Development and Implementation of an Internet Survey to Assess Community Health in the Face of a Health Crisis: Data from the Pregnancy and Birth Survey of the Fukushima Health Management Survey, 2016

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Survey Methods
2.3. Analysis Methods
2.4. Ethical Considerations
3. Results
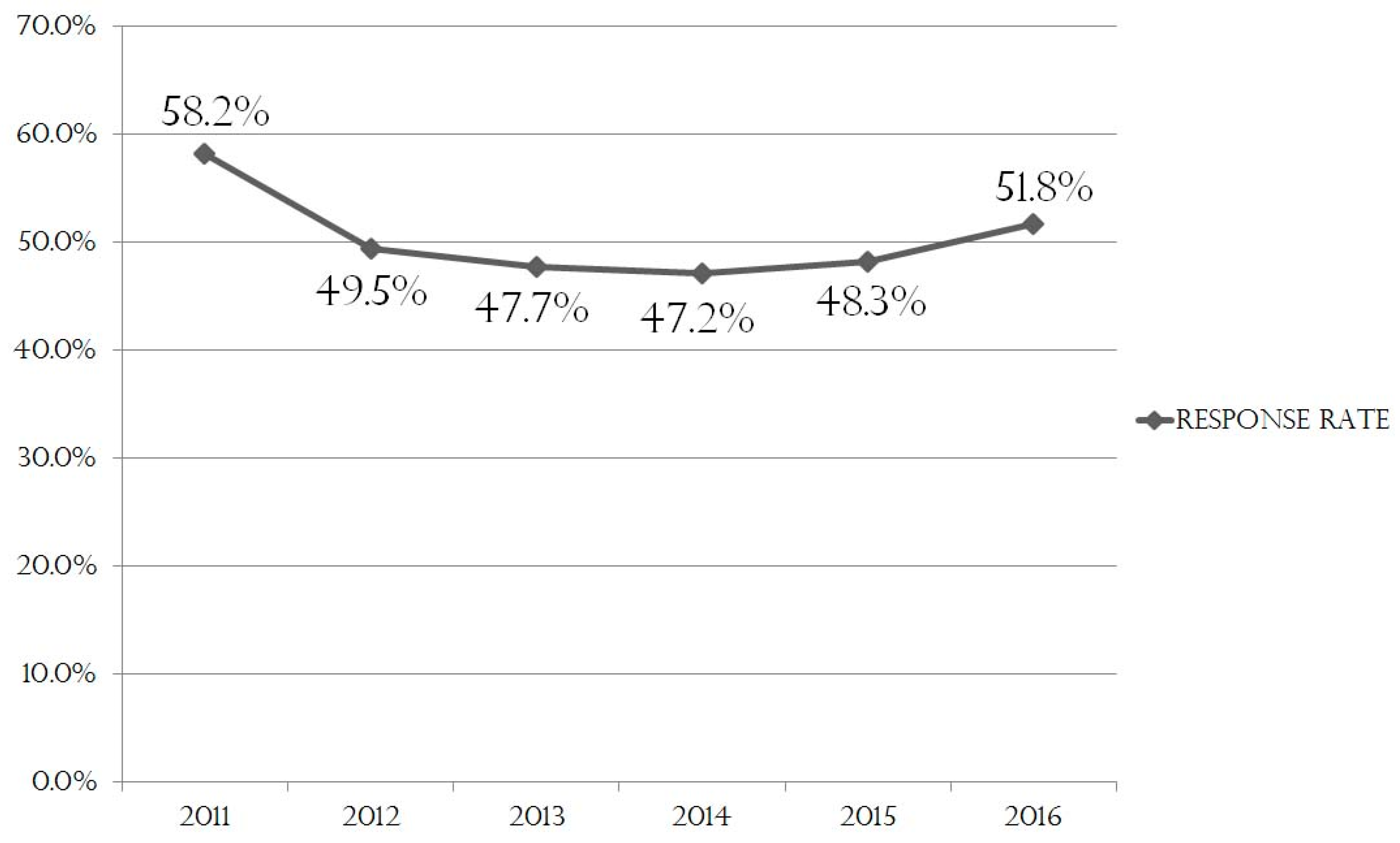
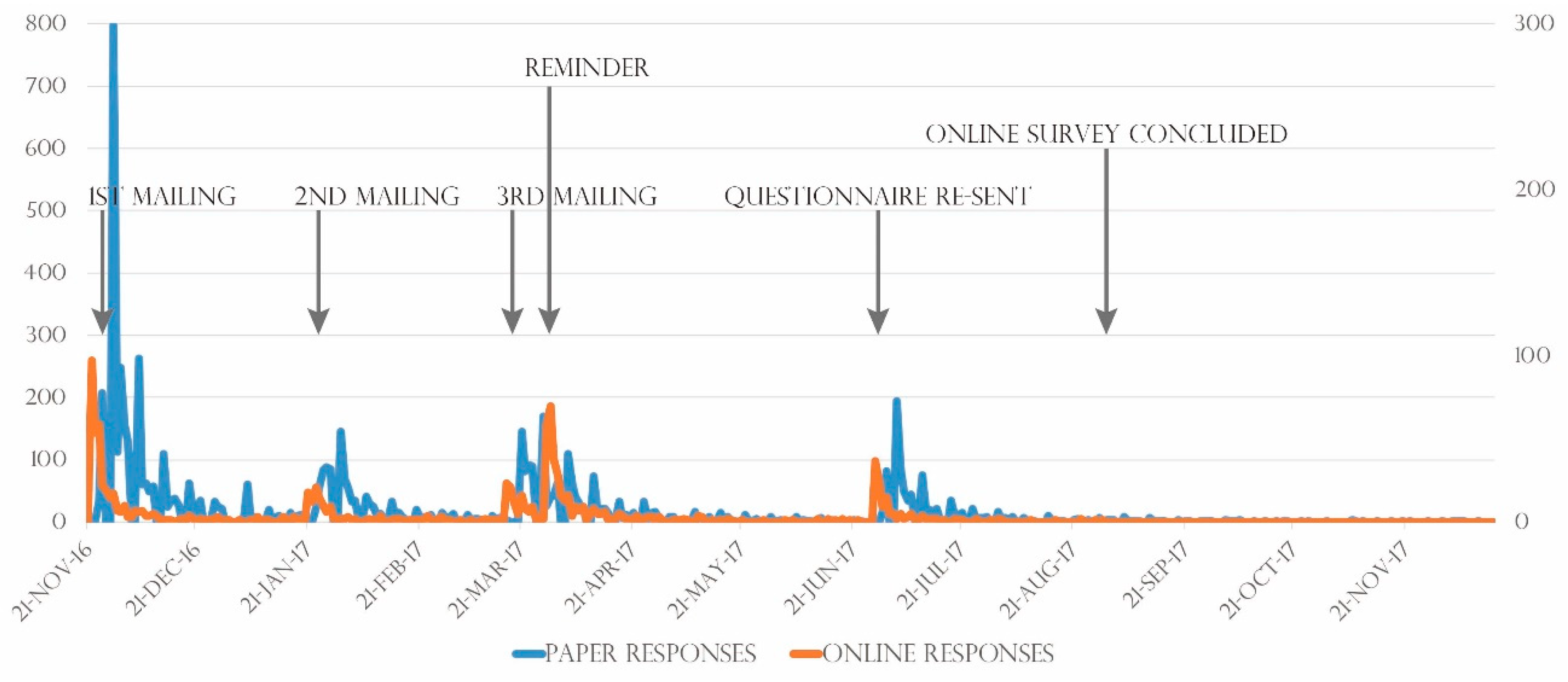
3.1. Response Rates
3.2. Characteristics of Online Respondents
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Yasumura, S.; Hosoya, M.; Yamashita, S.; Kamiya, K.; Abe, M.; Akashi, M.; Kodama, K.; Ozasa, K. Fukushima Health Management Survey Group. Study protocol for the Fukushima Health Management Survey. J. Epidemiol. 2012, 22, 375–383. [Google Scholar] [CrossRef]
- Harville, E.; Xiong, X.; Buekens, P. Disasters and perinatal health: A systematic review. Obstet. Gynecol. Surv. 2010, 65, 713–728. [Google Scholar] [CrossRef] [PubMed]
- Fujimori, K.; Kyozuka, H.; Yasuda, S.; Goto, A.; Yasumura, S.; Ota, M.; Ohtsuru, A.; Nomura, Y.; Hata, K.; Suzuki, K.; et al. Pregnancy and Birth Survey Group of the Fukushima Health Management Survey. Pregnancy and birth survey after the Great East Japan Earthquake and Fukushima Daiichi Nuclear Power Plant accident in Fukushima prefecture. Fukushima J. Med. Sci. 2014, 60, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Dolk, H.; Nichos, R. Evaluation of the impact of Chernobyl on the prevalence of congenital anomalies in 16 regions of Europe. EUROCAT Working Group. Int. J. Epidemiol. 1999, 28, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, W. Fallout from the Chernobyl nuclear disaster and congenital malformations in Europe. Arch. Environ. Health 2001, 56, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Little, J. The Chernobyl accident, congenital anomalies and other reproductive outcomes. Paediatr. Perinat. Epidemiol. 1993, 7, 121–151. [Google Scholar] [CrossRef] [PubMed]
- Feshchenko, S.P.; Schröder, H.C.; Müller, W.E.; Lazjuk, G.I. Congenital malformations among newborns and developmental abnormalities among human embryos in Belarus after Chernobyl accident. Cell. Mol. Biol. (Noisy-le-grand) 2002, 48, 423–436. [Google Scholar]
- Akio, M.; Haniguchi, T.; Masahiro, T. Challenges in personal information protection and new methods of data collection in social surveys. E-J. GEO 2014, 9, 1–11. [Google Scholar] [CrossRef]
