Screening of the Maturity Status of the Tibial Tuberosity by Ultrasonography in Higher Elementary School Grade Schoolchildren



Abstract
:1. Introduction
2. Hypothesis
3. Materials and Methods
3.1. Study Type
3.2. Subjects
3.3. Musculoskeletal Examination
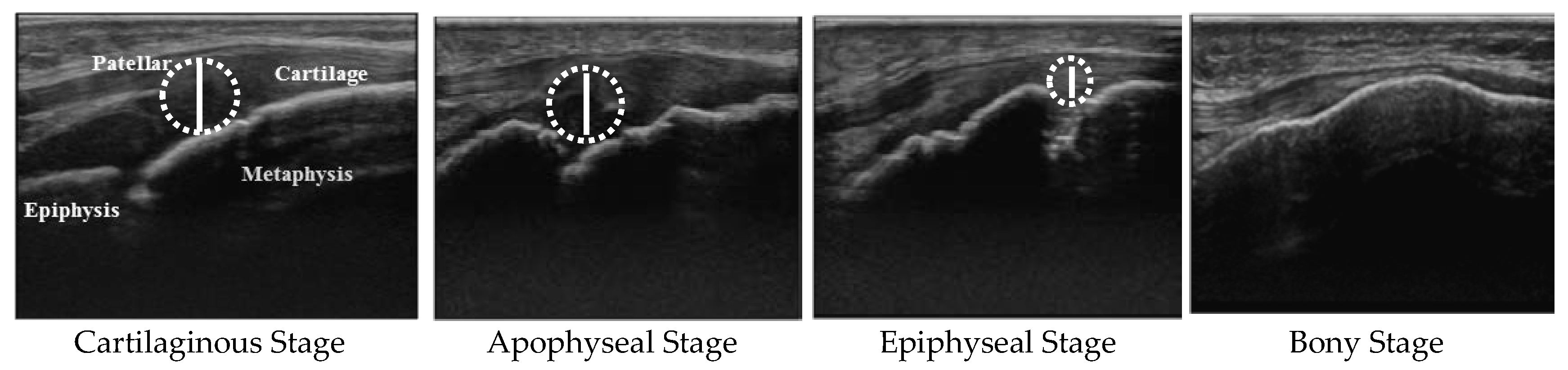
3.4. Determination of Maturity Stages and Cartilage Thickness of the Tibial Tuberosity
3.5. Longitudinal Survey
3.6. Statistics
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Auringer, S.T.; Anthony, E.Y. Common pediatric sports injuries. Semin. Musculoskelet Radiol. 1999, 3, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Junge, T.; Runge, L.; Juul-Kristensen, B.; Wedderkopp, N. Risk factors for knee injuries in children 8 to 15 years, the CHAMPS Study DK. Med. Sci. Sports Exerc. 2016, 48, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Nowinski, R.J.; Mehlman, C.T. Hyphenated history, Osgood-Schlatter disease. Am. J. Orthop. (Belle Mead NJ). 1998, 27, 584–585. [Google Scholar] [PubMed]
- Gholve, P.A.; Scher, D.M.; Khakharia, S.; Widmann, R.F.; Green, D.W. Osgood Schlatter syndrome. Curr. Opin. Pediatr. 2007, 19, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Vaishya, R.; Azizi, A.T.; Agarwal, A.K.; Vijay, V. Apophysitis of the tibial tuberosity (Osgood-Schlatter disease), A review. Cureus 2016, 8, e780. [Google Scholar] [CrossRef]
- Kujala, U.M.; Kvist, M.; Heinonen, O. Osgood-Schlatter’s disease in adolescent athletes. Retrospective study of incidence and duration. Am. J. Sports Med. 1985, 13, 236–241. [Google Scholar] [CrossRef] [PubMed]
- de Lucena, G.L.; dos Santos Gomes, C.; Guerra, R.O. Prevalence and associated factors of Osgood-Schlatter syndrome in a population-based sample of Brazilian adolescents. Am. J. Sports Med. 2011, 39, 415–420. [Google Scholar] [CrossRef]
- Ross, M.D.; Villard, D. Disability levels of college-aged men with a history of Osgood-Schlatter disease. J. Strength Cond. Res. 2003, 17, 659–663. [Google Scholar]
