Road Traffic Noise Exposure and Birth Outcomes: An Updated Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Systematic Review Protocol
2.2. Data Extraction
2.3. Risk of Bias Assessment
2.4. Meta-Analysis
2.5. Quality of Evidence Assessment
3. Results
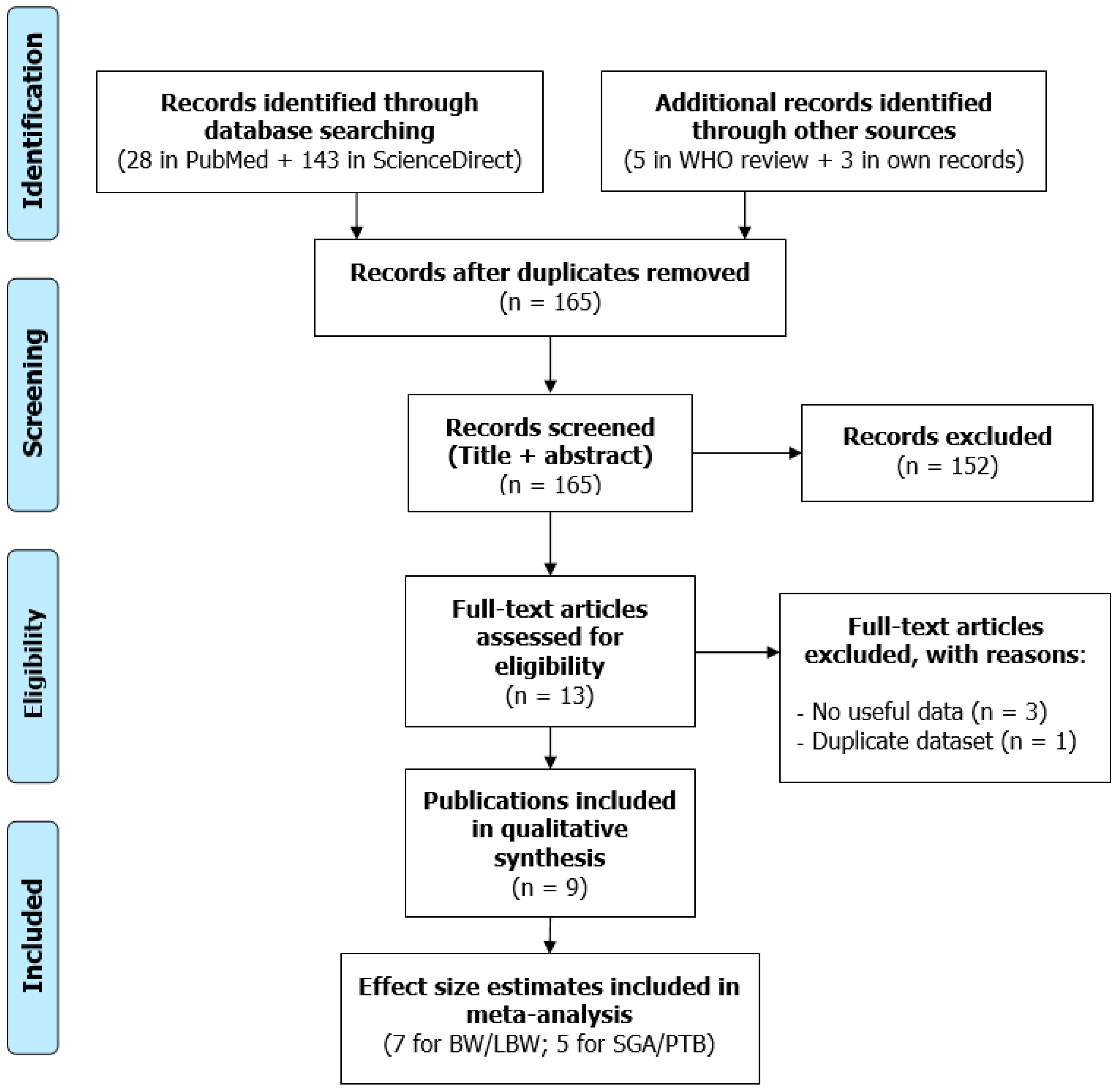
3.1. Literature Search Results
3.2. Narrative Description of the Studies Included
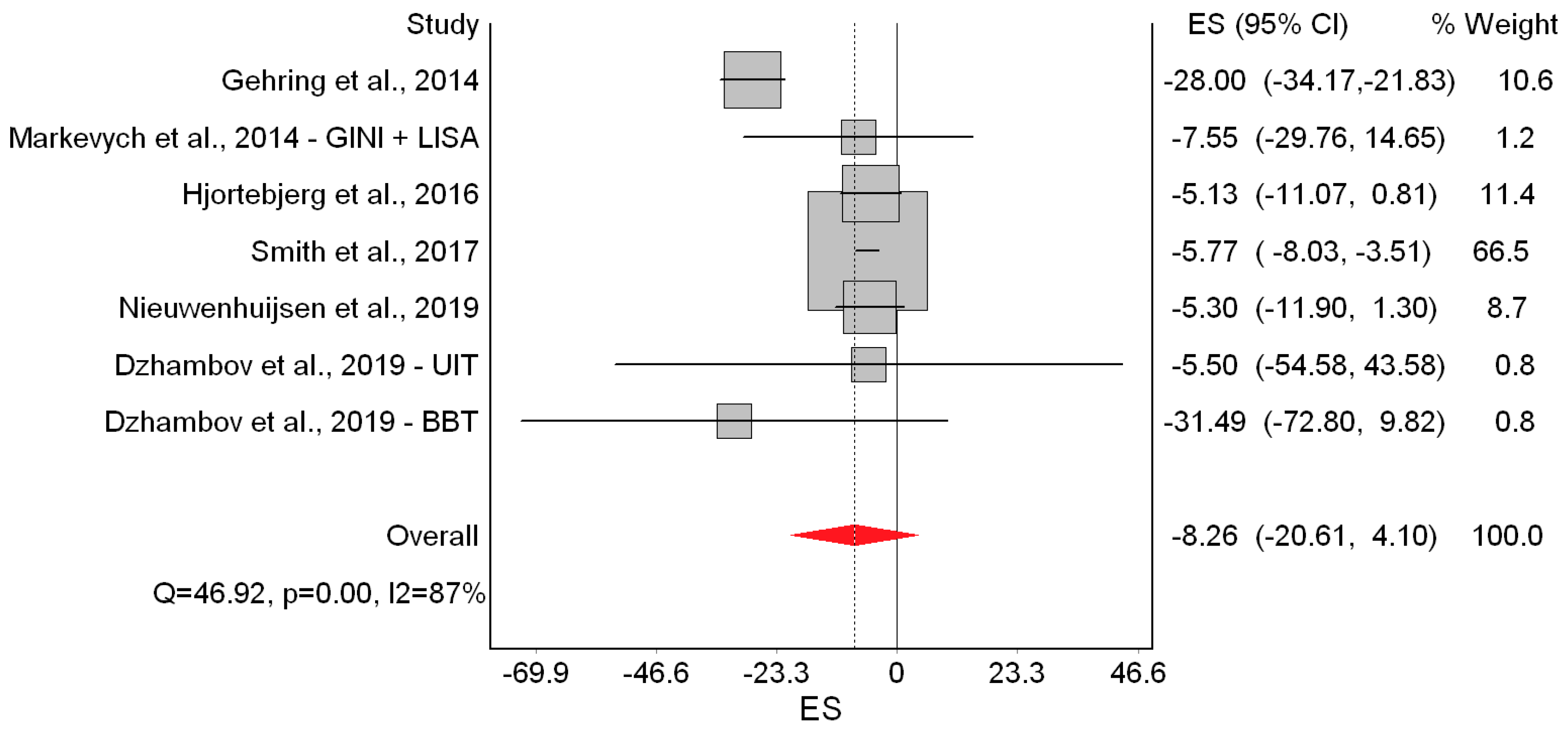
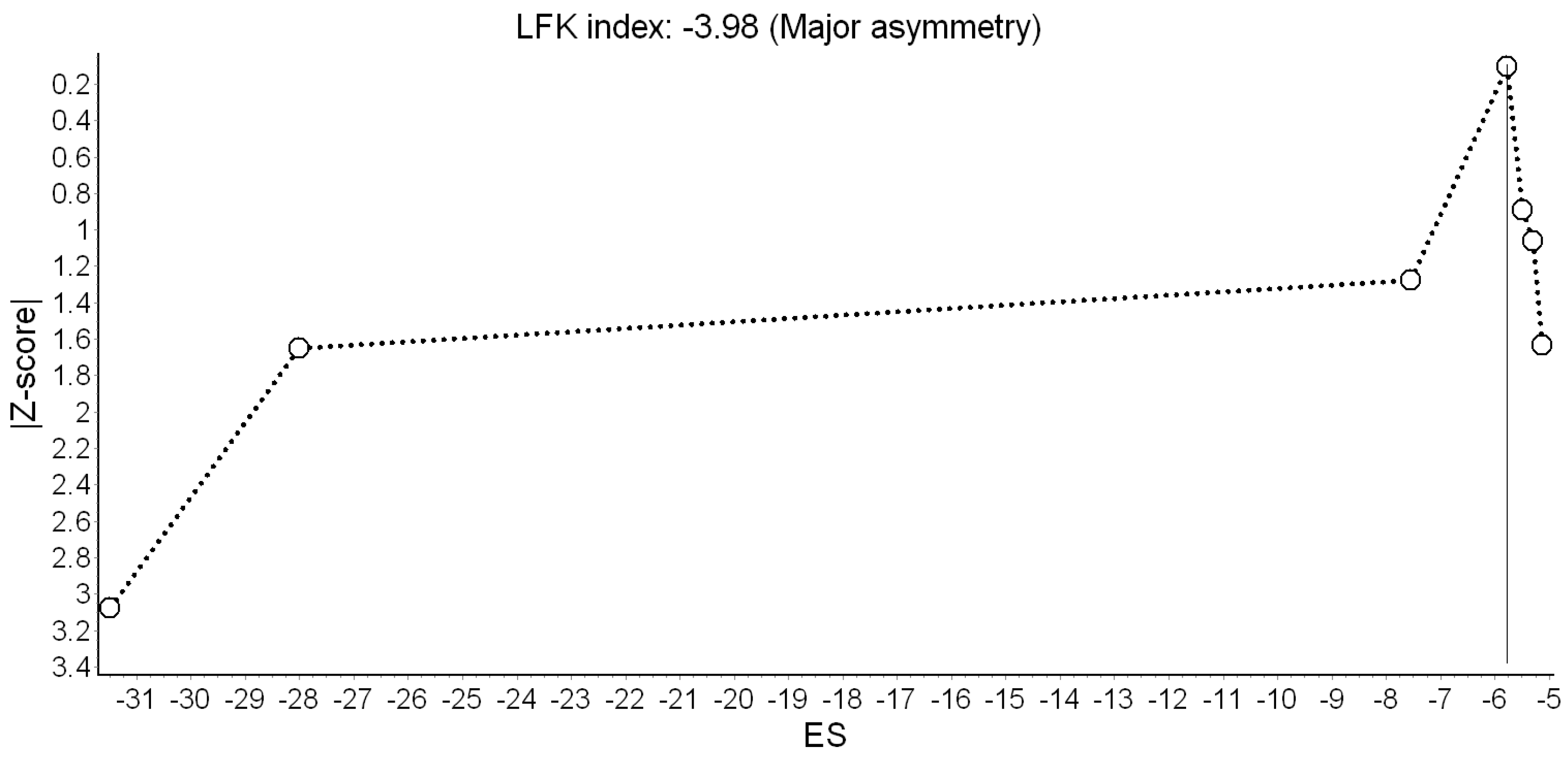
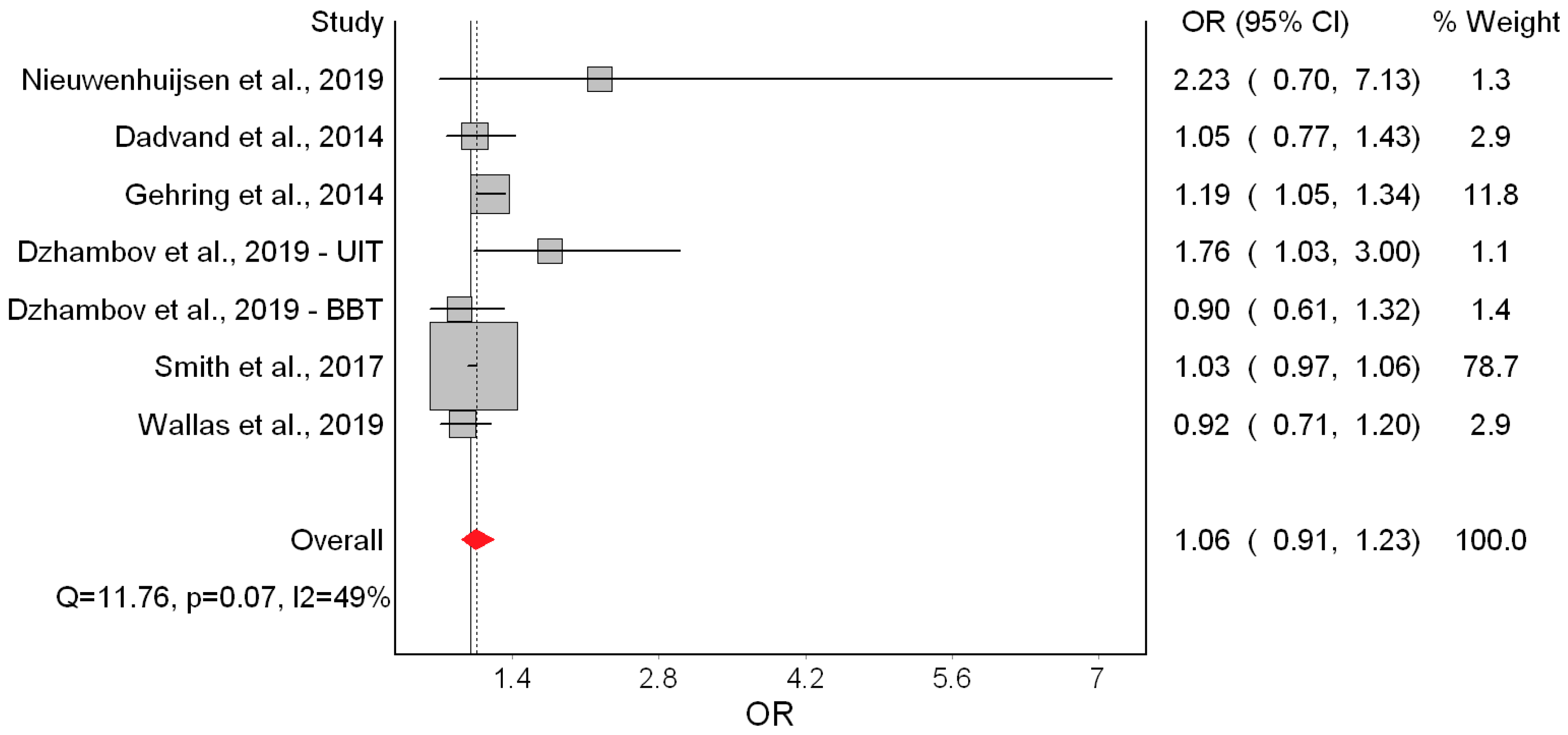
3.3. Main Meta-Analysis
3.4. Crude and Air Pollution-Adjusted Effects
4. Discussion
4.1. Major Findings
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bias Criteria |
|---|
| Publication type |
| 0 = Not peer reviewed |
| 1 = Peer reviewed article |
| Study design |
| 0 = Ecological |
| 1 = Cross-sectional |
| 2 = Case control |
| 3 = Cohort study |
| Selection of participants |
| 0 = No random sampling OR response rate less than 60% OR attrition rate higher than 20% OR no information provided |
| 3 = Participants randomly sampled from a known population AND response rate higher than 60%/whole source population sampled AND attrition rate less than 20% in follow-up studies |
| Noise exposure quality |
| 0 = Subjective method |
| 1 = Objective method, low accuracy (e.g., land-use regression model, missing values) |
| 2 = Objective method, limited accuracy or validity (e.g., postcode/street-level exposure, modelling only/no measurements, no data on floor, noise barriers, poor data on traffic) |