- Matsuda, E. New possibilities of internet surveys: Sharing information and lessons by tracing survey history. Policy Res. 2015, 9, 5–18. [Google Scholar]
- Deguchi, S. The utilities and challenges of conducting an internet survey. Jpn. J. Behav. 2015, 35, 47–57. [Google Scholar]
- Yasunaga, H.; Ide, H.; Imamura, T.; Ohe, K. Medical research using internet questionnaire in Japan. Nihon Koshu Eisei Zasshi 2006, 53, 40–50. [Google Scholar] [PubMed]
- Ministry of Internal Affairs and Communication. Promotion on Survey Using Online Mode. Available online: http://www.soumu.go.jp/main_content/000506432.pdf (accessed on 11 May 2019). (In Japanese)
- Ministry of Internal Affairs and Communication. Usage of Online Mode in 2015 Census. Available online: https://www.stat.go.jp/data/kokusei/2015/houdou/pdf/2016022601.pdf (accessed on 11 May 2019). (In Japanese)
- Matsuda, E. Issues of survey methodology in the 2015 Census Japan: Proposing a new questionnaire layout. Policy Res. 2015, 8, 45–72. (In Japanese) [Google Scholar]
- Hayashi, M. Differences in Results Between Internet and Paper Surveys. Telecommunications Advancement Foundation Research Gant Report. No. 32. 2017. Available online: https://www.taf.or.jp/files/items/747/File/030.pdf (accessed on 11 May 2019). (In Japanese).
- LimeSurvey Online Survey System Startup Guide. Available online: https://www.d-ip.jp/download/images/limesurvey250_startupguide_min.pdf (accessed on 20 August 2017).
- 2017 White Paper on Information and Communications in Japan: “Advent of Smartphone Society”. Available online: http://www.soumu.go.jp/johotsusintokei/whitepaper/ja/h29/pdf/n1100000.pdf (accessed on 20 August 2017).
- Nihei, T. A new trend in online surveys: An increase of smartphone users leads to new possibilities. Policy Res. 2015, 9, 59–66. [Google Scholar]
- Hohwü, L.; Lyshol, H.; Gissler, M.; Jonsson, S.H.; Petzold, M.; Obel, C. Web-based versus traditional paper questionnaires: A mixed-mode survey with a Nordic perspective. J. Med. Int. Res. 2013, 15, e173. [Google Scholar] [CrossRef] [PubMed]