- Ogden, J.A.; Hempton, R.J.; Southwick, W.O. Development of the tibial tuberosity. Anat. Rec. 1975, 182, 431–445. [Google Scholar] [CrossRef]
- Ogden, J.A.; Southwick, W.O. Osgood-Schlatter’s disease and tibial tuberosity development. Clin. Orthop. Relat. Res. 1976, 116, 180–189. [Google Scholar]
- Ehrenborg, G.; Lagergren, C. Roentgenologic changes in the Osgood-Schlatter lesion. Acta. Chir. Scand. 1961, 121, 315–327. [Google Scholar] [PubMed]
- Ducher, G.; Cook, J.; Lammers, G.; Coombs, P.; Ptazsnik, R.; Black, J.; Bass, S.L. The ultrasound appearance of the patellar tendon attachment to the tibia in young athletes is conditional on gender and pubertal stage. J. Sci. Med. Sport 2010, 13, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Ducher, G.; Cook, J.; Spurrier, D.; Coombs, P.; Ptasznik, R.; Black, J.; Bass, S. Ultrasound imaging of the patellar tendon attachment to the tibia during puberty, a 12-month follow-up in tennis players. Scand. J. Med. Sci. Sports 2010, 20, e35–e40. [Google Scholar] [CrossRef] [PubMed]
- Sailly, M.; Whiteley, R.; Johnson, A. Doppler ultrasound and tibial tuberosity maturation status predicts pain in adolescent male athletes with Osgood-Schlatter’s disease, a case series with comparison group and clinical interpretation. Br. J. Sports Med. 2013, 47, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Nakase, J.; Goshima, K.; Numata, H.; Oshima, T.; Takata, Y.; Tsuchiya, H. Precise risk factors for Osgood-Schlatter disease. Arch. Orthop. Trauma Surg. 2015, 135, 1277–1281. [Google Scholar] [CrossRef] [PubMed]
