Chronic Diseases and Employment: Which Interventions Support the Maintenance of Work and Return to Work among Workers with Chronic Illnesses? A Systematic Review

 , , , , , ,
, , , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
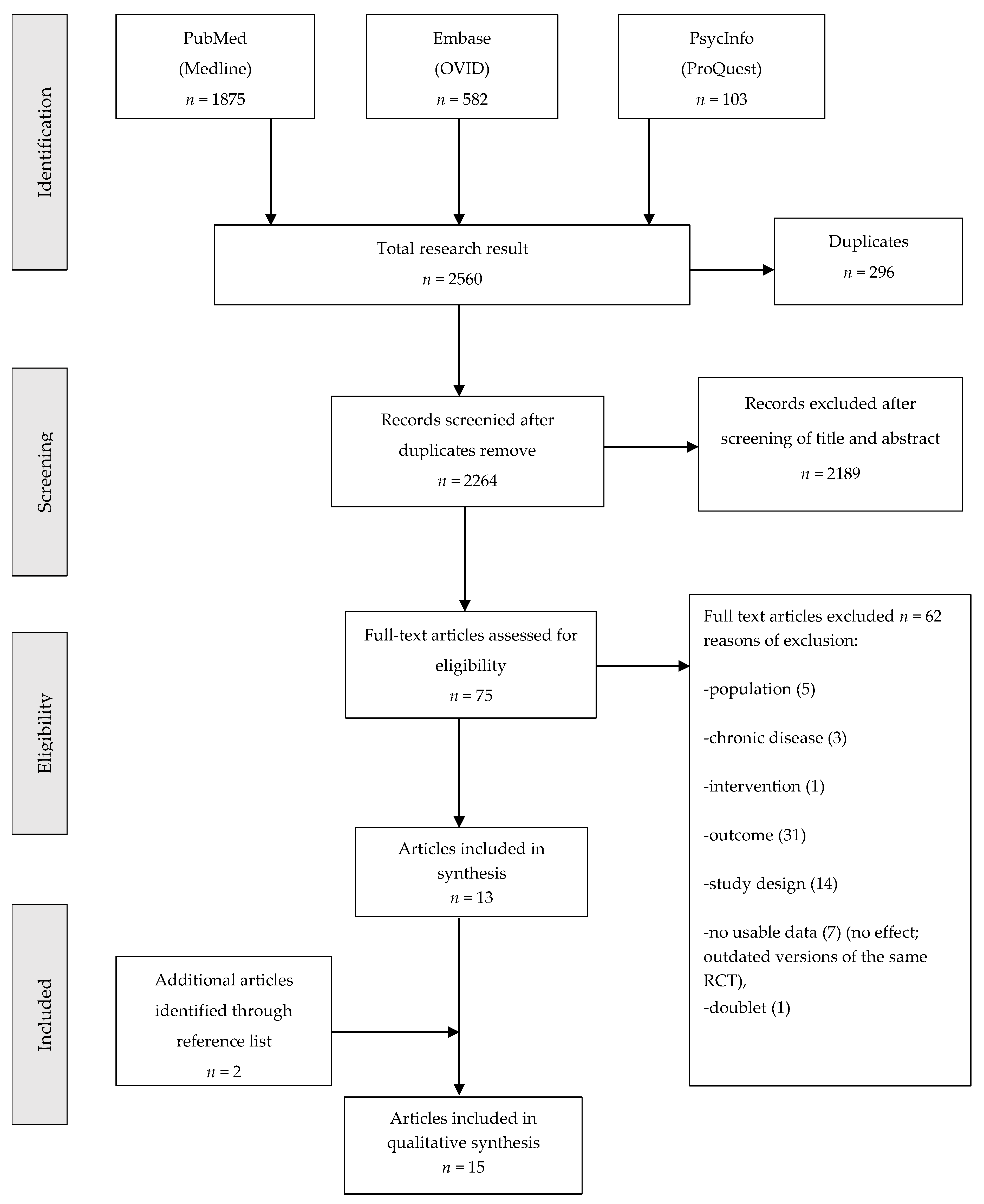
2.3. Selection of Studies
2.4. Quality Assessment
2.5. Data Extraction and Synthesis
3. Results
3.1. Study, Participants, and Interventions Characteristics
3.2. Effects of Interventions
3.2.1. Workplace-Oriented Intervention Programs
3.2.2. Cognitive Behavioral Therapy Interventions
3.2.3. Self-Management Programs
3.2.4. Vocational Rehabilitation (VR) Programs
3.2.5. Coaching Interventions
3.2.6. Comparative Intervention Strategies
3.2.7. Interventions That Prevent or Slow Down Chronicity
3.3. Secondary Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Detaille, S.I.; Heerkens, Y.F.; Engels, J.A.; van der Gulden, J.W.; van Dijk, F.J. Effect evaluation of a self-management program for dutch workers with a chronic somatic disease: A randomized controlled trial. J. Occup. Rehabil. 2013, 23, 189–199. [Google Scholar] [CrossRef]
- World Health Organization. Noncommunicable Diseases: Progress Monitor 2017; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Busse, R.; Blümel, M.; Scheller-Kreinsen, D.; Zentner, A. Tackling Chronic Disease in Europe. Strategies, Interventions and Challenges; WHO Regional Office for Europe: Copenhagen, Denmark, 2010. [Google Scholar]
- Hapke, U.; Bretschneider, J.; Thom, J. Depression in der Bevölkerung: Diagnoseraten im Versorgungskontext und epidemiologische Befunde. Epid Bull. 2017, 14, 121–123. [Google Scholar]
