Winter Exercise Reduces Allergic Airway Inflammation: A Randomized Controlled Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
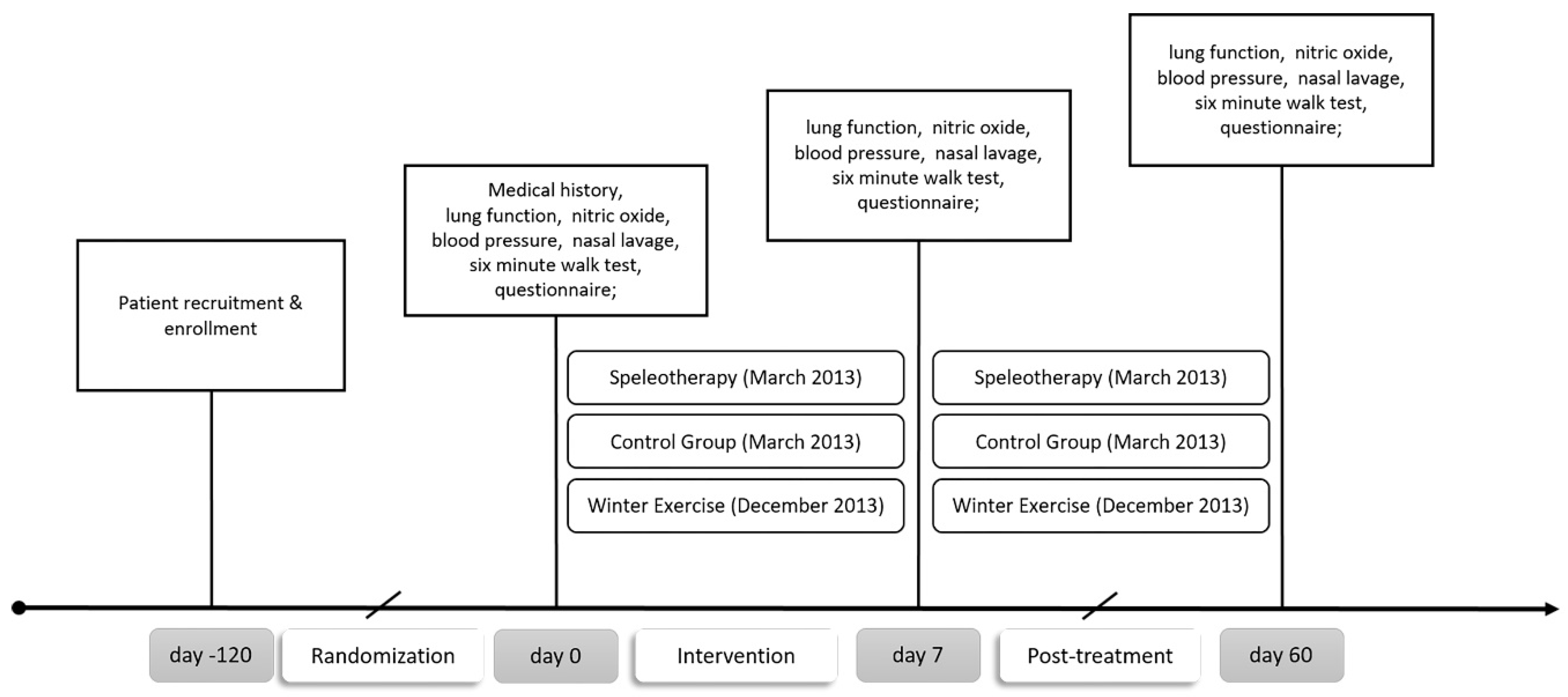
2.1. Study Design and Settings
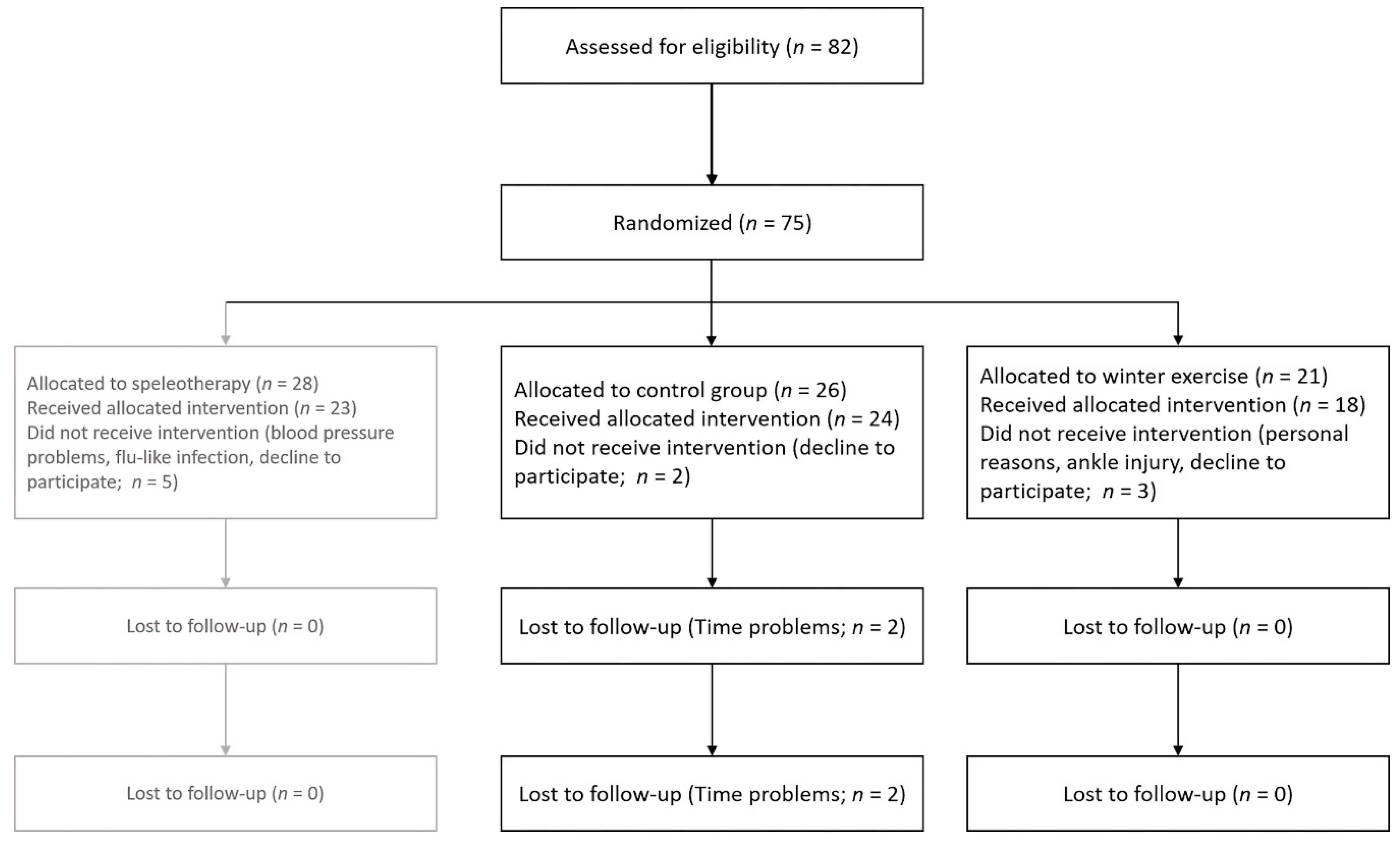
2.2. Participants
2.3. Intervention
2.4. Data Collection and Outcomes
2.4.1. Fractional Exhaled Nitric Oxide
2.4.2. Spirometry and Six-Minute Walk Test
2.4.3. Nasal Lavage and Saccharin Test
2.5. Randomization and Sample Size
2.6. Statistical Analysis
3. Results
3.1. Study Participants and Baseline Characteristics
3.2. Fractional Exhaled Nitric Oxide and Spirometry
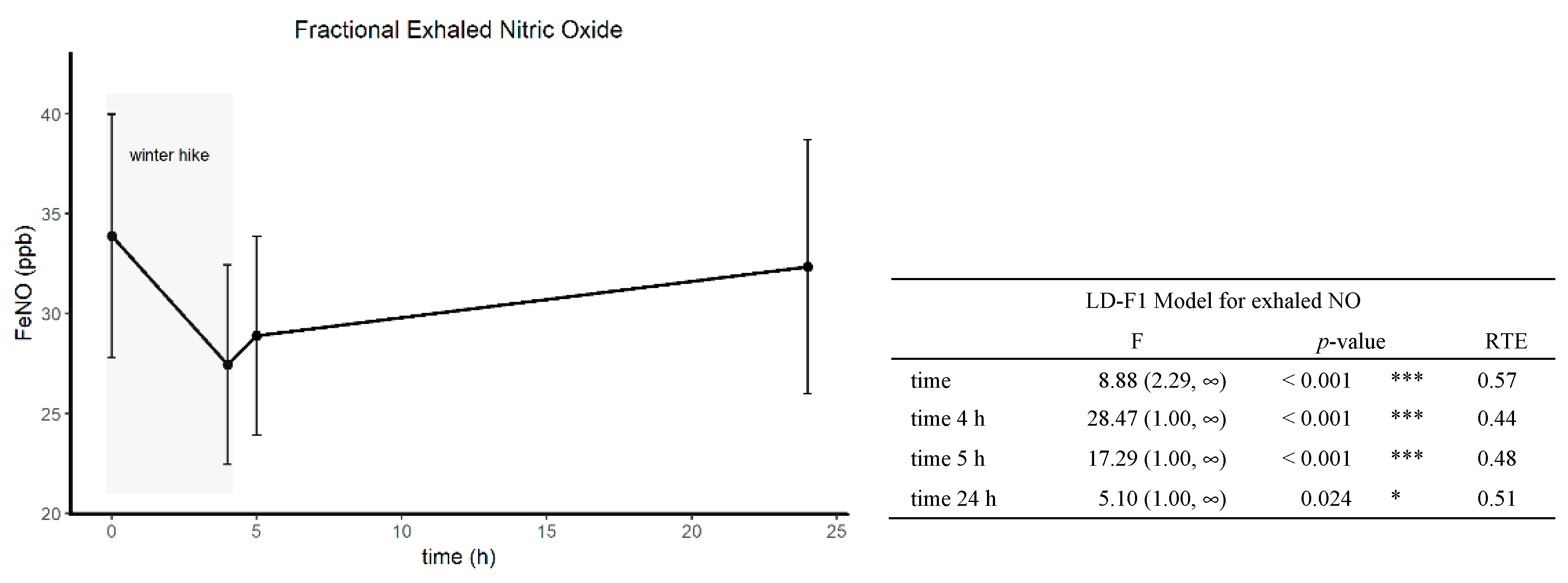
3.3. Short-Term Effects of Winter Hiking on FeNO
3.4. RhinAsthma Quality of Life Questionnaire (German adapted version)
3.5. Nasal Eosinophilic Count and Mucociliary Clearance Time
3.6. Differential Blood Count
3.7. Six-Minute Walk Test
3.8. Visual Analogue Scale
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
List of Abbreviations
| ACT | asthma control test |
| FeNO | fractional exhaled NO |
| FEV1 | forced expiratory volume in 1 second |
| FEV1/FVC | forced expiratory volume in 1 second of forced vital capacity |
| FVC | forced expiratory volume |
| IgE | immunoglobulin E |
| MEF25%–75% | mid-expiratory flow at 25%–75% of the FVC |
| NAL | nasal lavage |
| nparLD | nonparametric longitudinal data analysis |
| PEF | peak expiratory flow |
| RAST | radioallergosorbent test |
| RBC | red blood cell count |
| RTE | relative treatment effect |
| 6MWT | six-minute walk test |
References
- EAACI_Manifesto_brochure_Interactive.pdf. Available online: https://www.eaaci.org/images/media/EAACI_Manifesto_brochure_Interactive.pdf (accessed on 3 January 2019).