| 3 = Objective method, accurate and valid (e.g., modelling and measurements, traffic evaluation) |
| Noise exposure timeframe |
| 1 = Timeframe outside pregnancy and delivery |
| 2 = Exposure at the date of delivery |
| 3 = Exposure during pregnancy |
| Assessment of birth outcomes |
| 0 = Subjective assessment by report of mother |
| 2 = Objective (e.g., from medical records) |
| Confounding factors |
| 0 = None or only one important confounding factor considered (maternal age or smoking/alcohol or education/socioeconomic position) |
| 1 = Confounding factors considered and at least two of the following are considered: Maternal age; smoking/alcohol; education/socioeconomic position; gestational age (for birth weight and LBW—not relevant if only term births are considered) |
| 2 = Consideration of all of the above confounders |
| 3 = Consideration of all of the above and maternal BMI |
| 4 = Consideration of all of the above and at least one of the following: Ethnicity; marital status/single mother; obstetric history; season/temperature; urbanicity |
| Statistical analysis |
| 0 = Flaws in or inappropriate statistical testing or interpretation of statistical tests that may have affected results |
| 2 = Appropriate statistical testing and interpretation of tests |
| Additional bias |
| 0 = Several other study design or conduct issues that may have led to bias |
| 1 = One other serious study flaw |