- Kaneuchi, Y.; Otoshi, K.; Hakozaki, M.; Sekiguchi, M.; Watanabe, K.; Igari, T.; Konno, S. Bony Maturity of the tibial tuberosity with regard to age and sex and its relationship to pathogenesis of Osgood-Schlatter disease, an Ultrasonographic study. Orthop. J. Sports Med. 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- Yanagisawa, S.; Osawa, T.; Saito, K.; Kobayashi, T.; Tajika, T.; Yamamoto, A.; Iizuka, H.; Takagishi, K. Assessment of Osgood-Schlatter disease and the skeletal maturation of the distal attachment of the patellar tendon in preadolescent males. Orthop. J. Sports Med. 2014, 2. [Google Scholar] [CrossRef]
- de Flaviis, L.; Nessi, R.; Scaglione, P.; Balconi, G.; Albisetti, W.; Derchi, L.E. Ultrasonic diagnosis of Osgood-Schlatter and Sinding-Larsen-Johansson diseases of the knee. Skeletal Radiol. 1989, 18, 193–197. [Google Scholar] [CrossRef]
- Lanning, P.; Heikkinen, E. Ultrasonic features of the Osgood-Schlatter lesion. J. Pediatr. Orthop. 1991, 11, 538–540. [Google Scholar] [CrossRef]
- Blankstein, A.; Cohen, I.; Heim, M.; Diamant, L.; Salai, M.; Chechick, A.; Ganel, A. Ultrasonography as a diagnostic modality in Osgood-Schlatter disease. A clinical study and review of the literature. Arch. Orthop. Trauma Surg. 2001, 121, 536–539. [Google Scholar] [CrossRef]
- Vreju, F.; Ciurea, P.; Rosu, A. Osgood-Schlatter disease—Ultrasonographic diagnostic. Med. Ultrason. 2010, 12, 336–339. [Google Scholar] [PubMed]
- Czyrny, Z. Osgood-Schlatter disease in ultrasound diagnostics—A pictorial essay. Med. Ultrason. 2010, 12, 323–335. [Google Scholar] [PubMed]
- Kaya, D.O.; Toprak, U.; Baltaci, G.; Yosmaoglu, B.; Ozer, H. Long-term functional and sonographic outcomes in Osgood-Schlatter disease. Knee Surg. Sports Traumatol Arthrosc. 2013, 21, 1131–1139. [Google Scholar] [CrossRef]
- Yamaguchi, N.; Chosa, E.; Yamamoto, K.; Kawahara, K.; Hamada, H.; Taniguchi, N.; Tajima, T.; Funamoto, T.; Kurogi, S.; Ota, T.; et al. Screening for musculoskeletal problems in Japanese schoolchildren, a cross-sectional study nested in a cohort. Public Health 2016, 139, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Bloom, R.A.; Gomori, J.; Milgrom, C. Ossicles anterior to the proximal tibia. Clin. Imaging 1993, 17, 137–141. [Google Scholar] [CrossRef]
