Air Pollution/Irritants, Asthma Control, and Health-Related Quality of Life among 9/11-Exposed Individuals with Asthma

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
2.2. Study Outcomes and Variables
2.2.1. Determining Air Pollution/Irritants as Trigger
2.2.2. Asthma Control and HRQoL
2.3. Covariates
2.4. Statistical Analyses
3. Results
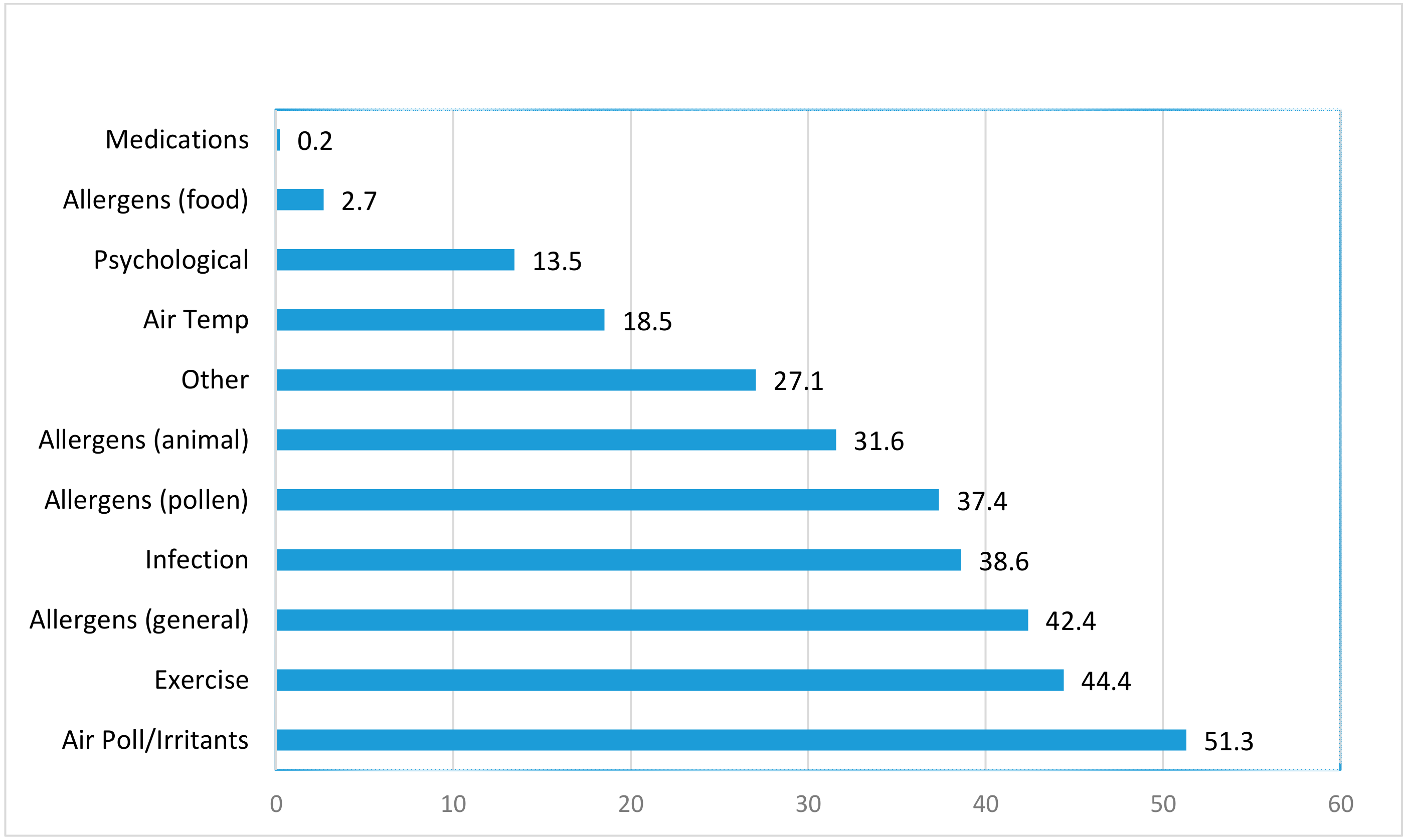
3.1. Asthma Trigger
3.2. Self-Reported Air Pollution/Irritants as Trigger and Asthma Control
3.3. Asthma Control and HRQoL
3.4. Mental Health, Asthma Control and HRQoL
4. Discussion
4.1. Main Findings
4.2. Air Pollution/Irritants and Asthma Control
4.3. Asthma Control and HRQoL
4.4. Mental Health, Air Pollution/Irritants, and Asthma Control
4.5. Strength and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Nurmagambetov, T.; Kuwahara, R.; Garbe, P. The Economic Burden of Asthma in the United States, 2008–2013. Ann. Am. Thorac. Soc. 2018, 15, 348–356. [Google Scholar] [CrossRef]
- Jordan, H.T.; Stellman, S.D.; Reibman, J.; Farfel, M.R.; Brackbill, R.M.; Friedman, S.M.; Li, J.; Cone, J.E. Factors associated with poor control of 9/11-related asthma 10–11 years after the 2001 World Trade Center terrorist attacks. J. Asthma 2015, 52, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Price, D.; Dale, P.; Elder, E.; Chapman, K.R. Types, frequency and impact of asthma triggers on patients’ lives: A quantitative study in five European countries. J. Asthma 2014, 51, 127–135. [Google Scholar] [CrossRef]
- Ritz, T.; Steptoe, A.; Bobb, C.; Harris, A.H.; Edwards, M. The asthma trigger inventory: Validation of a questionnaire for perceived triggers of asthma. Psychosom. Med. 2006, 68, 956–965. [Google Scholar] [CrossRef] [PubMed]
- Vernon, M.K.; Wiklund, I.; Bell, J.A.; Dale, P.; Chapman, K.R. What do we know about asthma triggers? A review of the literature. J. Asthma 2012, 49, 991–998. [Google Scholar] [CrossRef]
