google Scholar] [CrossRef] [PubMed]
- Rosvold, E.O.; Bjertness, E. Physicians who do not take sick leave: Hazardous heroes? Scand. J. Public Health 2001, 29, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Bauer, J.; Stamm, A.; Virnich, K.; Wissing, K.; Muller, U.; Wirsching, M.; Schaarschmidt, U. Correlation between burnout syndrome and psychological and psychosomatic symptoms among teachers. Int. Arch. Occup. Environ. Health 2006, 79, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Voltmer, E.; Bussing, A.; Thomas, C.; Spahn, C. Religiositat, Spiritualitat, Gesundheit und berufsbezogene Verhaltensmuster bei Pastoren zweier freikirchlich-protestantischer Denominationen (Religiosity, spirituality, health and work-related behaviour patterns in pastors of two free protestant denominations). Psychother. Psychosom. Med. Psychol. 2010, 60, 425–433. [Google Scholar] [CrossRef] [PubMed]
- Gabassi, P.G.; Cervai, S.; Rozbowsky, P.; Semeraro, A.; Gregori, D. Burnout syndrome in the helping professions. Psychol. Rep. 2002, 90, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Voltmer, E.; Kieschke, U.; Schwappach, D.L.B.; Wirsching, M.; Spahn, C. Psychosocial health risk factors and resources of medical students and physicians: A cross-sectional study. BMC Med. Educ. 2008, 8, 46. [Google Scholar] [CrossRef] [PubMed]
- Voltmer, E.; Spahn, C.; Schaarschmidt, U.; Kieschke, U. Work-related behavior and experience patterns of entrepreneurs compared to teachers and physicians. Int. Arch. Occup. Environ. Health 2011, 84, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Miraglia, M.; Johns, G. Going to work ill: A meta-analysis of the correlates of presenteeism and a dual-path model. J. Occup. Health Psychol. 2016, 21, 261–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voltmer, E.; Rosta, J.; Aasland, O.G.; Spahn, C. Study-related health and behavior patterns of medical students: A longitudinal study. Med. Teach. 2010, 32, e422–e428. [Google Scholar] [CrossRef] [PubMed]
- Schaarschmidt, U. AVEM: Ein persönlichkeitsdiagnostisches Instrument für die berufsbezogene Rehabilitation (A personality diagnostic measure for occupational rehabilitation). In Psychologische Diagnostik; Weichenstellung für den Reha-Verlauf. 24. Jahrestagung des Arbeitskreises Klinische Psychologie in der Rehabilitation, Erkner, 18.-20.11.; Deutscher Psychologen Verlag: Bonn, Germany, 2005; pp. 59–82. [Google Scholar]
- Van Dick, R.; Wagner, U. Der AVEM im Lehrerberuf (The AVEM in teaching professions): Eine Validierungsstudie (A validation study). Z. Differ. Diagn. Psychol. 2001, 22, 267–278. [Google Scholar] [CrossRef]
- Rath, H.M.; Steimann, M.; Ullrich, A.; Rotsch, M.; Zurborn, K.-H.; Koch, U.; Kriston, L.; Bergelt, C. Psychometric properties of the Occupational Stress and Coping Inventory (AVEM) in a cancer population. Acta Oncol. 2015, 54, 232–242. [Google Scholar] [CrossRef] [PubMed]
- Heitzmann, B.; Schaarschmidt, U.; Kieschke, U. Diagnostik beruflichen Bewältigungsverhaltens bei Rehapatienten (Diagnostic of occupational coping behavior in rehabilitation): Die Leistungsmöglichkeiten des Verfahrens AVEM im Bereich medizinischer Rehabilitation (Performance of the AVEM in rehabilitation). Praxis Klinische Verhaltensmedizin und Rehabilitation 2005, 70, 269–280. [Google Scholar]
- Schaarschmidt, U.; Fischer, A.W. AVEM. In Diagnostische Verfahren in der Rehabilitation; Bengel, J., Wirtz, M., Zwingmann, C., Eds.; Hogrefe: Göttingen, Germany, 2008; pp. 360–363. [Google Scholar]
- Müller, B.H. Der WAI (The WAI). Available online: http://www.arbeitsfaehigkeit.uni-wuppertal.de/index.php?der-wai (accessed on 8 December 2014).
