Assessment of Cardiometabolic Risk Factors, Physical Activity Levels, and Quality of Life in Stratified Groups up to 10 Years after Bariatric Surgery


 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
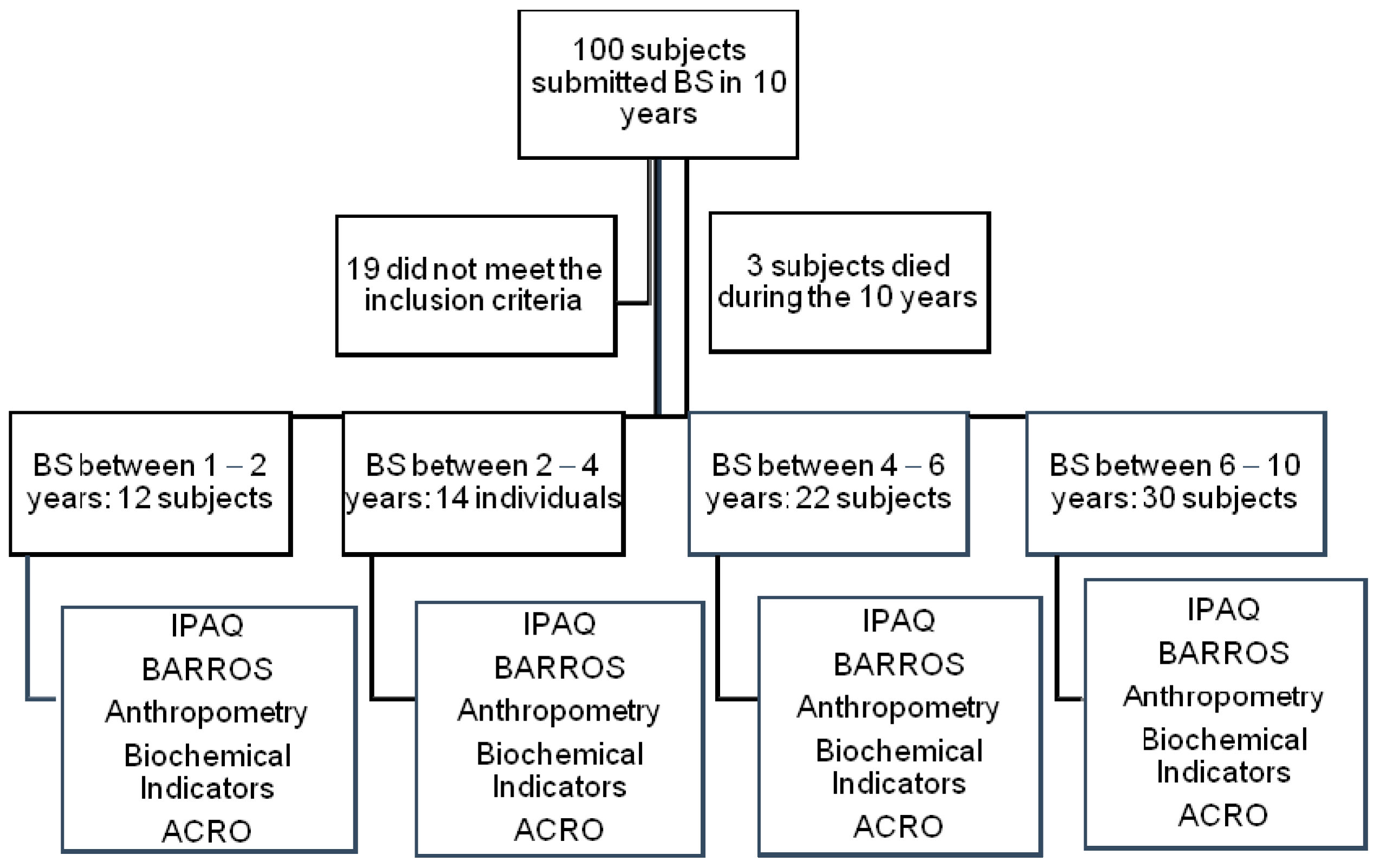
2.1. Sample
2.2. Data Collection (Anthropometric Data)
2.3. Biochemical Data
2.4. Evaluation of Comorbidities Associated with Obesity (ACRO)
2.5. Data on Quality of Life
2.6. International Physical Activity Questionnaire (IPAQ)
2.7. IPAQ Classification
2.8. Study
2.9. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Beamish, A.J.; Olbers, T.; Kelly, A.S.; Inge, T.H. Cardiovascular effects of bariatric surgery. Nat. Rev. Cardiol. 2016, 13, 730–743. [Google Scholar] [CrossRef] [PubMed]
- Schumann, R.; Shikora, S.A.; Sigl, J.C.; Kelley, S.D. Association of metabolic syndrome and surgical factors with pulmonary adverse events, and longitudinal mortality in bariatric surgery. Br. J. Anaesth. 2014, 114, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Brazil Vigitel Brasil. Surveillance of Risk Factors and Protection for Chronic Diseases by Telephone Inquiry: Estimates of Frequency and Sociodemographic Distribution of Risk Factors and Protection for Chronic Diseases in the Capitals of the 26 Brazilian States and in the Federal District in 2016; Ministry of Health: Brasília, Brazil, 2017.
