Air Health Trend Indicator: Association between Short-Term Exposure to Ground Ozone and Circulatory Hospitalizations in Canada for 17 Years, 1996–2012

Abstract
:1. Introduction
- The population most at risk for hospitalization related to air pollution may change over time.
- The effect modifiers such as heart or lung related health care including medical treatments and medicines may change over time.
- The association between exposure and hospitalization may be non-linear.
2. Materials and Methods
2.1. Circulatory Hospitalizations
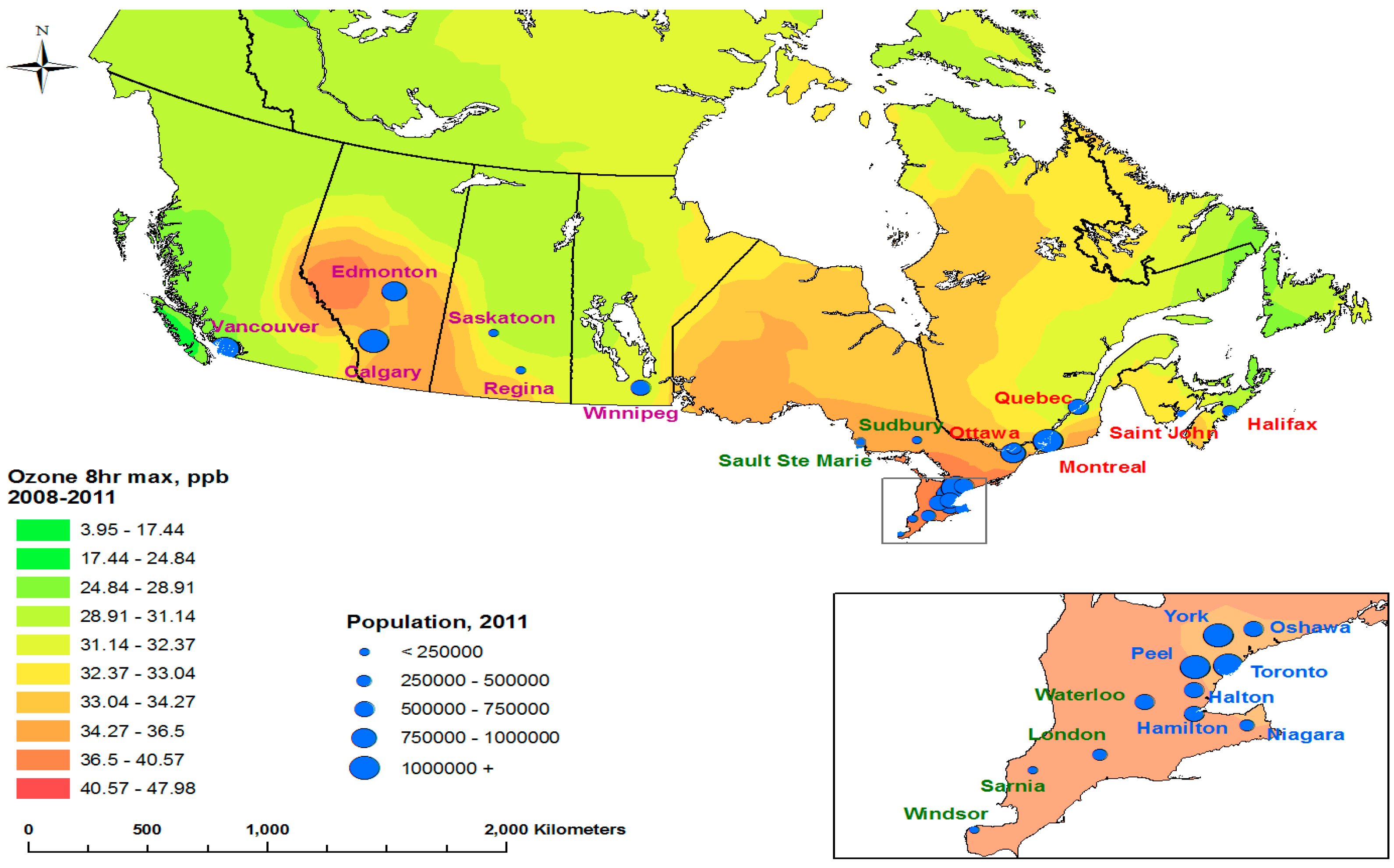
2.2. Spatial Coverage
2.3. Data Sources
2.3.1. Ozone Concentrations
2.3.2. Daily Counts of Cause-Specific Hospitalization
2.3.3. Potential Confounders to the Hospitalization-Air Pollution Association
2.4. Annual Hierarchical Model
2.5. Sensitivity Analysis
3. Results
3.1. Trends in Annual Data
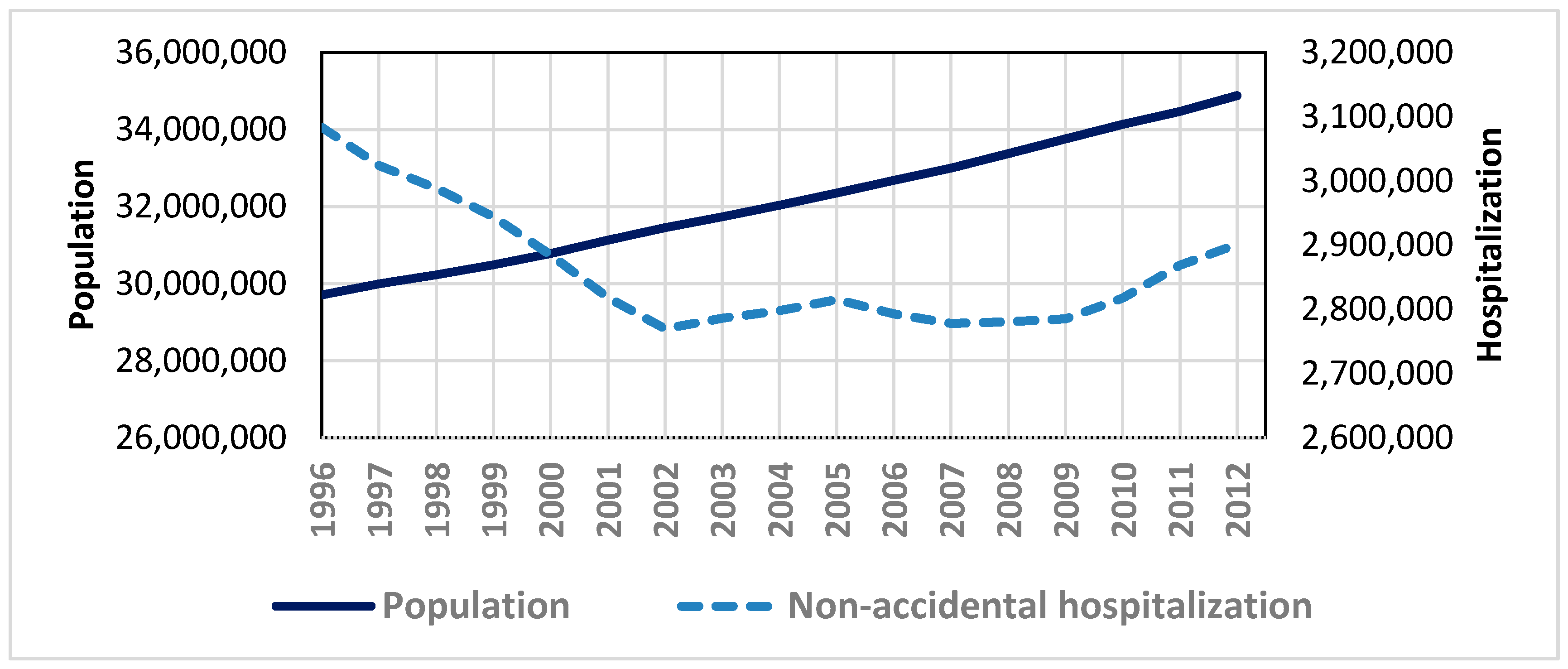
3.1.1. Population and Hospitalization
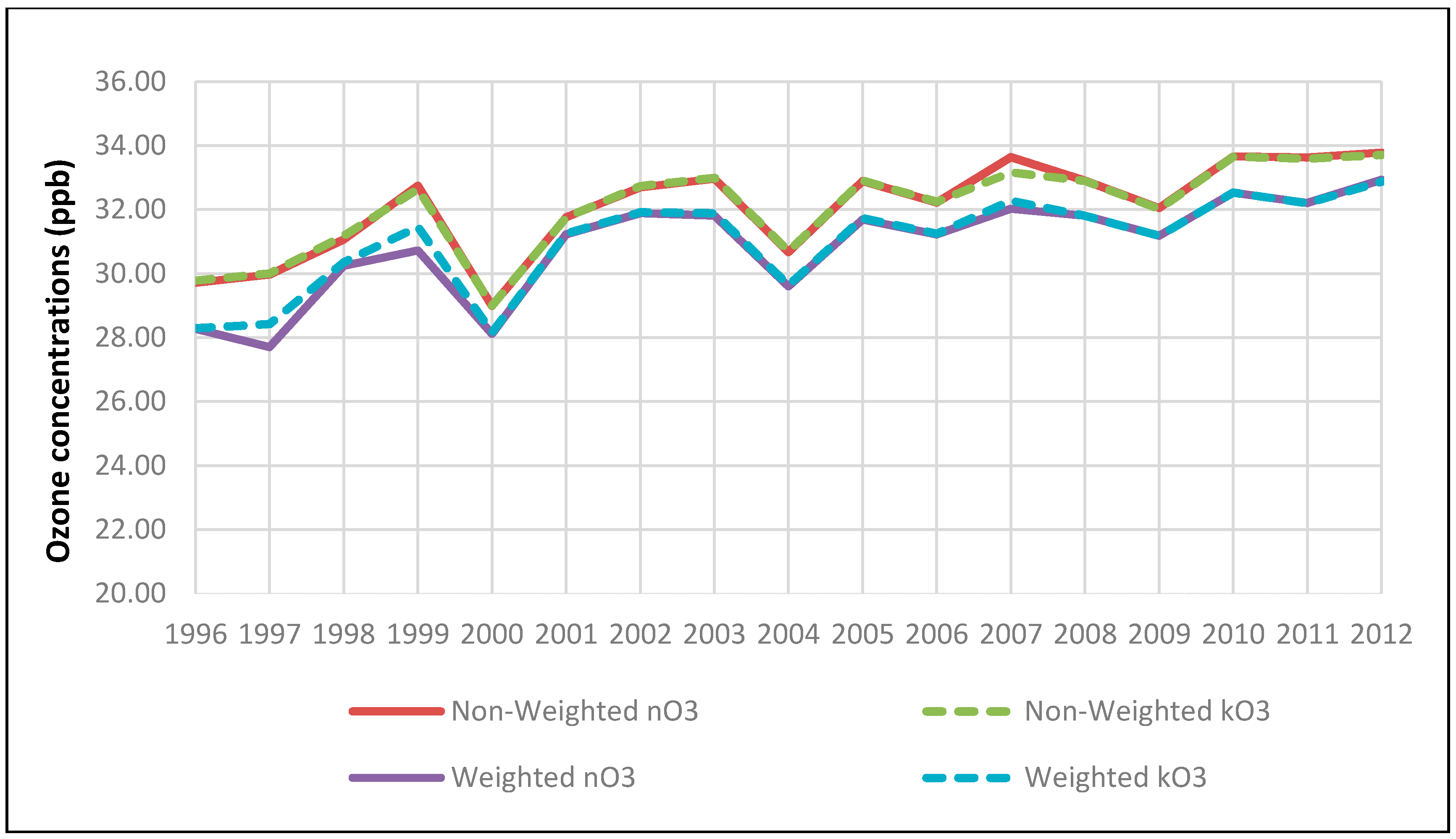
3.1.2. Trend in Ozone Concentrations
3.2. Trends in Relative Risk of Circulatory Hospitalizations by Age and Sex
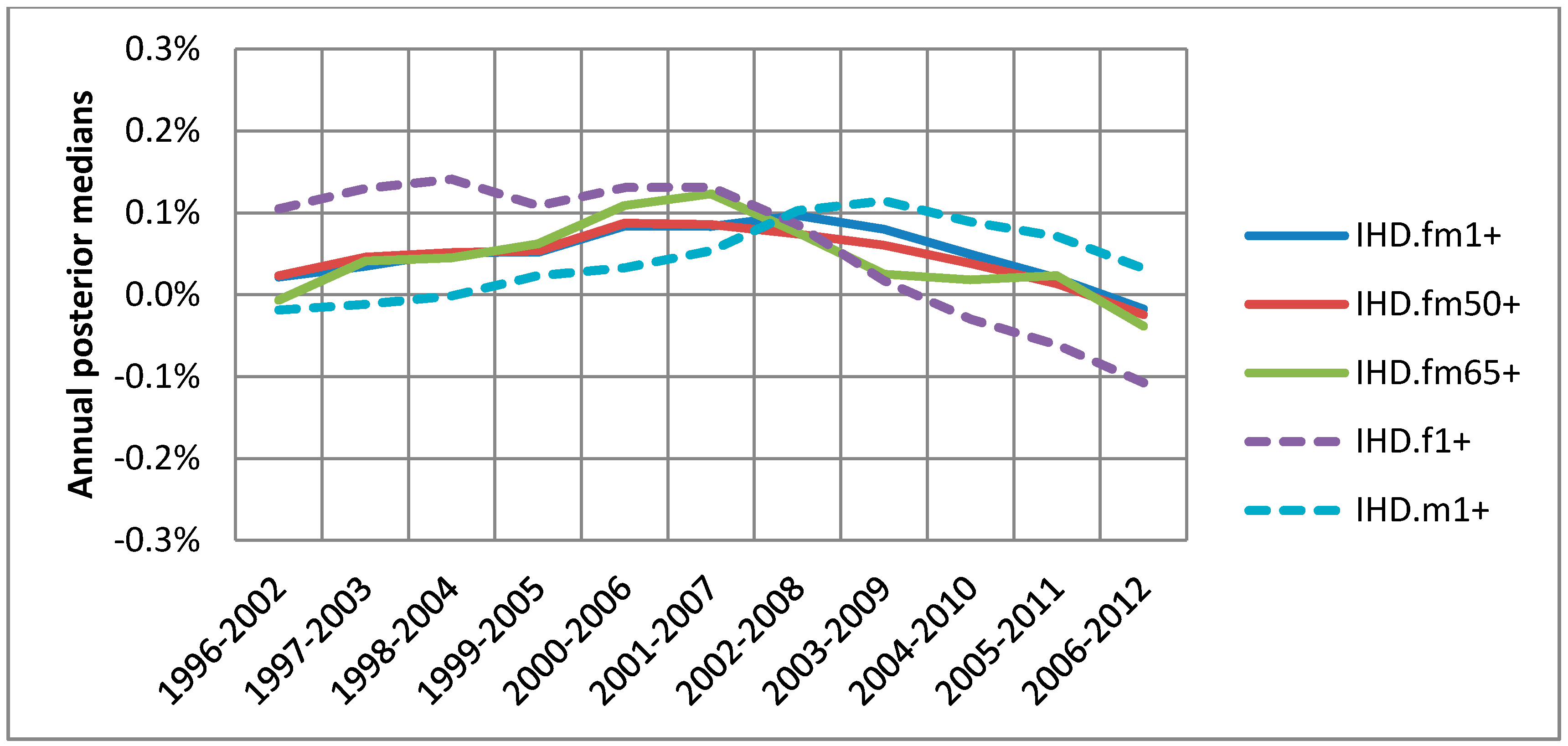
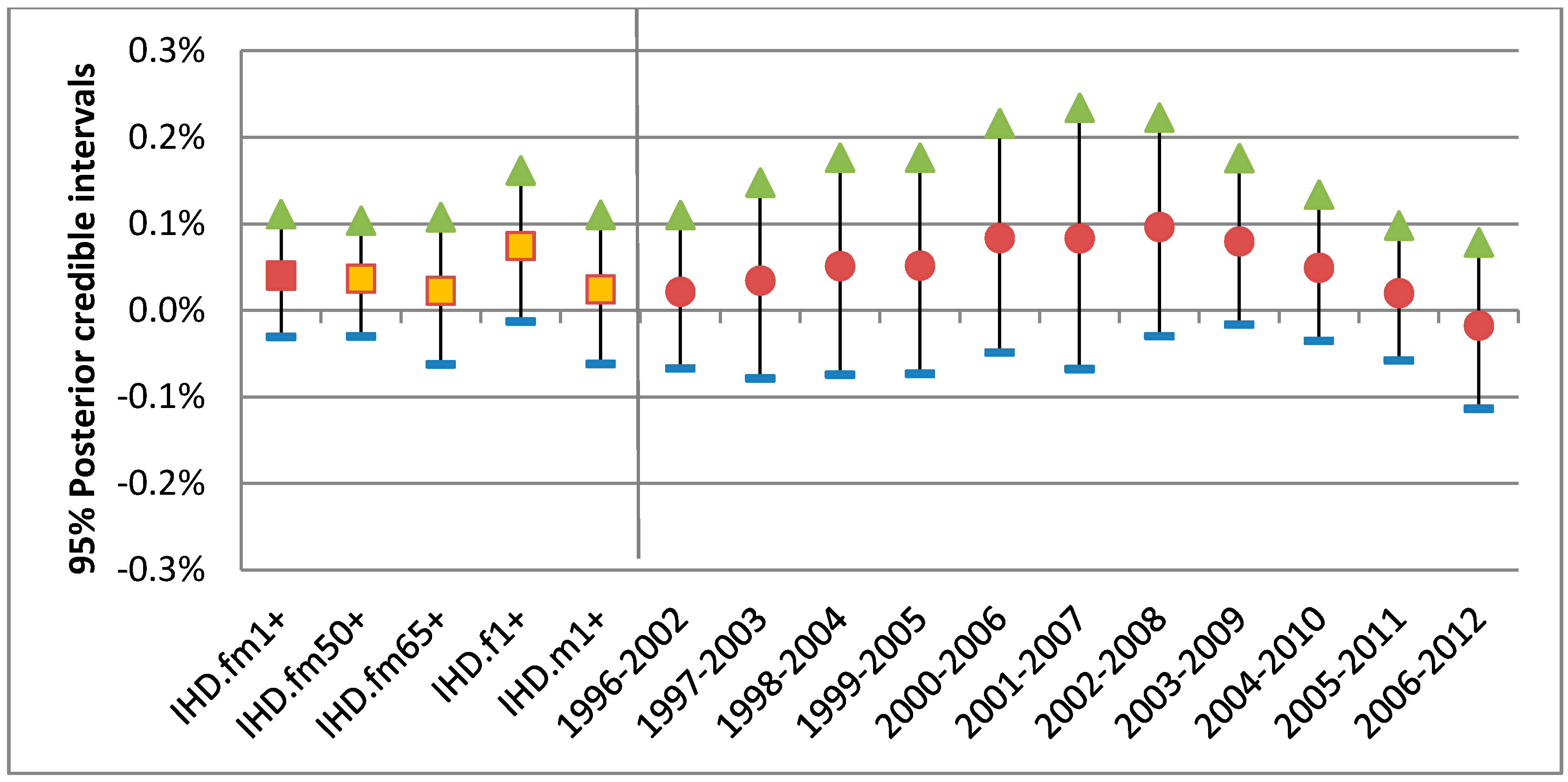
3.2.1. Trend in Ozone-IHD Associations
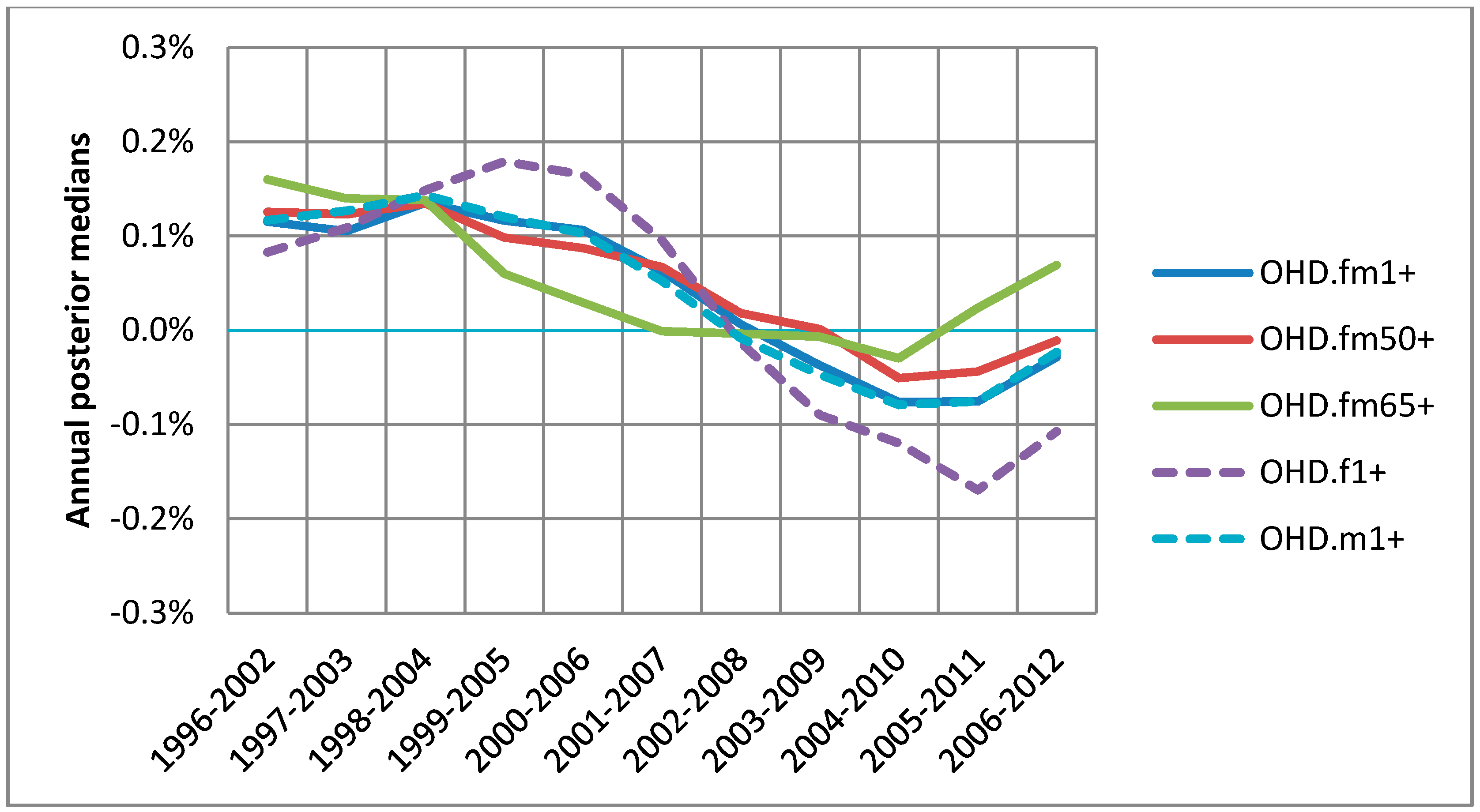
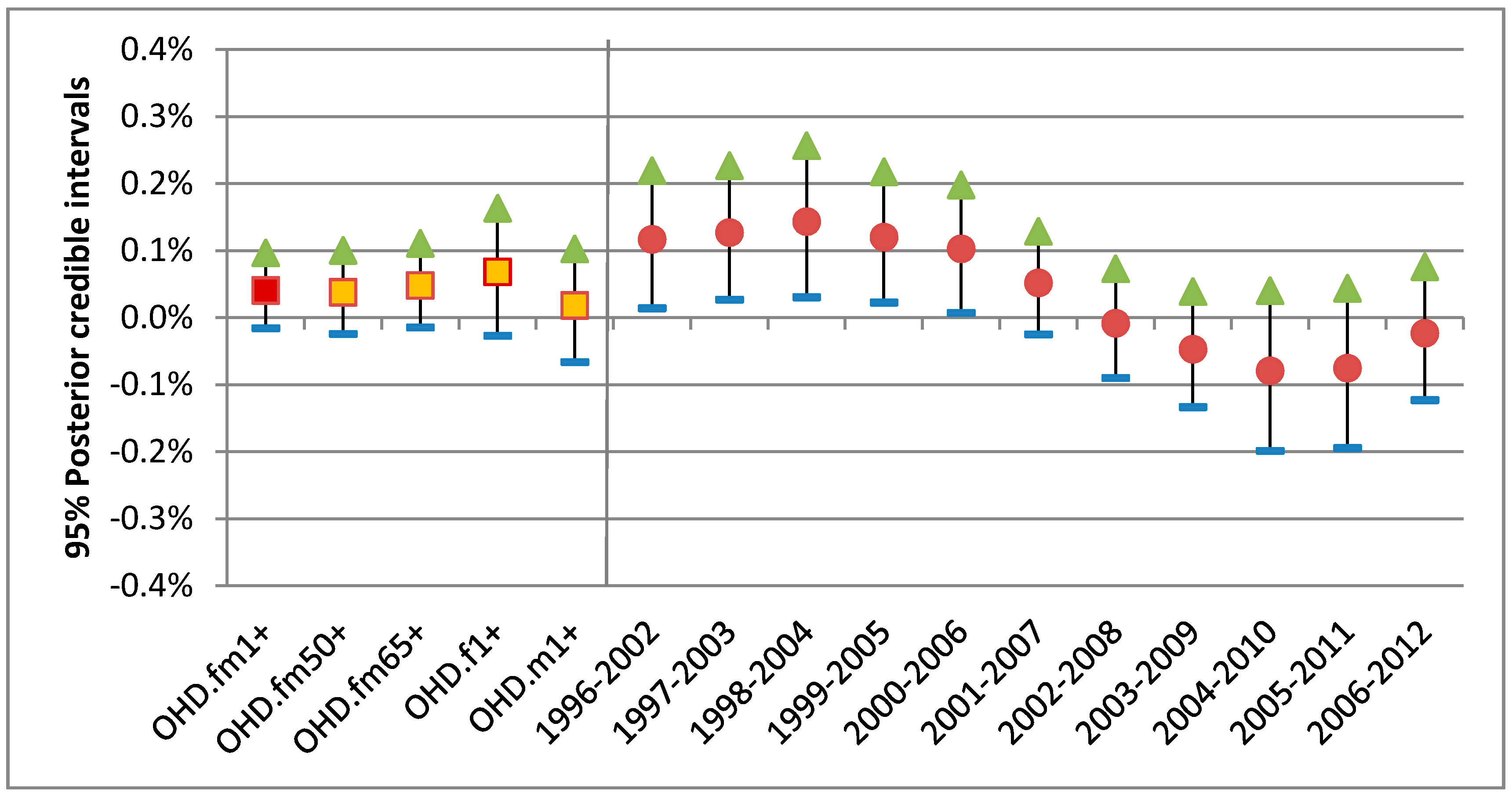
3.2.2. Trend in Ozone-OHD Associations
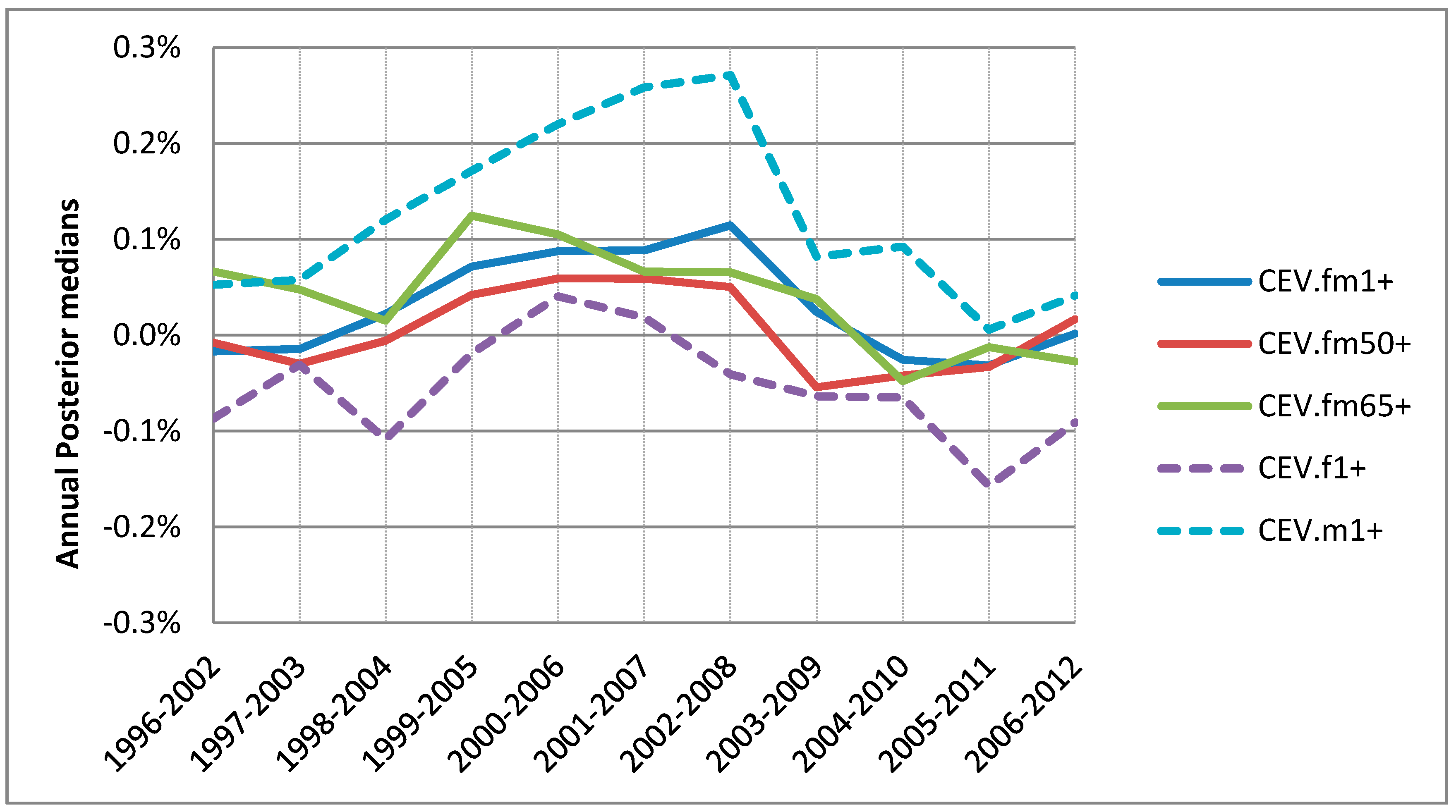
3.2.3. Trend in Ozone-CEV Associations
4. Discussion
4.1. Air Health Indicator with Trend
- Is the observed decline true, and not model-related?
- Why do the concentrations and adverse effects of ozone for recent years show opposite time trends?
- Are there some other confounders that led to declines for recent years?
- Further investigations are necessary to be able to answer these questions.
4.2. Little Difference by Age
4.3. Noticeable Sex-Specific Differences