- International Diabetes Federation; Alberti, G.; Zimmet, P.; Shaw, J.; Grundy, S.M. The IDF Consensus Worldwide Definition of the Metabolic Syndrome; International Diabetes Federation: Brussels, Belgium, 2006. [Google Scholar]
- World Health Organization. Depression and Other Common Mental Disorders. Global Health Estimates. Available online: http://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf?sequence=1 (accessed on 16 August 2018).
- OECD/EU. Health at a Glance: Europe 2016: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2016; Available online: https://doi.org/10.1787/9789264265592-en (accessed on 16 August 2018).
- Angerer, P.; Wege, N. Psychische erkrankungen—Auswirkungen auf die arbeitsfähigkeit und versorgung psychisch erkrankter erwerbstätiger. Psychiatrie 2013, 10, 71–81. [Google Scholar]
- Vooijs, M.; Leensen, M.C.J.; Hoving, J.L.; Wind, H.; Frings-Dresen, M.H.W. Interventions to enhance work participation of workers with a chronic disease: A systematic review of reviews. Occup. Environ. Med. 2015, 72, 820–826. [Google Scholar] [CrossRef]
- Weber, A.; Peschkes, L.; de Boer, W.E.L. Return to Work—Arbeit für Alle. Grundlagen der Beruflichen Reintegration; Gentner: Stuttgart, Germany, 2015. [Google Scholar]
- Lamore, K.; Dubois, T.; Rothe, U.; Leonardi, M.; Girard, I.; Manuwald, U.; Nazarov, S.; Silvaggi, F.; Guastafierro, E.; Scaratti, C.; et al. Return to work interventions for cancer survivors: A systematic review and a methodological critique. Int. J. Environ. Res. Public Health 2019, 16, 1343. [Google Scholar] [CrossRef] [PubMed]
- Nöllenheidt, C.; Brenscheidt, S.; Bundesanstalt für Arbeitsschutz und Arbeitsmedizin. Arbeitswelt im Wandel. Zahlen—Daten—Fakten. Available online: https://www.baua.de/DE/Angebote/Publikationen/Praxis/A95.pdf?__blob=publicationFile&v=1 (accessed on 24 September 2018).