- Amato, M.D.; Cecchi, L.; Annesi-Maesano, I.; d’Amato, G. News on Climate Change, Air Pollution, and Allergic Triggers of Asthma. J. Investig. Allergol. Clin. Immunol. 2018, 28, 91–97. [Google Scholar] [CrossRef] [Green Version]
- Goksel, O.; Celik, G.E.; Erkekol, F.O.; Gullu, E.; Mungan, D.; Misirligil, Z. Triggers in adult asthma: Are patients aware of triggers and doing right? Allergol. Immunopathol. (Madr.) 2009, 37, 122–128. [Google Scholar] [CrossRef]
- Morales-Raveendran, E.; Goodman, E.; West, E.; Cone, J.E.; Katz, C.; Weiss, J.; Feldman, J.M.; Harrison, D.; Markowitz, S.; Federman, A.; et al. Associations between asthma trigger reports, mental health conditions, and asthma morbidity among world trade center rescue and recovery workers. J. Asthma 2018, 1–8. [Google Scholar] [CrossRef]
- Sharma, K.I.; Abraham, R.; Mowrey, W.; Toh, J.; Rosenstreich, D.; Jariwala, S. The association between pollutant levels and asthma-related emergency department visits in the Bronx after the World Trade Center attacks. J. Asthma 2018, 1–7. [Google Scholar] [CrossRef]
- Gonzalez-Barcala, F.J.; de la Fuente-Cid, R.; Tafalla, M.; Nuevo, J.; Caamano-Isorna, F. Factors associated with health-related quality of life in adults with asthma. A cross-sectional study. Multidiscip. Respir. Med. 2012, 7, 32. [Google Scholar] [CrossRef]
- Chen, H.; Gould, M.K.; Blanc, P.D.; Miller, D.P.; Kamath, T.V.; Lee, J.H.; Sullivan, S.D.; TENOR Study Group. Asthma control, severity, and quality of life: Quantifying the effect of uncontrolled disease. J. Allergy Clin. Immunol. 2007, 120, 396–402. [Google Scholar] [CrossRef]
- Archea, C.; Yen, I.H.; Chen, H.; Eisner, M.D.; Katz, P.P.; Masharani, U.; Yelin, E.H.; Earnest, G.; Blanc, P.D. Negative life events and quality of life in adults with asthma. Thorax 2007, 62, 139–146. [Google Scholar] [CrossRef] [Green Version]
- Luskin, A.T.; Chipps, B.E.; Rasouliyan, L.; Miller, D.P.; Haselkorn, T.; Dorenbaum, A. Impact of asthma exacerbations and asthma triggers on asthma-related quality of life in patients with severe or difficult-to-treat asthma. J. Allergy Clin. Immunol. Pract. 2014, 2, 544–552. [Google Scholar] [CrossRef]