- Buchwald, H.; Oien, D.M. Metabolic/bariatric surgery worldwide 2011. Obes. Surg. 2013, 23, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Colquitt, J.L.; Pickett, K.; Loveman, E.; Frampton, G.K. Surgery for Weight Loss in Adults; The Cochrane Library: Pitsburg, PA, USA, 2014. [Google Scholar]
- Barte, J.C.M.; Ter Bogt, N.C.W.; Bogers, R.P.; Teixeira, P.J.; Blissmer, B.; Bemelmans, W.J.E. Maintenance of weight loss after lifestyle interventions for overweight and obesity, a systematic review. Obes. Rev. 2010, 11, 899–906. [Google Scholar] [CrossRef] [PubMed]
- Gilbertson, N.M.; Paisley, A.S.; Kranz, S.; Kirby, J.L.; Hallowell, P.T.; Malin, S.K. Bariatric surgery resistance: Using preoperative lifestyle 42 medicine and/or pharmacology for metabolic responsiveness. Obes. Surg. 2017, 27, 3281–3291. [Google Scholar] [CrossRef] [PubMed]
- Welch, G.; Wesolowski, C.; Piepul, B.; Kuhn, J.; Romanelli, J.; Garb, J. Physical activity predicts weight loss following gastric bypass surgery: Findings from a support group survey. Obes. Surg. 2008, 18, 517–524. [Google Scholar] [CrossRef]
- Bond, D.S.; Phelan, S.; Wolfe, L.; Evans, R.K.; Kellum, J.M.; Wing, R.R. Becoming physically active after bariatric surgery is associated with improved weight loss and health-related quality of life. Obesity 2009, 17, 78–83. [Google Scholar] [CrossRef]
- Buchwald, H. The evolution of metabolic/bariatric surgery. Obes. Surg. 2014, 24, 1126–1135. [Google Scholar] [CrossRef]
- Bastos, E.C.L.; Barbosa, E.M.; Soriano, G.M.S.; Santos, E.A.D.; Vasconcelos, S.M.L. Determining factors of the ponderal regrowth in the postoperative period of bariatric surgery. Arq. Bras. Cir. Dig. 2013, 26, 26–32. [Google Scholar] [CrossRef]
- King, W.C.; Chen, J.Y.; Bond, D.S.; Belle, S.H.; Courcoulas, A.P.; Cook, B. Objective assessment of changes in physical activity and sedentary behavior: Pre-through 3 years post-bariatric surgery. Obesity 2015, 23, 1143–1150. [Google Scholar] [CrossRef]
- Herring, L.Y.; Stevinson, C.; Biddle, S.; Sutton, C.; Bowrey, D.; Carter, P. Changes in physical activity behaviour and physical function after bariatric surgery: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 250–261. [Google Scholar] [CrossRef] [PubMed]
- Jassil, F.C.; Manning, S.; Lewis, N.; Steinmo, S.; Kingett, H.; Doyle, J. Feasibility and impact of a combined supervised exercise and nutritional-behavioral intervention following bariatric surgery: A pilot study. J. Obes. 2015, 8, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Livhits, M.; Mercado, C.; Parikh, J.A.; Dutson, E.; Mehran, A.; Gibbons, M.M. Exercise following bariatric surgery: Systematic review. Obes. Surg. 2010, 20, 657–665. [Google Scholar] [CrossRef] [PubMed]
- Vatier, C.; Henegar, C.; Ciangura, C. Dynamic relations between sedentary behavior, physical activity, and body composition after bariatric surgery. Obes. Surg. 2012, 22, 1251–1256. [Google Scholar] [CrossRef]
- Aidar, F.J.; Silva, A.J.; Reis, V.M.; Carneiro, A.L.; Cotta, S.S. A study on the quality of life in ischaemic vascular accidents and its relation to physical activity. Rev. Neurol. 2007, 45, 518–522. [Google Scholar] [PubMed]
- Aidar, F.J.; Oliveira, R.J.; Silva, A.J.; Matos, D.G.; Carneiro, A.L.; Garrido, N.; Hickner, R.C.; Reis, V.M. Quality of life of stroke survivors according to the level of physical activity and the human development index. Health Qual. Life Outcomes 2011, 9, 89. [Google Scholar] [CrossRef] [PubMed]