- Valovirta, E. EFA Book on Respiratory Allergies: Raise Awareness, Relieve the Burden. 2011. Available online: http://www.efanet.org (accessed on 3 January 2019).
- Guerra, S.; Sherrill, D.L.; Martinez, F.D.; Barbee, R.A. Rhinitis as an independent risk factor for adult-onset asthma. J. Allergy Clin. Immunol. 2002, 109, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Leynaert, B.; Neukirch, C.; Kony, S.; Guénégou, A.; Bousquet, J.; Aubier, M.; Neukirch, F. Association between asthma and rhinitis according to atopic sensitization in a population-based study. J. Allergy Clin. Immunol. 2004, 113, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Shaaban, R.; Zureik, M.; Soussan, D.; Neukirch, C.; Heinrich, J.; Sunyer, J.; Wjst, M.; Cerveri, I.; Pin, I.; Bousquet, J.; et al. Rhinitis and onset of asthma: A longitudinal population-based study. Lancet Lond. Engl. 2008, 372, 1049–1057. [Google Scholar] [CrossRef]
- Bousquet, J.; Van Cauwenberge, P.; Khaltaev, N. Aria Workshop Group; World Health Organization. Allergic rhinitis and its impact on asthma. J. Allergy Clin. Immunol. 2001, 108, 147–334. [Google Scholar] [CrossRef]
- Bousquet, J.; Khaltaev, N.; Cruz, A.A.; Denburg, J.; Fokkens, W.J.; Togias, A.; Zuberbier, T.; Baena-Cagnani, C.E.; Canonica, G.W.; van Weel, C.; et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy 2008, 86, 8–160. [Google Scholar] [CrossRef] [PubMed]
- Giavina-Bianchi, P.; Aun, M.V.; Takejima, P.; Kalil, J.; Agondi, R.C. United airway disease: Current perspectives. J. Asthma Allergy 2016, 9, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, E.O. Allergic Rhinitis: Burden of Illness, Quality of Life, Comorbidities, and Control. Immunol. Allergy Clin. North. Am. 2016, 36, 235–248. [Google Scholar] [CrossRef]
- Crystal-Peters, J.; Crown, W.H.; Goetzel, R.Z.; Schutt, D.C. The cost of productivity losses associated with allergic rhinitis. Am. J. Manag. Care 2000, 6, 373–378. [Google Scholar]
- Chawes, B.L.K. Low-grade disease activity in early life precedes childhood asthma and allergy. Dan Med. J. 2016, 63, 27. [Google Scholar]
- Schofield, M.L. Asthma pharmacotherapy. Otolaryngol. Clin. North. Am. 2014, 47, 55–64. [Google Scholar] [CrossRef]
- May, J.R.; Dolen, W.K. Management of Allergic Rhinitis: A Review for the Community Pharmacist. Clin. 2017, 39, 2410–2419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinnikov, D.; Khafagy, A.; Blanc, P.D.; Brimkulov, N.; Steinmaus, C. High-altitude alpine therapy and lung function in asthma: Systematic review and meta-analysis. ERJ Open Res. 2016, 2, 00097–02015. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, C.; Hense, G.; Rueckert, B.; Mantel, P.Y.; Ichters, B.; Blaser, K.; Menz, G.; Schmidt-Weber, C.B. High-altitude climate therapy reduces local airway inflammation and modulates lymphocyte activation. Scand. J. Immunol. 2006, 63, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Eichenberger, P.A.; Diener, S.N.; Kofmehl, R.; Spengler, C.M. Effects of Exercise Training on Airway Hyperreactivity in Asthma: A Systematic Review and Meta-Analysis. Sports Med. 2013, 43, 1157–1170. [Google Scholar] [CrossRef] [PubMed]
- Avallone, K.M.; McLeish, A.C. Asthma and aerobic exercise: A review of the empirical literature. J. Asthma Off J. Assoc. Care Asthma 2013, 50, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Laveneziana, P.; Lotti, P.; Coli, C.; Binazzi, B.; Chiti, L.; Stendardi, L.; Duranti, R.; Scano, G. Mechanisms of dyspnoea and its language in patients with asthma. Eur. Respir. J. 2006, 27, 742–747. [Google Scholar] [CrossRef]
- Thompson Coon, J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? A systematic review. Env. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef]
- Niedermeier, M.; Einwanger, J.; Hartl, A.; Kopp, M. Affective responses in mountain hiking-A randomized crossover trial focusing on differences between indoor and outdoor activity. PloS ONE 2017, 12, 0177719. [Google Scholar] [CrossRef]
- Carson, K.V.; Chandratilleke, M.G.; Picot, J.; Brinn, M.P.; Esterman, A.J.; Smith, B.J. Physical training for asthma. Cochrane Database Syst. Rev. 2013, 9, CD001116. [Google Scholar] [CrossRef]
- Klingberg, E.; Oleröd, G.; Konar, J.; Petzold, M.; Hammarsten, O. Seasonal variations in serum 25-hydroxy vitamin D levels in a Swedish cohort. Endocrine 2015, 49, 800–808. [Google Scholar] [CrossRef] [Green Version]
- Rabenberg, M.; Scheidt-Nave, C.; Busch, M.A.; Rieckmann, N.; Hintzpeter, B.; Mensink, G.B.M. Vitamin D status among adults in Germany—Results from the German Health Interview and Examination Survey for Adults (DEGS1). BMC Public Health 2015, 15, 641. [Google Scholar] [CrossRef] [PubMed]