4.4. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- McDonnell, W.F.; Abbey, D.E.; Nishino, N.; Lebowitz, M.D. Long-term ambient ozone concentration and the incidence of asthma in nonsmoking adults: The AHSMOG Study. Environ. Res. 1999, 80, 110–121. [Google Scholar] [CrossRef] [PubMed]
- Henrotin, J.-B.; Besancenot, J.-P.; Bejot, Y.; Giroud, M. Short-term effects of ozone air pollution on ischaemic stroke occurrence: A case-crossover analysis from a 10-year population-based study in Dijon, France. Occup. Environ. Med. 2007, 64, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.C.; Lee, J.T.; Kim, H.; Kwon, H.J. Air pollution: A new risk factor in ischemic stroke mortality. Stroke 2002, 33, 2165–2169. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Dominici, F.; Samet, J.M. A Meta-Analysis of Time-Series Studies of Ozone and Mortality with Comparison to the National Morbidity, Mortality, and Air Pollution Study. Epidemiology 2005, 16, 436–445. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A.; Burnett, R.T.; Thurston, G.D.; Thun, M.J.; Calle, E.E.; Krewski, D.; Godleski, J.J. Cardiovascular mortality and long-term exposure to particulate air pollution: Epidemiological evidence of general pathophysiological pathways of disease. Circulation 2004, 109, 71–77. [Google Scholar] [CrossRef] [PubMed]
- McConnell, R.; Berhane, K.; Gilliland, F.; London, S.J.; Islam, T.; Gauderman, W.J.; Avol, E.; Margolis, H.G.; Peters, J.M. Asthma in exercising children exposed to ozone: A cohort study. Lancet 2002, 359, 386–391. [Google Scholar] [CrossRef]
- Sunyer, J.; Basagana, X.; Belmonte, J.; Anto, J.M. Effect of nitrogen dioxide and ozone on the risk of dying in patients with severe asthma. Thorax 2002, 57, 687–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, M.L.; McDermott, A.; Zeger, S.L.; Samet, J.M.; Dominici, F. Ozone and short-term mortality in 95 US urban communities, 1987–2000. JAMA 2004, 292, 2372–2378. [Google Scholar] [CrossRef] [PubMed]