- Vetter, M.L.; Faulconbridge, L.F.; Webb, V.L.; Wadden, T.A. Behavioral and pharmacologic therapies for obesity. Nat. Rev. Endocrinol. 2010, 6, 578–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busetto, L.; Mozzi, E.; Schettino, A.M.; Giardiello, C.; Micheletto, G.; Lap-Band, I.G. Three years durability of the improvements in health-related quality of life observed after gastric banding. Surg. Obes. Relat. Dis. 2015, 11, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Josbeno, D.A.; Kalarchian, M.; Sparto, P.J.; Otto, A.D.; Jakicic, J.M. Physical activity and physical function in individuals post-bariatric surgery. Obes. Surg. 2011, 21, 1243–1249. [Google Scholar] [CrossRef] [PubMed]
- Arcila, D.; Velázquez, D.; Gamino, R.; Salin-Pascual, R.; GonzálezBarranco, J.; Herrera, M.F. Quality of life in bariatric surgery. Obes. Surg. 2002, 12, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Overs, S.E.; Freeman, R.A.; Zarshenas, N.; Walton, K.L.; Jorgensen, J.O. Food tolerance and gastrointestinal quality of life following three bariatric procedures: Adjustable gastric banding, Roux-en-Y gastric bypass, and sleeve gastrectomy. Obes. Surg. 2012, 22, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Backman, O.; Stockeld, D.; Rasmussen, F.; Näslund, E.; Marsk, R. Alcohol and substance abuse, depression and suicide attempts after Roux-en-Y gastric bypass surgery. Br. J. Surg. 2016, 103, 1336–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peacock, J.C.; Sloan, S.S.; Cripps, B. A qualitative analysis of bariatric patients’ post-surgical barriers to exercise. Obes. Surg. 2014, 24, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Zabatiero, J.; Hill, K.; Gucciardi, D.F.; Taylor, S.F.; Hagger, M.S.; Smith, A. Beliefs, barriers and facilitators to physical activity in bariatric surgery candidates. Obes. Surg. 2016, 26, 1097–1109. [Google Scholar] [CrossRef] [PubMed]
- Creel, D.B.; Schuh, L.M.; Reed, C.A. A randomized trial comparing two interventions to increase physical activity among patients undergoing bariatric surgery. Obesity 2016, 24, 1660–1668. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D. Compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exer. 2011, 43, 1575–1581. [Google Scholar] [CrossRef]
- Gelinas, B.L.; Delparte, C.A.; Wright, K.D.; Hart, R. Problematic eating behaviors among bariatric surgical candidates: A psychometric investigation and factor analytic approach. Eat. Behav. 2015, 16, 34–39. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Obesity: Preventing and Managing the Global Epidemic: Report of a WHO Consultation; Technical Report Series 894; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Silva-Neto, E.F.; Vázquez, C.M.P.; Soares, F.M.; Silva, D.G.; Souza, M.F.C.; Barbosa, K.B.F. Bariatric surgery reverses metabolic risk in outpatient-assisted patients. Arq. Bras. Cir. Dig. 2014, 27, 38–42. [Google Scholar] [CrossRef]
- Ali, M.R.; Fuller, W.D.; Rasmussen, J. Detailed description of early response of metabolic syndrome after laparoscopic Roux-en-Y gastrc bypass. Surg. Obes. Relat. Dis. 2009, 5, 346–351. [Google Scholar] [CrossRef]
- Oria, H.E.; Moorehead, M.K. Bariatric Analysis and Reporting Outcome System (BAROS). Obes. Surg. 1998, 8, 487–499. [Google Scholar] [CrossRef]
- Hallal, P.C.; Victora, C.G. Reliability and validity of the International Physical Activity Questionnaire (IPAQ). Med. Sci. Sports Exerc. 2004, 36, 556. [Google Scholar] [CrossRef]
