Laryngopharyngeal Reflux Diagnosis in Obstructive Sleep Apnea Patients Using the Pepsin Salivary Test


 ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects of the Study
2.2. Clinical and Endoscopic Investigation of LPR
2.3. Salivary Specimen Collection and Salivary Pepsin Concentration Estimation (PEP-Test)
2.4. Statistical Analysis
3. Results
3.1. LPR Prevalence in OSA Patients
3.2. LPR and Age
3.3. LPR and AHI
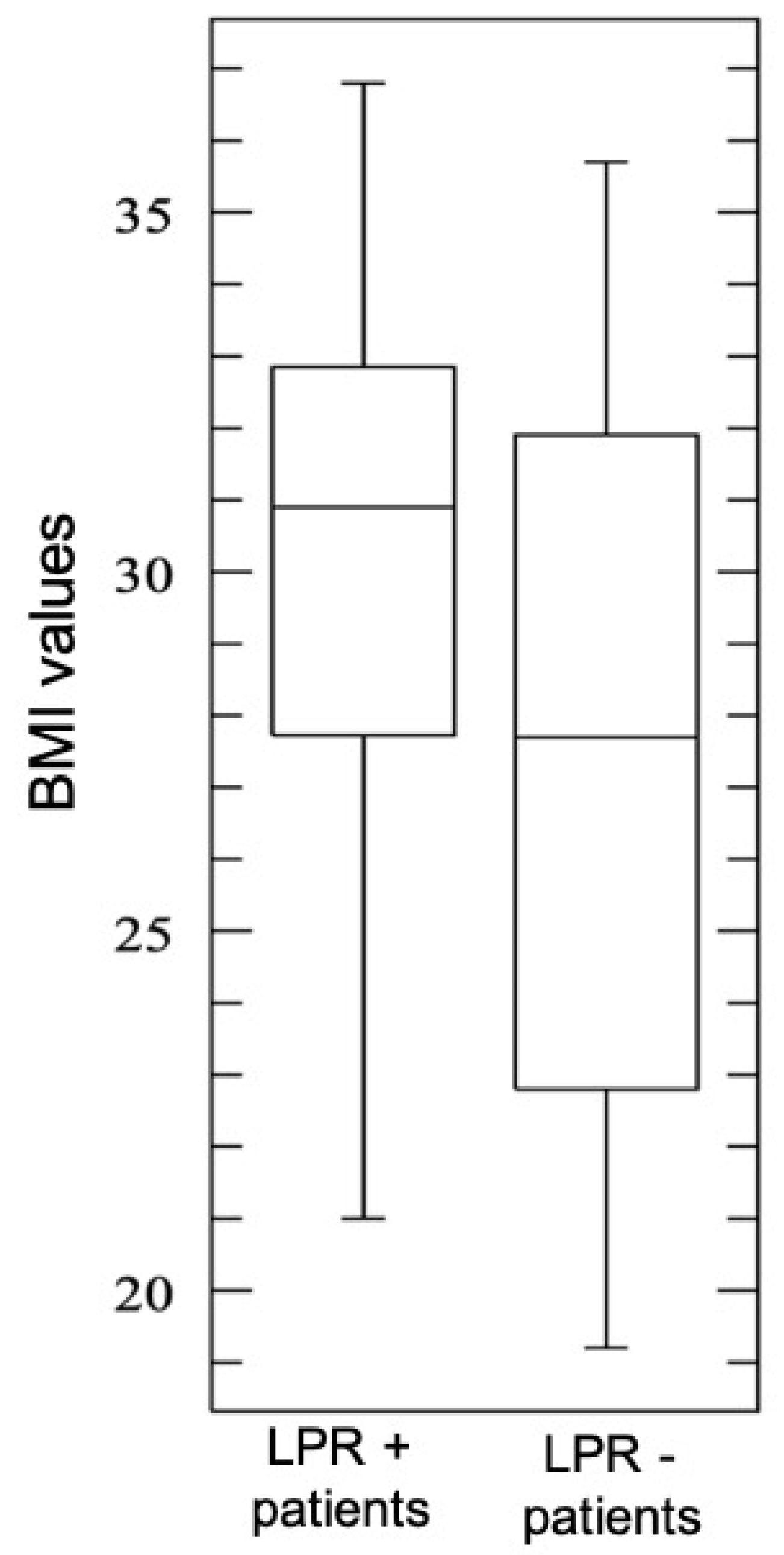
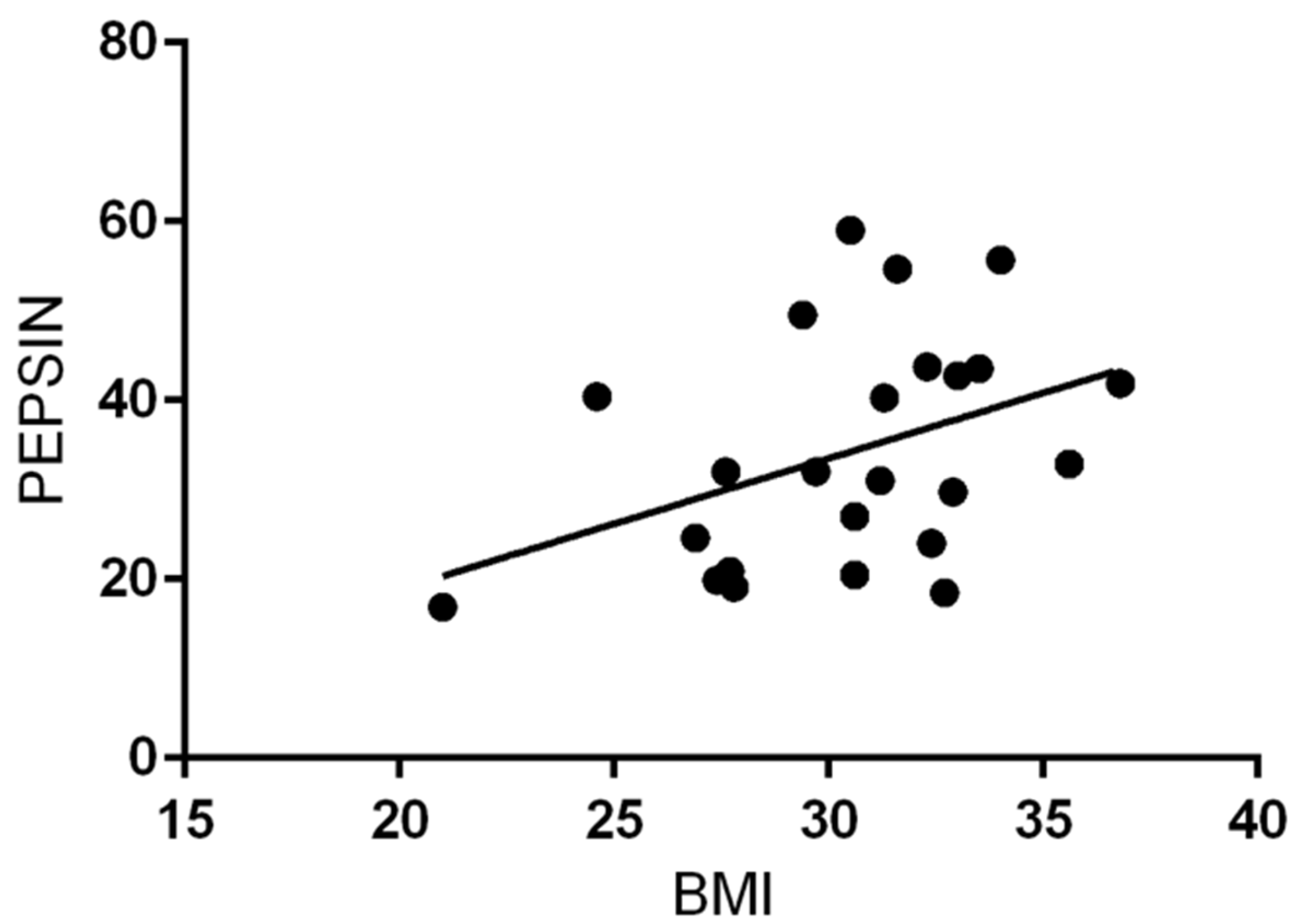
3.4. LPR and BMI
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Young, T.; Palta, M.; Dempsey, J.; Skatrud, J.; Weber, S.; Badr, S. The occurrence of sleep-disordered breathing among middle-aged adults. N. Engl. J. Med. 1993, 328, 1230–1235. [Google Scholar] [CrossRef] [PubMed]
- Cruz, A.A. Global Surveillance, Prevention and Control of Chronic Respiratory Diseases: A Comprehensive Approach; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Magliulo, G.; de Vincentiis, M.; Iannella, G.; Ciofalo, A.; Manno, A.; Pasquariello, B. Eustachian tube evaluation in patients with obstructive sleep apnea syndrome. Acta Otolaryngol. 2018, 138, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Eastwood, P.R.; Malhotra, A.; Palmer, L.J.; Kezirian, E.J.; Horner, R.L.; Ip, M.S.; Thurnheer, R.; Antic, N.A.; Hillman, D.R. Obstructive Sleep Apnoea: From pathogenesis to treatment: Current controversies and future directions. Respirology 2010, 15, 587–595. [Google Scholar] [CrossRef] [PubMed]
- White, D.P. Pathogenesis of obstructive and central sleep apnea. Am. J. Respir. Crit. Care Med. 2005, 172, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Vicini, C.; De Vito, A.; Iannella, G.; Gobbi, R.; Corso, R.M.; Montevecchi, F.; Polimeni, A.; De Vincentiis, M.; Meccariello, G.; D’Agostino, G.; et al. The aging effect on upper airways collapse of patients with obstructive sleep apnea syndrome. Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 2983–2990. [Google Scholar] [CrossRef] [PubMed]
- Caparroz, F.A.; Campanholo, M.D.A.T.; Regina, C.G.; Park, S.W.; Haddad, L.; Gregório, L.C.; Haddad, F.L.M. Clinical and polysomnographic predictors of laryngopharyngeal reflux in obstructive sleep apnea syndrome. Braz. J. Otorhinolaryngol. 2018, 18, 1808–1809. [Google Scholar] [CrossRef]