- Upton, J.; Lewis, C.; Humphreys, E.; Price, D.; Walker, S. Asthma-specific health-related quality of life of people in Great Britain: A national survey. J. Asthma 2016, 53, 975–982. [Google Scholar] [CrossRef]
- Geraldo Jose Cunha, A.; Zbonik Mendes, A.; Dias Wanderley de Carvalho, F.; Aparecida Ribeiro de Paula, M.; Goncalves Brasil, T. The impact of asthma on quality of life and anxiety: A pilot study. J. Asthma 2018, 1–6. [Google Scholar] [CrossRef]
- Brackbill, R.M.; Hadler, J.L.; DiGrande, L.; Ekenga, C.C.; Farfel, M.R.; Friedman, S.; Perlman, S.E.; Stellman, S.D.; Walker, D.J.; Wu, D.; et al. Asthma and posttraumatic stress symptoms 5 to 6 years following exposure to the World Trade Center terrorist attack. JAMA 2009, 302, 502–516. [Google Scholar] [CrossRef]
- Farfel, M.; DiGrande, L.; Brackbill, R.; Prann, A.; Cone, J.; Friedman, S.; Walker, D.J.; Pezeshki, G.; Thomas, P.; Galea, S.; et al. An overview of 9/11 experiences and respiratory and mental health conditions among World Trade Center Health Registry enrollees. J. Urban Health Bull. N. Y. Acad. Med. 2008, 85, 880–909. [Google Scholar] [CrossRef]
- National Asthma Education and Prevention Program. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. National Heart, Lung, and Blood Institute. Available online: https://www.ncbi.nlm.nih.gov/books/NBK7232/ (accessed on 28 May 2019).
- Moriarty, D.G.; Zack, M.M.; Kobau, R. The Centers for Disease Control and Prevention’s Healthy Days Measures-population tracking of perceived physical and mental health over time. Health Qual. Life Outcomes 2003, 1, 37. [Google Scholar] [CrossRef]
- Center for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion. Division of Population Health Health-Related Quality of Life (HRQOL). Available online: https://www.cdc.gov/hrqol/syntax.htm (accessed on 3 May 2019).