- Müller, B.H. WAI Online Questionnaire (Short Version). Available online: http://www.arbeitsfaehigkeit.uni-wuppertal.de/index.php?wai-online-en (accessed on 8 December 2014).
- Reeuwijk, K.G.; Robroek, S.J.W.; Niessen, M.A.J.; Kraaijenhagen, R.A.; Vergouwe, Y.; Burdorf, A. The prognostic value of the Work Ability Index for sickness absence among office workers. PLoS ONE 2015, 10, e0126969. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, G. PLS Path Modeling with R; Trowchez Editions: Berkeley, CA, USA, 2013. [Google Scholar]
- Wilcox, J.B.; Howell, R.D.; Breivik, E. Questions about formative measurement. J. Bus. Res. 2008, 61, 1219–1228. [Google Scholar] [CrossRef]
- Radkiewicz, P.; Widerszal-Bazyl, M. Psychometric properties of Work Ability Index in the light of comparative survey study. In Assessment and Promotion of Work Ability, Health and Well-Being of Ageing Workers, Proceedings of the 2nd International Symposium on Work Ability, Verona, Italy, 18–20 October 2004; Costa, G., Willem, J.A., Ilmarinen, J., Eds.; Elsevier: San Diego, CA, USA, 2005; pp. 304–309. [Google Scholar]
- De Zwart, B.C.H.; Frings-Dresen, M.H.W.; van Duivenbooden, J.C. Test-retest reliability of the Work Ability Index questionnaire. Occup. Med. 2002, 52, 177–181. [Google Scholar] [CrossRef] [Green Version]
- Evers, A.; Muñiz, J.; Hagemeister, C.; Høstmælingen, A.; Lindley, P.; Sjöberg, A.; Bartram, D. Assessing the quality of tests: Revision of the EFPA review model. Psicothema 2013, 25, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, K.-H.; Kleinbeck, U. Job Diagnostic Survey (JDS—deutsche Fassung) (Job Diagnostic Survey (JDS—German version)). In Handbuch Psychologischer Arbeitsanalyseverfahren [Handbook of Psychological Work Analysis Methods]; Dunckel, H., Ed.; vdf, Hochschulverlag an der ETH Zürich: Zürich, Switzerland, 1999; pp. 205–230. [Google Scholar]
- Hackman, J.R.; Oldham, G.R. The Job Diagnostic Survey. An Instrument for the Diagnosis of Jobs and the Evaluation of Job Redesign Projects; Yale University: New Haven, CT, USA, 1974. [Google Scholar]
- Loher, B.T.; Noe, R.A.; Moeller, N.L.; Fitzgerald, M.P. A meta-analysis of the relation of job characteristics to job satisfaction. J. Appl. Psychol. 1985, 70, 280. [Google Scholar] [CrossRef]
- Walsh, J.P.; Ashford, S.J.; Hill, T.E. Feedback Obstruction: The Influence of the Information Environment on Employee Turnover Intentions. Hum. Relat. 1985, 38, 23–46. [Google Scholar] [CrossRef]
- Eisinga, R.; Grotenhuis, M.T.; Pelzer, B. The reliability of a two-item scale: Pearson, Cronbach, or Spearman-Brown? Int. J. Public Health 2013, 58, 637–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Barber, C.; Beck, A.; Berglund, P.; Cleary, P.D.; McKenas, D.; Pronk, N.; Simon, G.; Stang, P.; Ustun, T.B.; et al. The World Health Organization Health and Work Performance Questionnaire (HPQ). J. Occup. Environ. Med. 2003, 45, 156–174. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Ames, M.; Hymel, P.A.; Loeppke, R.; McKenas, D.K.; Richling, D.E.; Stang, P.E.; Ustun, T.B. Using the World Health Organization Health and Work Performance Questionnaire (HPQ) to evaluate the indirect workplace costs of illness. J. Occup. Environ. Med. 2004, 46, S23–S37. [Google Scholar] [CrossRef] [PubMed]
- Scuffham, P.A.; Vecchio, N.; Whiteford, H.A. Exploring the validity of HPQ-based presenteeism measures to estimate productivity losses in the health and education sectors. Med. Decis. Mak. 2014, 34, 127–137. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R. A Language and Environment for Statistical Computing [Computer Software]; R Core Team: Vienna, Austria, 2014; Available online: http://www.R-project.org/ (accessed on 17 July 2018).