- Grissom, R.J.; Kim, J.J. Effect Sizes for Research: A Broad Practical Approach; Lawrence Erlbaum Associates Publishers: Pittsburgh, PA, USA, 2005. [Google Scholar]
- Buchwald, H.; Avidor, Y.; Braunwald, E. Bariatric surgery: A systematic review and meta-analysis. JAMA 2004, 292, 1724–1737. [Google Scholar] [CrossRef]
- Padwal, R.S.; Klarenbach, S.W.; Wang, X. A simple prediction rule for all-cause mortality in a cohort eligible for bariatric surgery. JAMA Surg. 2013, 148, 1109–1115. [Google Scholar] [CrossRef]
- Farinholt, G.N.; Carr, A.D.; Chang, E.J.; Ali, M.R. A call to arms: Obese men with more severe comorbid disease and underutilization of bariatric operations. Surg. Endosc. 2013, 27, 4556–4563. [Google Scholar] [CrossRef]
- Arterburn, D.E.; Courcoulas, A.P. Bariatric surgery for obesity and metabolic conditions in adults. BMJ 2014, 349, g3961. [Google Scholar] [CrossRef]
- Bergh, I.; Kvalem, I.L.; Risstad, H.; Cameron, L.D.; Sniehotta, F.F. Predictors of preoperative weight loss in morbidly obese adults waiting for bariatric surgery: A prospective cohort study. Obes. Surg. 2015, 25, 1610–1617. [Google Scholar] [CrossRef]
- Courcoulas, A.P.; Belle, S.H.; Neiberg, R.H. Three-year outcomes of bariatric surgery vs lifestyle intervention for type 2 diabetes mellitus treatment: A randomized clinical trial. JAMA Surg. 2015, 150, 931–940. [Google Scholar] [CrossRef]
- Still, C.D.; Wood, G.C.; Chu, X. Clinical factors associated with weight loss outcomes after Roux-en-Y gastric bypass surgery. Obesity 2014, 22, 888–894. [Google Scholar] [CrossRef]
- Chang, S.H.; Stoll, C.R.; Song, J.; Varela, J.E.; Eagon, C.J.; Colditz, G.A. The effectiveness and risks of bariatric surgery: An updated systematic review and meta-analysis, 2003–2012. JAMA Surg. 2014, 149, 275–287. [Google Scholar] [CrossRef]
- Hamdi, A.; Julien, C.; Brown, P.; Woods, I.; Hamdi, A.; Ortega, G.; Tran, D. Midterm outcomes of revisional surgery for gastric pouch and gastrojejunal anastomotic enlargement in patients with weight regain after gastric bypass for morbid obesity. Obes. Surg. 2014, 24, 1386–1390. [Google Scholar] [CrossRef]
- Dagan, S.S.; Keidar, A.; Raziel, A. Do bariatric patients follow dietary and lifestyle recommendations during the first postoperative year? Obes. Surg. 2017, 22, 1–14. [Google Scholar]
- Gumbs, A.A.; Pomp, A.; Gagner, M. Revisional bariatric surgery for inadequate weight loss. Obes. Surg. 2007, 17, 1137–1145. [Google Scholar] [CrossRef]
- Carneiro, I.B.P.; Sampaio, H.; Carioca, A.; Pinto, F.; Damasceno, N.R. Old and new anthropometric indicators as predictors of insulin resistance in adolescents. Arq. Bras. Endocrinol. Metab. 2014, 58, 838–843. [Google Scholar] [CrossRef]
- Lim, S.M.; Choi, D.P.; Rhee, Y.; Kim, H.C. Association between obesity indices and insulin resistance among healthy Korean adolescents: The JS high school study. PLoS ONE 2015, 10, e0125238. [Google Scholar] [CrossRef]
- Andersson, D.P.; Wahrenberg, H.; Toft, E. Waist circumference to assess reversal of insulin resistance following weight reduction after bariatric surgery: Cohort and cross-sectional studies. Intern. J. Obes. 2014, 38, 438. [Google Scholar] [CrossRef]
- Elbelt, U.; Schuetz, T.; Hoffmann, I.; Pirlich, M.; Strasburger, C.J.; Lochs, H. Differences of energy expenditure and physical activity patterns in subjects with various degrees of obesity. Clin. Nut. 2010, 29, 766–772. [Google Scholar] [CrossRef]