- Blanchard, E.B.; Jones-Alexander, J.; Buckley, T.C.; Forneris, C.A. Psychometric properties of the PTSD Checklist (PCL). Behav. Res. Ther. 1996, 34, 669–673. [Google Scholar] [CrossRef]
- Ventureyra, V.A.; Yao, S.N.; Cottraux, J.; Note, I.; De Mey-Guillard, C. The validation of the Posttraumatic Stress Disorder Checklist Scale in posttraumatic stress disorder and nonclinical subjects. Psychother. Psychosom. 2002, 71, 47–53. [Google Scholar] [CrossRef]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Cohen, S.; Underwood, L.G.; Gottlieb, B.H. Social Support Measurement and Intervention: A Guide for Health and Social Scientists; Oxford University Press: Oxford, UK, 2000. [Google Scholar]
- Huang, G.; Zhou, W.; Qian, Y.; Fisher, B. Breathing the same air? Socioeconomic disparities in PM2.5 exposure and the potential benefits from air filtration. Sci. Total Environ. 2019, 657, 619–626. [Google Scholar] [CrossRef]
- Leas, B.F.; D’Anci, K.E.; Apter, A.J.; Bryant-Stephens, T.; Lynch, M.P.; Kaczmarek, J.L.; Umscheid, C.A. Effectiveness of indoor allergen reduction in asthma management: A systematic review. J. Allergy Clin. Immunol. 2018, 141, 1854–1869. [Google Scholar] [CrossRef] [Green Version]
- Bobb, C.; Ritz, T.; Rowlands, G.; Griffiths, C. Effects of allergen and trigger factor avoidance advice in primary care on asthma control: A randomized-controlled trial. Clin. Exp. Allergy 2010, 40, 143–152. [Google Scholar] [CrossRef]
- Rojano, B.; West, E.; Goodman, E.; Weiss, J.J.; de la Hoz, R.E.; Crane, M.; Crowley, L.; Harrison, D.; Markowitz, S.; Wisnivesky, J.P. Self-management behaviors in World Trade Center rescue and recovery workers with asthma. J. Asthma 2018, 1–11. [Google Scholar] [CrossRef]
- Sundh, J.; Wireklint, P.; Hasselgren, M.; Montgomery, S.; Stallberg, B.; Lisspers, K.; Janson, C. Health-related quality of life in asthma patients—A comparison of two cohorts from 2005 and 2015. Respir. Med. 2017, 132, 154–160. [Google Scholar] [CrossRef]
- Tarraf, H.; Al-Jahdali, H.; Al Qaseer, A.H.; Gjurovic, A.; Haouichat, H.; Khassawneh, B.; Mahboub, B.; Naghshin, R.; Montestruc, F.; Behbehani, N. Asthma control in adults in the Middle East and North Africa: Results from the ESMAA study. Respir. Med. 2018, 138, 64–73. [Google Scholar] [CrossRef]
- Pate, C.A.; Zahran, H.S.; Bailey, C.M. Impaired health-related quality of life and related risk factors among US adults with asthma. J. Asthma 2018, 1–9. [Google Scholar] [CrossRef]
- Correia de Sousa, J.; Pina, A.; Cruz, A.M.; Quelhas, A.; Almada-Lobo, F.; Cabrita, J.; Oliveira, P.; Yaphe, J. Asthma control, quality of life, and the role of patient enablement: A cross-sectional observational study. Prim. Care Respir. J. 2013, 22, 181–187. [Google Scholar] [CrossRef]
- Calciano, L.; Corsico, A.G.; Pirina, P.; Trucco, G.; Jarvis, D.; Janson, C.; Accordini, S. Assessment of asthma severity in adults with ever asthma: A continuous score. PLoS ONE 2017, 12, e0177538. [Google Scholar] [CrossRef] [PubMed]
