Asbestos Exposure and the Mesothelioma Incidence in Poland


Abstract
:1. Introduction
2. Materials and Methods
3. Results
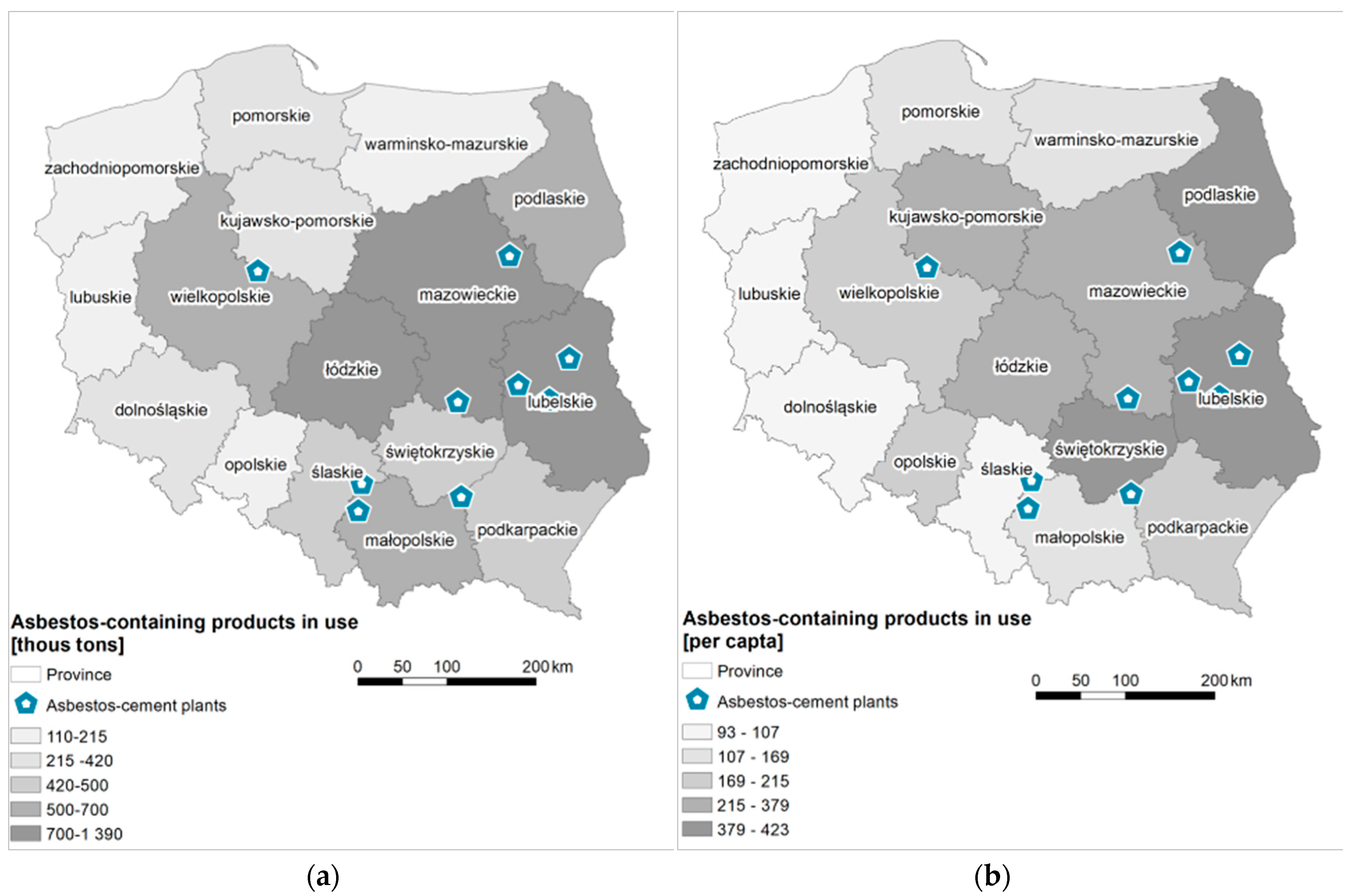
3.1. The Quantity of Asbestos-Cement Products in Use
3.2. Asbestos Manufacturing Plants
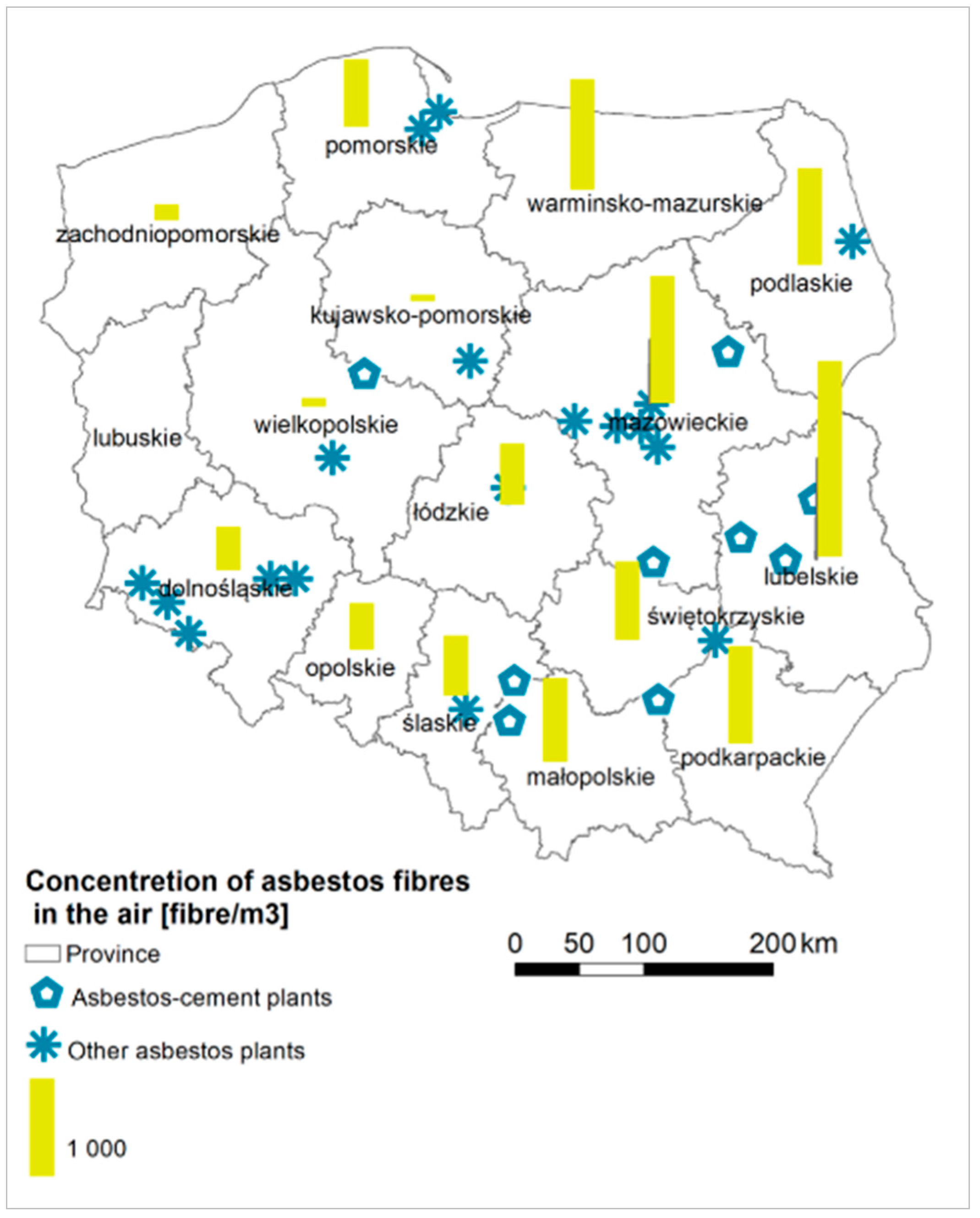
3.3. Concentrations of Asbestos Fibers in the Air
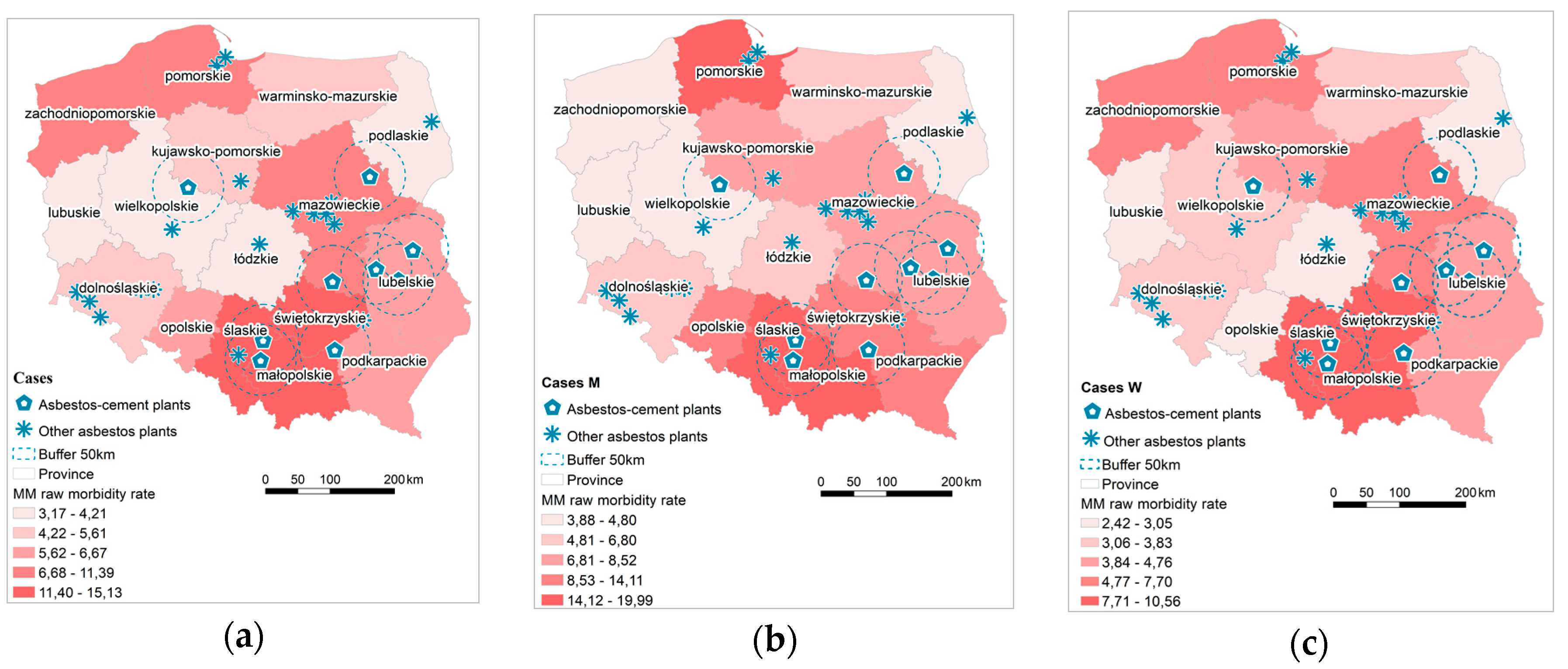
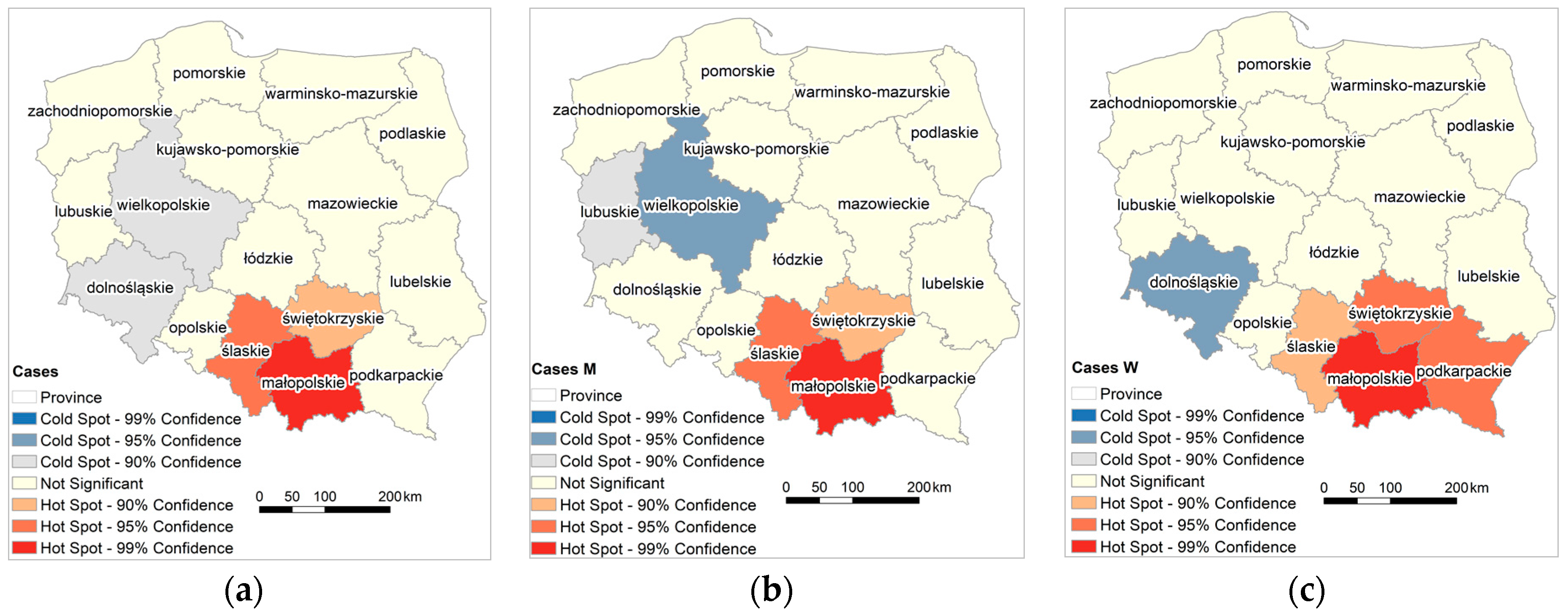
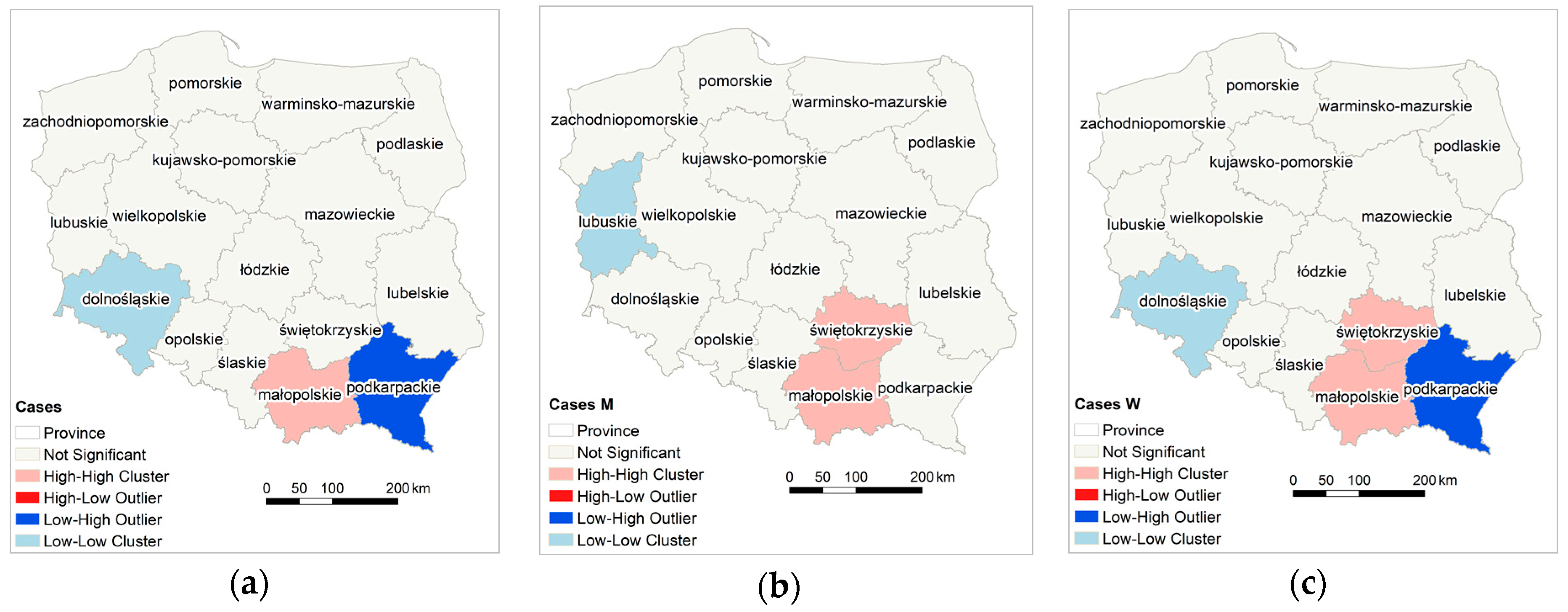
3.4. Malignant Mesothelioma Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Available online: http://www.who.int/news-room/fact-sheets/detail/asbestos-elimination-of-asbestos-related-diseases (accessed on 10 October 2015).
- Hendry, N. The Geology, Occurrences, and Major Uses of Asbestos. Ann. N. Y. Acad. Sci. 1965, 132, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Virta, R. Asbestos: Geology, Mineralogy, Mining, and Uses. Open-File Report 02-149. Available online: https://pubs.usgs.gov/of/2002/of02-149/ (accessed on 10 October 2015).