- Gota, C.E.; Kaouk, S.; Wilke, W.S. Fibromyalgia and obesity: The association between body mass index and disability, depression, history of abuse, medications, and comorbidities. J. Clin. Rheum. 2015, 21, 289–295. [Google Scholar] [CrossRef]
- King, W.C.; Chen, J.Y.; Belle, S.H. Change in pain and physical function following bariatric surgery for severe obesity. JAMA 2016, 315, 1362–1371. [Google Scholar] [CrossRef]
- Egberts, K.; Brown, W.A.; Brennan, L.; O’Brien, P.E. Does exercise improve weight loss after bariatric surgery? A systematic review. Obes. Surg. 2012, 22, 335–341. [Google Scholar] [CrossRef]
- Jacobi, D.; Ciangura, C.; Couet, C.; Oppert, J.M. Physical activity and weight loss following bariatric surgery. Obes. Rev. 2011, 12, 366–377. [Google Scholar] [CrossRef]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M. Obesity Society: 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. Circulation 2014, 129, S102–S138. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Blair, S.N.; Jakicic, J.M.; Manore, M.M.; Rankin, J.W.; Smith, B.K. American College of Sports Medicine Position Stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med. Sci. Sports Exerc. 2009, 41, 459–471. [Google Scholar] [CrossRef]
- King, W.C.; Hsu, J.Y.; Belle, S.H. Pre-to postoperative changes in physical activity: Report from the longitudinal assessment of bariatric surgery-2 (LABS-2). Surg. Obes. Relat. Dis. 2012, 8, 522–532. [Google Scholar] [CrossRef]
- Afshar, S.; Seymour, K.; Kelly, S.B.; Woodcock, S.; van Hees, V.T.; Mathers, J.C. Changes in physical activity after bariatric surgery: Using objective and self-reported measures. Surg. Obes. Relat. Dis. 2017, 13, 474–483. [Google Scholar] [CrossRef]
- Berglind, D.; Willmer, M.; Tynelius, P.; Ghaderi, A.; Näslund, E.; Rasmussen, F. Accelerometer-measured versus self-reported physical activity levels and sedentary behavior in women before and 9 months after Roux-en-Y gastric bypass. Obes. Surg. 2016, 26, 1463–1470. [Google Scholar] [CrossRef]
- Bobowicz, M.; Lehmann, A.; Orlowski, M.; Lech, P.; Michalik, M. Preliminary outcomes 1 year after laparoscopic sleeve gastrectomy based on Bariatric Analysis and Reporting Outcome System (BAROS). Obes. Surg. 2011, 21, 1843–1848. [Google Scholar] [CrossRef]
- Carswell, K.A.; Belgaumkar, A.P.; Amiel, S.A.; Patel, A.G. A systematic review and meta-analysis of the effect of gastric bypass surgery on plasma lipid levels. Obes. Surg. 2016, 26, 843–855. [Google Scholar] [CrossRef]
- Cunha, F.M.; Oliveira, J.; Preto, J.; Saavedra, A.; Costa, M.M.; Carvalho, D. The effect of bariatric surgery type on lipid profile: An age, sex, body mass index and excess weight loss matched study. Obes. Surg. 2016, 26, 1041–1047. [Google Scholar] [CrossRef]
- Heffron, S.P.; Parikh, A.; Volodarskiy, A. Changes in lipidprofile of obese patients following contemporary bariatric surgery: A meta-analysis. Am. J. Med. 2016, 129, 952–959. [Google Scholar] [CrossRef]
- Rêgo, A.D.S.; Zulin, A.; Scolari, S.; Marcon, S.S.; Radovanovic, C.A.T. Analysis of the clinical conditions of obese people in the pre and postoperative period of bariatric surgery. Rev. Col. Bras. Cir. 2017, 44, 171–178. [Google Scholar] [CrossRef]
- Gero, D.; Favre, L.; Allemann, P.; Fournier, P.; Demartines, N.; Suter, M. Laparoscopic Roux-En-Y gastric bypass improves lipid profile and decreases cardiovascular risk: A 5-year longitudinal cohort study of 1048 patients. Obes. Surg. 2017, 14, 1–7. [Google Scholar] [CrossRef]