- Munir, F.; Yarker, J.; Haslam, C.; Kazi, A.; Cooper, L.; Mackay, C.; Myron, R. Returning to Work. The Role of Depression; Mental Health Foundation: London, UK, 2009. [Google Scholar]
- Collins, J.J.; Baase, C.M.; Sharda, C.E.; Ozminkowski, R.J.; Nicholson, S.; Billotti, G.M.; Turpin, R.S.; Olson, M.; Berger, M.L. The assessment of chronic health conditions on work performance, absence, and total economic impact for employers. J. Occup. Environ. Med. 2005, 47, 547–557. [Google Scholar] [CrossRef] [PubMed]
- American Lung Association Epidemiology and Statistics Unit Trends in COPD (Chronic Bronchitis and Emphysema). Morbidity and Mortality. 2013. Available online: http://www.lung.org/assets/documents/research/copd-trend-report.pdf (accessed on 23 August 2018).
- Chen, W.; Thomas, J.; Sadatsafavi, M.; FitzGerald, J.M. Risk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis. Lancet Respir. Med. 2015, 3, 631–639. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Program, C.A.S. CASP (Insert Name of Checklist i.e. Randomized Controlled Trial). Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Randomised-Controlled-Trial-Checklist.pdf (accessed on 23 August 2018).
- De Buck, P.D.M.; Le Cessie, S.; Van Den Hout, W.B.; Peeters, A.J.; Ronday, H.K.; Westedt, M.L.; Breedveld, F.C.; Vlieland, T.P.M.V. Randomized comparison of a multidisciplinary job-retention vocational rehabilitation program with usual outpatient care in patients with chronic arthritis at risk for job loss. Arthritis Care Res. 2005, 53, 682–690. [Google Scholar] [CrossRef]
- Friedrich, M.; Gittler, G.; Arendasy, M.; Friedrich, K.M. Long-term effect of a combined exercise and motivational program on the level of disability of patients with chronic low back pain. Spine (Phila Pa 1976) 2005, 30, 995–1000. [Google Scholar] [CrossRef]
- Linton, S.J.; Andersson, T. Can chronic disability be prevented? A randomized trial of a cognitive-behavior intervention and two forms of information for patients with spinal pain. Discussion 2824. Spine (Phila Pa 1976) 2000, 25, 2825–2831. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, K.; Schoutens, A.M.C.; Frings-Dresen, M.H.W.; Sluiter, J.K. Evaluation of a randomized controlled trial on the effect on return to work with coaching combined with light therapy and pulsed electromagnetic field therapy for workers with work-related chronic stress. BMC Public Health 2017, 17, 761. [Google Scholar] [CrossRef]
- Ntsiea, M.V.; Van Aswegen, H.; Lord, S.; Olorunju, S.S. The effect of a workplace intervention programme on return to work after stroke: A randomised controlled trial. Clin. Rehabil. 2015, 29, 663–673. [Google Scholar] [CrossRef]
- Bakker, I.M.; Terluin, B.; van Marwijk, H.W.J.; van der Windt, D.A.W.M.; Rijmen, F.; van Mechelen, W.; Stalman, W.A.B. A cluster-randomised trial evaluating an intervention for patients with stress-related mental disorders and sick leave in primary care. PLoS Clin. Trials 2007, 2, e26. [Google Scholar] [CrossRef]
- Varekamp, I.; Verbeek, J.H.; de Boer, A.; van Dijk, F.J.H. Effect of job maintenance training program for employees with chronic disease—A randomized controlled trial on self-efficacy, job satisfaction, and fatigue. Scand. J. Work Environ. Health 2011, 37, 288–297. [Google Scholar] [CrossRef]