| 3 = No other study serious flaws |
| Study | Publication Type | Study Design | Selection of Participants | Noise Exposure Quality | Noise Exposure Timeframe | Birth Outcomes | Confounding Factors | Statistics | Bias | Overall Bias |
|---|---|---|---|---|---|---|---|---|---|---|
| Gehring et al. [18] | 1 | 3 | 3 | 2 (postcode-level) | 3 | 2 | 2 | 2 | 3 | 21 |
| Dadvand et al. [19] | 1 | 3 | 3 | 2 (street-level) | 3 | 2 | 4 | 2 | 3 | 23 |
| Markevych et al. [15] | 1 | 1 | 0 (1818 of 9086) | 2 (no floor) | 1 | 2 | 2 | 2 | 3 | 14 |
| Hjortebjerg et al. [22] | 1 | 3 | 3 | 2 (no floor/barriers) | 3 | 2 | 4 | 2 | 3 | 23 |
| Barba-Vasseur et al. [9] | 1 | 2 | 3 | 3 (floor data) | 2 | 2 | 1 | 2 | 0 1,2 | 16 |
| Smith et al. [10] | 1 | 3 | 3 | 2 (no floor/barriers) | 2 | 2 | 2 | 2 | 0 1,3 | 17 |
| Wallas et al. [11] | 1 | 3 | 0 (baseline response not reported) | 2 (no floor/barriers) | 3 | 2 | 1 | 2 | 3 | 17 |
| Nieuwenhuijsen et al. [12] | 1 | 3 | 0 (baseline response not reported) | 1 (45% missing values) | 2 | 2 | 4 | 2 | 1 1 | 16 |
| Dzhambov et al. UIT [13] | 1 | 1 | 0 (573 of 1280) | 2 (less precise than the BBT survey) | 1 | 2 | 2 | 2 | 3 | 14 |
| Dzhambov et al. BBT [13] | 1 | 1 | 0 (518 of 1251) | 3 (advanced scientific methods, high resolution) | 1 | 2 | 2 | 2 | 3 | 15 |
| Study | Birth Weight (Study Weight %) | LBW (Study Weight %) | SGA (Study Weight %) | PTB (Study Weight %) | ||||
|---|---|---|---|---|---|---|---|---|