- Rake, C.; Gilham, C.; Hatch, J.; Darnton, A.; Hodgson, J.; Peto, J. Occupational, domestic and environmental mesothelioma risks in the British population: A case control study. Br. J. Cancer 2009, 100, 1175–1183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, A.D.; Case, B.W.; Churg, A.; Dufresne, A.; Gibbs, G.W.; Sébastien, P.; McDonald, J.C. Mesothelioma in Quebec chrysotile miners and millers: Epidemiology and aetiology. Ann. Occup. Hyg. 1997, 41, 707–719. [Google Scholar] [CrossRef]
- Britton, M. The epidemiology of mesothelioma. Semin. Oncol. 2002, 29, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Hanley, D.; Kess, S.; Yee-Wan, S.; Wilbur, S.; Williams, M. Toxicological Profile for Asbestos; Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2001; pp. 149–185.
- Harper, M.; Butler, C.; Berry, D.; Wroble, J. Where occupation and environment overlap: US forest service worker exposure to libby amphibole fibers. J. Occup. Environ. Hyg. 2015, 12, D47–D53. [Google Scholar] [CrossRef] [PubMed]
- Ledda, C.; Pomara, C.; Bracci, M.; Mangano, D.; Ricceri, V.; Musumeci, A.; Ferrante, M.; Musumeci, G.; Loreto, C.; Fenga, C.; et al. Natural carcinogenic fiber and pleural plaques assessment in a general population: A cross-sectional study. Environ. Res. 2016, 150, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Murray, R. Asbestos: A chronology of its origins and health effects. Br. J. Ind. Med. 1990, 47, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.N.; Cullinan, P.; Blanc, P.; Pickerin, A. Parkes’ Occupational Lung Disorders, 4th ed.; CRC Press: London, UK, 2002; ISBN 9781482240702. [Google Scholar]
- International Agency for Research on Cancer, Arsenic, Metals, Fibres and Dusts. Volume 100c. 2012. Available online: https://monographs.iarc.fr/wp-content/uploads/2018/06/mono100C.pdf (accessed on 25 July 2018).
- McDonald, A.D.; McDonald, J.C. Mesothelioma after crocidolite exposure during gas mask manufacture. Environ. Res. 1978, 17, 340–346. [Google Scholar] [CrossRef]
- McDonald, J.C.; McDonald, A.D. The epidemiology of mesothelioma in historical context. Eur. Respir. J. 1996, 9, 1932–1942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, F.; Sporn, T.A.; Roggli, V.L. Crocidolite and mesothelioma. Ultrastruct. Pathol. 2008, 32, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Ledda, C.; Senia, P.; Rapisarda, V. Biomarkers for early diagnosis and prognosis of malignant pleural mesothelioma: The quest goes on. Cancers 2018, 10, 203. [Google Scholar] [CrossRef] [PubMed]
- IARC Monographs Supplement 7: Asbestos. Available online: http://monographs.iarc.fr/ENG/Monographs/suppl7/Suppl7-20.pdf (accessed on 20 October 2017).