- McGonagle, A.K.; Beatty, J.E.; Joffe, R. Coaching for workers with chronic illness: Evaluating an intervention. J. Occup. Health Psychol. 2014, 19, 385–398. [Google Scholar] [CrossRef]
- Bergstrom, C.; Jensen, I.; Hagberg, J.; Busch, H.; Bergstrom, G. Effectiveness of different interventions using a psychosocial subgroup assignment in chronic neck and back pain patients: A 10-year follow-up. Disabil. Rehabil. 2012, 34, 110–118. [Google Scholar] [CrossRef]
- Lambeek, L.C.; Van Mechelen, W.; Knol, D.L.; Loisel, P.; Anema, J.R. Randomised controlled trial of integrated care to reduce disability from chronic low back pain in working and private life. BMJ (Online) 2010, 340, C1035. [Google Scholar] [CrossRef]
- Dalgaard, V.L.; Andersen, L.P.S.; Andersen, J.H.; Willert, M.V.; Carstensen, O.; Glasscock, D.J. Work-focused cognitive behavioral intervention for psychological complaints in patients on sick leave due to work-related stress: Results from a randomized controlled trial. J. Negat. Results Biomed. 2017, 16, 13. [Google Scholar] [CrossRef]
- Wong, K.K.; Chiu, R.; Tang, B.; Mak, D.; Liu, J.; Chiu, S.N. A randomized controlled trial of a supported employment program for persons with long-term mental illness in Hong Kong. Psychiatr. Serv. 2008, 59, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Christensen, F.B.; Laurberg, I.; Bunger, C.E. Importance of the back-cafe concept to rehabilitation after lumbar spinal fusion: A randomized clinical study with a 2-year follow-up. Spine (Phila Pa 1976) 2003, 28, 2561–2569. [Google Scholar] [CrossRef] [PubMed]
- Bendix, T.; Bendix, A.; Labriola, M.; Haestrup, C.; Ebbehoj, N. Functional restoration versus outpatient physical training in chronic low back pain. A randomized comparative study. Spine 2000, 25, 2494–2500. [Google Scholar] [CrossRef] [PubMed]
- Varekamp, I.; Verbeek, J.H.A.M.; Van Dijk, F.J.H. How can we help employees with chronic diseases to stay at work? A review of interventions aimed at job retention and based on an empowerment perspektive. Int. Arch. Occup. Environ. Health 2006, 80, 87–97. [Google Scholar] [CrossRef]
- Varekamp, I.; van Dijk, F.J.; Kroll, L.E. Workers with a chronic disease and work disability. Problems and solutions. Bundesgesundheitsblatt Gesundh. Gesundh. 2013, 56, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Van Vilsteren, M.; van Oostrom, S.H.; de Vet, H.C.W.; Franche, R.L.; Boot, C.R.L.; Anema, J.R. Workplace interventions to prevent work disability in workers on sick leave. Cochrane Database Syst. Rev. 2015, 10, CD006955. [Google Scholar] [CrossRef] [PubMed]
- Sabariego, C.; Coenen, M.; Ito, E.; Fheodoroff, K.; Scaratti, C.; Leonardi, M.; Vlachou, A.; Stavroussi, P.; Brecelj, V.; Kovacˇic, D.S.; et al. Effectiveness of integration and re-integration into work strategies for persons with chronic conditions: A systematic review of European strategies. Int. J. Environ. Res. Public Health 2018, 15, 552. [Google Scholar] [CrossRef] [PubMed]
- Hoefsmit, N.; Houkes, I.; Nijhuis, F.J. Intervention characteristics that facilitate return to work after sickness absence: A systematic literature review. J. Occup. Rehabil. 2012, 22, 462–477. [Google Scholar] [CrossRef]