| WHO Scores | Alternative Scores | WHO Scores | Alternative Scores | WHO Scores | Alternative Scores | WHO Scores | Alternative Scores | |
| Gehring et al. [18] | 10.6% | 12.6% | 11.8% | 13.7% | 10.4% | 13.6% | 79.9% | 79.8% |
| Dadvand et al. [19] | - | - | 2.9% | 6.1% | 2.4% | 6.9% | - | - |
| Markevych et al. [15] | 1.2% | 3.0% | - | - | - | - | - | - |
| Hjortebjerg et al. [22] | 11.4% | 14.5% | - | - | - | - | - | - |
| Barba-Vasseur et al. [9] | - | - | - | - | - | - | 5.5% | 5.4% |
| Smith et al. [10] | 66.5% | 55.5% | 78.7% | 65.4% | 85.0% | 71.5% | - | - |
| Wallas et al. [11] | - | - | 2.9% | 5.0% | - | - | 7.6% | 7.2% |
| Nieuwenhuijsen et al. [12] | 8.7% | 8.7% | 1.3% | 3.2% | - | - | - | - |
| Dzhambov et al. [13] – UIT | 0.8% | 2.7% | 1.1% | 3.1% | 1.1% | 3.8% | 3.4% | 3.6% |
| Dzhambov et al. [13] – BBT | 0.8% | 2.9% | 1.4% | 3.6% | 1.1% | 4.1% | 3.5% | 4.0% |
References
- Guski, R.; Schreckenberg, D.; Schuemer, R. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Annoyance. Int. J. Environ. Res. Public Health 2017, 14, 1539. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.; Paunovic, K. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Quality of Life, Wellbeing and Mental Health. Int. J. Environ. Res. Public Health 2018, 15, 2400. [Google Scholar] [CrossRef] [PubMed]
- Basner, M.; McGuire, S. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Effects on Sleep. Int. J. Environ. Res. Public Health 2018, 15, 519. [Google Scholar] [CrossRef] [PubMed]