- Donaldson, K.; Brown, R.C.; Brown, G.M. Respirable industrial fibres: Mechanisms of pathogenicity. Thorax 1993, 48, 390–395. [Google Scholar] [CrossRef] [PubMed]
- United Nations Environment Programme, International Labour Organisation, World Health Organization International Programme on Chemical Safety, Environmental Health Criteria 203. Chrysotile Asbestos. Available online: http://www.inchem.org/documents/ehc/ehc/ehc203.htm#partnumber:4 (accessed on 20 October 2017).
- Matsuzaki, H.; Maeda, M.; Lee, S.; Nishimura, Y.; Kumagai-Takei, N.; Hayashi, H.; Yamamoto, S.; Hatayama, T.; Kojima, Y.; Tabata, R.; et al. Asbestos-induced cellular and molecular alteration of immunocompetent cells and their relationship with chronic inflammation and carcinogenesis. J. Biomed. Biotechnol. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, K.; Brown, G.M.; Brown, D.M.; Bolton, R.E.; Davis, J.M.G. Inflammation generating potential of long and short fibre amosite asbestos samples. Br. J. Ind. Med. 1989, 46, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Haegens, A.; Barrett, T.F.; Gell, J.; Shukla, A.; MacPherson, M.; Vacek, P.; Poynter, M.E.; Butnor, K.J.; Janssen-Heininger, Y.M.; Steele, C.; et al. Airway epithelial NF-κB activation modulates asbestos-induced inflammation and mucin production in vivo. J. Immunol. 2007, 178, 1800–1808. [Google Scholar] [CrossRef] [PubMed]
- Ledda, C.; Caltabiano, R.; Loreto, C.; Cinà, D.; Senia, P.; Musumeci, A.; Ricceri, V.; Pomara, C.; Rapisarda, V. Prevalence of anti-nuclear autoantibodies in subjects exposed to natural asbestiform fibers: A cross-sectional study. J. Immunotoxicol. 2018, 15, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Kodavanti, U.P.; Andrews, D.; Schladweiler, M.C.; Gavett, S.H.; Dodd, D.E.; Cyphert, J.M. Early and delayed effects of naturally occurring asbestos on serum biomarkers of inflammation and metabolism. J. Toxicol. Environ. Health Part A 2014, 77, 1024–1039. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Rivera, V.; Negrete-García, M.C.; Ávila-Moreno, F.; Ortiz-Quintero, B. Secreted and tissue miRNAs as diagnosis biomarkers of malignant pleural mesothelioma. Int. J. Mol. Sci. 2018, 19, 595. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Cancer Control: Knowledge into Action: WHO Guide for Effective Programs. Available online: http://www.who.int/cancer/modules/Prevention%20Module.pdf?ua=1 (accessed on 20 October 2017).
- Wagner, J.C.; Sleggs, C.A.; Marchand, P. Diffuse pleural mesothelioma and asbestos exposure in the North Western Cape Province. Br. J. Ind. Med. 1960, 17, 260–271. [Google Scholar] [CrossRef] [PubMed]
- Carbone, M.; Bedrossian, C.W. The pathogenesis of mesothelioma. Semin. Diagn. Pathol. 2006, 23, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Burdorf, A.; Heederik, D. Applying quality criteria to exposure in asbestos epidemiology increases the estimated risk. Ann. Occup. Hyg. 2011, 55, 565–568. [Google Scholar] [CrossRef] [PubMed]
- Huncharek, M. Changing risk groups for malignant mesothelioma. Cancer 1992, 69, 2704–2711. [Google Scholar] [CrossRef] [Green Version]
- Agudo, A.; Gonzalez, C.A.; Bleda, M.J.; Ramirez, J.; Hernandez, S.; Lopez, F.; Calleja, A.; Panades, R.; Turuguet, D.; Escoalr, A.; et al. Occupation and risks of malignant pleural mesothelioma: A case-control study in Spain. Am. J. Ind. Med. 2000, 37, 159–168. [Google Scholar] [CrossRef]
- Neyens, T.; Lawson, A.; Kirby, R.; Nuyts, V.; Watjou, K.; Aregay, M.; Carroll, R.; Nawrot, T.; Faes, C.H. Disease mapping of zero-excessive mesothelioma data in Flanders. Ann. Epidemiol. 2017, 27, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, C.; Giarelli, L.; Grandi, G.; Brollo, A.; Ramani, L.; Zuch, C. Latency periods in asbestos-related mesothelioma of the pleura. Eur. J. Cancer Prev. 1997, 6, 162–166. [Google Scholar] [PubMed]
- Mowe, G.; Gylseth, B.; Hartveit, F.; Skaug, V. Occupational asbestos exposure, lung-fiber concentration and latency time in malignant mesothelioma. Scand. J. Work Environ. Health 1984, 10, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Chouaid, C.; Assié, J.B.; Andujar, P.; Blein, C.; Tournier, C.; Vainchtock, A.; Scherpereel, A.; Monnet, I.; Pairon, J.C. Determinants of malignant pleural mesothelioma survival and burden of disease in France: A national cohort analysis. Cancer Med. 2018, 7, 1102–1109. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B.; Chahinian, A. Mesothelioma, 1st ed.; Martin Dunitz; CRC Press: London, UK, 2002; ISBN 9780203994474. [Google Scholar]
- World Health Organization. Available online: http://apps.who.int/classifications/icd10/browse/2016/en (accessed on 20 October 2017).