- Guo, P.; Wang, Y.; Feng, W.; Wu, J.; Fu, C.; Deng, H.; Huang, J.; Wang, L.; Zheng, M.; Liu, H. Ambient Air Pollution and Risk for Ischemic Stroke: A Short-Term Exposure Assessment in South China. Int. J. Environ. Res. Public Health 2017, 14, 1091. [Google Scholar] [CrossRef] [PubMed]
- Ruidavets, J.B.; Cournot, M.; Cassadou, S.; Giroux, M.; Meybeck, M.; Ferrières, J. Ozone air pollution is associated with acute myocardial infarction. Circulation 2005, 111, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Peters, A.; Dockery, D.W.; Muller, J.E.; Mittleman, M.A. Increased particulate air pollution and the triggering of myocardial infarction. Circulation 2001, 103, 2810–2815. [Google Scholar] [CrossRef] [PubMed]
- Ren, C.; Williams, G.M.; Morawska, L.; Mengersen, K.; Tong, S. Ozone modifies associations between temperature and cardiovascular mortality: Analysis of the NMMAPS data. Occup. Environ. Med. 2008, 65, 255–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, R.; Brook, R.; Bard, R.; Conner, T.; Shin, H.; Burnett, R. Impact of personal and ambient-level exposures to nitrogen dioxide and particulate matter on cardiovascular function. Int. J. Environ. Health Res. 2012, 22, 71–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, M.L.; Peng, R.D.; Dominici, F. The exposure–response curve for ozone and risk of mortality and the adequacy of current ozone regulations. Environ. Health Perspect. 2006, 114, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Stieb, D.M.; Judek, S.; Burnett, R.T. Meta-analysis of time-series studies of air pollution and mortality: Effects of gases and particles and the influence of cause of death, age, and season. J. Air Waste Manag. Assoc. 2002, 52, 470–484. [Google Scholar] [CrossRef] [PubMed]