- Siroux, V.; Boudier, A.; Anto, J.M.; Cazzoletti, L.; Accordini, S.; Alonso, J.; Cerveri, I.; Corsico, A.; Gulsvik, A.; Jarvis, D.; et al. Quality-of-life and asthma-severity in general population asthmatics: Results of the ECRHS II study. Allergy 2008, 63, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Ritz, T.; Wittchen, H.U.; Klotsche, J.; Muhlig, S.; Riedel, O.; sap-NEEDs Study Group. Asthma Trigger Reports Are Associated with Low Quality of Life, Exacerbations, and Emergency Treatments. Ann. Am. Thorac. Soc. 2016, 13, 204–211. [Google Scholar]
- Jayawardene, W.P.; Youssefagha, A.H.; Lohrmann, D.K.; El Afandi, G.S. Prediction of asthma exacerbations among children through integrating air pollution, upper atmosphere, and school health surveillances. Allergy Asthma Proc. 2013, 34, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, K.K.; Galanter, J.M.; Roth, L.A.; Oh, S.S.; Thakur, N.; Nguyen, E.A.; Thyne, S.; Farber, H.J.; Serebrisky, D.; Kumar, R.; et al. Early-life air pollution and asthma risk in minority children. The GALA II and SAGE II studies. Am. J. Respir. Crit. Care Med. 2013, 188, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Gemicioglu, B.; Bayram, H.; Cimrin, A.; Abadoglu, O.; Cilli, A.; Uzaslan, E.; Gunen, H.; Akyildiz, L.; Suerdem, M.; Ozlu, T.; et al. Asthma control and adherence in newly diagnosed young and elderly adult patients with asthma in Turkey. J. Asthma 2018, 1–9. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics at Wave 4 * | Total * | % Controlled | % Poorly-Controlled | % Very Poorly-Controlled |
|---|---|---|---|---|
| Gender | ||||
| Male | 3357 | 38.2 | 26.2 | 35.6 |
| Female | 2845 | 43.6 | 28.2 | 28.2 |
| Age | ||||
| <45 | 1026 | 59.2 | 22.2 | 18.6 |
| 45–64 | 3897 | 38.0 | 27.8 | 34.2 |
| ≥65 | 1279 | 33.9 | 29.2 | 36.9 |
| Race/Ethnicity | ||||
| White non-Hispanic | 4109 | 44.3 | 25.0 | 30.7 |
| Black non-Hispanic | 622 | 31.4 | 33.6 | 35.1 |
| Hispanic | 938 | 29.5 | 33.5 | 37.0 |
| Asian | 286 | 46.9 | 25.9 | 27.3 |
| Other | 247 | 38.5 | 24.3 | 37.3 |
| Marital Status | ||||
| Never married | 961 | 44.8 | 27.4 | 27.9 |
| Married/living with a partner | 3978 | 42.6 | 26.6 | 30.8 |
| Widowed, divorced, or separated | 1163 | 32.0 | 28.1 | 39.9 |
| Education | ||||
| College/post-graduate | 3194 | 52.5 | 24.1 | 23.5 |
| Some college | 1964 | 31.7 | 29.7 | 38.7 |
| High school or less | 970 | 20.3 | 31.4 | 48.3 |
| Smoking Status | ||||
| Never smoker | 3832 | 44.0 | 26.3 | 29.7 |
| Previous smoker | 1791 | 39.1 | 26.8 | 34.1 |
| Current smoker | 438 | 24.2 | 31.3 | 44.5 |
| BMI | ||||
| Normal (<25) | 1450 | 54.6 | 22.7 | 22.8 |
| Overweight (25–29) | 2111 | 41.8 | 27.5 | 30.7 |
| Obese (>30) | 2436 | 31.7 | 29.2 | 39.2 |
| Social Integration | ||||
| High | 5587 | 42.8 | 26.9 | 30.3 |
| Low | 411 | 16.8 | 28.7 | 54.5 |
| Depression | ||||
| No | 4384 | 50.2 | 25.9 | 23.9 |
| Yes | 1452 | 15.8 | 28.4 | 55.8 |
| Probable PTSD | ||||
