Premature Adult Death and Equity Impact of a Reduction of NO2, PM10, and PM2.5 Levels in Paris—A Health Impact Assessment Study Conducted at the Census Block Level

Abstract
:1. Introduction
2. Materiel and Methods
2.1. Study Area
2.2. Health Data
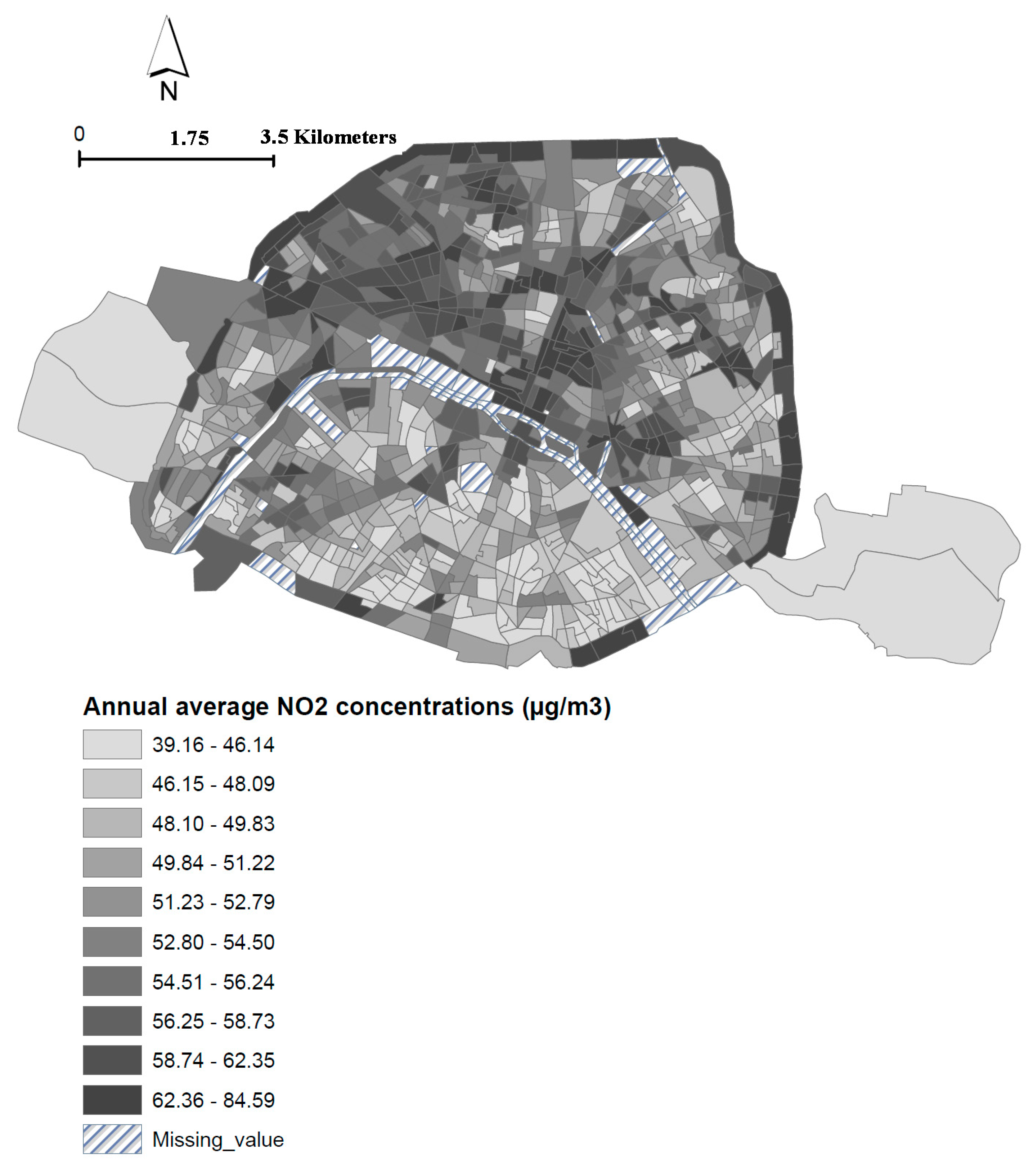
2.3. Air Pollution
2.4. Socioeconomic Deprivation Index
2.5. Health Impact Assessments (HIAs)
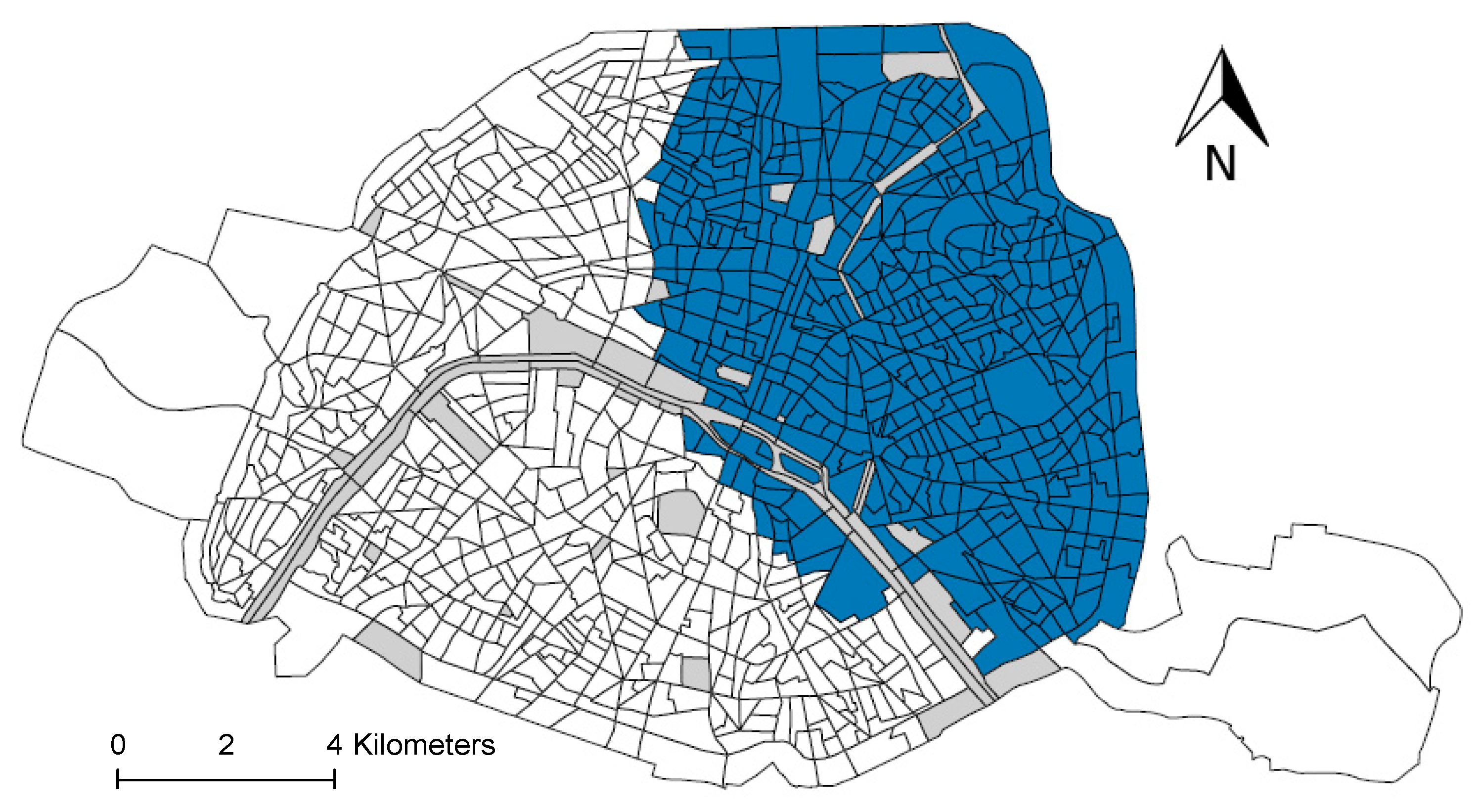
2.6. Spatial Analysis
3. Results