- Prueitt, R.L.; Lynch, H.N.; Zu, K.; Sax, S.N.; Venditti, F.J.; Goodman, J.E. Weight-of-evidence evaluation of long-term ozone exposure and cardiovascular effects. Crit. Rev. Toxicol. 2014, 44, 791–822. [Google Scholar] [CrossRef] [PubMed]
- Hastie, T.; Tibshirani, R. Generalized Additive Models. Stat. Sci. 1986, 1, 297–318. [Google Scholar] [CrossRef]
- Hastie, T.J.; Tibshirani, R.J. Generalized Additive Models, 1st ed.; Chapman & Hall: New York, NY, USA, 1990; ISBN 0-412-34390-8. [Google Scholar]
- Dominici, F.; Samet, J.M.; Zeger, S.L. Combining evidence on air pollution and daily mortality from the 20 largest US cities: A hierarchical modelling strategy. J. R. Stat. Soc. Ser. A Stat. Soc. 2000, 163, 263–302. [Google Scholar] [CrossRef]
- Chen, K.; Zhou, L.; Chen, X.; Bi, J.; Kinney, P.L. Acute effect of ozone exposure on daily mortality in seven cities of Jiagsu Province, China: No clear evidence for threshold. Environ. Res. 2017, 155, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.H.; Burnett, R.; Stieb, D.; Takahara, G.; Brion, O.; Smith-Doiron, M.; Jessiman, B. E-034: Temporal trend in cardio-pulmonary mortality risks associated with ozone of warm season in Canada. Epidemiology 2012, 23. [Google Scholar] [CrossRef]
- Shah, A.S.; Lee, K.K.; McAllister, D.A.; Hunter, A.; Nair, H.; Whiteley, W.; Langrish, J.P.; Newby, D.E.; Mills, N.L. Short term exposure to air pollution and stroke: Systematic review and meta-analysis. BMJ 2015, 350, h1295. [Google Scholar] [CrossRef] [PubMed]
- Montresor-López, J.A.; Yanosky, J.D.; Mittleman, M.A.; Sapkota, A.; He, X.; Hibbert, J.D.; Wirth, M.D.; Puett, R.C. Short-term exposure to ambient ozone and stroke hospital admission: A case-crossover analysis. J. Expos. Sci. Environ. Epidemiol. 2016, 26, 162. [Google Scholar] [CrossRef] [PubMed]
