Environmental Tobacco Smoke and Cardiovascular Disease

Abstract
:1. Introduction
2. Methods
3. ETS: Definition and Physical/Biochemical Properties
4. Physiology of Atherogenesis and Thrombosis
5. Epidemiology
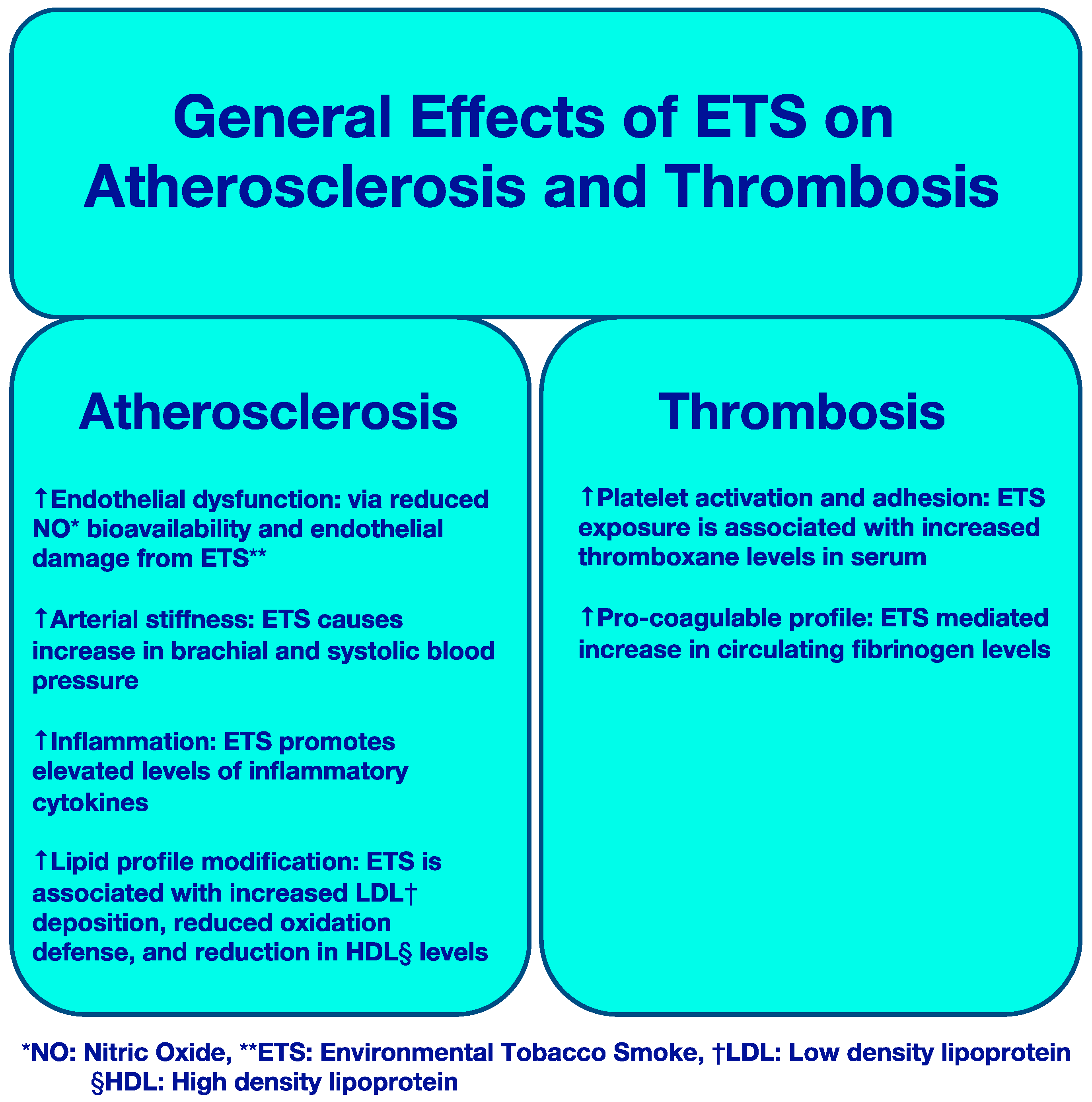
6. ETS and Atherosclerosis: Clinical and Experimental Observations
6.1. Effects on Endothelial Function
6.2. Effects on Arterial Stiffness
6.3. Inflammation
6.4. Modification of Lipid Profile
6.5. ETS and Progression of Atherosclerosis
7. ETS and Thrombosis: Clinical and Experimental Observations
7.1. ETS and Platelet Function
7.2. ETS and Coagulation Cascade
7.3. Effect on Heart Rate and Heart Rate Variability
7.4. ETS and Anginal Symptoms
7.5. ETS and Infarct Size
8. Factors and Mechanisms Responsible for ETS-Mediated Cardiovascular Dysfunction
9. Public Health Implications of ETS-Mediated Cardiovascular Disease
10. Emerging Areas in the Study of ETS
11. Conclusions
Author Contributions
Conflicts of Interest
References
- National Center for Chronic Disease Prevention; Health Promotion Office on Smoking and Health; Reports of the Surgeon General. The Health Consequences of Smoking-50 Years of Progress: A Report of the Surgeon General; Centers for Disease Control and Prevention (US): Atlanta, GA, USA, 2014. [Google Scholar]
- National Research Council Committee on Passive Smoking. Environmental Tobacco Smoke: Measuring Exposures and Assessing Health Effects; National Academies Press: Washington, DC, USA, 1986. [Google Scholar]
- Tseung, J. Robbins and Cotran Pathologic Basis of Disease: 7th Edition. Pathology 2005, 37, 190. [Google Scholar] [CrossRef]
- Garland, C.; Barrett-Connor, E.; Suarez, L.; Criqui, M.H.; Wingard, D.L. Effects of passive smoking on ischemic heart disease mortality of nonsmokers. A prospective study. Am. J. Epidemiol. 1985, 121, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, T. Lung cancer in Japan: Effects of nutrition and passive smoking. In Lung Cancer: Causes and Prevention; Mizell, M., Correa, P., Eds.; Verlag Chemie, International, Inc.: New York, NY, USA, 1984; pp. 175–195. [Google Scholar]
- Svendsen, K.H.; Kuller, L.H.; Martin, M.J.; Ockene, J.K. Effects of passive smoking in the Multiple Risk Factor Intervention Trial. Am. J. Epidemiol. 1987, 126, 783–795. [Google Scholar] [CrossRef] [PubMed]
- Barnoya, J.; Glantz, S.A. Cardiovascular effects of secondhand smoke: Nearly as large as smoking. Circulation 2005, 111, 2684–2698. [Google Scholar] [CrossRef] [PubMed]
- West, H.W.; Juonala, M.; Gall, S.L.; Kähönen, M.; Laitinen, T.; Taittonen, L.; Viikari, J.S.; Raitakari, O.T.; Magnussen, C.G. Exposure to parental smoking in childhood is associated with increased risk of carotid atherosclerotic plaque in adulthood: The Cardiovascular Risk in Young Finns Study. Circulation 2015, 131, 1239–1246. [Google Scholar] [CrossRef]
- Ambrose, J.A.; Barua, R.S. The pathophysiology of cigarette smoking and cardiovascular disease: An update. J. Am. Coll. Cardiol. 2004, 43, 1731–1737. [Google Scholar] [CrossRef]