- Lee, J.S.; Heo, S.J.; Kim, J.S.; Ahn, D.; Sohn, J.H.; Kim, H. Relationship between the severity of laryngopharyngeal reflux and sleep apnea: Using drug-induced sleep endoscopy (DISE). Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 219–224. [Google Scholar] [CrossRef]
- Kim, S.J.; Kim, H.Y.; Jeong, J.I.; Hong, S.D.; Chung, S.-K.; Dhong, H.-J. Changes in the Reflux Symptom Index After Multilevel Surgery for Obstructive Sleep Apnea. Clin. Exp. Otorhinolaryngol. 2017, 10, 259–264. [Google Scholar] [CrossRef]
- Altintaş, A.; Soylu, A.; Yegin, Y.; Çelik, M.; Kaya, K.H. Impact of Laryngopharyngeal Reflux on the Levels of Depression and Anxiety in Patients With Obstructive Sleep Apnea Syndrome. J. Craniofacial Surg. 2017, 28, 121–124. [Google Scholar] [CrossRef]
- Elhennawi, D.M.; Ahmed, M.R.; Abou-Halawa, A.S. Correlation of obstructive sleep apnoea and laryngopharyngeal reflux: Phmetry study. Clin. Otolaryngol. 2016, 41, 758–761. [Google Scholar] [CrossRef] [PubMed]
- Qu, Y.; Ye, J.-Y.; Han, D.-M.; Zheng, L.; Cao, X.; Zhang, Y.-H.; Ding, X. Esophageal Functional Changes in Obstructive Sleep Apnea/Hypopnea Syndrome and Their Impact on Laryngopharyngeal Reflux Disease. Chin. Med. J. (Engl.) 2015, 128, 2162–2167. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.M.; Dibbern, R.S.; Santos, V.J.B.; Passeri, L.A. Influence of obesity on the correlation between laryngopharyngeal reflux and obstructive sleep apnea. Braz. J. Otorhinolaryngol. 2014, 80, 5–10. [Google Scholar] [CrossRef]
- Xavier, S.D.; Moraes, J.P.; Eckley, C.A. Prevalence of signs and symptoms of laryngopharyngeal reflux in snorers with suspected obstructive sleep apnea. Braz. J. Otorhinolaryngol. 2013, 79, 589–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eryılmaz, A.; Erişen, L.; Demir, U.L.; Kasapoglu, F.; Ozmen, O.A.; Ursavaş, A.; Kıyıcı, M.; Hızalan, I.; Eryilmaz, A.; Kiyici, M. Management of patients with coexisting obstructive sleep apnea and laryngopharyngeal reflux disease. Eur. Arch. Otorhinolaryngol. 2012, 269, 2575–2780. [Google Scholar] [CrossRef] [PubMed]