- Auriba, R. Short-Term Exposure to Ozone in Relation to Mortality and Out-of-Hospital Cardiac Arrest: Exploring Sensitive Subgroups by Previous Hospitalization. Ph.D. Thesis, Karolinska Institutet, Solna, Sweden, 2018. [Google Scholar]
- Liu, H.; Tian, Y.; Song, J.; Cao, Y.; Xiang, X.; Huang, C.; Li, M.; Hu, Y. Effect of ambient air pollution on hospitalization for heart failure in 26 of China’s largest cities. Am. J. Cardiol. 2018, 121, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Carugno, M.; Consonni, D.; Randi, G.; Catelan, D.; Grisotto, L.; Bertazzi, P.A.; Biggeri, A.; Baccini, M. Air pollution exposure, cause-specific deaths and hospitalizations in a highly polluted Italian region. Environ. Res. 2016, 147, 415–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gan, W.Q.; FitzGerald, J.M.; Carlsten, C.; Sadatsafavi, M.; Brauer, M. Associations of ambient air pollution with chronic obstructive pulmonary disease hospitalization and mortality. Am. J. Respir. Crit. Care Med. 2013, 187, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Canadian Smog Science Assessment Volume 2: Health Effects. 2013. Available online: http://publications.gc.ca/collections/collection_2014/sc-hc/En88-5-2-2013-eng.pdf (accessed on 22 April 2018).
- US Environmental Protection Agency. Health Risk and Exposure Assessment for Ozone Final Report 2014. Available online: https://www3.epa.gov/ttn/naaqs/standards/ozone/data/20140829healthrea.pdf (accessed on 22 April 2018).
- Filleul, L.; Cassadou, S.; Médina, S.; Fabres, P.; Lefranc, A.; Eilstein, D.; Le Tertre, A.; Pascal, L.; Chardon, B.; Blanchard, M.; et al. The relation between temperature, ozone, and mortality in nine French cities during the heat wave of 2003. EHP 2006, 114, 1344–1347. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.H.; Stieb, D.M.; Jessiman, B.; Goldberg, M.S.; Brion, O.; Brook, J.; Ramsay, T.; Burnett, R.T. A Temporal, Multi-City Model to Estimate the Effects of Short-Term Exposure to Ambient Air Pollution on Health. EHP 2008, 116, 1147–1153. [Google Scholar] [CrossRef] [PubMed]