- Regulation of the Minister of Economy of December 13, 2010 on the Requirements for the Use of Asbestos-containing Products and the Use and Treatment of Installations or Equipment in Which Asbestos-containing Products Have Been or Are Used. Journal of Law of 2011, No. 8, Item 31. Available online: http://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20110080031 (accessed on 26 February 2016).
- Bianchi, C.; Bianchi, T. Global mesothelioma epidemic: Trend and features. Indian J. Occup. Environ. Med. 2014, 18, 82–88. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Register. Available online: http://onkologia.org.pl (accessed on 10 October 2015).
- Carlin, D.J.; Larson, T.C.; Pfau, J.C.; Gavett, S.H.; Shukla, A.; Miller, A.; Hines, R. Current Research and Opportunities to Address Environmental Exposures. Environ. Health Perspect. 2015, 123, 194–197. [Google Scholar] [CrossRef] [PubMed]
- Krówczyńska, M.; Wilk, E. Aerial imagery and geographic information systems used in the asbestos removal process in Poland. In Proceedings of the 33th EARSeL Symposium Towards Horizon 2020: Earth Observation and Social Perspectives, Matera, Italy, 3–6 June 2013; pp. 823–828. [Google Scholar]
- Local Data Bank of Poland. Available online: https://bdl.stat.gov.pl/BDL (accessed on 26 February 2016).
- Tender Specification GMES Fast Track Service Precursor on Land Monitoring. High Resolution Core Land Cover Data for Built-Up Areas, Including Degree of Soil Sealing. Data Enhancement in Support of Member States Requirements. EEA/SES/09/003. Available online: http://www.eea.europa.eu/about-us/tenders/eea-ses-09-003 (accessed on 26 February 2016).
- Krówczyńska, M.; Soszyńska, A.; Pabjanek, P.; Wilk, E.; Hurbanek, P.; Rosina, K. Accuracy of the Soil Sealing Enhancement Product for Poland. Quest. Geogr. 2016, 35, 89–95. [Google Scholar] [CrossRef] [Green Version]
- Census Mosaic Project, Max Planck Institute for Demographic Research. Available online: http://www.censusmosaic.org/data/historical-gis-files (accessed on 1 March 2015).
- Wilk, E.; Krówczyńska, M.; Zagajewski, B. Asbestos manufacturing plants in Poland. Misc. Geogr. 2014, 18, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Wilk, E.; Krówczyńska, M.; Pabjanek, P.; Mędrzycki, P. Estimation of the amount of asbestos-cement roofing in Poland. Waste Manag. Res. 2017, 35, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Report—Spatial Analyses As a Report on the Actions Taken in the Field of Exposure and Health Protection in the Years 2004–2013; Ministry of Economy: Warsaw, Poland, 2015.
- Tossavainen, A. Asbestos, asbestosis and cancer: The Helsinki criteria for diagnosis and attribution. Scand. J. Work Environ. Health 1997, 23, 311–316. [Google Scholar] [CrossRef]
- Szubert, Z.; Stankiewicz-Choroszucha, B.; Wrońska-Sobolewska, M.; Cwynar, E.; Dobrowolska, J.; Wróbel, R.; Ratka, M.; Jakubowski, J.; Skórska-Ciszewska, I.; Turbańska, R.; et al. Realizacja programu badań profilaktycznych pracowników byłych zakładów przetwórstwa azbestu “Amiantus”. Medycyna Pracy 2011, 62, 465–472. [Google Scholar]
- Tobler, W. Computer Movie Simulating Urban Growth in the Detroit Region. Econ. Geogr. 1970, 46, 234–240. [Google Scholar] [CrossRef]
- Moran, P.A.P. Notes on Continuous Stochastic Phenomena. Biometrika 1950, 37, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Calder, C.A.; Cressie, N. Beyond Moran’s I: Testing for Spatial Dependence Based on the Spatial Autoregressive Model. Geogr. Anal. 2007, 39, 357–375. [Google Scholar] [CrossRef]
- Getis, A.; Ord, J.K. The Analysis of Spatial Association by Use of Distance Statistics. Geogr. Anal. 1992, 24, 189–206. [Google Scholar] [CrossRef]
- Ord, J.K.; Getis, A. Local spatial autocorrelation statistics: Distributional issues and an application. Geogr. Anal. 1995, 27, 286–306. [Google Scholar] [CrossRef]
- Harris, N.L.; Goldman, E.; Gabris, C.; Nordling, J.; Minnemeyer, S.; Ansari, S.; Lippmann, M.; Bennett, L.; Raad, M.; Hansen, M. Using spatial statistics to identify emerging hot spots of forest loss. Environ. Res. Lett. 2017, 12, 024012. [Google Scholar] [CrossRef] [Green Version]
- Anselin, L. Local Indicators of Spatial Association—LISA. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Państwowy Rejestr Granic (PRG). Available online: http://www.codgik.gov.pl/index.php/darmowe-dane/prg.html (accessed on 26 May 2017).