- Van Kempen, E.; Casas, M.; Pershagen, G.; Foraster, M. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Cardiovascular and Metabolic Effects: A Summary. Int. J. Environ. Res. Public Health 2018, 15, 379. [Google Scholar] [CrossRef] [PubMed]
- Jarosińska, D.; Héroux, M.-È.; Wilkhu, P.; Creswick, J.; Verbeek, J.; Wothge, J.; Paunović, E. Development of the WHO Environmental Noise Guidelines for the European Region: An Introduction. Int. J. Environ. Res Public Health 2018, 15, 813. [Google Scholar] [CrossRef] [PubMed]
- WHO. Environmental Noise Guidelines for the European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- Nieuwenhuijsen, M.J.; Ristovska, G.; Dadvand, P. WHO Environmental Noise Guidelines for the European Region: A Systematic Review on Environmental Noise and Adverse Birth Outcomes. Int. J. Environ. Res Public Health 2017, 14, 1252. [Google Scholar] [CrossRef] [PubMed]
- Dzhambov, A.M.; Dimitrova, D.D.; Dimitrakova, E.D. Noise exposure during pregnancy, birth outcomes and fetal development: Meta-analyses using quality effects model. Folia Med. 2014, 56, 204–214. [Google Scholar] [CrossRef]
- Barba-Vasseur, M.; Bernard, N.; Pujol, S.; Sagot, P.; Riethmuller, D.; Thiriez, G.; Houot, H.; Defrance, J.; Mariet, A.S.; Luu, V.P.; et al. Does low to moderate environmental exposure to noise and air pollution influence preterm delivery in medium-sized cities? Int. J. Epidemiol. 2017, 46, 2017–2027. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.B.; Fecht, D.; Gulliver, J.; Beevers, S.D.; Dajnak, D.; Blangiardo, M.; Ghosh, R.E.; Hansell, A.L.; Kelly, F.J.; Anderson, H.R.; et al. Impact of London’s road traffic air and noise pollution on birth weight: Retrospective population based cohort study. BMJ 2017, 359, 5299. [Google Scholar] [CrossRef] [PubMed]
- Wallas, A.; Ekström, S.; Bergström, A.; Eriksson, C.; Gruzieva, O.; Sjöström, M.; Pyko, A.; Ögren, M.; Bottai, M.; Pershagen, G. Traffic noise exposure in relation to adverse birth outcomes and body mass between birth and adolescence. Environ. Res. 2019, 169, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuijsen, M.J.; Agier, L.; Basagaña, X.; Urquiza, J.; Tamayo-Uria, I.; Giorgis-Allemand, L.; Robinson, O.; Siroux, V.; Maitre, L.; de Castro, M.; et al. Influence of the Urban Exposome on Birth Weight. Environ. Health Perspect. 2019, 127, 47007. [Google Scholar] [CrossRef] [PubMed]
- Dzhambov, A.M.; Markevych, I.; Lercher, P. Associations of residential greenness, traffic noise, and air pollution with birth outcomes across Alpine areas. Sci. Total Environ. 2019, 678, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; the PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Int. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Markevych, I.; Fuertes, E.; Tiesler, C.M.; Birk, M.; Bauer, C.P.; Koletzko, S.; von Berg, A.; Berdel, D.; Heinrich, J. Surrounding greenness and birth weight: Results from the GINIplus and LISAplus