3.1. Description of the Study Area and the Population
3.2. Health Impact
3.2.1. Overall Estimates
3.2.2. Estimates by Socioeconomic Deprivation Class
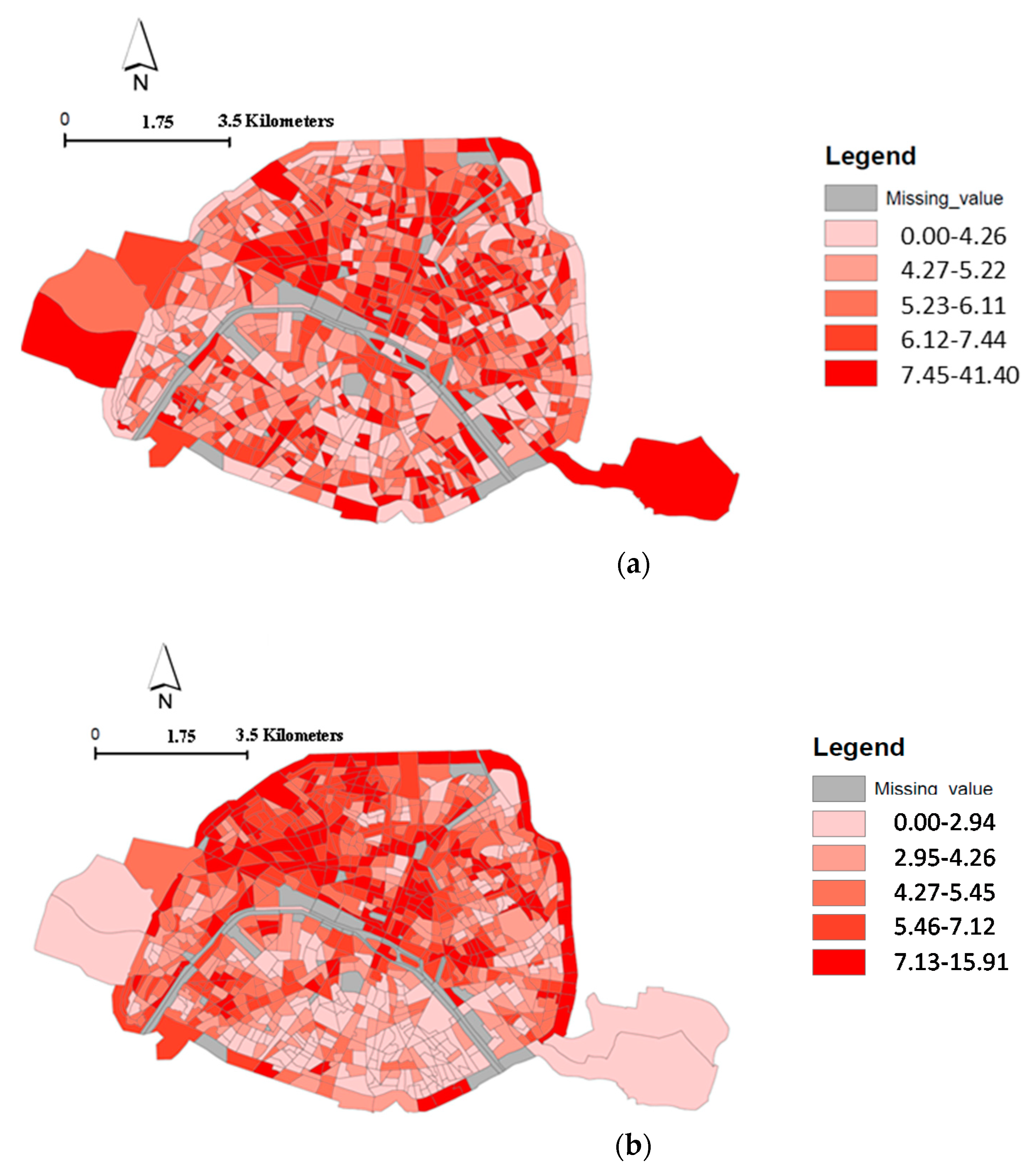
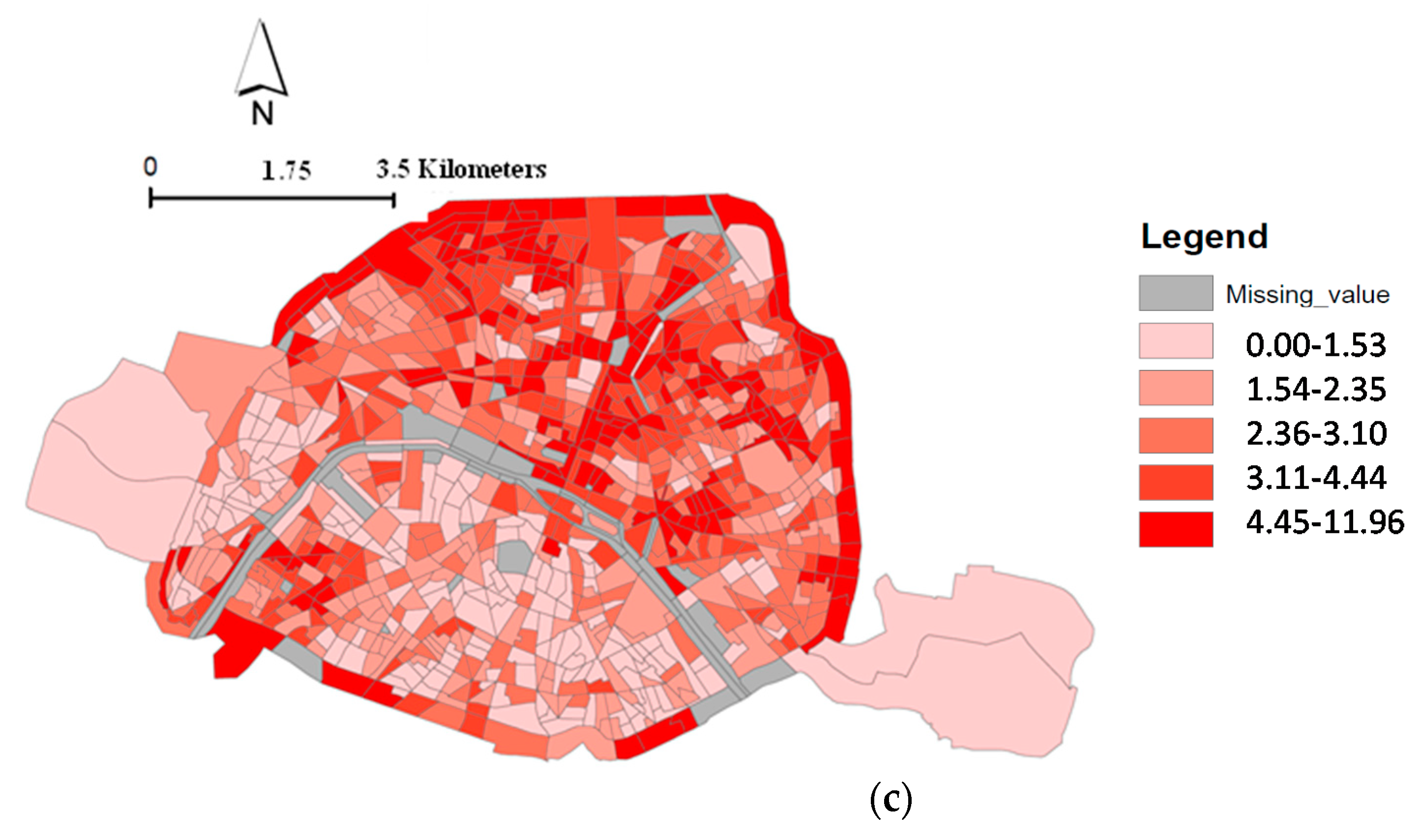
3.3. Spatial Distribution
4. Discussion
Benefits of this Research for Public Health
- Quantification of the number of “premature” deaths attributable to a reduction of NO2, PM10, and PM2.5 stratified by residential socioeconomic deprivation status.