- van Gelder, M.M.; Bretveld, R.W.; Roeleveld, N. Web-based questionnaires: The future in epidemiology? Am. J. Epidemiol. 2010, 172, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Rebecca, J.S.; Donna, M.B.; Helen, M.S.; Jeneva, L.O. Psychometric properties and norms for the strengths and difficulties questionnaire administered online in an Australian sample. Aust. Psychol. 2018, 53, 116–124. [Google Scholar]
- Sato, A.; Kitamiya, C.; Lee, S.; Menzawa, K. Neonate home-visit guidance by public health nurses and midwives: An evaluation indexed by reduction of mother’s child-care anxiety. Jpn. J. Public Health 2005, 53, 328–337. [Google Scholar]
- Zuidgeest, M.; Hendriks, M.; Koopman, L.; Spreeuwenberg, P.; Rademakers, J. A comparison of a postal survey and mixed-mode survey using a questionnaire on patients’ experiences with breast care. J. Med. Int. Res. 2011, 13, e68. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Paper Responses (n = 6029) | Online Responses (n = 1134) | AOR | 95% CI | p Value * | |
|---|---|---|---|---|---|
| Maternal age | |||||
| ≤24 years | 497 (83.5%) | 98 (16.5%) | 1.00 | ||
| 25−29 years | 1619 (82.2%) | 350 (17.8%) | 1.10 | 0.86–1.40 | 0.46 |
| 30−34 years | 2175 (84.8%) | 390 (15.2%) | 0.91 | 0.71–1.16 | 0.44 |
| ≥35 years | 1738 (85.4%) | 296 (14.6%) | 0.86 | 0.67–1.11 | 0.25 |
| Area of residence (3 regions of Fukushima) | |||||
| Nakadori (n = 4496) | 3790 (84.3%) | 706 (15.7%) | 1.00 | ||
| Hamadori (n = 1700) | 1425 (83.8%) | 275 (16.2%) | 1.03 | 0.89–1.20 | 0.68 |
| Aizu (n = 967) | 814 (84.2%) | 153 (15.8%) | 1.01 | 0.83–1.22 | 0.93 |
| Parity | |||||
| Primiparous | 2663 (80.8%) | 632 (19.2%) | 1.00 | ||
| Multiparous | 3155 (86.4%) | 495 (13.6%) | 0.68 | 0.59–0.77 | <0.001 |
| Singleton/Twin | |||||
| Singleton | 5975 (84.2%) | 1,125 (15.8%) | 1.00 | ||
| Twin | 52 (85.2%) | 9 (14.8%) | 0.94 | 0.46–1.92 | 0.87 |
| Paper Responses (n = 6029) | Online Responses (n = 1134) | p Value * | |
|---|---|---|---|
| Pregnancy outcome | |||
| Birth | 5958 (98.8%) | 1121 (98.9%) | |
| Other | 71 (1.2%) | 13 (1.1%) | 1.00 |
| Depressive tendency | |||
| No | 4732 (79.0%) | 896 (79.2%) | |
| Yes | 1261 (21.0%) | 236 (20.8%) | 0.76 |
| Preterm birth | |||
| No | 5817 (97.0%) | 1088 (96.9%) | |
| Yes | 180 (3.0%) | 35 (3.1%) | 0.68 |
| Low birth weight | |||
| No | 5415 (90.9%) | 1017 (91.0%) | |
| Yes | 544 (9.1%) | 101 (9.0%) | 0.97 |
| Congenital defects/abnormalities | |||
| No | 5748 (97.4%) | 1093 (97.7%) | |
| Yes | 156 (2.6%) | 26 (2.3%) | 0.63 |