- Heiss, C.; Amabile, N.; Lee, A.C.; Real, W.M.; Schick, S.F.; Lao, D.; Wong, M.L.; Jahn, S.; Angeli, F.S.; Minasi, P.; et al. Brief secondhand smoke exposure depresses endothelial progenitor cells activity and endothelial function: Sustained vascular injury and blunted nitric oxide production. J. Am. Coll. Cardiol. 2008, 51, 1760–1771. [Google Scholar] [CrossRef]
- Otsuka, R.; Watanabe, H.; Hirata, K.; Tokai, K.; Muro, T.; Yoshiyama, M.; Takeuchi, K.; Yoshikawa, J. Acute effects of passive smoking on the coronary circulation in healthy young adults. JAMA 2001, 286, 436–441. [Google Scholar] [CrossRef]
- Celermajer, D.S.; Adams, M.R.; Clarkson, P.; Robinson, J.; McCredie, R.; Donald, A.; Deanfield, J.E. Passive smoking and impaired endothelium-dependent arterial dilatation in healthy young adults. N. Engl. J. Med. 1996, 334, 150–154. [Google Scholar] [CrossRef]
- Adams, T.; Wan, E.; Wei, Y.; Wahab, R.; Castagna, F.; Wang, G.; Emin, M.; Russo, C.; Homma, S.; Le Jemtel, T.H.; et al. Secondhand Smoking Is Associated with Vascular Inflammation. Chest 2015, 148, 112–119. [Google Scholar] [CrossRef]
- Zhu, B.Q.; Parmley, W.W. Hemodynamic and vascular effects of active and passive smoking. Am. Heart J. 1995, 130, 1270–1275. [Google Scholar] [CrossRef]
- Hutchison, S.J.; Sudhir, K.; Chou, T.M.; Sievers, R.E.; Zhu, B.Q.; Sun, Y.P.; Deedwania, P.C.; Glantz, S.A.; Parmley, W.W.; Chatterjee, K. Testosterone worsens endothelial dysfunction associated with hypercholesterolemia and environmental tobacco smoke exposure in male rabbit aorta. J. Am. Coll. Cardiol. 1997, 29, 800–807. [Google Scholar] [CrossRef]
- Wells, A.J. Passive smoking as a cause of heart disease. J. Am. Coll. Cardiol. 1994, 24, 546–554. [Google Scholar] [CrossRef]
- Mullick, A.E.; McDonald, J.M.; Melkonian, G.; Talbot, P.; Pinkerton, K.E.; Rutledge, J.C. Reactive carbonyls from tobacco smoke increase arterial endothelial layer injury. Am. J. Physiol. Heart Circ. Physiol. 2002, 283, H591–H597. [Google Scholar] [CrossRef] [PubMed]
- Mahmud, A.; Feely, J. Effects of passive smoking on blood pressure and aortic pressure waveform in healthy young adults—Influence of gender. Br. J. Clin. Pharmacol. 2004, 57, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Mack, W.J.; Islam, T.; Lee, Z.; Selzer, R.H.; Hodis, H.N. Environmental tobacco smoke and carotid arterial stiffness. Prev. Med. 2003, 37, 148–154. [Google Scholar] [CrossRef]
- Shima, M.; Adachi, M. Effects of environmental tobacco smoke on serum levels of acute phase proteins in schoolchildren. Prev. Med. 1996, 25, 617–624. [Google Scholar] [CrossRef]
- Anderson, R.; Theron, A.J.; Richards, G.A.; Myer, M.S.; van Rensburg, A.J. Passive smoking by humans sensitizes circulating neutrophils. Am. Rev. Respir. Dis. 1991, 144, 570–574. [Google Scholar] [CrossRef]