- Spatial distribution of health and equity impacts of reducing these three pollutants.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A





References
- World Health Organization. WHO Releases Country Estimates on Air Pollution Exposure and Health Impact; WHO: Geneva, Switzerland, 2016; Available online: http://www.who.int/news-room/detail/27-09-2016-who-releases-country-estimates-on-air-pollution-exposure-and-health-impact (accessed on 23 May 2018).
- Guillerm, N.; Cesari, G. Fighting ambient air pollution and its impact on health: From human rights to the right to a clean environment. Int. J. Tubercul. Lung Dis. 2015, 19, 887–897. [Google Scholar] [CrossRef] [PubMed]
- OECD. Organisation for Economic Co-Operation and Development—The Cost of Air Pollution. Health Impacts of Road Transport. 2014. Available online: http://www.keepeek.com/Digital-Asset-Management/oecd/environment/the-cost-of-air-pollution_9789264210448-en#page1 (accessed on 9 February 2015).
- WHO. WHO Mortality and Burden of Disease from Ambient Air Pollution; WHO: Geneva, Switzerland, 2012; Available online: http://www.who.int/gho/phe/outdoor_air_pollution/burden/en/ (accessed on 23 May 2018).
- Deguen, S.; Petit, C.; Delbarre, A.; Kihal, W.; Padilla, C.; Benmarhnia, T.; Lapostolle, A.; Chauvin, P.; Zmirou-Navier, D. Neighbourhood Characteristics and Long-Term Air Pollution Levels Modify the Association between the Short-Term Nitrogen Dioxide Concentrations and All-Cause Mortality in Paris. PLoS ONE 2015, 10, e0131463. [Google Scholar] [CrossRef] [PubMed]
- Padilla, C.M.; Deguen, S.; Lalloue, B.; Blanchard, O.; Beaugard, C.; Troude, F.; Navier, D.Z.; Vieira, V.M. Cluster analysis of social and environment inequalities of infant mortality. A spatial study in small areas revealed by local disease mapping in France. Sci. Total Environ. 2013, 454–455, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.H.; Knutsen, S.F.; Shavlik, D.; Beeson, W.L.; Petersen, F.; Ghamsary, M.; Abbey, D. The association between fatal coronary heart disease and ambient particulate air pollution: Are females at greater risk? Environ. Health Perspect. 2005, 113, 1723–1729. [Google Scholar] [CrossRef] [PubMed]
- U.S. Environmental Protection Agency. Final Regulatory Impact Analysis (RIA) for the NO2 National Ambient Air Quality Standards (NAAQS); Office of Air Quality Planning and Standards: Washington, DC, USA, 2010.
- Pope, C.A.; Ezzati, M.; Dockery, D.W. Fine-particulate air pollution and life expectancy in the United States. N. Engl. J. Med. 2009, 360, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.; Künzli, N.; Götschi, T. Health benefits of a reduction of PM10 and NO2 exposure after implementing a clean air plan in the Agglomeration Lausanne-Morges. Int. J. Hyg. Environ. Health 2017, 220, 829–839. [Google Scholar] [CrossRef] [PubMed]
- Morelli, X.; Rieux, C.; Cyrys, J.; Forsberg, B.; Slama, R. Air pollution, health and social deprivation: A fine-scale risk assessment. Environ. Res. 2016, 147, 59–70. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Ito, K.; Buonocore, J.J.; Levy, J.I.; Arcaya, M.C. A health impact assessment of proposed public transportation service cuts and fare increases in Boston, Massachusetts (USA). Int. J. Environ. Res. Public Health 2014, 11, 8010–8024. [Google Scholar] [CrossRef] [PubMed]
- Cesaroni, G.; Badaloni, C.; Gariazzo, C.; Stafoggia, M.; Sozzi, R.; Davoli, M.; Forastiere, F. Long-term exposure to urban air pollution and mortality in a cohort of more than a million adults in Rome. Environ. Health Perspect. 2013, 121, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Fischer, P.H.; Marra, M.; Ameling, C.B.; Hoek, G.; Beelen, R.; de Hoogh, K.; Breugelmans, O.; Kruize, H.; Janssen, N.A.; Houthuijs, D. Air Pollution and Mortality in Seven Million Adults: The Dutch Environmental Longitudinal Study (DUELS). Environ. Health Perspect. 2015, 123, 697–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ined—Inst. Natl. D’études Démographiques. 2004. Available online: https://www.ined.fr/en/everything_about_population/graphs-maps/interpreted-graphs/age-risk-mortality/ (accessed on 13 December 2018).