- Krówczyńska, M.; Wilk, E. Geoazbest—Serwis Do Monitorowania Procesu Usuwania Wyrobów Azbestowych. Roczniki Geomatyki 2016, 14, 477–486. Available online: http://rg.ptip.org.pl/index.php/rg/article/view/RG2016-4-KrowczynskaWilk/1649 (accessed on 26 May 2017).
- Krówczyńska, M.; Wilk, E.; Zagajewski, B. The Electronic Spatial Information System—Tools for the monitoring of asbestos in Poland. Misc. Geogr. 2014, 18, 59–64. [Google Scholar] [CrossRef]
- Dyczek, J. Surface of Asbestos-cement (AC) Roof Sheets and Assessment of the Risk of Asbestos Release. In Proceedings of the International Seminar held in AGH on Asbestos Risk Reduction and Measurement of Asbestos Fibre Concentration, Kracow, Poland, 28–29 September 2006; pp. 57–63. [Google Scholar]
- Dyczek, J. Azbest i materiały zawierające azbest. Ocena ryzyka emisji włókien azbestu. In Bezpieczne Postępowanie z Azbestem i Materiałami Zawierającymi azbest; Akademia Górniczo-Hutnicza w Krakowie: Kracow, Poland, 20–21 September 2007; pp. 7–26. [Google Scholar]
- Statistical Yearbook of Foreign Trade for 1958, 1965, 1967, 1970, 1971, 1976, 1978, 1980, 1981, 1985, 1987, 1989–1992. GUS: Warszawa, Poland. Available online: https://stat.gov.pl/en/topics/statistical-yearbooks/statistical-yearbooks (accessed on 26 May 2017).
- Virta, R. Worldwide Asbestos Supply and Consumption Trends from 1900 through 2003, USGS Open-File Report 03-083. Available online: http://pubs.usgs.gov/circ/2006/1298/c1298.pdf (accessed on 10 October 2015).
- World Mineral Production, British Geological Service, 2000s. Available online: http://www.bgs.ac.uk/mineralsuk/statistics/worldArchive.html (accessed on 10 October 2015).
- Act of 19 June 1997 on the Prohibition of the Use of Asbestos-Containing Products. Journal of Laws 1997, No. 101, Item 628, with Later Amendments. Available online: http://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20170002119 (accessed on 26 February 2017).
- Wojciechowska, U.; Didkowska, J. Zachorowania i Zgony na Nowotwory Złośliwe w Polsce. Krajowy Rejestr Nowotworów, Centrum Onkologii—Instytut im. Marii Skłodowskiej—Curie. Available online: http://onkologia.org.pl/raporty/ (accessed on 20 October 2017).
- Rokicki, W.; Rokicki, M.; Wojtacha, J.; Rydel, M. Malignant mesothelioma as a difficult interdisciplinary problem. Kardiochirurgia i Torakochirurgia Polska/Pol. J. Thorac. Cardiovasc. Surg. 2017, 14, 263–267. [Google Scholar] [CrossRef] [PubMed]
- WHO Mortality DataBase. Available online: http://www.who.int/healthinfo/statistics/mortality_rawdata/en/ (accessed on 10 October 2015).
- Szeszenia-Dąbrowska, N.; Sobala, W.; Swiątkowska, B.; Stroszejn-Mrowca, G.; Wilczyńska, U. Environmental asbestos pollution—Situation in Poland. Int. J. Occup. Med. Environ. Health 2012, 25, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Świątkowska, B. Epidemiologiczne dowody skutków kanceorgennego narażenia na pył azbestu w środowisku—Na podstawie przeglądu piśmiennictwa. Probl. Hig. Epidemiol. 2009, 90, 299–305. [Google Scholar]
- Kameda, T.; Takahashi, K.; Kim, R.; Ying, J.; Movahed, M.; Park, E.; Rantanen, J. Asbestos: Use, bans and disease burden in Europe. Bull. World Health Organ. 2014, 92, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Le, G.V.; Takahashi, K.; Karjalainen, A.; Delgermaa, V.; Hoshuyama, T.; Miyamura, Y.; Furuya, S.; Higashi, T.; Pan, G.; Wagner, G. National Use of Asbestos in Relation to Economic Development. Environ. Health Perspect. 2010, 118, 116–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Grisogono, F.M.; Mottana, A. The impact of malignant pleural mesothelioma throughout Italy in the years 1995–2002: A geo-referenced study relating death rate to population distribution. Rend. Fis. Lincei 2009, 20, 117–137. [Google Scholar] [CrossRef]
- Kotela, I.; Bednarenko, M.; Wilk-Frańczuk, M.; Kotela, P.; Wołowiec, B.; Laskowicz, K. The effects of environmental exposition to asbestos dust on health. Przegląd Lekarski 2010, 67, 107–109. [Google Scholar] [PubMed]
- Szeszenia-Dąbrowska, N.; Szymczak, W.; Wilczyńska, U. Występowanie międzybłoniaka opłucnej w Polsce w latach 1980–1993. Przegląd Epidemiologiczny 1996, 50, 447–455. [Google Scholar] [PubMed]