- Bozzetto, S.; Carraro, S.; Giordano, G.; Boner, A.; Baraldi, E. Asthma, allergy and respiratory infections: The vitamin D hypothesis: Vitamin D role in allergic and respiratory diseases. Allergy 2012, 67, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Jolliffe, D.A.; Greenberg, L.; Hooper, R.L.; Griffiths, C.J.; Camargo, C.A.; Kerley, C.P.; Jensen, M.E.; Mauger, D.; Stelmach, I.; Urashima, M.; et al. Vitamin D supplementation to prevent asthma exacerbations: A systematic review and meta-analysis of individual participant data. Lancet Respir. Med. 2017, 5, 881–890. [Google Scholar] [CrossRef]
- Kohl, H.W.; Craig, C.L.; Lambert, E.V.; Inoue, S.; Alkandari, J.R.; Leetongin, G.; Kahlmeier, S. Lancet Physical Activity Series Working Group. The pandemic of physical inactivity: Global action for public health. Lancet Lond. Engl. 2012, 380, 294–305. [Google Scholar] [CrossRef]
- Matz, C.J.; Stieb, D.M.; Davis, K.; Egyed, M.; Rose, A.; Chou, B.; Brion, O. Effects of Age, Season, Gender and Urban-Rural Status on Time-Activity: Canadian Human Activity Pattern Survey 2 (CHAPS 2). Int. J. Env. Res. Public Health 2014, 11, 2108–2124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cariñanos, P.; Galán, C.; Alcázar, P.; Dominguez, E. Meteorological phenomena affecting the presence of solid particles suspended in the air during winter. Int. J. Biometeorol. 2000, 44, 6–10. [Google Scholar] [CrossRef] [PubMed]
- European Environment Agency. Air Quality in Europe—2018. EEA Report No 12/2018. Available online: https://www.eea.europa.eu/publications/air-quality-in-europe-2018 (accessed on 24 January 2019).
- Warburton, D.E.R.; Nicol, C.W.; Bredin, S.S.D. Health benefits of physical activity: The evidence. CMAJ Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Schauerte, G.; Oberhofer, E. Better control of asthma with winter sports. MMW Med. 2016, 158, 20–21. [Google Scholar]
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2018. Available online: https://ginasthma.org (accessed on 21 January 2019).
- Silva, D.; Moreira, A. The role of sports and exercise in allergic disease: Drawbacks and benefits. Expert Rev. Clin. Immunol. 2015, 11, 993–1003. [Google Scholar] [CrossRef]
- Nathan, R.A.; Sorkness, C.A.; Kosinski, M.; Schatz, M.; Li, J.T.; Marcus, P.; Murray, J.J.; Pendergraft, T.B. Development of the asthma control test: A survey for assessing asthma control. J. Allergy Clin. Immunol. 2004, 113, 59–65. [Google Scholar] [CrossRef]
- Mösges, R.; Schmalz, P.; Köberlein, J.; Kaciran, M.; Baiardini, I. The RHINASTHMA-Quality of Life Scale German Adapted Version: Validation of a new disease specific quality of life scale for patients suffering from allergic rhinitis and bronchial hyperreactivity. HNO 2007, 55, 357–364. [Google Scholar] [CrossRef] [PubMed]
- American Thoracic Society; European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide. Am. J. Respir Crit. Care Med. 2005, 171, 912–930. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ATS Statement. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [CrossRef] [PubMed]
- Chetta, A.; Zanini, A.; Pisi, G.; Aiello, M.; Tzani, P.; Neri, M.; Olivieri, D. Reference values for the 6-min walk test in healthy subjects 20–50 years old. Respir Med. 2006, 100, 1573–1578. [Google Scholar] [CrossRef]
- Andersen, I.; Camner, P.; Jensen, P.L.; Philipson, K.; Proctor, D.F. A comparison of nasal and tracheobronchial clearance. Arch. Env. Health 1974, 29, 290–293. [Google Scholar] [CrossRef]
- Kraus, D. Consolidated data analysis and presentation using an open-source add-in for the Microsoft Excel® spreadsheet software. Med. Writ. 2014, 23, 25–28. [Google Scholar] [CrossRef]
- Noguchi, K.; Gel, Y.R.; Brunner, E.; Konietschke, F. NparLD: An R software package for the nonparametric analysis of longitudinal data in factorial experiments. J. Stat. Softw 2012, 50. [Google Scholar] [CrossRef]
- Pakhale, S.; Luks, V.; Burkett, A.; Turner, L. Effect of physical training on airway inflammation in bronchial asthma: A systematic review. BMC Pulm. Med. 2013, 13, 38. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Mendes, F.A.R.; Almeida, F.M.; Cukier, A.; Stelmach, R.; Jacob-Filho, W.; Martins, M.A.; Carvalho, C.R.F. Effects of aerobic training on airway inflammation in asthmatic patients. Med. Sci. Sports Exerc. 2011, 43, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.J.; Cochrane, L.M. Assessment of work performance in asthma for determination of cardiorespiratory fitness and training capacity. Thorax 1988, 43, 745–749. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, M.; Moonie, S. Physical activity participation among adult Nevadans with self-reported asthma. J. Asthma Off J. Assoc. Care Asthma 2011, 48, 517–522. [Google Scholar] [CrossRef] [PubMed]
- An, R.; Zhang, S.; Ji, M.; Guan, C. Impact of ambient air pollution on physical activity among adults: A systematic review and meta-analysis. Perspect. Public Health 2018, 138, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Kranabetter, A.; Göbl, M.; Herzog, M. Messbericht Feinstaub im Winter 2013/2014. 2014. Available online: https://www.salzburg.gv.at/umweltnaturwasser_/Documents/Feinstaubmessprogramm-Winter2013-14.pdf (accessed on 21 January 2019).