- INSEE. 2016. Available online: https://www.insee.fr/fr/statistiques/3134763 (accessed on 13 December 2018).
- Lalloué, B.; Monnez, J.-M.; Padilla, C.; Kihal, W.; Le Meur, N.; Zmirou-Navier, D.; Deguen, S. A statistical procedure to create a neighborhood socioeconomic index for health inequalities analysis. Int. J. Equity Health 2013, 12, 21. [Google Scholar] [CrossRef] [PubMed]
- Kihal-Talantikite, W.; Padilla, C.M.; Lalloué, B.; Gelormini, M.; Zmirou-Navier, D.; Deguen, S. Green space, social inequalities and neonatal mortality in France. BMC Pregnancy Childbirth 2013, 13, 191. [Google Scholar] [CrossRef] [PubMed]
- Kihal-Talantikite, W.; Padilla, C.M.; Lalloue, B.; Rougier, C.; Defrance, J.; Zmirou-Navier, D.; Deguen, S. An exploratory spatial analysis to assess the relationship between deprivation, noise and infant mortality: An ecological study. Environ. Health Glob. Access. Sci. Source 2013, 12, 109. [Google Scholar] [CrossRef] [PubMed]
- Ostro, B. Outdoor Air Pollution—Assessing the Environmental Burden of Disease at National and Local Levels; World Health Organization: Geneva, Switzerland, 2004; Available online: http://www.who.int/quantifying_ehimpacts/national/en/ (accessed on 23 December 2018).
- Kulldorff, M. Information Management Services, Inc. SaTScan: Software for the Spatial, Temporal, and Space-Time Scan Statistics, Version 6.0. 2005. Available online: http://www.satscan.org/ (accessed on 8 October 2018).
- Kulldorff, M. A spatial scan statistic. Commun. Stat. Theory Methods 1997, 26, 1481–1496. [Google Scholar] [CrossRef]
- Kulldorff, M.; Nagarwalla, N. Spatial disease clusters: Detection and inference. Stat. Med. 1995, 14, 799–810. [Google Scholar] [CrossRef] [PubMed]
- Dwass, M. Modified Randomization Tests for Nonparametric Hypotheses. Ann. Math. Stat. 1957, 28, 181–187. [Google Scholar] [CrossRef]
- GBD 2015 LRI Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: A systematic analysis for the Global Burden of Disease Study 2015. Lancet. Infect. Dis. 2017, 17, 1133–1161. [Google Scholar] [CrossRef]
- Wheida, A.; Nasser, A.; El Nazer, M.; Borbon, A.; Abo El Ata, G.A.; Abdel Wahab, M.; Alfaro, S.C. Tackling the mortality from long-term exposure to outdoor air pollution in megacities: Lessons from the Greater Cairo case study. Environ. Res. 2018, 160, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Hensche, S.; Chan, G. Health Risks of Air Pollution in Europe—HRAPIE Project New Emerging Risks to Health from Air Pollution—Results from the Survey of Experts. 2013. Available online: http://www.euro.who.int/__data/assets/pdf_file/0017/234026/e96933.pdf (accessed on 8 October 2018).