- Panagiotakos, D.B.; Pitsavos, C.; Chrysohoou, C.; Skoumas, J.; Masoura, C.; Toutouzas, P.; Stefanadis, C. ATTICA Study. Effect of exposure to secondhand smoke on markers of inflammation: The ATTICA study. Am. J. Med. 2004, 116, 145–150. [Google Scholar] [CrossRef]
- Jones, M.R.; Magid, H.S.; Al-Rifai, M.; McEvoy, J.W.; Kaufman, J.D.; Hinckley Stukovsky, K.D.; Szklo, M.; Polak, J.; Burke, G.L.; Post, W.S.; et al. Secondhand Smoke Exposure and Subclinical Cardiovascular Disease: The Multi-Ethnic Study of Atherosclerosis. J. Am. Heart Assoc. 2016, 5, e002965. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, Y.; Shi, J.; Larson, D.F.; Watson, R.R. Side-stream cigarette smoke induces dose-response in systemic inflammatory cytokine production and oxidative stress. Exp. Biol. Med. 2002, 227, 823–829. [Google Scholar] [CrossRef]
- Yuan, H.; Wong, L.S.; Bhattacharya, M.; Ma, C.; Zafarani, M.; Yao, M.; Schneider, M.; Pitas, R.E.; Martins-Green, M. The effects of second-hand smoke on biological processes important in atherogenesis. BMC Cardiovasc. Disord. 2007, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Valkonen, M.; Kuusi, T. Passive smoking induces atherogenic changes in low-density lipoprotein. Circulation 1998, 97, 2012–2016. [Google Scholar] [CrossRef] [PubMed]
- Gairola, C.G.; Drawdy, M.L.; Block, A.E.; Daugherty, A. Sidestream cigarette smoke accelerates atherogenesis in apolipoprotein E−/− mice. Atherosclerosis 2001, 156, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Moffatt, R.J.; Stamford, B.A.; Biggerstaff, K.D. Influence of worksite environmental tobacco smoke on serum lipoprotein profiles of female nonsmokers. Metab. Clin. Exp. 1995, 44, 1536–1539. [Google Scholar] [CrossRef]
- Moffatt, R.J.; Chelland, S.A.; Pecott, D.L.; Stamford, B.A. Acute exposure to environmental tobacco smoke reduces HDL-C and HDL2-C. Prev. Med. 2004, 38, 637–641. [Google Scholar] [CrossRef] [PubMed]
- Neufeld, E.J.; Mietus-Snyder, M.; Beiser, A.S.; Baker, A.L.; Newburger, J.W. Passive cigarette smoking and reduced HDL cholesterol levels in children with high-risk lipid profiles. Circulation 1997, 96, 1403–1407. [Google Scholar] [CrossRef]
- Howard, G.; Wagenknecht, L.E.; Burke, G.L.; Diez-Roux, A.; Evans, G.W.; McGovern, P.; Javier Nieto, F.; Tell, G.S. Cigarette smoking and progression of atherosclerosis: The Atherosclerosis Risk in Communities (ARIC) Study. JAMA 1998, 279, 119–124. [Google Scholar] [CrossRef]
- He, Y.; Lam, T.H.; Li, L.S.; Li, L.S.; Du, R.Y.; Jia, G.L.; Huang, J.Y.; Zheng, J.S. The number of stenotic coronary arteries and passive smoking exposure from husband in lifelong non-smoking women in Xi’an, China. Atherosclerosis 1996, 127, 229–238. [Google Scholar] [CrossRef]
- Knight-Lozano, C.A.; Young, C.G.; Burow, D.L.; Burow, D.L.; Hu, Z.Y.; Uyeminami, D.; Pinkerton, K.E.; Ischiropoulos, H.; Ballinger, S.W. Cigarette smoke exposure and hypercholesterolemia increase mitochondrial damage in cardiovascular tissues. Circulation 2002, 105, 849–854. [Google Scholar] [CrossRef]