- Dweik, R.A.; Boggs, P.B.; Erzurum, S.C.; Irvin, C.G.; Leigh, M.W.; Lundberg, J.O.; Olin, A.-C.; Plummer, A.L.; Taylor, D.R. An Official ATS Clinical Practice Guideline: Interpretation of Exhaled Nitric Oxide Levels (FeNO) for Clinical Applications. Am. J. Respir. Crit. Care Med. 2011, 184, 602–615. [Google Scholar] [CrossRef] [PubMed]
- Scott, H.A.; Latham, J.R.; Callister, R.; Pretto, J.J.; Baines, K.; Saltos, N.; Upham, J.W.; Wood, L.G. Acute exercise is associated with reduced exhaled nitric oxide in physically inactive adults with asthma. Ann. Allergy Asthma Immunol. Off. Pub. Am. Col. Allergy Asthma Immunol. 2015, 114, 470–479. [Google Scholar] [CrossRef] [PubMed]
- Luks, V.; Burkett, A.; Turner, L.; Pakhale, S. Effect of physical training on airway inflammation in animal models of asthma: A systematic review. BMC Pulm. Med. 2013, 13, 24. [Google Scholar] [CrossRef]
- Pacheco, D.R.R.; Silva, M.J.B.; Alexandrino, A.M.S.; Torres, R.M.T. Exercise-related quality of life in subjects with asthma: A systematic review. J. Asthma Off. J. Assoc. Care Asthma 2012, 49, 487–495. [Google Scholar] [CrossRef]
- Ochmann, U.; Kotschy-Lang, N.; Raab, W.; Kellberger, J.; Nowak, D.; Jörres, R.A. Is an Individual Prediction of Maximal Work Rate by 6-Minute Walk Distance and Further Measurements Reliable in Male Patients with Different Lung Diseases? Respiration 2013, 86, 384–392. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Exercise Group (n = 18) | Control Group (n = 22) | |||
|---|---|---|---|---|
| Mean ± SD | Median ± IQR | Mean ± SD | Median ± IQR | |
| Gender | male n = 5 | female n = 13 | male n = 7 | female n = 15 |
| Residence * | rural n = 5 | urban n = 13 | rural n = 9 | urban n = 13 |
| RAST/PRICK | 2 or + n = 8 | >3 or > ++ n = 10 | 2 or + n = 10 | >3 or > ++ n = 12 |
| Age (years) | 40.6 ± 12.1 | 45.0 ± 22.3 | 31.6 ± 10.7 | 25.5 ± 18.3 |
| Height (m) | 172.6 ± 6.7 | 172.0 ± 7.5 | 172.7 ± 8.1 | 171.5 ± 10.8 |
| Weight (kg) | 69.8 ± 9.8 | 69.0 ± 10.0 | 66.9 ± 9.3 | 67.5 ± 13.3 |
| Pulse (bpm) | 71.0 ± 12.6 | 70.4 ± 23.0 | 68.7 ± 8.8 | 67.0 ± 10.8 |
| BP-Systole (mmHg) | 125.3 ± 14.5 | 123.5 ± 14.5 | 118.5 ± 12.4 | 117.0 ± 20.0 |
| BP-Diastole (mmHg) | 76.4 ± 10.0 | 78.0 ± 15.0 | 73.0 ± 10.2 | 70.0 ± 17.8 |
| ACT (score) | 21.4 ± 3.6 | 22.5 ± 4.5 | 22.9 ± 3.2 | 24.0 ± 2.8 |
| FeNO (ppb) | 40.8 ± 23.0 | 38.0 ± 39.0 | 38.9 ± 22.3 | 36.0 ± 22.5 |
| FEV1 (%) | 96.3 ± 21.0 | 98.5 ± 21.3 | 103.7 ± 13.2 | 99.5 ± 18.5 |
| FVC (%) | 108.2 ± 17.7 | 108.0 ± 12.8 | 110.3 ± 16.1 | 109.0 ± 24.5 |
| FEV1/FVC (%) | 93.4 ± 11.8 | 95.0 ± 17.0 | 97.7 ± 8.2 | 99.5 ± 9.8 |
| 6MWT Distance (%) | 104.4 ± 8.2 | 106.0 ± 11.0 | 103.4 ± 10.5 | 102.6 ± 15.8 |
| Parameter | F1-LD-F1 Model | Relative Treatment Effects | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | p-value | Time | Interaction Effects | |||||||||
| Oral FeNO (ppb) | Treat | 1.15 (1.00, ∞) | 1.000 | n.s | Exercise | 0.42 | T0 | 0.54 | Exercise × T0 | 0.55 | Control × T0 | 0.52 |
| Time | 4.39 (1.63, ∞) | 0.055 | Control | 0.53 | T1 | 0.39 | Exercise × T1 | 0.29 | Control × T1 | 0.49 | ||
| Treat × Time | 3.17 (1.63, ∞) | 0.261 | n.s | T2 | 0.50 | Exercise × T2 | 0.41 | Control × T2 | 0.58 | |||
| Treat × T1 | 10.23 (1.0, ∞) | 0.008 | ** | |||||||||
| Nasal FeNO (ppb) | Treat | 0.37 (1.00, ∞) | 1.000 | n.s | Exercise | 0.46 | T0 | 0.52 | Exercise × T0 | 0.55 | Control × T0 | 0.48 |
| Time | 0.65 (1.83, ∞) | 0.509 | n.s | Control | 0.52 | T1 | 0.44 | Exercise × T1 | 0.40 | Control × T1 | 0.47 | |
| Treat × Time | 0.99 (1.83, ∞) | 0.733 | n.s | T2 | 0.51 | Exercise × T2 | 0.44 | Control × T2 | 0.59 | |||