- Grosjean, P.; Ibanez, F. Pastecs. Package for Analysis of Space-Time Ecological Series. 2014. Available online: http://CRAN.R-project.org/package=pastecs (accessed on 17 July 2018).
- Revelle, W. Psych. Procedures for Psychological, Psychometric, and Personality Research [Computer Software]; Northwestern University: Evanston, IL, USA, 2014; Available online: http://CRAN.R-project.org/package=psych (accessed on 17 July 2018).
- Showalter, S.E. Compassion fatigue: What is it? Why does it matter? Recognizing the symptoms, acknowledging the impact, developing the tools to prevent compassion fatigue, and strengthen the professional already suffering from the effects. Am. J. Hosp. Palliat. Care 2010, 27, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Schwarze, M.; Egen, C.; Gutenbrunner, C.; Schriek, S. Early workplace intervention to improve the work ability of employees with musculoskeletal disorders in a German university hospital: Results of a pilot study. Healthcare 2016, 4, 64. [Google Scholar] [CrossRef] [PubMed]
- Cooklin, A.; Joss, N.; Husser, E.; Oldenburg, B. Integrated approaches to occupational health and safety: A systematic review. Am. J. Health Promot. 2017, 31, 401–412. [Google Scholar] [CrossRef] [PubMed]
- De Boer, A.; Verbeek, J.H.A.M.; Spelten, E.R.; Uitterhoeve, A.L.J.; Ansink, A.C.; de Reijke, T.M.; Kammeijer, M.; Sprangers, M.A.G.; van Dijk, F.J.H. Work ability and return-to-work in cancer patients. Br. J. Cancer 2008, 98, 1342–1347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Boer, A.G.E.M.; van Beek, J.-C.; Durinck, J.; Verbeek, J.H.A.M.; van Dijk, F.J.H. An occupational health intervention programme for workers at risk for early retirement: A randomised controlled trial. Occup. Environ. Med. 2004, 61, 924–929. [Google Scholar] [CrossRef] [PubMed]
- Kettunen, O.; Vuorimaa, T.; Vasankari, T. 12-mo intervention of physical exercise improved work ability, especially in subjects with low baseline work ability. Int. J. Environ. Res. Public Health 2014, 11, 3859–3869. [Google Scholar] [CrossRef] [PubMed]
- Gerüstet für den Schulalltag (Equipped for Daily School Life). Psychologische Unterstützungsangebote für Lehrerinnen und Lehrer (Psychological Support Offers for Teachers); Schaarschmidt, U.; Kieschke, U. (Eds.) Dr. Nach Typoskript; Beltz: Weinheim, Germany, 2007. [Google Scholar]
- Andersen, L.N.; Kristensen, B.J.; Sorensen, T.L.; Gram, L. Reduced sickness absence after a physical activity intervention among health care workers: One-year follow-up of a randomised controlled trial. Int. J. Phys. Med. Rehabil. 2016, 4. [Google Scholar] [CrossRef]
- Klaperski, S.; Seelig, H.; Fuchs, R. Sportaktivität als Stresspuffer (Sporting activities as a stress buffer). Z. Sportpsychol. 2012, 19, 80–90. [Google Scholar] [CrossRef]
- Badura, B.; Ritter, W.; Scherf, M. Betriebliches Gesundheitsmanagement (Occupational Health Management). Ein Leitfaden für die Praxis (Guidelines for Praxis); Sigma: Berlin, Germany, 1999. [Google Scholar]