- Shin, H.H.; Burnett, R.T.; Stieb, D.M.; Jessiman, B. Measuring public health accountability of air quality management. Air Qual. Atmos. Health 2009, 2, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Shin, H.H.; Stieb, D.; Burnett, R.; Takahara, G.; Jessiman, B. Tracking national and regional spatial-temporal mortality risk associated with NO2 concentrations in Canada: A Bayesian hierarchical two-level model. Risk Anal. 2012, 32, 513–530. [Google Scholar] [CrossRef] [PubMed]
- Burr, W.S.; Takahara, G.; Shin, H.H. Bias correction in estimation of public health risk attributable to short-term air pollution exposure. Environmetrics 2015, 26, 298–311. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. ICD-10 Classifications of Mental and Behavioural Disorder: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- Environment Canada. National Climate Data and Information Archive Historical Data. Available online: http://climate.weather.gc.ca/historical_data/search_historic_data_e.html (accessed on 24 April 2018).
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; ISBN 3-900051-07-0. [Google Scholar]
- Burr, W.S. Air Pollution and Health: Time Series Tools and Analysis. Ph.D. Thesis, Queen’s University, Kingston, ON, Canada, 2012. [Google Scholar]
- Matz, C.J.; Stieb, D.M.; Davis, K.; Egyed, M.; Rose, A.; Chou, B.; Brion, O. Effects of age, season, gender and urban-rural status on time-activity: Canadian Human Activity Pattern Survey 2 (CHAPS 2). Int. J. Environ. Res. Public Health 2014, 11, 2108–2124. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency. Air Quality Criteria for Ozone and Related Photochemical Oxidants. Final Report; 2006. Available online: http://cfpub.epa.gov/ncea/cfm/recordisplay.cfm?deid=149923 (accessed on 22 April 2018).