- Wahida, K.-T.; Padilla, C.M.; Denis, Z.-N.; Olivier, B.; Géraldine, L.N.; Philippe, Q.; Séverine, D. A Conceptual Framework for the Assessment of Cumulative Exposure to Air Pollution at a Fine Spatial Scale. Int. J. Environ. Res. Public Health 2016, 13, 319. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2004–2009 | Population > 30 Years | Death Rate (per 100,000 Inhabitants) | NO2 (µg/m3) | Surface (km2) |
|---|---|---|---|---|
| Total | 8,152,966 | 1007.20 | 53.39 | 105.4 |
| 1 (Less deprived) | 718,290 | 1129.91 | 52.66 | 9.20 |
| 2 | 724,338 | 977.86 | 54.01 | 9.87 |
| 3 | 781,848 | 1006.33 | 54.10 | 7.54 |
| 4 | 802,248 | 985.23 | 53.53 | 7.14 |
| 5 | 782,280 | 1005.14 | 54.02 | 10.04 |
| 6 | 874,356 | 1002.57 | 53.73 | 6.66 |
| 7 | 872,640 | 917.90 | 52.63 | 7.17 |
| 8 | 862,818 | 1010.06 | 50.96 | 12.37 |
| 9 | 863,826 | 960.96 | 51.00 | 13.62 |
| 10 (More deprived) | 819,006 | 1071.05 | 54.11 | 14.75 |
| 2007–2009 | Population > 30 Years | Death Rate (per 100,000 Population) | PM10 (g/m3) | PM2.5 (g/m3) | Surface (km2) |
|---|---|---|---|---|---|
| Total | 4,103,250 | 992.14 | 31.07 | 20.9 | 105.4 |
| 1 (Less deprived) | 370,011 | 1112.67 | 30.8 | 20.74 | 9.20 |
| 2 | 370,800 | 924.22 | 31.24 | 21.01 | 9.87 |
| 3 | 395,459 | 979.87 | 31.34 | 21.07 | 7.54 |
| 4 | 407,266 | 982.4 | 31.16 | 21 | 7.14 |
| 5 | 394,149 | 987.19 | 31.31 | 21.09 | 10.04 |
| 6 | 442,374 | 964.57 | 31.15 | 20.96 | 6.66 |
| 7 | 443,739 | 901.21 | 30.9 | 20.83 | 7.17 |
| 8 | 435,338 | 986.82 | 30.29 | 20.41 | 12.37 |
| 9 | 442,427 | 933.94 | 30.34 | 20.42 | 13.62 |
| 10 (More deprived) | 414,934 | 1048.12 | 31.17 | 20.84 | 14.75 |
| Air Pollutants | Socioeconomic Deprivation Class | |||||
|---|---|---|---|---|---|---|
| High (1–2) | Moderate/High (3–4) | Medium (5–6) | Moderate/ Low (7–8) | Low (9–10) | ||
| NO2 | HR | 1.013 | 1.036 | 1.022 | 1.027 | 1.031 |
| LL | 1.002 | 1.027 | 1.014 | 1.02 | 1.025 | |
| UL | 1.023 | 1.046 | 1.03 | 1.034 | 1.038 | |
| PM10 | HR | 1.048 | 1.099 | 1.052 | 1.091 | 1.094 |
| LL | 1.013 | 1.064 | 1.024 | 1.067 | 1.074 | |
| UL | 1.084 | 1.137 | 1.08 | 1.114 | 1.113 | |
| Air Pollutants | Socioeconomic Deprivation Class | |||
|---|---|---|---|---|
| High (1–3) | Medium (4–7) | Low (8–10) | ||
| NO2 | HR | 1.024 | 1.016 | 1.034 |
| LL | 1.012 | 1.002 | 1.024 | |
| UL | 1.036 | 1.03 | 1.045 | |
| PM2.5 | HR | 1.04 | 1.018 | 1.05 |
| LL | 1.02 | 0.99 | 1.03 | |
| UL | 1.06 | 1.04 | 1.07 | |
| Socioeconomic Deprivation Classes | Rate of Attributable Deaths (per 100,000 Population) [95% CI] | |
|---|---|---|
| NO2 Dose-Response Function 1 | NO2 Dose-Response Function 2 | |
| Decile 1 (less deprived) | 18.3 [2.8; 21.1] | 33.4 [16.9; 49.5] |