| No | 4632 | 50.0 | 25.9 | 24.1 |
| Yes | 1452 | 12.4 | 29.5 | 58.1 |
| GERS | ||||
| No | 3450 | 50.7 | 25.1 | 24.2 |
| Yes | 2344 | 27.8 | 29.0 | 43.2 |
| Sleep Apnea | ||||
| No | 4081 | 49.7 | 25.6 | 24.7 |
| Yes | 1647 | 21.9 | 28.5 | 49.5 |
| Had at least one regular healthcare provider | ||||
| No | 415 | 42.4 | 28.2 | 29.4 |
| Yes | 5681 | 40.7 | 26.9 | 32.4 |
| Air pollution/irritants as an important trigger | ||||
| No | 2777 | 49.2 | 24.8 | 26.0 |
| Yes | 2926 | 30.3 | 29.9 | 39.8 |
| Dust cloud exposure at 9/11 | ||||
| No | 2587 | 46.9 | 25.3 | 27.8 |
| Yes | 3592 | 36.1 | 28.5 | 35.4 |
| Characteristics at Wave 4 * | Poorly-Controlled | Very Poorly-Controlled |
|---|---|---|
| Adjusted OR (95% CI) | Adjusted OR (95% CI) | |
| Gender | ||
| Female | referent | referent |
| Male | 1.08 (0.91–1.28) | 1.52 (1.27–1.82) |
| Age | ||
| <45 | referent | referent |
| 45–64 | 1.41 (1.13–1.75) | 1.53 (1.21–1.94) |
| ≥65 | 1.78 (1.36–2.33) | 2.13 (1.60–2.83) |
| Education | ||
| College/post-graduate | referent | referent |
| Some college | 1.44 (1.20–1.71) | 1.79 (1.50–2.15) |
| High school or less | 1.80 (1.39–2.33) | 2.76 (2.14–3.55) |
| Smoking Status | ||
| Never smoker | referent | referent |
| Former smoker | 1.07 (0.90–1.27) | 1.19 (1.00–1.42) |
| Current smoker | 2.11 (1.50–2.97) | 2.61 (1.86–3.67) |
| BMI | ||
| Normal (<25) | referent | referent |
| Overweight (25–29) | 1.32 (1.08–1.63) | 1.22 (0.98–1.52) |
| Obese (>30) | 1.58 (1.28–1.95) | 1.68 (1.35–2.10) |
| Social Integration | ||
| High | referent | referent |
| Low | 1.60 (1.09–2.37) | 1.77 (1.21–2.60) |
| Depression | ||
| No | referent | referent |
| Yes | 1.46 (1.14–1.87) | 2.32 (1.83–2.94) |
| Probable PTSD | ||
| No | referent | referent |
| Yes | 2.64 (2.04–3.43) | 3.39 (2.63–4.37) |
| GERS | ||
| No | referent | referent |
| Yes | 1.47 (1.24–1.73) | 1.72 (1.45–2.03) |
| Sleep Apnea | ||
| No | referent | referent |
| Yes | 1.38 (1.13–1.68) | 1.78 (1.46–2.16) |
| Dust cloud exposure at 9/11 | ||
| No | referent | referent |
| Yes | 1.22 (1.05–1.43) | 1.36 (1.16–1.59) |
| Air pollution/irritants | ||
| No | referent | referent |
| Yes | 1.70 (1.45–1.99) | 2.15 (1.83–2.53) |
| Characteristics at Wave 4 * | ≥14 Days of Poor Physical or Mental Health | ≥14 Days of Activity Limitation | Fair/Poor General Health |
|---|---|---|---|
| Adjusted OR (95% CI) | Adjusted OR (95% CI) | Adjusted OR (95% CI) | |
| Sex | |||
| Female | referent | referent | referent |
| Male | 0.81 (0.70–0.95) | 1.12 (0.92–1.35) | 1.16 (0.99–1.37) |
| Age | |||
| <45 | referent | referent | referent |
| 45–64 | 1.26 (1.03–1.55) | 1.35 (1.03–1.77) | 1.58 (1.28–1.97) |
| ≥65 | 1.33 (1.03–1.71) | 1.92 (1.40–2.63) | 1.76 (1.36–2.29) |
| Race/ethnicity | |||
| White non-Hispanic | referent | referent | referent |
| Black non-Hispanic | 1.05 (0.81–1.35) | 1.37 (1.03–1.81) | 1.32 (1.03–1.70) |
| Hispanic | 1.13 (0.91–1.40) | 1.05 (0.83–1.33) | 1.40 (1.13–1.73) |