| Nasal Eosinophil Count (%) | Treat | 0.08 (1.00, ∞) | 1.000 | n.s | Exercise | 0.51 | T0 | 0.50 | Exercise × T0 | 0.57 | Control × T0 | 0.42 |
| Time | 2.40 (1.98, ∞) | 0.183 | n.s | Control | 0.49 | T1 | 0.46 | Exercise × T1 | 0.45 | Control × T1 | 0.47 | |
| Treat × Time | 3.90 (1.98, ∞) | 0.021 | * | T2 | 0.55 | Exercise × T2 | 0.52 | Control × T2 | 0.58 | |||
| Mucociliary Clearance Time (min) | Treat | 0.50 (1.00, ∞) | 0.754 | n.s | Exercise | 0.47 | T0 | 0.52 | Exercise × T0 | 0.50 | Control × T0 | 0.55 |
| Time | 3.64 (1.8,1 ∞) | 0.061 | n.s | Control | 0.52 | T1 | 0.44 | Exercise × T1 | 0.38 | Control × T1 | 0.50 | |
| Treat × Time | 1.88 (1.81, ∞) | 0.470 | n.s | T2 | 0.53 | Exercise × T2 | 0.53 | Control × T2 | 0.52 | |||
| FVC (%) | Treat | 0.06 (1.00, ∞) | 1.000 | n.s | Exercise | 0.49 | T0 | 0.50 | Exercise × T0 | 0.47 | Control × T0 | 0.52 |
| Time | 0,65 (1.81, ∞) | 1.000 | n.s | Control | 0.51 | T1 | 0.49 | Exercise × T1 | 0.48 | Control × T1 | 0.51 | |
| Treat × Time | 1,92 (1.81, ∞) | 0.303 | n.s | T2 | 0.51 | Exercise × T2 | 0.51 | Control × T2 | 0.50 | |||
| FEV1 | Treat | 0.89 (1.00, ∞) | 0.689 | n.s | Exercise | 0.45 | T0 | 0.49 | Exercise × T0 | 0.44 | Control × T0 | 0.54 |
| Time | 1.58 (1.81, ∞) | 0.416 | n.s | Control | 0.54 | T1 | 0.51 | Exercise × T1 | 0.47 | Control × T1 | 0.55 | |
| Treat × Time | 0.49 (1.81, ∞) | 1.000 | n.s | T2 | 0.48 | Exercise × T2 | 0.45 | Control × T2 | 0.52 | |||
| FEV1/FVC (%) | Treat | 1.71 (1.00, ∞) | 0.585 | n.s | Exercise | 0.43 | T0 | 0.49 | Exercise × T0 | 0.43 | Control × T0 | 0.55 |
| Time | 4.10 (1.85, ∞) | 0.076 | Control | 0.55 | T1 | 0.52 | Exercise × T1 | 0.47 | Control × T1 | 0.56 | ||
| Treat × Time | 2.61 (1.85, ∞) | 0.313 | n.s | T2 | 0.47 | Exercise × T2 | 0.40 | Control × T2 | 0.55 | |||
| PEF (%) | Treat | 0.05 (1.00, ∞) | 1.000 | n.s | Exercise | 0.49 | T0 | 0.46 | Exercise × T0 | 0.48 | Control × T0 | 0.45 |
| Time | 2.70 (1.98, ∞) | 0.068 | Control | 0.51 | T1 | 0.52 | Exercise × T1 | 0.48 | Control × T1 | 0.56 | ||
| Treat × Time | 2.59 (1.88, ∞) | 0.302 | n.s | T2 | 0.51 | Exercise × T2 | 0.51 | Control × T2 | 0.52 | |||
| MEF 25%-75% | Treat | 1.94 (1.00, ∞) | 0.328 | n.s | Exercise | 0.43 | T0 | 0.49 | Exercise × T0 | 0.41 | Control × T0 | 0.56 |
| Time | 2.73 (1.76, ∞) | 0.145 | n.s | Control | 0.56 | T1 | 0.52 | Exercise × T1 | 0.47 | Control × T1 | 0.56 | |
| Treat × Time | 2.00 (1.76, ∞) | 0.284 | n.s | T2 | 0.48 | Exercise × T2 | 0.41 | Control × T2 | 0.55 | |||
| WBC (10³/µL) | Treat | 9.16 (1.00, ∞) | 0.005 | ** | Exercise | 0.62 | T0 | 0.52 | Exercise × T0 | 0.67 | Control × T0 | 0.36 |
| Time | 0.27 (1.98, ∞) | 0.758 | n.s | Control | 0.40 | T1 | 0.49 | Exercise × T1 | 0.52 | Control × T1 | 0.47 | |
| Treat × Time | 6.31 (1.98, ∞) | 0.002 | ** | T2 | 0.52 | Exercise × T2 | 0.66 | Control × T2 | 0.38 | |||
| RBC (106/µL) | Treat | 0.24 (1.00, ∞) | 0.622 | n.s | Exercise | 0.52 | T0 | 0.53 | Exercise × T0 | 0.54 | Control × T0 | 0.53 |
| Time | 1.35 (1.93, ∞) | 0.520 | n.s | Control | 0.48 | T1 | 0.49 | Exercise × T1 | 0.52 | Control × T1 | 0.45 | |
| Treat × Time | 0.40 (1.93, ∞) | 1.000 | n.s | T2 | 0.49 | Exercise × T2 | 0.51 | Control × T2 | 0.46 | |||
| Blood Neutrophil count (%) | Treat | 0.65 (1.00, ∞) | 0.419 | n.s | Exercise | 0.54 | T0 | 0.51 | Exercise × T0 | 0.59 | Control × T0 | 0.44 |
| Time | 0.16 (1.57, ∞) | 0.798 | n.s | Control | 0.47 | T1 | 0.50 | Exercise × T1 | 0.52 | Control × T1 | 0.48 | |
| Treat × Time | 2.25 (1.57, ∞) | 0.235 | n.s | T2 | 0.50 | Exercise × T2 | 0.51 | Control × T2 | 0.49 | |||