- Goetzel, R.Z.; Ozminkowski, R.J. The health and cost benefits of work site health-promotion programs. Annu. Rev. Public Health 2008, 29, 303–323. [Google Scholar] [CrossRef] [PubMed]
- Hasle, P.; Limborg, H.J. A review of the literature on preventive occupational health and safety activities in small enterprises. Ind. Health 2006, 44, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Effektive Betriebliche Gesundheitsförderung (Effective Occupational Health Promotion). Konzepte und Methodische Ansätze zur Evaluation und Qualitätssicherung (Concepts and Methodological Approaches for Evaluation and Quality Management); Pfaff, H.; Slesina, W. (Eds.) Juventa-Verl.: Weinheim, Germany, 2001. [Google Scholar]
- Montano, D. Supervisor behaviour and its associations with employees’ health in Europe. Int. Arch. Occup. Environ. Health 2016, 89, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Gregersen, S.; Kuhnert, S.; Zimber, A.; Nienhaus, A. Führungsverhalten und Gesundheit (Leadership behavior and health): Zum Stand der Forschung (State of research). Gesundheitswesen 2011, 73, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Koch, A.R.; Binnewies, C. Setting a good example: Supervisors as work-life-friendly role models within the context of boundary management. J. Occup. Health Psychol. 2015, 20, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Köhler, T.; Janssen, C.; Plath, S.-C.; Steinhausen, S.; Pfaff, H. Determinanten der betrieblichen Gesundheitsförderung in der Versicherungsbranche (Determinants of the occupational health promotion in the insurance industry): Ergebnisse einer Vollerhebung bei deutschen Versicherungen im Jahr 2006 (Results of a full census of German insurance companies in 2006). Gesundheitswesen 2009, 71, 722–731. [Google Scholar] [CrossRef] [PubMed]
- Thielscher, C.; Hahn, E.; Klumpp, M.; Lindenberg, B.; Matusiewicz, D. Rückenschmerz in Versicherungsunternehmen (Backache in insurance companies): Betriebliches Gesundheitsmanagement (Occupational health management). Der Orthopäde 2016, 45, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Hoenig, J.M.; Heisey, D.M. The abuse of power. Am. Stat. 2001, 55, 19–24. [Google Scholar] [CrossRef]
- Field, A.P.; Miles, J.; Field, Z. Discovering Statistics Using R; Sage: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Johnston, D.W.; Propper, C.; Shields, M.A. Comparing subjective and objective measures of health: Evidence from hypertension for the income/health gradient. J. Health Econ. 2009, 28, 540–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oswald, A.J.; Wu, S. Objective confirmation of subjective measures of human well-being: Evidence from the U.S.A. Science 2010, 327, 576–579. [Google Scholar] [CrossRef] [PubMed]
- Podsakoff, P.M.; MacKenzie, S.B.; Lee, J.-Y.; Podsakoff, N.P. Common method biases in behavioral research: A critical review of the literature and recommended remedies. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef] [PubMed]