- Magliulo, G.; Iannella, G.; Polimeni, A.; De Vincentiis, M.; Meccariello, G.; Gulotta, G.; Pasquariello, B.; Montevecchi, F.; De Vito, A.; D’Agostino, G.; et al. Laryngopharyngeal reflux in obstructive sleep apnoea patients: Literature review and meta-analysis. Am. J. Otolaryngol. 2018, 39, 776–780. [Google Scholar] [CrossRef]
- Belafsky, P.C.; Postma, G.N.; Koufman, J.A. The validity and reliability of the reflux finding score (RFS). Laryngoscope 2001, 111, 1313–1317. [Google Scholar] [CrossRef]
- Belafsky, P.C.; Postma, G.N.; Koufman, J.A. Validity and reliability of the reflux symptom index (RSI). J. Voice 2002, 16, 274–277. [Google Scholar] [CrossRef]
- Kawamura, O.; Aslam, M.; Rittmann, T.; Hofmann, C.; Shaker, R. Physical and pH properties of gastroesophagopharyngeal refluxate: A 24-hour simultaneous ambulatory impedance and pH monitoring study. Am. J. Gastroenterol. 2004, 99, 1000–1010. [Google Scholar] [CrossRef]
- Srinivasan, R.; Vela, M.F.; Katz, P.O.; Tutuian, R.; Castell, J.A.; Castell, D.O. Esophageal function testing using multichannel intraluminal impedance. Am. J. Physiol. Gastrointest. Liver Physiol. 2001, 280, G457–G462. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Akst, L.M.; Hamdan, A.L.; Schindler, A.; Karkos, P.D.; Barillari, M.R.; Calvo-Henriquez, C.; Crevier-Buchman, L.; Finck, C.; Eun, Y.-G.; et al. Evaluation and Management of Laryngopharyngeal Reflux Disease: State of the Art Review. Otolaryngol. Head Neck Surg. 2019, 160, 762–782. [Google Scholar] [CrossRef] [PubMed]
- Iannella, G.; Di Nardo, G.; Plateroti, R.; Rossi, P.; Plateroti, A.M.; Mariani, P.; Magliulo, G. Investigation of pepsin in tears of children with laryngopharyngeal reflux disease. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 2312–2315. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Saussez, S.; Karkos, P.D. Laryngopharyngeal reflux disease: Clinical presentation, diagnosis and therapeutic challenges in 2018. Curr. Opin. Otolaryngol. Head Neck Surg. 2018, 26, 392–402. [Google Scholar] [CrossRef]