| Blood Eosinophil count (%) | Treat | 0.01 (1.00, ∞) | 0.907 | n.s | Exercise | 0.49 | T0 | 0.50 | Exercise × T0 | 0.51 | Control × T0 | 0.49 |
| Time | 0.18 (1.62, ∞) | 0.787 | n.s | Control | 0.50 | T1 | 0.49 | Exercise × T1 | 0.50 | Control × T1 | 0.48 | |
| Treat × Time | 1.21 (1.62, ∞) | 0.292 | n.s | T2 | 0.51 | Exercise × T2 | 0.48 | Control × T2 | 0.54 | |||
| Parameter | F1-LD-F1 Model | Relative Treatment Effects | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | p-value | Time | Interaction Effects | |||||||||
| RhinAsthma Questionnaire Total Score | Treat | 0.45 (1.00, ∞) | 1.000 | n.s | Exercise | 0.47 | T0 | 0.56 | Exercise × T0 | 0.55 | Control × T0 | 0.57 |
| Time | 4.71 (1.80, ∞) | 0.034 | * | Control | 0.52 | T1 | 0.45 | Exercise × T1 | 0.45 | Control × T1 | 0.45 | |
| Treat × Time | 2.47 (1.80, ∞) | 0.505 | n.s | T2 | 0.48 | Exercise × T2 | 0.41 | Control × T2 | 0.56 | |||
| RhinAsthma Questionnaire Limitation in Daily Life | Treat | 0.12 (1.00, ∞) | 1.000 | n.s | Exercise | 0.48 | T0 | 0.55 | Exercise × T0 | 0.55 | Control × T0 | 0.56 |
| Time | 3.36 (1.80, ∞) | 0.079 | Control | 0.51 | T1 | 0.46 | Exercise × T1 | 0.47 | Control × T1 | 0.45 | ||
| Treat × Time | 1.20 (1.80, ∞) | 0.960 | n.s | T2 | 0.48 | Exercise × T2 | 0.44 | Control × T2 | 0.53 | |||
| RhinAsthma Questionnaire Respiratory Problems | Treat | 0.38 (1.00, ∞) | 1.000 | n.s | Exercise | 0.53 | T0 | 0.55 | Exercise × T0 | 0.60 | Control × T0 | 0.51 |
| Time | 2.80 (1.82, ∞) | 0.070 | Control | 0.48 | T1 | 0.46 | Exercise × T1 | 0.49 | Control × T1 | 0.42 | ||
| Treat × Time | 0.73 (1.82, ∞) | 0.587 | n.s | T2 | 0.50 | Exercise × T2 | 0.49 | Control × T2 | 0.50 | |||
| RhinAsthma Questionnaire Rhinoconjunctivitis Score | Treat | 1.81 (1.00, ∞) | 0.717 | n.s | Exercise | 0.45 | T0 | 0.52 | Exercise × T0 | 0.54 | Control × T0 | 0.50 |
| Time | 1.95 (1.83, ∞) | 0.251 | n.s | Control | 0.54 | T1 | 0.45 | Exercise × T1 | 0.37 | Control × T1 | 0.52 | |
| Treat × Time | 4.11 (1.83, ∞) | 0.058 | T2 | 0.52 | Exercise × T2 | 0.42 | Control × T2 | 0.61 | ||||
| RhinAsthma Questionnaire Treatment and Medication Problems | Treat | 0.05 (1.00, ∞) | 1.000 | n.s | Exercise | 0.49 | T0 | 0.55 | Exercise × T0 | 0.56 | Control × T0 | 0.54 |
| Time | 4.01 (1.89, ∞) | 0.044 | n.s | Control | 0.51 | T1 | 0.46 | Exercise × T1 | 0.48 | Control × T1 | 0.44 | |
| Treat × Time | 3.80 (1.89, ∞) | 0.098 | n.s | T2 | 0.49 | Exercise × T2 | 0.43 | Control × T2 | 0.55 | |||
| RhinAsthma Questionnaire Impairment in Sensory Perceptions | Treat | 0.08 (1.00, ∞) | 1.000 | n.s. | Exercise | 0.49 | T0 | 0.55 | Exercise × T0 | 0.52 | Control × T0 | 0.58 |
| Time | 2.98 (1.93, ∞) | 0.105 | n.s. | Control | 0.51 | T1 | 0.47 | Exercise × T1 | 0.50 | Control × T1 | 0.43 | |
| Treat × Time | 2.47 (1.93, ∞) | 0.347 | n.s. | T2 | 0.48 | Exercise × T2 | 0.44 | Control × T2 | 0.52 | |||
| Visual Analogue Scale General Health | Treat | 0.95 (1.00, ∞) | 0.661 | n.s. | Exercise | 0.46 | T0 | 0.44 | Exercise × T0 | 0.32 | Control × T0 | 0.56 |
| Time | 2.51 (1.90, ∞) | 0.169 | n.s. | Control | 0.53 | T1 | 0.54 | Exercise × T1 | 0.55 | Control × T1 | 0.53 | |
| Treat × Time | 5.60 (1.90, ∞) | 0.009 | * | T2 | 0.51 | Exercise × T2 | 0.51 | Control × T2 | 0.50 | |||
| Visual Analogue Scale Allergic Symptoms | Treat | 0.42 (1.00, ∞) | 1.000 | n.s | Exercise | 0.53 | T0 | 0.46 | Exercise × T0 | 0.38 | Control × T0 | 0.46 |
| Time | 7.50 (1.98, ∞) | 0.002 | ** | Control | 0.48 | T1 | 0.59 | Exercise × T1 | 0.65 | Control × T1 | 0.59 | |