- Doty, D.H.; Glick, W.H. Common methods bias: Does common methods variance really bias results? Organ. Res. Methods 2016, 1, 374–406. [Google Scholar] [CrossRef]
- Spector, P.E. Method variance in organizational research: Truth or urban legend? Organ. Res. Methods 2016, 9, 221–232. [Google Scholar] [CrossRef]
- Conway, J.M.; Lance, C.E. What reviewers should expect from authors regarding common method bias in organizational research. J. Bus. Psychol. 2010, 25, 325–334. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Sample w/o AVEM (n = 224) | AVEM Sample (n = 182) | Pχ² | ||
|---|---|---|---|---|---|
| Gender female n (%) | 109 | 49.1 | 79 | 43.4 | 0.254 |
| Age m (SD) | 44.6 | 10.5 | 43.9 | 10.2 | 0.492 |
| Education n (%) | - | - | - | - | 0.063 |
| (Intermediate) secondary | 76 | 35.5 | 56 | 30.8 | - |
| Higher education entrance | 94 | 43.9 | 69 | 37.9 | - |
| Tertiary education | 43 | 20.1 | 57 | 31.3 | - |
| PhD | 1 | 0.5 | 0 | 0.0 | - |
| Leadership n (%) | 12 | 5.6 | 21 | 11.7 | 0.030 |
| Partner n (%) | 165 | 73.7 | 140 | 76.9 | 0.450 |
| AVEM Dimensions | Item Example |
|---|---|
| 1. Subjective significance of work | Work is the most important element in my life |
| 2. Career ambition | I want to achieve more in my career than most people I know |
| 3. Tendency to exert | If necessary, I will work until I am exhausted |
| 4. Striving for perfection | My work should never contain errors or deficiencies |
| 5. Emotional distancing | After work is over I can forget about it quickly |
| 6. Resignation tendencies | I quickly resign myself to lack of success |
| 7. Offensive coping with problems | For me, difficulties are there to overcome |
| 8. Balance and mental stability | I do not get upset easily |
| 9. Satisfaction with work | Until now I have been successful in my work |
| 10. Satisfaction with life | So far, I have been satisfied with my life |
| 11. Experience of social support | My partner shows understanding for my work |
| Variable | n | min | max | m | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | AVEM Professional Ambition | 182 | 1.2 | 7.6 | 4.6 | 1.0 | 0.87 | ||||||||||
| 2 | AVEM Resistance toward stress | 182 | 1.8 | 6.8 | 4.8 | 0.9 | 0.32 *** | 0.50 | |||||||||
| 3 | AVEM Emotional wellbeing | 182 | 1.0 | 8.3 | 4.7 | 1.3 | 0.21 ** | 0.40 *** | 0.70 | ||||||||
| 4 | Work ability Index (WAI) | 182 | 5.0 | 23.0 | 16.1 | 3.9 | 0.17 * | 0.32 *** | 0.42 *** | ||||||||
| 5 | Work ability Survey (WAS-R) | 144 | 25.6 | 94.8 | 66.9 | 11.7 | 0.21 * | 0.36 *** | 0.65 *** | 0.50 *** | 0.94 | ||||||
| 6 | Job Satisfaction | 182 | 6.0 | 21.0 | 15.7 | 3.6 | 0.26 *** | 0.18 * | 0.37 *** | 0.32 *** | 0.57 *** | 0.68 | |||||
| 7 | Turnover Intention | 182 | 2.0 | 14.0 | 5.3 | 3.4 | −0.06 | −0.02 | −0.20 ** | −0.19 * | −0.39 *** | −0.62 *** | 0.87 | ||||
| 8 | UWES Vigor | 179 | 4.0 | 21.0 | 11.9 | 3.6 | 0.36 *** | 0.29 *** | 0.47 *** | 0.44 *** | 0.69 *** | 0.56 *** | −0.34 *** | 0.88 | |||