- Börjesson, A.E.; Lagerquist, M.K.; Windahl, S.H.; Ohlsson, C. The role of estrogen receptor α in the regulation of bone and growth plate cartilage. Cell. Mol. Life Sci. 2013, 70, 4023–4037. [Google Scholar] [CrossRef] [PubMed]
- Schicht, M.; Ernst, J.; Nielitz, A.; Fester, L.; Tsokos, M.; Guddat, S.S.; Bräuer, L.; Bechmann, J.; Delank, K.S.; Wohlrab, D.; et al. Articular cartilage chondrocytes express aromatase and use enzymes involved in estrogen metabolism. Arthritis Res. Ther. 2014, 16, R93. [Google Scholar] [CrossRef] [PubMed]
- Flowers, M.J.; Bhadreshwar, D.R. Tibial tuberosity excision for symptomatic Osgood-Schlatter disease. J. Pediatr. Orthop. 1995, 15, 292–297. [Google Scholar] [CrossRef]
- Yousefzadeh, D.K.; Doerger, K.; Sullivan, C. The blood supply of early, late, and nonossifying cartilage, preliminary gray-scale and Doppler assessment and their implications. Pediatr. Radiol. 2008, 38, 146–158. [Google Scholar] [CrossRef]
- Benjamin, M.; Rufai, A.; Ralphs, J.R. The mechanism of formation of bony spurs (enthesophytes) in the achilles tendon. Arthritis Rheum. 2000, 43, 576–583. [Google Scholar] [CrossRef]
- Achar, S.; Yamanaka, J. Apophysitis and osteochondrosis: Common causes of pain in growing bones. Am. Fam. Physician 2019, 99, 610–618. [Google Scholar] [PubMed]
- Hirano, A.; Fukubayashi, T.; Ishii, T.; Ochiai, N. Magnetic resonance imaging of Osgood-Schlatter disease, the course of the disease. Skeletal Radiol. 2002, 31, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Frank, J.B.; Jarit, G.J.; Bravman, J.T.; Rosen, J.E. Lower extremity injuries in the skeletally immature athlete. J. Am. Acad. Orthop. Surg. 2007, 15, 356–366. [Google Scholar] [CrossRef] [PubMed]