- Schauer, P.R.; Bhatt, D.L.; Kirwan, J.P. Bariatric surgery versus intensive medical therapy for diabetes—5-year outcomes. N. Engl. J. Med. 2017, 376, 641–651. [Google Scholar] [CrossRef]
- Mingrone, G.; Panunzi, S.; De Gaetano, A. Bariatric–metabolic surgery versus conventional medical treatment in obese patients with type 2 diabetes: 5 year follow-up of an open-label, single-centre, randomized controlled trial. Lancet 2015, 386, 964–973. [Google Scholar] [CrossRef]
- Purnell, J.Q.; Selzer, F.; Wahed, A.S. Type 2 diabetes remission rates after laparoscopic gastric bypass and gastric banding: Results of the Longitudinal Assessment of Bariatric Surgery Study. Diabetes Care 2016, 39, 1101–1107. [Google Scholar] [CrossRef]
- Iaconelli, A.; Panunzi, S.; De Gaetano, A. Effects of bilio-pancreatic diversion on diabetic complications. Diabetes Care 2011, 34, 561–567. [Google Scholar] [CrossRef]
- Adams, T.D.; Davidson, L.E.; Litwin, S.E. Weight and metabolic outcomes 12 years after gastric bypass. N. Engl. J. Med. 2017, 377, 1143–1155. [Google Scholar] [CrossRef]
- Garcez, M.R.; Pereira, J.L.; de Mello, M.; Marchioni, D.M.L.; Fisberg, R.M. Prevalence of dyslipidemia according to nutritional status in a representative sample of São Paulo. Arq. Bras. Cardiol. 2014, 103, 476–484. [Google Scholar] [CrossRef]
- Crémieux, P.Y.; Ledoux, S.; Clerici, C.; Cremieux, F.; Buessing, M. The impact of bariatric surgery on comorbidities and medication use among obese patients. Obes. Surg. 2010, 20, 861–870. [Google Scholar] [CrossRef]
- Ghiassi, S.; Morton, J.; Bellatorre, N.; Eisenberg, D. Short-term medication cost savings for treating hypertension and diabetes after gastric bypass. Surg. Obes. Relat. Dis. 2012, 8, 269–274. [Google Scholar] [CrossRef]
- Pontiroli, A.E.; Ceriani, V.; Sarro, G.; Micheletto, G.; Folli, F. Incidence of diabetes mellitus, cardiovascular diseases, and cancer in patients undergoing malabsorptive surgery (biliopancreatic diversion and biliointestinal bypass) vs. medical treatment. Obes. Surg. 2019, 29, 935–942. [Google Scholar] [CrossRef]
- Azevedo, F.R.; Santoro, S.; Correa-Giannella, M.L.; Giannella-Neto, D.; Calderaro, D.; Caramelli, B. A prospective randomized controlled trial of the metabolic effects of sleeve gastrectomy with transit bipartition. Obes. Surg. 2018, 28, 3012–3019. [Google Scholar] [CrossRef]
- Zhao, X.; Duan, W.; Sun, C. Decreased cardiovascular risk after Roux-en-Y gastric bypass surgery in Chinese diabetic patients with obesity. J. Diab. Res. 2017, 4, 5–9. [Google Scholar] [CrossRef]
- Ricci, C.; Gaeta, M.; Rausa, E.; Asti, E.; Bandera, F.; Bonavina, L. Long-term effects of bariatric surgery on type II diabetes, hypertension and hyperlipidemia: A meta-analysis and meta-regression study with 5-year follow-up. Obes. Surg. 2015, 25, 397–405. [Google Scholar] [CrossRef]
- Lizcano, F.; Guzmán, G. Estrogen deficiency and the origin of obesity during menopause. BioMed Res. Int. 2014, 32, 321–328. [Google Scholar] [CrossRef]
- Vryonidou, A.; Paschou, S.A.; Muscogiuri, G.; Orio, F.; Goulis, D.G. Mechanisms in endocrinology: Metabolic syndrome through the female life cycle. Eur. J. Endoc. 2015, 173, R153–R163. [Google Scholar] [CrossRef]
- Savastano, S.; Di Somma, C.; Barrea, L.; Colao, A. The complex relationship between obesity and the somatropic axis: The long and winding road. Growth Horm. Igf Res. 2014, 24, 221–226. [Google Scholar] [CrossRef]