| Asian | 1.10 (0.77–1.59) | 0.76 (0.46–1.25) | 2.46 (1.72–3.52) |
| Other | 1.11 (0.76–1.63) | 1.32 (0.87–2.01) | 1.48 (1.01–2.17) |
| Marital Status | |||
| Never married | referent | referent | referent |
| Married/living with a partner | 0.87 (0.71–1.07) | 0.71 (0.55–0.90) | 0.78 (0.64–0.97) |
| Widowed, divorced, or separated | 1.11 (0.87–1.43) | 0.93 (0.71–1.23) | 0.91 (0.71–1.17) |
| Highest Education Attainment | |||
| College/post-graduate | referent | referent | referent |
| Some college | 1.29 (1.09–1.51) | 1.47 (1.22–1.78) | 1.40 (1.19–1.65) |
| High school or less | 1.47 (1.18–1.84) | 1.94 (1.53–2.46) | 1.90 (1.53–2.37) |
| BMI | |||
| Normal (<25) | referent | referent | referent |
| Overweight (25–29) | 1.09 (0.90–1.32) | 0.98 (0.77–1.25) | 1.29 (1.05–1.58) |
| Obese (>30) | 1.17 (0.96–1.42) | 1.11 (0.87–1.41) | 1.50 (1.22–1.83) |
| Social Integration | |||
| High | referent | referent | referent |
| Low | 1.80 (1.25–2.59) | 1.51 (1.12–2.04) | 1.95 (1.40–2.70) |
| Depression | |||
| No | referent | referent | referent |
| Yes | 5.24 (4.22–6.51) | 3.18 (2.58–3.92) | 2.65 (2.17–3.24) |
| Probable PTSD | |||
| No | referent | referent | referent |
| Yes | 3.08 (2.46–3.86) | 2.13 (1.72–2.64) | 2.04 (1.66–2.51) |
| GERS | |||
| No | referent | referent | referent |
| Yes | 1.46 (1.25–1.70) | 1.57 (1.32–1.87) | 1.72 (1.48–2.00) |
| Sleep Apnea | |||
| No | referent | referent | referent |
| Yes | 1.55 (1.30–1.85) | 1.52 (1.25–1.83) | 1.81 (1.53–2.14) |
| Asthma Control | |||
| Controlled | referent | referent | referent |
| Poorly-controlled | 2.12 (1.78–2.52) | 2.17 (1.70–2.77) | 2.66 (2.22–3.18) |
| Very poorly-controlled | 3.60 (3.02–4.30) | 4.37 (3.48–5.50) | 4.92 (4.11–5.89) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yung, J.; Osahan, S.; Friedman, S.M.; Li, J.; Cone, J.E. Air Pollution/Irritants, Asthma Control, and Health-Related Quality of Life among 9/11-Exposed Individuals with Asthma. Int. J. Environ. Res. Public Health 2019, 16, 1924. https://doi.org/10.3390/ijerph16111924
Yung J, Osahan S, Friedman SM, Li J, Cone JE. Air Pollution/Irritants, Asthma Control, and Health-Related Quality of Life among 9/11-Exposed Individuals with Asthma. International Journal of Environmental Research and Public Health. 2019; 16(11):1924. https://doi.org/10.3390/ijerph16111924
Chicago/Turabian StyleYung, Janette, Sukhminder Osahan, Stephen M. Friedman, Jiehui Li, and James E. Cone. 2019. "Air Pollution/Irritants, Asthma Control, and Health-Related Quality of Life among 9/11-Exposed Individuals with Asthma" International Journal of Environmental Research and Public Health 16, no. 11: 1924. https://doi.org/10.3390/ijerph16111924
APA StyleYung, J., Osahan, S., Friedman, S. M., Li, J., & Cone, J. E. (2019). Air Pollution/Irritants, Asthma Control, and Health-Related Quality of Life among 9/11-Exposed Individuals with Asthma. International Journal of Environmental Research and Public Health, 16(11), 1924. https://doi.org/10.3390/ijerph16111924