- Cairns, G.; Owen, T.; Kluzek, S.; Thurley, N.; Holden, S.; Rathleff, M.S.; Dean, B.J.F. Therapeutic interventions in children and adolescents with patellar tendon related pain: A systematic review. BMJ Open Sport Exerc. Med. 2018, 4, e000383. [Google Scholar] [CrossRef] [PubMed]


 , Apophyseal stage
, Apophyseal stage  , Epiphyseal stage
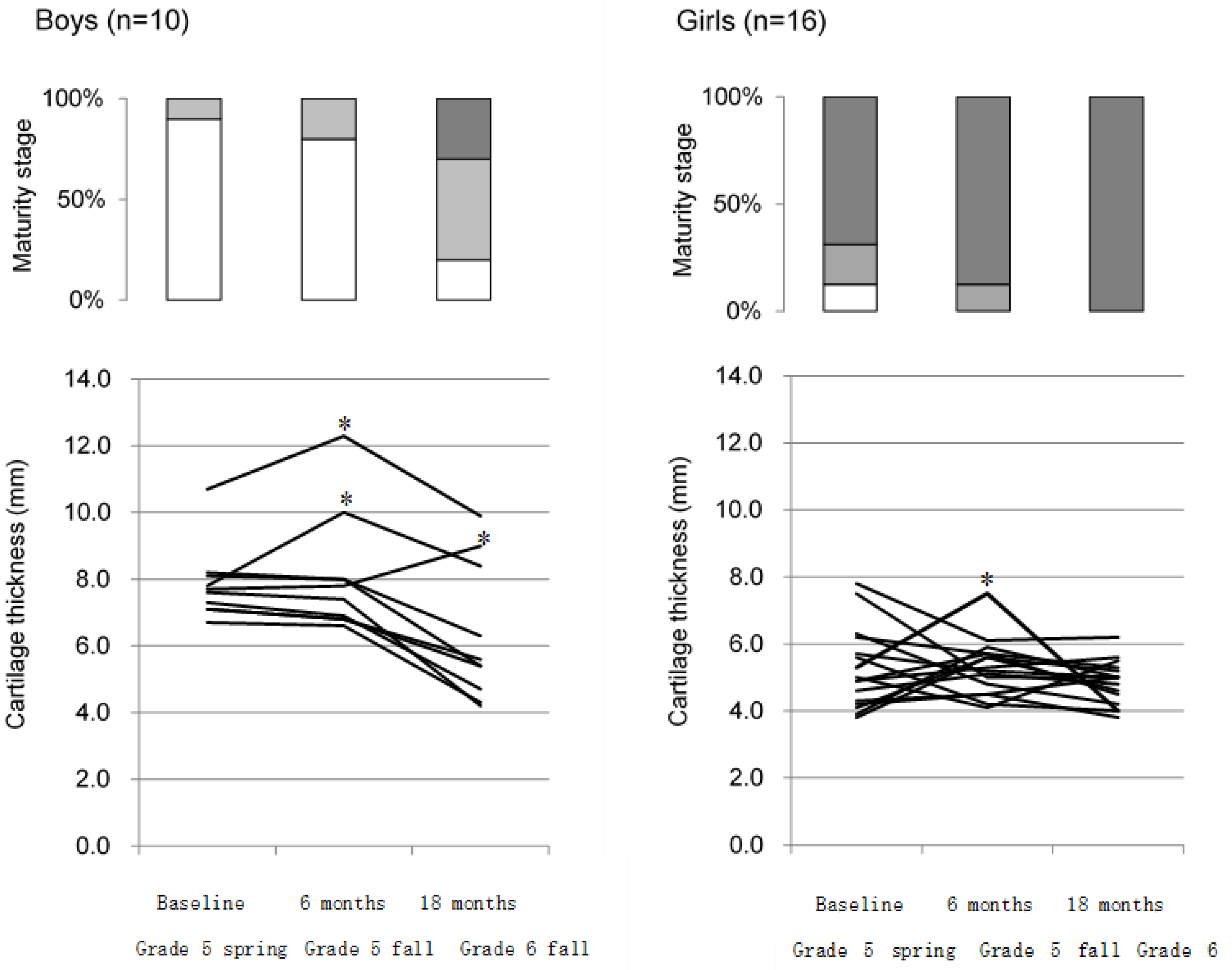
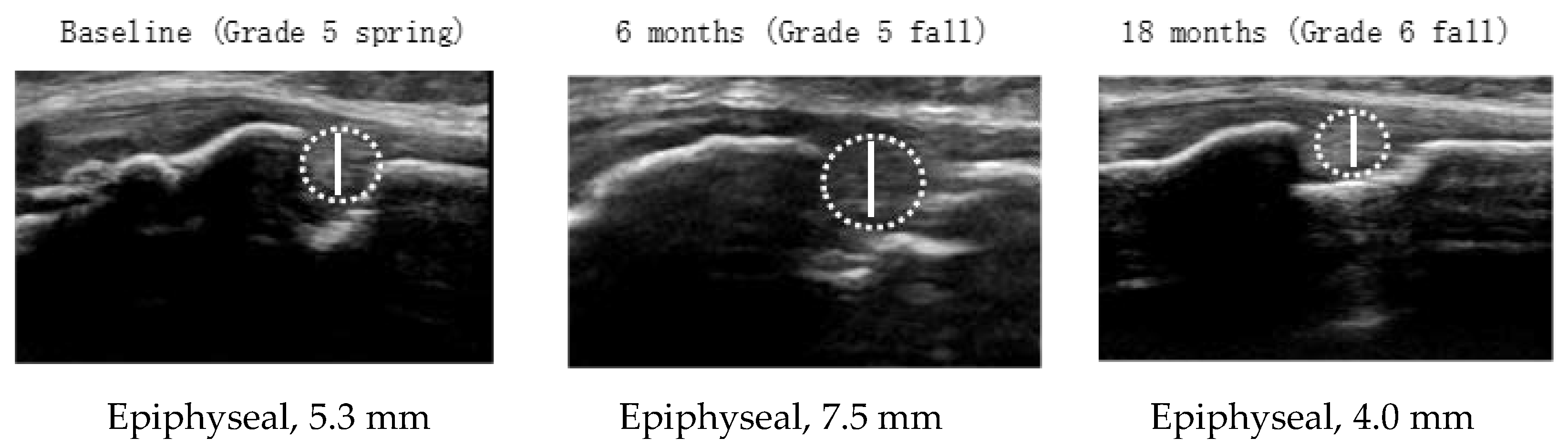
, Epiphyseal stage  . * Measurement points showing ≥20% consecutive increases in cartilage thickness from the previous measurement during observation. A girl who showed ≥20% consecutive increases in cartilage thickness in grade 5 fall developed OSD.
, Apophyseal stage , Epiphyseal stage . * Measurement points showing ≥20% consecutive increases in cartilage thickness from the previous measurement during observation. A girl who showed ≥20% consecutive increases in cartilage thickness in grade 5 fall developed OSD.
. * Measurement points showing ≥20% consecutive increases in cartilage thickness from the previous measurement during observation. A girl who showed ≥20% consecutive increases in cartilage thickness in grade 5 fall developed OSD.
, Apophyseal stage , Epiphyseal stage . * Measurement points showing ≥20% consecutive increases in cartilage thickness from the previous measurement during observation. A girl who showed ≥20% consecutive increases in cartilage thickness in grade 5 fall developed OSD.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Profiles of Subjects | Boys (n = 52) | Girls (n = 72) | |
|---|---|---|---|
| Demographic characteristics | |||
| Age (year) | 10.9 ± 0.7 | 10.9 ± 0.8 | |
| Height (cm) | 144 ± 6 | 147 ± 8 | |
| Weight (kg) | 36.5 ± 5.4 | 39.3 ± 7.9 | |
| Appearance of secondary sex characteristics * | 1 (2) | 28 (39) | |
| Sports club affiliation | 35 (69) | 46 (64) | |
| Results of a musculoskeletal examination | |||
| Basic movements | |||
| Inability to squat | 5 (10) | 14 (19) | |
| Inability to bend forward | 13 (25) | 7 (10) | |