| 9 | UWES Dedication | 174 | 3.0 | 21.0 | 12.3 | 3.8 | 0.36 *** | 0.15 | 0.46 *** | 0.34 *** | 0.65 *** | 0.62 *** | −0.36 *** | 0.80 *** | 0.86 | ||
| 10 | UWES Absorption | 175 | 3.0 | 21.0 | 11.8 | 4.0 | 0.45 *** | 0.20 ** | 0.42 *** | 0.33 *** | 0.63 *** | 0.58 *** | −0.36 *** | 0.80 *** | 0.86 *** | 0.86 | |
| 11 | Presenteeism—absolute | 166 | 10.0 | 100.0 | 71.0 | 18.8 | 0.30 *** | 0.26 *** | 0.38 *** | 0.36 *** | 0.43 *** | 0.37 *** | −0.13 | 0.43 *** | 0.43 *** | 0.43 *** | |
| 12 | Presenteeism—relative | 163 | 25.0 | 200.0 | 109.4 | 35.6 | 0.37 *** | 0.19 * | 0.22 ** | 0.22 ** | 0.15 | 0.22 ** | −0.11 | 0.20 * | 0.18 * | 0.20 * | 0.65 *** |
| Variable | Pattern G “Health” | Pattern S “Unambitious” | Risk Pattern A “Overexertion” | Risk Pattern B “Burnout” | HSD p∆ < 0.05 |
|---|---|---|---|---|---|
| n | 32–36 | 62–84 | 18–22 | 32–40 | - |
| m (SD) | m (SD) | m (SD) | m (SD) | - | |
| WAI | 17.72 (0.60) | 16.44 (0.36) | 16.23 (0.84) | 13.78 (0.68) | G > B, S > B |
| WAS-R | 75.71 (1.41) | 68.31 (1.26) | 62.49 (3.01) | 57.92 (1.82) | G > S, G > A, G > B, S > B |
| Job satisfaction | 17.39 (0.51) | 15.65 (0.39) | 15.95 (0.61) | 14.05 (0.60) | G > B |
| Turnover intention | 4.97 (0.60) | 5.02 (0.36) | 5.27 (0.70) | 6.17 (0.58) | - |
| UWES Vigor | 14.53 (0.51) | 11.67 (0.36) | 11.95 (0.79) | 9.74 (0.48) | G > S, G > A, G > B, S > B |
| UWES Dedication | 15.11 (0.48) | 11.57 (0.42) | 12.77 (0.68) | 10.84 (0.60) | G > S, G > B |
| UWES Absorption | 15.06 (0.56) | 10.91 (0.41) | 12.50 (0.78) | 10.26 (0.59) | G > S, G > B |
| P: absolute | 81.21 (2.60) | 69.74 (2.07) | 74.74 (3.77) | 62.43 (3.34) | G > S, G > B |
| P: relative | 123.17 (5.30) | 103.05 (3.98) | 123.19 (8.26) | 102.72 (6.29) | G > S |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voltmer, J.-B.; Voltmer, E.; Deller, J. Differences of Four Work-Related Behavior and Experience Patterns in Work Ability and Other Work-Related Perceptions in a Finance Company. Int. J. Environ. Res. Public Health 2018, 15, 1521. https://doi.org/10.3390/ijerph15071521
Voltmer J-B, Voltmer E, Deller J. Differences of Four Work-Related Behavior and Experience Patterns in Work Ability and Other Work-Related Perceptions in a Finance Company. International Journal of Environmental Research and Public Health. 2018; 15(7):1521. https://doi.org/10.3390/ijerph15071521
Chicago/Turabian StyleVoltmer, Jan-Bennet, Edgar Voltmer, and Jürgen Deller. 2018. "Differences of Four Work-Related Behavior and Experience Patterns in Work Ability and Other Work-Related Perceptions in a Finance Company" International Journal of Environmental Research and Public Health 15, no. 7: 1521. https://doi.org/10.3390/ijerph15071521
APA StyleVoltmer, J. -B., Voltmer, E., & Deller, J. (2018). Differences of Four Work-Related Behavior and Experience Patterns in Work Ability and Other Work-Related Perceptions in a Finance Company. International Journal of Environmental Research and Public Health, 15(7), 1521. https://doi.org/10.3390/ijerph15071521