- Richardson, K.M.; Rothstein, H.R. Effects of occupational stress management intervention programs: A meta-analysis. J. Occup. Health Psychol. 2008, 13, 69–93. [Google Scholar] [CrossRef]
- Lindner, H.; Menzies, D.; Kelly, J.; Taylor, S.; Shearer, M. Coaching for behaviour change in chronic disease: A review of the literature and the implications for coaching as a self-management intervention. Aust. J. Prim. Health 2003, 9, 177–185. [Google Scholar] [CrossRef]


{kind=link}
| Author | CASP Questions (Q) | Judgement | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Section A 1 | Section B 2 | Section C 3 | Score 4 | |||||||||||
| Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | ∑ yes | ∑ no | ∑ can’t tell | |
| Bakker et al. [24] | + | + | + | + | + | + | + | + | + | + | + | 11 | ||
| Bendix et al. [32] | + | + | + | − | + | + | + | + | + | + | − | 9 | 2 | |
| Bergström et al. [27] | + | + | + | + | + | + | + | + | + | + − | + | 10 | 1 | |
| Christensen et al. [31] | + | + − | + | + − | + − | + | + | + − | + | + | + − | 6 | 5 | |
| Daalgard et al. [29] | + | + | + | + − | + | + | + | + | + | + | + | 10 | 1 | |
| De Buck et al. [19] | + | + | + | + | + | + | + | + | + | + | + | 11 | ||
| Detaille et al. [1] | + | + | + | + | + | + | + | + | + | + − | + − | 9 | 2 | |
| Friedrich et al. [20] | + | + | + | + | + | + | + | + | + | + | + | 11 | ||
| Lambeek et al. [28] | + | + | + | − | + | + | + | + | + | + | + | 10 | 1 | |
| Linton et al. [21] | + | + | + | + | + | + | + | + | + | + | + | 11 | ||
| McGonagle et al. [26] | + | + | − | + − | + | + | + | + | + | + | + | 9 | 1 | 1 |
| Nieuwenhuijsen et al. [22] | + | + | + | + | + | + | + | + | + | + | + | 11 | ||
| Ntsiea et al. [23] | + | + | + | + | + | + | + | + | + | + | + | 11 | ||
| Varekamp et al. [25] | + | + | + | − | + − | + | + | + | + | + | + − | 8 | 1 | 2 |
| Kin Wong et al. [30] | + | + | + | − | + | + | + | + | + − | + | + − | 8 | 1 | 2 |
| Number of Studies | Number of Participants | |
|---|---|---|
| Country of publication | ||
| Netherlands | 6 | |
| Denmark | 3 | |
| Sweden | 2 | |
| Austria | 1 | |
| USA | 1 | |
| South Africa | 1 | |
| China | 1 | |
| Intervention adapted to one of chronic disease | ||
| Diabetes | 0 | 0 |
| Cardiovascular diseases and neurological disease (stroke) | 1 | 80 (4%) |
| Metabolic vascular syndrome | 0 | 0 |
| Respiratory disease | 0 | 0 |
| Mental diseases | 5 | 851 (41%) |
| Musculoskeletal disorders | 7 | 956 (46%) |
| Different chronic disease | 2 | 181 (9%) |
| Interventions | ||
| Workplace oriented intervention programs | 4 | |
| Cognitive behavioral therapy interventions | 2 | |
| Self-management programs | 1 | |
| Vocational rehabilitation programs | 1 | |
| Coaching interventions | 2 | |
| Comparative intervention strategies | 3 | |
| Interventions that prevent or slow down chronicity | 2 | |
| Participants (N included in the intervention) | ||
| Total | 2068 | |
| female | 1319 (64%) | |
| male | 749 (36%) |
| Outcome/Diseases | Intervention | Study n | Participants n | Statistical method | Effect size |
|---|---|---|---|---|---|
| 1. RTW (lasting RTW, RTW rate, RTW percentage, employment rate, work resumed) | 5 | ||||
| 1.1. Adjustment disorder | Work focused CBT | 1 | 163 | Hazard Ratio (95% CI) | 1.7 (1.01 to 2.44) |
| 1.2. Work-related chronic stress | PEMF | 1 | 84 | Mean difference p-value | 0.92 |