| Musculoskeletal problems | |||
| Chronic pain (systemic) | 2 (4) | 16 (22) | |
| Chronic pain (knee) | 1 (2) | 9 (13) | |
| Musculoskeletal disorder (systemic) | 10 (19) | 14 (19) | |
| Osgood–Schlatter disease | 0 | 5 (7) | |
| Boys | Cartilaginous Stage a | Apophyseal Stage b | Epiphyseal Stage c | Bony Stage | p-Value # | Multiple Comparisons ## |
| n = 52 (100) | 22 (42) | 12 (23) | 18 (35) | 0 | ||
| Demographic characteristics | ||||||
| Age (years) | 10.5 ± 0.6 | 11.3 ± 0.6 | 11.3 ± 0.5 | - | <0.001 | a < b **, a < c ** |
| Height (cm) | 139 ± 4 | 145 ± 3 | 150 ± 5 | - | <0.001 | a < b **, a < c **, b < c ** |
| Weight (kg) | 33 ± 4 | 34 ± 5 | 40 ± 7 | - | <0.001 | a < b *, a < c **, b < c * |
| Appearance of voice change | 0 | 0 | 1/18 (6) | - | 0.382 | |
| Sports club affiliation | 11/22 (50) | 9/12 (75) | 15/18 (83) | - | 0.067 | |
| Osgood–Schlatter disease | 0 | 0 | 0 | - | - | |
| Cartilage thickness (mm) | 8.1 ± 1.4 | 6.2 ± 1.2 | 5.3 ± 0.7 | - | <0.001 | a > b **, a > c ** |
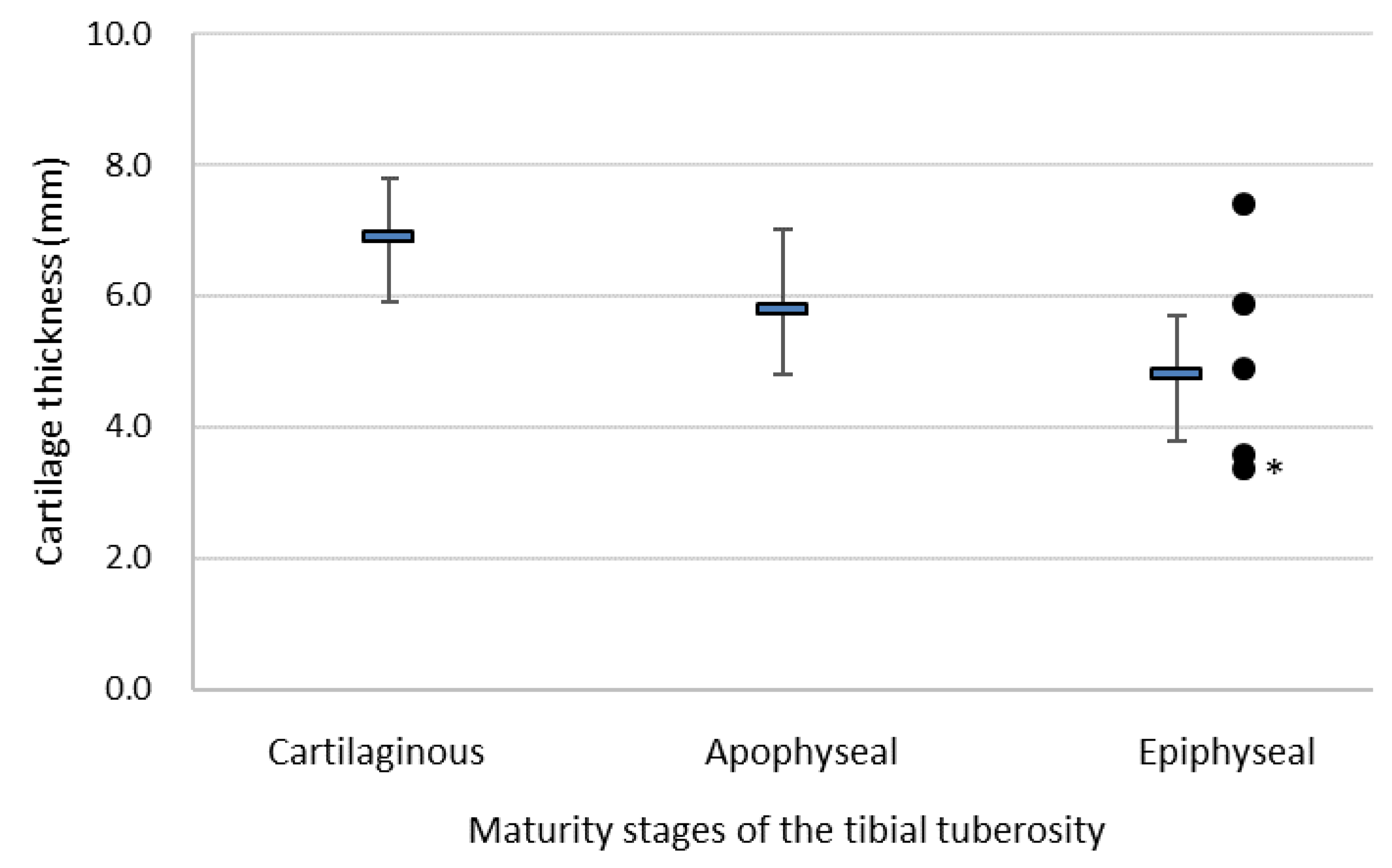
| Girls | Cartilaginous Stage a | Apophyseal Stage b | Epiphyseal Stage c | Bony Stage | p-Value # | Multiple Comparisons ## |
| n = 72 (100) | 2 (3) | 5 (7) | 64 (89) | 1 (1) | ||
| Demographic characteristics | ||||||
| Age (years) | 10.0 ± 0.0 | 10.2 ± 0.4 | 11.0 ± 0.8 | 11 | 0.013 | a’< c’ **, b’ < c’ * |
| Height (cm) | 132 ± 4 | 136 ± 2 | 148 ± 7 | 154 | 0.008 | b’ < c’ ** |
| Weight (kg) | 29 ± 0 | 29 ± 2 | 40 ± 7 | 53 | <0.001 | a’ < c’ **, b’ < c’ ** |
| Appearance of menarche | 0 | 0 | 27/64 (42) | 1/1(100) | 0.097 | |
| Sports club affiliation | 2/2 (100) | 4/5 (80) | 39/64 (61) | 1/1(100) | 0.475 | |
| Osgood–Schlatter disease | 0 | 0 | 5/64 (8) | 0 | 0.880 | |
| Cartilage thickness (mm) | 6.9 ± 0.9 | 5.8 ± 1.2 | 4.8 ± 0.9 | 0 | 0.002 | a > c * |
| Variables | n | Cartilage Thickness (mm) | p-Value ** | |
|---|---|---|---|---|