- Mancini, M.C.; Costa, A.P.; De Melo, M.E.; Cercato, C.; Giannella-Neto, D.; Halpern, A. Effect of gastric bypass on spontaneous growth hormone and ghrelin release profiles. Obesity 2006, 14, 383–387. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BS 2 Years | BS 4 Years | BS 6 Years | BS+6 Years | |
|---|---|---|---|---|
| Age | 45.0 ± 11.0 | 37.0 ± 6.6 | 40.0 ± 11.7 | 40.0 ± 9.0 |
| Age—♂ | 46.0 ± 4.0 | 36.0 ± 6.9 | 37.0 ± 12.8 | 39.0 ± 9.4 |
| Age—♀ | 45.0 ± 11.5 | 36.0 ± 5.6 | 40.0 ± 11.7 | 40.0 ± 9.0 |
| Gender ♂(%)/♀(%) | 2(16.7)/10(83.3) | 5(35.7)/9(64.3) | 3(13.6)/19(86.4) | 8(26.7)/22(73.3) |
| ACRO Score | Description |
|---|---|
| Diabetes Mellitus | |
| 0 | Absence |
| 1 | Glucose intolerance |
| 2 | Diabetes mellitus (diagnosed) |
| 3 | Controlled with oral antidiabetic |
| 4 | Insulin therapy |
| 5 | Clinical complications |
| Dyslipidemia | |
| 0 | Absence |
| 1 | Borderline (200–239 mg/dL) |
| 2 | Conventional control (diet + physical activity) |
| 3 | Single medicinal product |
| 4 | Multiple medication |
| 5 | Uncontrolled |
| Systemic arterial hypertension | |
| 0 | Absence |
| 1 | Borderline (systolic: 130–139 mmHg, diastolic: 85–89 mmHg) |
| 2 | Conventional control (diet + physical activity) |
| 3 | Single medicinal product |
| 4 | Multiple medication |
| 5 | Uncontrolled |
| BS2 n: 12 | BS4 n: 14 | BS6 n: 22 | BS+6 n:30 | p | f2 de Cohen | |
|---|---|---|---|---|---|---|
| Admission weight | 124.8 ± 24.6 a | 127.1 ± 21.0 a | 111.6 ± 21.8 a | 143.8 ± 29.3 a | ||
| Preoperative weight | 120.5 ± 21.7 a | 120.7 ± 15.6 a | 108.8 ± 22.4 | 134.3 ± 29.6 a | ||
| Postoperative weight | 111.8 ± 19.1 | 116.4 ± 14.0 | 101.6 ± 23.0 | 124.5 ± 28.4 a | ||
| Current weight | 83.5 ± 21.1 ab | 85.4 ± 10.1 ab | 77.3 ± 16.5 ab | 97.2 ± 25.1 | ||
| Minimum weight | 83.5 ± 21.2 ab | 83.8 ± 12.0 ab | 75.8 ± 17.2 ab | 94.1 ± 24.3 ab | 0.001 | 0.458 # |
| IPAQ Admission | 135.00 ± 27.47 | 134.67 ± 24.75 | 151.67 ± 25.66 | 109.67 ± 27.98 | ||
| IPAQ after 1 year | 207.50 ± 30.79 a | 210.67 ± 33.69 ab | 220.00 ± 42.78 ab | 197.67 ± 58.70 a | ||
| Current IPAQ | 189.17 ± 28.43 | 162.67 ± 29.63 | 193.33 ± 45.64 | 172.67 ± 53.24 | 0.001 | 0.438 # |
| BS2 | BS4 | BS6 | BS+6 | p | f2 de Cohen | |
|---|---|---|---|---|---|---|
| HDL Admission | 42.33 ± 7.74 | 43.80 ± 13.49 | 42.38 ± 14.48 | 41.40 ± 9.82 | ||
| HDL Release | 45.17 ± 9.61 | 42.09 ± 10.40 | 48.31 ± 14.57 | 43.13 ± 8.87 | ||
| HDL post BS | 40.67 ± 9.23 | 42.07 ± 12.33 | 42.05 ± 12.68 | 47.30 ± 12.86 | ||
| HDL Final | 47.92 ± 14.96 | 47.87 ± 9.45 | 49.19 ± 12.03 | 44.17 ± 12.13 | 0.098 | --- |
| LDL Admission | 120.32 ± 42.81 | 117.32 ± 39.52 | 14135 ± 41.23 a | 120.49 ± 25.02 | ||
| LDL Release | 110.58 ± 26.43 | 111.25 ± 38.70 | 124.17 ± 37.51 | 118.90 ± 30.75 | ||
| LDL post BS | 104.92 ± 28.19 | 117.47 ± 23.47 | 110.24 ± 29.11 | 109.37 ± 25.07 | ||
| LDL Final | 90.42 ± 17.31 ab | 93.40 ± 17.20 ab | 111.95 ± 29.99 | 85.71 ± 22.86 ab | 0.003 | 0.153 # |
| Cholesterol Admission | 189.25 ± 33.27 | 195.07 ± 40.57 | 227.00 ± 38.49 a | 187.90 ± 32.13 | ||
| Cholesterol Release | 178.92 ± 22.85 | 178.90 ± 31.53 | 197.60 ± 18.74 | 185.93 ± 34.19 | ||
| Cholesterol post BS | 153.92 ± 21.99 ab | 162.27 ± 38.45 | 171.71 ± 31.94 | 180.60 ± 35.45 | ||
| Cholesterol final | 155.50 ± 18.79 a | 156.47 ± 28.68 | 171.95 ± 35.04 | 146.50 ± 34.30 a | 0.001 | 0.234 # |