| Paper Responses (n = 6029) | Online Responses (n = 1134) | p Value * | |
|---|---|---|---|
| Free response | |||
| No | 791 (13.1%) | 158 (13.9%) | |
| Yes | 5238 (86.9%) | 976 (86.1%) | 0.47 |
| Categorized content | |||
| Economic anxiety | |||
| No | 5955 (98.8%) | 1120 (98.8%) | |
| Yes | 74 (1.2%) | 14 (1.2%) | 1.00 |
| Physical or mental disorders | |||
| No | 5841 (96.9%) | 1113 (98.1%) | |
| Yes | 188 (3.1%) | 21 (1.9%) | <0.05 |
| Desire for childcare services | |||
| No | 5806 (96.3%) | 1099 (96.9%) | |
| Yes | 223 (3.7%) | 35 (3.1%) | 0.34 |
| Childcare consultations | |||
| No | 5799 (96.2%) | 1111 (98.0%) | |
| Yes | 230 (3.8%) | 23 (2.0%) | <0.01 |
| 164.3 ± 144.7 | 118.8 ± 105.5 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakano, H.; Ishii, K.; Goto, A.; Yasumura, S.; Ohira, T.; Fujimori, K. Development and Implementation of an Internet Survey to Assess Community Health in the Face of a Health Crisis: Data from the Pregnancy and Birth Survey of the Fukushima Health Management Survey, 2016. Int. J. Environ. Res. Public Health 2019, 16, 1946. https://doi.org/10.3390/ijerph16111946
Nakano H, Ishii K, Goto A, Yasumura S, Ohira T, Fujimori K. Development and Implementation of an Internet Survey to Assess Community Health in the Face of a Health Crisis: Data from the Pregnancy and Birth Survey of the Fukushima Health Management Survey, 2016. International Journal of Environmental Research and Public Health. 2019; 16(11):1946. https://doi.org/10.3390/ijerph16111946
Chicago/Turabian StyleNakano, Hironori, Kayoko Ishii, Aya Goto, Seiji Yasumura, Tetsuya Ohira, and Keiya Fujimori. 2019. "Development and Implementation of an Internet Survey to Assess Community Health in the Face of a Health Crisis: Data from the Pregnancy and Birth Survey of the Fukushima Health Management Survey, 2016" International Journal of Environmental Research and Public Health 16, no. 11: 1946. https://doi.org/10.3390/ijerph16111946
APA StyleNakano, H., Ishii, K., Goto, A., Yasumura, S., Ohira, T., & Fujimori, K. (2019). Development and Implementation of an Internet Survey to Assess Community Health in the Face of a Health Crisis: Data from the Pregnancy and Birth Survey of the Fukushima Health Management Survey, 2016. International Journal of Environmental Research and Public Health, 16(11), 1946. https://doi.org/10.3390/ijerph16111946