| 1.3. Stroke | Work place intervention | 1 | 80 | Odds ratio (95% CI) | 5.2 (1.8 to 15.0) |
| 1.4. Long-term mental illness | Supported employment program | 1 | 92 | Odds ratio (95% CI) | 5.63 (2.28 to 13.84) |
| 1.5. Isthmic spondylolisthesis | Three different rehabilitation programs | 1 | 90 | Mean difference p-value | 0.04 |
| 2. Work ability | 4 | ||||
| 2.1. Chronic low back pain | 2.1.1. Functional restoration program | 2 | 99 | Mean difference p-value | 0.64 |
| 2.1.2 Vocational rehabilitation | 56 | Mean difference p-value | 0.005 | ||
| 2.2. Chronic rheumatic disease | Job-retention vocational rehabilitation program | 1 | 140 | Mean difference p-value | 0.13 |
| 2.3. Different diseases | Phone-based coaching | 1 | 59 | Pre-mean (SD) | 3.39 (0.75) |
| Post-mean (SD) | 3.82 (0.39) | ||||
| 3. Sick leave until full RTW, long-term sick leave, sickness absence | 4 | ||||
| 3.1. Stress related mental disease | 1 | 433 | Hazard Ratio (95% CI) | 1.06 (0.87 to 1.29) | |
| 3.2. Chronic low back pain | 3.2.1. Different intervention (behavioral oriented physiotherapy, cognitive behavioral therapy, behavioral medicine rehabilitation) using a psychosocial subgroup | 2 | |||
| 194 | mean difference, (95% CI) | BM: −16.08, (−38.0 to 5.8) PT: −0.55, (−22.5 to 21.4), CBT: −7.79, (−26.9 to 11.3) | |||
| 3.2.2. Workplace and patient-oriented interventions | 134 | Hazard Ratio (95% CI) | 1.9 (1.2 to2.8) | ||
| 3.3. Spinal pain | Cognitive behavioral intervention and two forms of information | 1 | 243 | Mean difference p-value | <0.05, RR = 9.3 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nazarov, S.; Manuwald, U.; Leonardi, M.; Silvaggi, F.; Foucaud, J.; Lamore, K.; Guastafierro, E.; Scaratti, C.; Lindström, J.; Rothe, U. Chronic Diseases and Employment: Which Interventions Support the Maintenance of Work and Return to Work among Workers with Chronic Illnesses? A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1864. https://doi.org/10.3390/ijerph16101864
Nazarov S, Manuwald U, Leonardi M, Silvaggi F, Foucaud J, Lamore K, Guastafierro E, Scaratti C, Lindström J, Rothe U. Chronic Diseases and Employment: Which Interventions Support the Maintenance of Work and Return to Work among Workers with Chronic Illnesses? A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(10):1864. https://doi.org/10.3390/ijerph16101864
Chicago/Turabian StyleNazarov, Soja, Ulf Manuwald, Matilde Leonardi, Fabiola Silvaggi, Jérôme Foucaud, Kristopher Lamore, Erika Guastafierro, Chiara Scaratti, Jaana Lindström, and Ulrike Rothe. 2019. "Chronic Diseases and Employment: Which Interventions Support the Maintenance of Work and Return to Work among Workers with Chronic Illnesses? A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 10: 1864. https://doi.org/10.3390/ijerph16101864
APA StyleNazarov, S., Manuwald, U., Leonardi, M., Silvaggi, F., Foucaud, J., Lamore, K., Guastafierro, E., Scaratti, C., Lindström, J., & Rothe, U. (2019). Chronic Diseases and Employment: Which Interventions Support the Maintenance of Work and Return to Work among Workers with Chronic Illnesses? A Systematic Review. International Journal of Environmental Research and Public Health, 16(10), 1864. https://doi.org/10.3390/ijerph16101864