- Zhu, B.Q.; Sun, Y.P.; Sievers, R.E.; Isenberg, W.M.; Glantz, S.A.; Parmley, W.W. Passive smoking increases experimental atherosclerosis in cholesterol-fed rabbits. J. Am. Coll. Cardiol. 1993, 21, 225–232. [Google Scholar] [CrossRef]
- Sun, Y.; Lin, Z.; Ding, W.J.; Shi, Y.; Zhu, L.; Wei, Q.; Wang, C. Secondhand smoking and matrix metalloproteinase-2 and -9 gene expression in saphenous veins of women nonsmokers. Ann. Thorac. Surg. 2014, 98, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.W.; Shelton, L.; Watanabe, I.S.; Arnold, J. Passive smoking affects endothelium and platelets. Arch. Intern. Med. 1989, 149, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Karanikas, G.; Kritz, H.; Pirich, C.; Stamatopoulos, Y.; Peskar, B.A.; Sinzinger, H. Passive smoking and platelet thromboxane. Thromb. Res. 1996, 81, 451–460. [Google Scholar] [CrossRef]
- Srikanth, S.; Sy, F.; Kotak, K.; Kiel, R.G.; Bajwa, M.; Tandon, A.; Loures-Vale, A.A.; Aftab, W.; Tringali, S.; Ambrose, J.A. A Single Controlled Exposure to Secondhand Smoke May Not Alter Thrombogenesis or Trigger Platelet Activation. Nicotine Tob. Res. 2016, 18, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Iso, H.; Shimamoto, T.; Sato, S.; Koike, K.; Iida, M.; Komachi, Y. Passive smoking and plasma fibrinogen concentrations. Am. J. Epidemiol. 1996, 144, 1151–1154. [Google Scholar] [CrossRef] [PubMed]
- Stavroulakis, G.A.; Makris, T.K.; Hatzizacharias, A.N.; Tsoukala, C.; Kyriakidis, M.K. Passive smoking adversely affects the haemostasis/fibrinolytic parameters in healthy non-smoker offspring of healthy smokers. Thromb. Haemost. 2000, 84, 923–924. [Google Scholar] [CrossRef]
- Raupach, T.; Schafer, K.; Konstantinides, S.; Andreas, S. Secondhand smoke as an acute threat for the cardiovascular system: A change in paradigm. Eur. Heart J. 2006, 27, 386–392. [Google Scholar] [CrossRef]
- Koplan, B.A.; Stevenson, W.G. Ventricular tachycardia and sudden cardiac death. Mayo Clin. Proc. 2009, 84, 289–297. [Google Scholar] [CrossRef]
- Pope, C.A., 3rd; Eatough, D.J.; Gold, D.R.; Pang, Y.; Nielsen, K.R.; Nath, P.; Verrier, R.L.; Kanner, R.E. Acute exposure to environmental tobacco smoke and heart rate variability. Environ. Health Perspect. 2001, 109, 711–716. [Google Scholar] [CrossRef]
- Zhu, B.Q.; Sun, Y.P.; Sievers, R.E.; Glantz, S.A.; Parmley, W.W.; Wolfe, C.L. Exposure to environmental tobacco smoke increases myocardial infarct size in rats. Circulation 1994, 89, 1282–1290. [Google Scholar] [CrossRef] [PubMed]
- Luquette, A.J.; Landess, C.W.; Merki, D.J. Some immediate effects of a smoking environment on children of elementary school age. J. Sch. Health 1970, 40, 533–535. [Google Scholar] [CrossRef] [PubMed]