| Sex | ||||
| Males | 52 | 5.9 ± 1.2 | ||
| Female | 72 | 5.5 ± 1.0 | 0.060 | |
| Age | ||||
| 10 or 11 y | 94 | 5.7 ± 1.1 | ||
| 12 y | 30 | 5.2 ± 1.0 | 0.013 | |
| Height | ||||
| ≥145cm | 57 | 5.6 ± 1.2 | ||
| <145cm | 67 | 5.7 ± 1.0 | 0.846 | |
| Weight | ||||
| ≥37kg | 59 | 5.9 ± 1.1 | ||
| <37kg | 65 | 5.4 ± 1.0 | 0.057 | |
| Secondary sex characteristics * | ||||
| None | 95 | 5.7 ± 1.0 | ||
| Present | 29 | 5.1 ± 1.1 | 0.009 | |
| Sports club affiliation | ||||
| Belonged | 81 | 5.8 ± 1.1 | ||
| Not belonged | 43 | 5.3 ± 0.9 | 0.021 | |
| Osgood–Schlatter disease | ||||
| No | 119 | 5.6 ± 1.1 | ||
| Yes | 5 | 6.1 ± 1.5 | 0.321 | |
| Boys (n = 10) | Base Line a Grade 5 Spring | 6 Months b Grade 5 Fall | 18 Months c Grade 6 Fall | p-Value # | Multiple Comparisons ## |
| Demographic characteristics | |||||
| Age (y) | 10.1 ± 0.3 | 10.5 ± 0.5 | 11.6 ± 0.5 | <0.001 | a < b *, a < c **, b < c ** |
| Height (cm) | 138 ± 4 | 140 ± 4 | 147 ± 5 | <0.001 | a < b **, a < c **, b < c ** |
| Weight (kg) | 32.8 ± 4.9 | 34.3 ± 5.1 | 37.8 ± 5.1 | <0.001 | a < b **, a < c **, b < c ** |
| Appearance of voice change | 0 | 0 | 0 | ||
| Sports club affiliation | 6 (60) | 6 (60) | 7 (70) | ||
| Osgood–Schlatter disease | 0 | 0 | 0 | ||
| Tibial tuberosity maturity stages | |||||
| Cartilaginous stage | 9 (90) | 8 (80) | 2 (20) | ||
| Apophyseal stage | 1 (10) | 2 (20) | 5 (50) | ||
| Epiphyseal stage | 0 | 0 | 3 (30) | ||
| Bony stage | 0 | 0 | 0 | ||
| Cartilage thickness (mm) | 7.8 ± 1.1 | 8.1 ± 1.8 | 6.3 ± 2.0 | <0.001 | a > c **, b > c ** |
| Girls (n = 16) | Base Line a Grade 5 Spring | 6 Months b Grade 5 Fall | 18 Months c Grade 6 Fall | p-Value # | Multiple Comparisons ## |
| Demographic characteristics | |||||
| Age (y) | 10.1 ± 0.3 | 10.5 ± 0.5 | 11.6 ± 0.5 | <0.001 | a < b **, a < c **, b < c ** |
| Height (cm) | 139 ± 5 | 142 ± 5 | 149 ± 4 | <0.001 | a < b **, a < c **, b < c ** |