| Decile 2 | 17.5 [2.7; 30.7] | 31.9 [16.2; 47.3] |
| Decile 3 | 48.9 [37.1; 61.8] | 33.1 [16.8; 48.9] |
| Decile 4 | 46.0 [34.9; 56.2] | 20.9 [2.7; 38.6] |
| Decile 5 | 30.2 [19.4; 40.8] | 22.1 [2.8; 40.8] |
| Decile 6 | 29.5 [18.9; 39.9] | 21.6 [2.7; 39.9] |
| Decile 7 | 30.4 [22.7; 37.9] | 18.1 [2.3; 33.6] |
| Decile 8 | 33.2 [26.9; 40.4] | 36.3 [25.9; 47.6] |
| Decile 9 | 31.7 [25.7; 38.6] | 34.7 [25.7; 45.4] |
| Decile 10 (more deprived) | 45.2 [36.7; 54.9] | 49.4 [35.2; 64.5] |
| Socioeconomic Deprivation Classes | Rate of Attributable Deaths (per 100 000 Population) [95% CI] | |
|---|---|---|
| PM10 Dose-Response Function 1 | PM2.5 Dose-Response Function 2 | |
| Decile 1 (less deprived) | 54.9 [15.4; 92.8] | 45.9 [23.4; 67.5] |
| Decile 2 | 47.4 [13.3; 80.1] | 39.1 [19.9; 57.4] |
| Decile 3 | 99.5 [66.5; 132.8] | 41.6 [21.2; 61.2] |
| Decile 4 | 98.2 [65.7; 131.1] | 19.1 [0; 41.5] |
| Decile 5 | 55 [26.1; 82.3] | 19.3 [0; 42] |
| Decile 6 | 53 [25.1; 79.3] | 18.7 [0; 40.6] |
| Decile 7 | 81.6 [61.5; 100] | 17.2 [0; 37.5] |
| Decile 8 | 84.6 [63.7; 103.7] | 48.9 [29.9; 67.1] |
| Decile 9 | 82.8 [66.5; 97.9] | 46.3 [28.3; 63.6] |
| Decile 10 (more deprived) | 100.1 [80.3; 118.1] | 54.0 [33.3; 74.1] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kihal-Talantikite, W.; Legendre, P.; Le Nouveau, P.; Deguen, S. Premature Adult Death and Equity Impact of a Reduction of NO2, PM10, and PM2.5 Levels in Paris—A Health Impact Assessment Study Conducted at the Census Block Level. Int. J. Environ. Res. Public Health 2019, 16, 38. https://doi.org/10.3390/ijerph16010038
Kihal-Talantikite W, Legendre P, Le Nouveau P, Deguen S. Premature Adult Death and Equity Impact of a Reduction of NO2, PM10, and PM2.5 Levels in Paris—A Health Impact Assessment Study Conducted at the Census Block Level. International Journal of Environmental Research and Public Health. 2019; 16(1):38. https://doi.org/10.3390/ijerph16010038
Chicago/Turabian StyleKihal-Talantikite, Wahida, Pierre Legendre, Pauline Le Nouveau, and Séverine Deguen. 2019. "Premature Adult Death and Equity Impact of a Reduction of NO2, PM10, and PM2.5 Levels in Paris—A Health Impact Assessment Study Conducted at the Census Block Level" International Journal of Environmental Research and Public Health 16, no. 1: 38. https://doi.org/10.3390/ijerph16010038
APA StyleKihal-Talantikite, W., Legendre, P., Le Nouveau, P., & Deguen, S. (2019). Premature Adult Death and Equity Impact of a Reduction of NO2, PM10, and PM2.5 Levels in Paris—A Health Impact Assessment Study Conducted at the Census Block Level. International Journal of Environmental Research and Public Health, 16(1), 38. https://doi.org/10.3390/ijerph16010038