- Sawyer, K.; Brown, J.; Hazucha, M.; Bennett, W.D. The effect of exercise on nasal uptake of ozone in healthy human adults. J. Appl. Physiol. 2007, 102, 1380–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuller, C.H.; Feeser, K.R.; Sarnat, J.A.; O’Neill, M.S. Air pollution, cardiovascular endpoints and susceptibility by stress and material resources: A systematic review of the evidence. Environ. Health 2017, 16, 58. [Google Scholar] [CrossRef] [PubMed]
- Alexeeff, S.E.; Litonjua, A.A.; Wright, R.O.; Baccarelli, A.; Suh, H.; Sparrow, D.; Vokonas, P.S.; Schwartz, J. Ozone exposure, antioxidant genes, and lung function in an elderly cohort: VA normative aging study. Occup. Environ. Med. 2008, 65, 736–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buadong, D.; Jinsart, W.; Funatagawa, I.; Karita, K.; Yano, E. Association between PM10 and O3 levels and hospital visits for cardiovascular diseases in Bangkok, Thailand. J. Epidemiol. 2009, 19, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Halonen, J.I.; Lanki, T.; Tiittanen, P.; Niemi, J.V.; Loh, M.; Pekkanen, J. Ozone and cause-specific cardiorespiratory morbidity and mortality. J. Epidemiol. Community Health 2009, 64, 814–820. [Google Scholar] [CrossRef] [PubMed]
- Medina-Ramón, M.; Schwartz, J. Who is more vulnerable to die from ozone air pollution? Epidemiology 2008, 19, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Zanobetti, A.; Schwartz, J. Is there adaptation in the ozone mortality relationship: A multi-city case-crossover analysis. Environ. Health 2008, 7, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Middleton, N.; Yiallouros, P.; Kleanthous, S.; Kolokotroni, O.; Schwartz, J.; Dockery, D.W.; Demokritou, P.; Koutrakis, P. A 10-year time-series analysis of respiratory and cardiovascular morbidity in Nicosia, Cyprus: The effect of short-term changes in air pollution and dust storms. Environ. Health 2008, 7, 39. [Google Scholar] [CrossRef] [PubMed]
- Villeneuve, P.J.; Chen, L.; Stieb, D.; Rowe, B.H. Associations between outdoor air pollution and emergency department visits for stroke in Edmonton, Canada. Eur. J. Epidemiol. 2006, 21, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.; Sarnat, J.; Suh, H.; Coull, B.; Koutrakis, P. Factors influencing relationships between personal and ambient concentrations of gaseous and particulate pollutants. Sci. Total Environ. 2009, 407, 3754–3765. [Google Scholar] [CrossRef] [PubMed]
- Klepeis, N.E. An Introduction to the Indirect Exposure Assessment Approach: Modeling Human Exposure Using Microenvironmental Measurements and the Recent National Human Activity Pattern Survey. Environ. Health Perspect. 1999, 107, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Zeger, S.L.; Thomas, D.; Dominici, F.; Samet, J.M.; Schwartz, J.; Dockery, D.; Cohen, A. Exposure measurement error in time-series studies of air pollution: Concepts and consequences. Environ. Health Perspect. 2000, 108, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Dominici, F. Effect modification by community characteristics on the short-term effects of ozone exposure and mortality in 98 US communities. Am. J. Epidemiol. 2008, 167, 986–997. [Google Scholar] [CrossRef] [PubMed]
- Medina-Ramon, M.; Zanobetti, A.; Schwartz, J. The effect of ozone and PM10 on hospital admissions for pneumonia and chronic obstructive pulmonary disease: A national multicity study. Am. J. Epidemiol. 2006, 163, 579–588. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| City Name (East to West) | Pop. in 1000 1996–2012 (Trend %) 1 | Pop. 50 ≤ Age < 65 in 1000 1996–2012 (Trend %) 1 | Pop. Aged > 65 in 1000 1996–2012 (Trend %) 1 | Female Aged > 65 in 1000 1996–2012 (Trend %) 1 | Males Aged > 65 in 1000 1996–2012 (Trend %) 1 |
|---|---|---|---|---|---|
| Halifax | 351–407 (16) | 47–85 (81) | 36–54 (51) | 14–24 (64) | 21–30 (43) |
| Saint John | 74–70 (−4) | 10–15 (47) | 11–12 (4) | 4–5 (12) | 7–7 (−1) |
| Quebec | 513–567 (11) | 83–103 (52) | 65–103 (59) | 24–42 (78) | 40–60 (48) |
| Montreal | 1798–1941 (8) | 278–359 (29) | 266–299 (12) | 101–123 (21) | 164–176 (7) |
| Ottawa | 741–924 (25) | 102–184 (80) | 81–123 (52) | 33–54 (64) | 49–69 (43) |
| Durham | 472–636 (35) | 59–130 (120) | 42–79 (87) | 18–35 (94) | 24–44 (81) |
| York | 611–1086 (78) | 85–219 (159) | 50–131 (164) | 22–60 (176) | 28–71 (154) |
| Toronto | 2456–2741 (12) | 350–512 (46) | 324–390 (20) | 135–166 (23) | 189–224 (18) |
| Peel | 879–1365 (55) | 116–255 (120) | 63–146 (134) | 27–67 (148) | 36–80 (123) |
| Halton | 350–528 (51) | 54–99 (85) | 38–71 (85) | 17–31 (87) | 22–40 (84) |
| Hamilton | 481–541 (12) | 69–111 (61) | 67–85 (26) | 28–37 (31) | 39–48 (23) |
| Niagara | 415–444 (7) | 64–97 (52) | 65–85 (29) | 28–37 (35) | 38–47 (26) |
| Waterloo | 417–530 (27) | 54–100 (86) | 45–67 (49) | 18–29 (62) | 27–37 (41) |
| Windsor | 204–218 (7) | 28–43 (51) | 29–35 (18) | 12–15 (28) | 18–20 (12) |
| Sarnia | 75–74 (−1) | 11–17 (51) | 11–14 (29) | 5–6 (33) | 7–8 (26) |
| London | 335–382 (14) | 44–76 (73) | 41–56 (37) | 17–24 (44) | 25–32 (32) |
| Sudbury | 170–165 (−3) | 25–36 (44) | 20–27 (35) | 9–12 (36) | 11–15 (35) |
| Sault Ste. Marie | 82–76 (−7) | 13–18 (37) | 11–15 (33) | 5–7 (37) | 6–9 (30) |
| Winnipeg | 629–690 (10) | 83–135 (62) | 85–98 (15) | 34–41 (23) | 52–57 (9) |
| Regina | 186–206 (11) | 23–39 (62) | 22–27 (22) | 9–11 (27) | 13–16 (18) |
| Saskatoon | 199–239 (20) | 23–43 (86) | 23–29 (29) | 9–12 (33) | 14–17 (27) |