- Van der Borre, L.; Deboosere, P. Asbestos in Belgium: An understimated health risk. The evolution of mesothelioma mortality rates (1969–2009). Int. J. Occup. Environ. Health 2014, 20, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, S.; Rey, G.; Luce, D.; Ilg, A.G.S.; Rolland, P.; Brochard, P.; Imbernon, E.; Goldberg, M. Possible effect on environmental variation in mesothelioma rates. Occup. Environ. Med. 2010, 67, 417–421. [Google Scholar] [CrossRef] [PubMed]
- Fazzo, L.; De Santis, M.; Minelli, G.; Bruno, C.; Zona, A.; Marinaccio, A.; Conti, S.; Comba, P. Pleural mesothelioma mortality and asbestos exposure mapping in Italy. Am. J. Ind. Med. 2012, 55, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Corfiati, M.; Scarselli, A.; Binazzi, A.; Di Mazrio, D.; Verardo, M.; Mirabelli, D.; Gennaro, V.; Mensi, C.; Schallemberg, G.; Merler, E.; et al. Epidemiological patterns of asbestos exposure and spatial clusters of incident cases of malignant mesothelioma from the Italian national registry. BMC Cancer 2015, 15, 286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maule, N.; Magnani, C.; Dalmasso, P.; Mirabelli, D.; Merletti, F.; Biggeri, A. Modeling Mesothelioma Risk Associated with Environmental Asbestos Exposure. Environ. Health Perspect. 2007, 115, 1066–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dockery, D.W.; Pope, C.A.; Xu, X.; Spengler, J.D.; Ware, J.H.; Fay, M.A.; Ferris, B.G., Jr.; Speizer, F.E. An association between air pollution and mortality in six U.S. Cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Kobus, D.; Kostrzewa, J.; Iwanek, J.; Mitosek, G.; Parvi, R. Wyniki Pięcioletniej Oceny Jakości Powietrza w strefach w Polsce. Państwowy Monitoring Środowiska—Inspekcja Ochrony Środowiska. Available online: http://powietrze.gios.gov.pl/pjp/content/show/1000357 (accessed on 20 October 2017).
- Driece, H.A.L.; Siesling, S.; Swuste, P.H.J.J.; Burdorf, A. Assessment of cancer risks due to environmental exposure to asbestos. J. Expo. Sci. Environ. Epidemiol. 2010, 20, 478–485. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Huuskonen, M.S.; Tossavainen, A.; Higashi, T.; Okubo, T.; Rantanen, J. Ecological Relationship between Mesothelioma Incidence/Mortality and Asbestos Consumption in Ten Western Countries and Japan. J. Occup. Health 1999, 41, 8–11. [Google Scholar] [CrossRef]
- Marinaccio, A.; Montanaro, F.; Mastrantonio, M.; Uccelli, R.; Altavista, P.; Nesti, M.; Costantini, A.S.; Gorini, G. Predictions of mortality from pleural mesothelioma in Italy: A model based on asbestos consumption figures supports results from age-period-cohort models. Int. J. Cancer 2005, 115, 142–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, J.C. Health Implications of Environmental Exposure to Asbestos. Environ. Health. Perspect. 1985, 62, 319–328. [Google Scholar] [CrossRef] [PubMed]
- McCambridge, A.J.; Napolitano, A.; Mansfield, A.S.; Fennell, D.A.; Sekido, Y.; Nowak, A.K.; Reungwetwattana, T.; Mao, W.; Pass, H.I.; Carbone, M.; et al. Progress in the Management of Malignant Pleural Mesothelioma in 2017. J. Thorac. Oncol. 2018, 13, 606–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MM Morbidity Rate | Moran’s I | E (I) s 1 | Var (I) 2 | Z-Score 3 | P |
|---|---|---|---|---|---|
| Entire Population | 0.287 | −0.066 | 0.02 | 2166 | 0.03 |
| Man | 0.260 | −0.066 | 0.02 | 2012 | 0.04 |
| Women | 0.269 | −0.066 | 0.02 | 2012 | 0.03 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krówczyńska, M.; Wilk, E. Asbestos Exposure and the Mesothelioma Incidence in Poland. Int. J. Environ. Res. Public Health 2018, 15, 1741. https://doi.org/10.3390/ijerph15081741
Krówczyńska M, Wilk E. Asbestos Exposure and the Mesothelioma Incidence in Poland. International Journal of Environmental Research and Public Health. 2018; 15(8):1741. https://doi.org/10.3390/ijerph15081741
Chicago/Turabian StyleKrówczyńska, Małgorzata, and Ewa Wilk. 2018. "Asbestos Exposure and the Mesothelioma Incidence in Poland" International Journal of Environmental Research and Public Health 15, no. 8: 1741. https://doi.org/10.3390/ijerph15081741
APA StyleKrówczyńska, M., & Wilk, E. (2018). Asbestos Exposure and the Mesothelioma Incidence in Poland. International Journal of Environmental Research and Public Health, 15(8), 1741. https://doi.org/10.3390/ijerph15081741