- Harke, H.-P.; Bleichert, A. Zum Problem des Passivrauchens. Int. Arch. Arbeitsmed. 1972, 29, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Rummel, R.M.; Crawford, M.; Bruce, P. The physiological effects of inhaling exhaled cigarette smoke in relation to attitude of the nonsmoker. J. Sch. Health 1975, 45, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Hurshman, L.G.; Brown, B.S.; Guyton, E.G. The implications of sidestream cigarette smoke for cardiovascular health. J. Environ. Health 1978, 41, 145–149. [Google Scholar]
- Pimm, P.E.; Silverman, F.; Shephard, R.J. Physiological effects of acute passive exposure to cigarette smoke. Arch. Environ. Health 1978, 33, 201–213. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.P.; Zhu, B.Q.; Browne, A.E.; Sievers, R.E.; Bekker, J.M.; Chatterjee, K.; Parmley, W.W.; Glantz, S.A. Nicotine does not influence arterial lipid deposits in rabbits exposed to second-hand smoke. Circulation 2001, 104, 810–814. [Google Scholar] [CrossRef]
- Brownson, R.C.; Eriksen, M.P.; Davis, R.M.; Warner, K.E. Environmental Tobacco Smoke: Health Effects and Policies to Reduce Exposure. Annu. Rev. Public Health 1997, 18, 163–185. [Google Scholar] [CrossRef]
- Fichtenberg, C.M.; Glantz, S.A. Effect of smoke-free workplaces on smoking behaviour: Systematic review. BMJ 2002, 325, 188. [Google Scholar] [CrossRef]
- Matt, G.E.; Quintana, P.J.; Destaillats, H.; Gundel, L.A.; Sleiman, M.; Singer, B.C.; Jacob, P.; Benowitz, N.; Winickoff, J.P.; Rehan, V.; et al. Thirdhand tobacco smoke: Emerging evidence and arguments for a multidisciplinary research agenda. Environ. Health Perspect. 2011, 119, 1218–1226. [Google Scholar] [CrossRef]
- Whitlatch, A.; Schick, S. Thirdhand Smoke at Philip Morris. Nicotine Tob. Res. 2018. [Google Scholar] [CrossRef] [PubMed]
- Sleiman, M.; Gundel, L.A.; Pankow, J.F.; Jacob, P., 3rd; Singer, B.C.; Destaillats, H. Formation of carcinogens indoors by surface-mediated reactions of nicotine with nitrous acid, leading to potential thirdhand smoke hazards. Proc. Natl. Acad. Sci. USA 2010, 107, 6576–6581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Acuff, L.; Fristoe, K.; Hamblen, J.; Smith, M.; Chen, J. Third-Hand Smoke: Old Smoke, New Concerns. J. Community Health 2016, 41, 680–687. [Google Scholar] [CrossRef] [PubMed]
- Karim, Z.A.; Alshbool, F.Z.; Vemana, H.P.; Adhami, N.; Dhall, S.; Espinosa, E.V.; Martins-Green, M.; Khasawneh, F.T. Third-hand Smoke: Impact on Hemostasis and Thrombogenesis. J. Cardiovasc. Pharmacol. 2015, 66, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Barua, R.S.; Rigotti, N.A.; Benowitz, N.L.; Cummings, K.M.; Jazayeri, M.A.; Morris, P.B.; Ratchford, E.V.; Sarna, L.; Stecker, E.C.; Wiggins, B.S. 2018 ACC expert consensus decision pathway on tobacco cessation treatment. J. Am. Coll. Cardiol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Hess, I.M.; Lachireddy, K.; Capon, A. A systematic review of the health risks from passive exposure to electronic cigarette vapour. Public Health Res. Pract. 2016, 26, 2621617. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, A. Cardiovascular Perspective of the Promises and Perils of E-Cigarettes. Circ. Res. 2016, 118, 1872–1875. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Constituent—Chemical Group | Concentration | Human Biomarkers |