| Calgary | 789–1179 (50) | 95–217 (129) | 69–116 (67) | 29–51 (75) | 40–65 (62) |
| Edmonton | 632–869 (38) | 80–159 (98) | 69–99 (44) | 29–43 (49) | 40–56 (41) |
| Vancouver | 1905–2408 (26) | 263–483 (84) | 221–327 (48) | 93–149 (60) | 128–178 (40) |
| City Name | Number in 1000s of Circ 1996–2012 (trend, %) 1 | Number in 1000s of IHD 1996–2012 (trend, %) 1 | Number in 1000s of OHD 1996–2012 (trend, %) 1 | Number in 1000s of CEV 1996–2012 (trend, %) 1 |
|---|---|---|---|---|
| Halifax | 4.1–2.9 (−28) | 1.8–1.1 (−39) | 1.05–1.02 (−3) | 0.5–0.4 (−24) |
| Saint John | 1.2–0.9 (−25) | 0.4–0.3 (−36) | 0.3–0.4 (23) | 0.2–0.1 (−50) |
| Quebec | 8.3–6.8 (−18) | 3.2–2.2 (−31) | 1.9–2.5 (34) | 1.3–0.7 (−48) |
| Montreal | 29.2–20.5 (−30) | 10.0–6.0 (−40) | 7.2–7.4 (2) | 5.1–3.2 (−38) |
| Ottawa | 7.8–6.0 (−23) | 3.4–2.1 (−39) | 1.8–2.3 (27) | 1.3–0.9 (−30) |
| Durham | 3.8–2.9 (−22) | 1.5–0.9 (−38) | 1.13–1.15 (2) | 0.53–0.52 (−0.2) |
| York | 3.0–4.5 (51) | 1.1–1.7 (57) | 0.9–1.7 (87) | 0.6–0.7 (17) |
| Toronto | 32.0–22.3 (−30) | 12.7 –7.8 (−38) | 8.9–8.4 (−5) | 5.0–3.2 (−36) |
| Peel | 5.0–8.0 (61) | 1.8–3.3 (78) | 1.3–2.6 (94) | 0.8–1.1 (34) |
| Halton | 3.5–2.9 (−17) | 1.3–0.9 (−35) | 1.1–1.3 (16) | 0.5–0.4 (−20) |
| Hamilton | 7.1–5.5 (−22) | 3.1–1.7 (−47) | 1.9–2.3 (25) | 1.0–0.8 (−22) |
| Niagara | 6.7–4.1 (−39) | 2.6–1.4 (−46) | 2.1–1.6 (−22) | 1.0–0.6 (−38) |
| Waterloo | 4.2–2.9 (−31) | 1.4–1.1 (−25) | 1.3–1.0 (−18) | 0.7–0.5 (−30) |
| Windsor | 3.3–2.0 (−40) | 1.0–0.7( −31) | 1.1–0.7 (−30) | 0. 7–0.3 (−54) |
| Sarnia | 1.4–0.9 (−38) | 0.6–0.3 (−51) | 0.42–0.36 (−13) | 0.2–0.1 (−47) |
| London | 3.6–2.9 (−20) | 1.4–0.8 (−41) | 0.9–1.1 (24) | 0. 6–0.5 (−16) |
| Sudbury | 2.8–2.0 (−29) | 1.2–0.8 (−30) | 0.67–0.68 (2) | 0.3–0.2 (−32) |
| Sault Ste. Marie | 1.2–1.1 (−9) | 0.5–0.4 (−20) | 0.4–0.5 (17) | 0.2–0.1 (−17) |
| Winnipeg | 7.8–5.7 (−26) | 2.7–2.0 (−25) | 2.2–2.0(−8) | 1.5–0.9 (−35) |
| Regina | 1.8–2.1 (17) | 0.6–0.5 (−16) | 0.7–1.0 (44) | 0.2–0.3 (21) |
| Saskatoon | 2.6–2.2 (−16) | 0.9–0.6 (−27) | 0.8–0.9 (11) | 0.4–0. 3 (−31) |
| Calgary | 7.4–7.2 (−2) | 2.9–2.3 (−21) | 2.1–2.8 (32) | 0.99–1.03 (4) |
| Edmonton | 5.4–5.3 (−1) | 2.1–1.6 (−20) | 1.3–1.9 (55) | 0.8–0.9 (13) |
| Vancouver | 21.5–18.0 (−16) | 7.7–5.6 (−28) | 6.71–6.75 (1) | 3.4–3.0 (−11) |
| City Name | Number of NAPS 1 | Data Availability (%) 2 | Ozone Range (ppb) | Temperature Range (°C) | ||
|---|---|---|---|---|---|---|
| Mean 3 | Range 4 | Mean 5 | Range 6 | |||
| Halifax | 5 | 87.4 | 30.2 | 23.4–35.8 | 13.4 | 12.5–14.9 |
| Saint John | 4 | 100 | 33.0 | 29.2–37.4 | 12.5 | 11.5–13.5 |
| Quebec | 6 | 100 | 33.9 | 29.8–38.8 | 14.4 | 12.8–15.7 |
| Montreal | 14 | 100 | 35.0 | 29.8–39.4 | 16.4 | 15.0–17.4 |
| Ottawa | 3 | 99.4 | 36.2 | 27.2–41.2 | 16.1 | 14.9–17.3 |
| Durham | 2 | 96.8 | 41.4 | 36.7–47.6 | 15.6 | 14.3–16.9 |
| York | 2 | 93.2 | 47.4 | 42.5–53.3 | 15.9 | 14.4–17.0 |
| Toronto | 11 | 99.9 | 41.6 | 35.3–46.2 | 16.9 | 15.1–18.2 |
| Peel | 4 | 98.0 | 44.1 | 40.7–47.8 | 16.5 | 14.3–18.0 |
| Halton | 3 | 99.8 | 45.1 | 40.6–51.1 | 16.6 | 15.2–17.8 |
| Hamilton | 4 | 98.6 | 43.6 | 37.5–50.5 | 16.2 | 14.9–17.3 |
| Niagara | 2 | 95.7 | 45.2 | 38.5–51.7 | 16.9 | 15.4–18.0 |
| Waterloo | 2 | 97.3 | 46.1 | 41.4–53.2 | 15.6 | 14.1–16.8 |
| Windsor | 3 | 98.6 | 47.9 | 40.3–54.2 | 17.9 | 16.4–19.2 |
| Sarnia | 2 | 97.6 | 47.0 | 40.1–53.1 | 16.6 | 15.2–17.9 |
| London | 3 | 98.0 | 46.7 | 40.9–53.5 | 16.4 | 14.6–17.5 |
| Sudbury | 2 | 98.0 | 41.3 | 36.6–46.4 | 14.0 | 12.8–15.3 |
| Sault Ste. Marie | 3 | 99.6 | 40.8 | 37.1–43.7 | 12.8 | 11.1–14.0 |
| Winnipeg | 2 | 99.9 | 33.4 | 28.1–40.1 | 15.4 | 13.3–17.0 |
| Regina | 2 | 97.7 | 34.9 | 25.4–40.4 | 13.1 | 11.5–14.4 |
| Saskatoon | 1 | 92.8 | 31.5 | 20.7–39.5 | 13.2 | 11.8–14.6 |
| Calgary | 4 | 100 | 36.1 | 32.3–40.3 | 11.0 | 9.8–12.3 |
| Edmonton | 9 | 100 | 38.8 | 33.6–43.0 | 12.1 | 11.1–14.1 |
| Vancouver | 21 | 100 | 28.9 | 26.5–31.0 | 14.5 | 13.4–15.9 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, H.H.; Burr, W.S.; Stieb, D.; Haque, L.; Kalayci, H.; Jovic, B.; Smith-Doiron, M. Air Health Trend Indicator: Association between Short-Term Exposure to Ground Ozone and Circulatory Hospitalizations in Canada for 17 Years, 1996–2012. Int. J. Environ. Res. Public Health 2018, 15, 1566. https://doi.org/10.3390/ijerph15081566
Shin HH, Burr WS, Stieb D, Haque L, Kalayci H, Jovic B, Smith-Doiron M. Air Health Trend Indicator: Association between Short-Term Exposure to Ground Ozone and Circulatory Hospitalizations in Canada for 17 Years, 1996–2012. International Journal of Environmental Research and Public Health. 2018; 15(8):1566. https://doi.org/10.3390/ijerph15081566
Chicago/Turabian StyleShin, Hwashin Hyun, Wesley S. Burr, Dave Stieb, Lani Haque, Harun Kalayci, Branka Jovic, and Marc Smith-Doiron. 2018. "Air Health Trend Indicator: Association between Short-Term Exposure to Ground Ozone and Circulatory Hospitalizations in Canada for 17 Years, 1996–2012" International Journal of Environmental Research and Public Health 15, no. 8: 1566. https://doi.org/10.3390/ijerph15081566
APA StyleShin, H. H., Burr, W. S., Stieb, D., Haque, L., Kalayci, H., Jovic, B., & Smith-Doiron, M. (2018). Air Health Trend Indicator: Association between Short-Term Exposure to Ground Ozone and Circulatory Hospitalizations in Canada for 17 Years, 1996–2012. International Journal of Environmental Research and Public Health, 15(8), 1566. https://doi.org/10.3390/ijerph15081566