- Wang, L.; Liu, X.; Liu, Y.L. Correlation of pepsin-measured laryngopharyngeal reflux disease with symptoms and signs. Otolaryngol. Head Neck Surg. 2010, 143, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Samuels, T.L.; Johnston, N. Pepsin as a marker of extraesophageal reflux. Ann. Otol. Rhinol. Laryngol. 2010, 119, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Knight, J.; Lively, M.O.; Johnston, N.; Dettmar, P.W.; Koufman, J.A. Sensitive pepsin immunoassay for detection of laryngopharyngeal reflux. Laryngoscope 2005, 115, 1473–1478. [Google Scholar] [CrossRef] [PubMed]
- Jiang, A.; Liang, M.; Su, Z.; Chai, L.; Lei, W.; Wang, Z.; Wen, W.; Chen, M. Immunohistochemical detection of pepsin in laryngeal mucosa for diagnosing laryngopharyngeal reflux. Laryngoscope 2011, 121, 1426–1430. [Google Scholar] [CrossRef]
- Sereg-Bahar, M.; Jerin, A.; Jansa, R.; Stabuc, B.; Hocevar-Boltezar, I. Pepsin and bile acids in saliva in patients with laryngopharyngeal reflux-a prospective comparative study. Clin. Otolaryngol. 2015, 40, 234–239. [Google Scholar] [CrossRef]
- Barona-Lleo, L.; Barona-De Guzman, R.; Krstulovic, C. The Diagnostic Usefullness of the Salivary Pepsin Test in Symptomatic Laryngopharyngeal Reflux. J. Voice 2018. [Epub ahead of print]. [Google Scholar] [CrossRef]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [PubMed]
- Epstein, L.J.; Kristo, D.; Strollo, P.J., Jr.; Friedman, N.; Malhotra, A.; Patil, S.P.; Ramar, K.; Rogers, R.; Schwab, R.J.; Weaver, E.M.; et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J. Clin. Sleep Med. 2009, 5, 263–276. [Google Scholar] [PubMed]
- Li, J.; Zhang, L.; Zhang, C.; Cheng, J.Y.; Li, J.; Cheng, C.-F.J. Linguistic Adaptation, Reliability, Validation, and Responsivity of the Chinese Version of Reflux Symptom Index. J. Voice 2016, 30, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Huet, K.; Finck, C.; Khalife, M.; Fourneau, A.F.; Delvaux, V.; Piccaluga, M.; Harmegnies, B.; Saussez, S. Validity and Reliability of a French Version of Reflux Symptom Index. J. Voice 2017, 31, 512. [Google Scholar] [CrossRef] [PubMed]
- Eskiizmir, G.; Kezirian, E. Is there a vicious cycle between obstructive sleep apnea and laryngopharyngeal reflux disease? Med. Hypotheses 2009, 73, 706–708. [Google Scholar] [CrossRef]