|---|---|---|
| Acetaldehyde—Volatile Organic Compound | 200–300 µg/m3 | Tissue, Blood N2-ethylidene-dGuo levels |
| Formaldehyde—Volatile Organic Compound | 100–140 µg/m3 | Tissue, Blood N6-hydroxymethyl deoxyadenosine adducts |
| Nicotine—Tobacco Alkaloid | 10–100 µg/m3 | Total nicotine equivalents (TNE) * Blood, Salivary or Urinary Cotinine level |
| 1,3-Butadiene—Volatile Organic Compound | 20–40 µg/m3 | Urine Monohydroxybutenyl mercapturic acid (MHBMA) |
| Benzene—Polyaromatic Hydrocarbon | 15–30 µg/m3 | Urine C,S BAP-tetrol Urine 3-hydroxy-BAP Urine 1-Hydroxypyrene Urine PheT |
| NNK (nicotine-derived nitrosamine ketone)—Tobacco-specific nitrosamine | 0.2–29.3 µg/m3 | Urine NNK Urine NNAL Urine NNAL-N-Gluc Urine NNAL-O-Gluc |
| Carbon Monoxide—Variable Gas | 5–20 µg/m3 | Exhaled CO ([CO] in ppm) Blood carboxyhemoglobin (%saturation of Hgb) |
| NNN (N-nitrosonornicotine)—Tobacco Specific Nitrosamine | 0.7–23 µg/m3 | Urine NNN levels Urine NNN-Gluc levels |
| Study | Heart Rate | Blood Pressure | Skin Temperature (°C) |
|---|---|---|---|
| Luguette et al., 1970 (N = 40) [45] | Before ETS: 89 After ETS: 97 | Before ETS: 116/67 After ETS: 120/72 | Not studied |
| Harke and Bleichert, 1972 (N = 10) [46] | Before ETS: 72 ± 8 After ETS: 74 ± 12 | Before ETS: 123/84 After ETS: 121/84 | Before ETS: 0.0 degrees After ETS: 0.0273 degrees |
| Rummel et al., 1975 (N = 56) [47] | Before ETS: 72 ± 10 After ETS: 71 ± 11 | Before ETS: 117/71 After ETS: 117/71 | Not studied |
| Hurshman et al., 1978 (N = 8) [48] | Before ETS: 73 After ETS: 79 | Before ETS 107/67 After ETS: 114/68 | Not studied |
| Pimm et al., 1978 (N = 20) [49] | Before ETS: 84 (F), 77 (M) After ETS: 80 (F), 80 (M) | Not studied | Not studied |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
DiGiacomo, S.I.; Jazayeri, M.-A.; Barua, R.S.; Ambrose, J.A. Environmental Tobacco Smoke and Cardiovascular Disease. Int. J. Environ. Res. Public Health 2019, 16, 96. https://doi.org/10.3390/ijerph16010096
DiGiacomo SI, Jazayeri M-A, Barua RS, Ambrose JA. Environmental Tobacco Smoke and Cardiovascular Disease. International Journal of Environmental Research and Public Health. 2019; 16(1):96. https://doi.org/10.3390/ijerph16010096
Chicago/Turabian StyleDiGiacomo, Sydne I., Mohammad-Ali Jazayeri, Rajat S. Barua, and John A. Ambrose. 2019. "Environmental Tobacco Smoke and Cardiovascular Disease" International Journal of Environmental Research and Public Health 16, no. 1: 96. https://doi.org/10.3390/ijerph16010096
APA StyleDiGiacomo, S. I., Jazayeri, M. -A., Barua, R. S., & Ambrose, J. A. (2019). Environmental Tobacco Smoke and Cardiovascular Disease. International Journal of Environmental Research and Public Health, 16(1), 96. https://doi.org/10.3390/ijerph16010096