| Triglycerides Admission | 150.80 ± 33.94 | 164.40 ± 38.33 | 139.43 ± 20.09 | 152.35 ± 57.67 | ||
| triglycerides Release | 130.42 ± 25.67 | 132.86 ± 30.65 | 118.85 ± 18.07 | 141.97 ± 68.16 | ||
| triglycerides post BS | 92.33 ± 14.11 | 95.60 ± 31.45 | 99.52 ± 24.13 | 126.30 ± 41.03 | ||
| triglycerides Final | 87.42 ± 24.44 ab | 80.47 ± 12.51 ab | 79.86 ± 16.82 ab | 85.50 ± 31.99 ab | 0.001 | 0.196 # |
| Blood glucose Admission | 103.75 ± 32.52 | 101.84 ± 30.60 | 100.43 ± 20.46 | 106.40 ± 37.73 | ||
| Blood glucose Release | 111.17 ± 45.71 | 109.83 ± 27.31 | 89.50 ± 12.58 | 93.13 ± 17.62 | ||
| Blood glucose post BS | 92.58 ± 16.62 | 83.20 ± 7.85 | 86.10 ± 10.74 | 90.83 ± 25.60 | ||
| Blood glucose Final | 95.33 ± 21.27 | 82.73 ± 11.29 | 82.48 ± 8.48 | 79.57 ± 7.51 ab | 0.039 | 0.109 * |
| Diabetes Mellitus | n | At Admission | Release after BS | 12 Weeks | 24 Weeks | 52 Weeks |
| BS2 | 12 | 6 | 6 | 10 | 11 | 11 |
| BS4 | 14 | 12 | 11 | 13 | 13 | 13 |
| BS6 | 22 | 18 | 20 | 21 | 21 | 22 |
| BS+6 | 30 | 21 | 22 | 30 | 30 | 30 |
| Dyslipidemia | n | At admission | Release after BS | 12 weeks | 24 weeks | 52 weeks |
| BS 2 | 12 | 6 | 7 | 10 | 11 | 12 |
| BS 4 | 14 | 12 | 11 | 14 | 14 | 14 |
| BS 6 | 22 | 14 | 16 | 20 | 20 | 20 |
| BS +6 | 30 | 11 | 13 | 28 | 29 | 30 |
| Hypertension | n | At admission | Release after BS | 12 weeks | 24 weeks | 52 weeks |
| BS 2 | 12 | 1 | 1 | 7 | 7 | 8 |
| BS 4 | 14 | 9 | 4 | 10 | 12 | 13 |
| BS 6 | 22 | 9 | 11 | 17 | 18 | 18 |
| BS +6 | 30 | 7 | 7 | 26 | 26 | 26 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa Pereira, L.M.; Aidar, F.J.; de Matos, D.G.; de Farias Neto, J.P.; de Souza, R.F.; Sobral Sousa, A.C.; de Almeida, R.R.; Prado Nunes, M.A.; Nunes-Silva, A.; da Silva Júnior, W.M. Assessment of Cardiometabolic Risk Factors, Physical Activity Levels, and Quality of Life in Stratified Groups up to 10 Years after Bariatric Surgery. Int. J. Environ. Res. Public Health 2019, 16, 1975. https://doi.org/10.3390/ijerph16111975
Costa Pereira LM, Aidar FJ, de Matos DG, de Farias Neto JP, de Souza RF, Sobral Sousa AC, de Almeida RR, Prado Nunes MA, Nunes-Silva A, da Silva Júnior WM. Assessment of Cardiometabolic Risk Factors, Physical Activity Levels, and Quality of Life in Stratified Groups up to 10 Years after Bariatric Surgery. International Journal of Environmental Research and Public Health. 2019; 16(11):1975. https://doi.org/10.3390/ijerph16111975
Chicago/Turabian StyleCosta Pereira, Larissa Monteiro, Felipe J. Aidar, Dihogo Gama de Matos, Jader Pereira de Farias Neto, Raphael Fabrício de Souza, Antônio Carlos Sobral Sousa, Rebeca Rocha de Almeida, Marco Antonio Prado Nunes, Albená Nunes-Silva, and Walderi Monteiro da Silva Júnior. 2019. "Assessment of Cardiometabolic Risk Factors, Physical Activity Levels, and Quality of Life in Stratified Groups up to 10 Years after Bariatric Surgery" International Journal of Environmental Research and Public Health 16, no. 11: 1975. https://doi.org/10.3390/ijerph16111975
APA StyleCosta Pereira, L. M., Aidar, F. J., de Matos, D. G., de Farias Neto, J. P., de Souza, R. F., Sobral Sousa, A. C., de Almeida, R. R., Prado Nunes, M. A., Nunes-Silva, A., & da Silva Júnior, W. M. (2019). Assessment of Cardiometabolic Risk Factors, Physical Activity Levels, and Quality of Life in Stratified Groups up to 10 Years after Bariatric Surgery. International Journal of Environmental Research and Public Health, 16(11), 1975. https://doi.org/10.3390/ijerph16111975