- Chen, M.; Hou, C.; Chen, T.; Lin, Z.; Wang, X.; Zeng, Y. Reflux symptom index and reflux finding score in 91 asymptomatic volunteers. Acta Otolaryngol. 2018, 138, 659–663. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LPR+ Patients (n = 24) Average Value | LPR− Patients (n = 51) Average Value | p-Value (T-Student Test) | |
|---|---|---|---|
| Age | 51.5 (range 23–75) | 50.2 (range 19–66) | 0.7 |
| AHI (average value) | 27.1 (range 10.3–54.6) | 23.4 (range 8.5–47.1) | 0.2 |
| BMI (average value) | 30.4 (range 19.9–36.8) | 27.7 (range 33.8–18.5) | 0.02 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iannella, G.; Vicini, C.; Polimeni, A.; Greco, A.; Gobbi, R.; Montevecchi, F.; De Vito, A.; Meccariello, G.; Cammaroto, G.; D’Agostino, G.; et al. Laryngopharyngeal Reflux Diagnosis in Obstructive Sleep Apnea Patients Using the Pepsin Salivary Test. Int. J. Environ. Res. Public Health 2019, 16, 2056. https://doi.org/10.3390/ijerph16112056
Iannella G, Vicini C, Polimeni A, Greco A, Gobbi R, Montevecchi F, De Vito A, Meccariello G, Cammaroto G, D’Agostino G, et al. Laryngopharyngeal Reflux Diagnosis in Obstructive Sleep Apnea Patients Using the Pepsin Salivary Test. International Journal of Environmental Research and Public Health. 2019; 16(11):2056. https://doi.org/10.3390/ijerph16112056
Chicago/Turabian StyleIannella, Giannicola, Claudio Vicini, Antonella Polimeni, Antonio Greco, Riccardo Gobbi, Filippo Montevecchi, Andrea De Vito, Giuseppe Meccariello, Giovanni Cammaroto, Giovanni D’Agostino, and et al. 2019. "Laryngopharyngeal Reflux Diagnosis in Obstructive Sleep Apnea Patients Using the Pepsin Salivary Test" International Journal of Environmental Research and Public Health 16, no. 11: 2056. https://doi.org/10.3390/ijerph16112056
APA StyleIannella, G., Vicini, C., Polimeni, A., Greco, A., Gobbi, R., Montevecchi, F., De Vito, A., Meccariello, G., Cammaroto, G., D’Agostino, G., Pace, A., Cascella, R., Brunori, M., Lo Iacono, C. A. M., Pelucchi, S., & Magliulo, G. (2019). Laryngopharyngeal Reflux Diagnosis in Obstructive Sleep Apnea Patients Using the Pepsin Salivary Test. International Journal of Environmental Research and Public Health, 16(11), 2056. https://doi.org/10.3390/ijerph16112056