| Weight (kg) | 32.5 ± 5.5 | 34.8 ± 5.9 | 40.7 ± 6.0 | <0.001 | a < b **, a < c **, b < c ** |
| Appearance of menarche | 1 (6) | 2 (13) | 9 (56) | ||
| Sports club affiliation | 11 (69) | 12 (75) | 10 (63) | ||
| Osgood–Schlatter disease | 0 | 1 (6) | 1 (6) | ||
| Tibial tuberosity maturity stages | |||||
| Cartilaginous stage | 2 (13) | 0 | 0 | ||
| Apophyseal stage | 3 (19) | 2 (13) | 0 | ||
| Epiphyseal stage | 11 (69) | 14 (88) | 16 (100) | ||
| Bony stage | 0 | 0 | 0 | ||
| Cartilage thickness (mm) | 5.3 ± 1.2 | 5.4 ± 0.9 | 4.9 ± 0.7 | 0.282 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohtaka, M.; Hiramoto, I.; Minagawa, H.; Matsuzaki, M.; Kodama, H. Screening of the Maturity Status of the Tibial Tuberosity by Ultrasonography in Higher Elementary School Grade Schoolchildren. Int. J. Environ. Res. Public Health 2019, 16, 2138. https://doi.org/10.3390/ijerph16122138
Ohtaka M, Hiramoto I, Minagawa H, Matsuzaki M, Kodama H. Screening of the Maturity Status of the Tibial Tuberosity by Ultrasonography in Higher Elementary School Grade Schoolchildren. International Journal of Environmental Research and Public Health. 2019; 16(12):2138. https://doi.org/10.3390/ijerph16122138
Chicago/Turabian StyleOhtaka, Maiko, Izumi Hiramoto, Hiroshi Minagawa, Masashi Matsuzaki, and Hideya Kodama. 2019. "Screening of the Maturity Status of the Tibial Tuberosity by Ultrasonography in Higher Elementary School Grade Schoolchildren" International Journal of Environmental Research and Public Health 16, no. 12: 2138. https://doi.org/10.3390/ijerph16122138
APA StyleOhtaka, M., Hiramoto, I., Minagawa, H., Matsuzaki, M., & Kodama, H. (2019). Screening of the Maturity Status of the Tibial Tuberosity by Ultrasonography in Higher Elementary School Grade Schoolchildren. International Journal of Environmental Research and Public Health, 16(12), 2138. https://doi.org/10.3390/ijerph16122138