| Treat × Time | 10.32 (1.98, ∞) | <0.001 | *** | T2 | 0.46 | Exercise × T2 | 0.56 | Control × T2 | 0.46 | |||
| Treat × T1 | 10.55 (1.00, ∞) | 0.005 | ** | |||||||||
| Treat × T2 | 21.25 (1.00, ∞) | <0.001 | *** | |||||||||
| Parameter | F1-LD-F1 Model | Relative Treatment Effects | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | p-Value | Time | Interaction Effects | |||||||||
| Six-Minute Walk Distance (m) | Treat | 0.34 (1.00, ∞) | 1.000 | n.s. | Exercise | 0.47 | T0 | 0.44 | Exercise × T0 | 0.43 | Control × T0 | 0.43 |
| Time | 5.61 (1.84, ∞) | 0.009 | ** | Control | 0.52 | T1 | 0.54 | Exercise × T1 | 0.58 | Control × T1 | 0.58 | |
| Treat × Time | 1.18 (1.84, ∞) | 1.000 | n.s. | T2 | 0.52 | Exercise × T2 | 0.55 | Control × T2 | 0.55 | |||
| Peak Respiratory Frequency (1/min) | Treat | 0.17 (1.00, ∞) | 1.000 | n.s. | Exercise | 0.52 | T0 | 0.45 | Exercise × T0 | 0.55 | Control × T0 | 0.34 |
| Time | 2.45 (1.86, ∞) | 0.091 | Control | 0.49 | T1 | 0.54 | Exercise × T1 | 0.51 | Control × T1 | 0.58 | ||
| Treat × Time | 5.85 (1.86, ∞) | 0.015 | * | T2 | 0.51 | Exercise × T2 | 0.49 | Control × T2 | 0.54 | |||
| Peak Minute Ventilation (L/min) | Treat | 0.04 (1.00, ∞) | 1.000 | n.s. | Exercise | 0.50 | T0 | 0.45 | Exercise × T0 | 0.47 | Control × T0 | 0.43 |
| Time | 6.07 (1.68, ∞) | 0.012 | * | Control | 0.50 | T1 | 0.54 | Exercise × T1 | 0.53 | Control × T1 | 0.55 | |
| Treat × Time | 0.67 (1.68, ∞) | 1.000 | n.s. | T2 | 0.51 | Exercise × T2 | 0.51 | Control × T2 | 0.51 | |||
| BORG Scale Dyspnea Post-Test | Treat | 0.15 (1.00, ∞) | 1.000 | n.s. | Exercise | 0.52 | T0 | 0.55 | Exercise × T0 | 0.59 | Control × T0 | 0.50 |
| Time | 4.71 (1.83, ∞) | 0.056 | Control | 0.49 | T1 | 0.52 | Exercise × T1 | 0.51 | Control × T1 | 0.53 | ||
| Treat × Time | 1.13 (1.83, ∞) | 0.839 | n.s. | T2 | 0.44 | Exercise × T2 | 0.45 | Control × T2 | 0.43 | |||
| BORG Scale Fatigue Post-Test | Treat | 0.78 (1.00, ∞) | 0.577 | n.s. | Exercise | 0.54 | T0 | 0.52 | Exercise × T0 | 0.61 | Control × T0 | 0.44 |
| Time | 1.42 (1.76, ∞) | 1.000 | n.s. | Control | 0.47 | T1 | 0.52 | Exercise × T1 | 0.54 | Control × T1 | 0.51 | |
| Treat × Time | 2.64 (1.76, ∞) | 0.234 | n.s. | T2 | 0.44 | Exercise × T2 | 0.46 | Control × T2 | 0.47 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prossegger, J.; Huber, D.; Grafetstätter, C.; Pichler, C.; Braunschmid, H.; Weisböck-Erdheim, R.; Hartl, A. Winter Exercise Reduces Allergic Airway Inflammation: A Randomized Controlled Study. Int. J. Environ. Res. Public Health 2019, 16, 2040. https://doi.org/10.3390/ijerph16112040
Prossegger J, Huber D, Grafetstätter C, Pichler C, Braunschmid H, Weisböck-Erdheim R, Hartl A. Winter Exercise Reduces Allergic Airway Inflammation: A Randomized Controlled Study. International Journal of Environmental Research and Public Health. 2019; 16(11):2040. https://doi.org/10.3390/ijerph16112040
Chicago/Turabian StyleProssegger, Johanna, Daniela Huber, Carina Grafetstätter, Christina Pichler, Herbert Braunschmid, Renate Weisböck-Erdheim, and Arnulf Hartl. 2019. "Winter Exercise Reduces Allergic Airway Inflammation: A Randomized Controlled Study" International Journal of Environmental Research and Public Health 16, no. 11: 2040. https://doi.org/10.3390/ijerph16112040
APA StyleProssegger, J., Huber, D., Grafetstätter, C., Pichler, C., Braunschmid, H., Weisböck-Erdheim, R., & Hartl, A. (2019). Winter Exercise Reduces Allergic Airway Inflammation: A Randomized Controlled Study. International Journal of Environmental Research and Public Health, 16(11), 2040. https://doi.org/10.3390/ijerph16112040