birth cohorts in Munich. Health Place 2014, 26, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Díaz, J.; Ortiz, C.; Carmona, R.; Sáez, M.; Linares, C. Short term effect of air pollution, noise and heat waves on preterm births in Madrid (Spain). Environ. Res. 2016, 145, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V.; Díaz, J.; Carmona, R.; Ortiz, C.; Linares, C. Impact of air pollution and temperature on adverse birth outcomes: Madrid, 2001–2009. Environ. Pollut. 2016, 218, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Gehring, U.; Tamburic, L.; Sbihi, H.; Davies, H.W.; Brauer, M. Impact of noise and air pollution on pregnancy outcomes. Epidemiology 2014, 25, 351–358. [Google Scholar] [CrossRef]
- Dadvand, P.; Ostro, B.; Figueras, F.; Foraster, M.; Basagaña, X.; Valentín, A.; Martinez, D.; Beelen, R.; Cirach, M.; Hoek, G.; et al. Residential Proximity to Major Roads and Term Low Birth Weight: The Roles of Air Pollution, Heat, Noise, and Road-adjacent Trees. Epidemiology 2014, 25, 518–525. [Google Scholar] [CrossRef]
- Babisch, W. Road traffic noise and cardiovascular risk. Noise Health 2008, 10, 27–33. [Google Scholar] [CrossRef]
- Dzhambov, A.M.; Dimitrova, D.D. Residential road traffic noise as a risk factor for hypertension in adults: Systematic review and meta-analysis of analytic studies published in the period 2011–2017. Environ. Pollut. 2018, 240, 306–318. [Google Scholar] [CrossRef]
- Hjortebjerg, D.; Andersen, A.M.N.; Ketzel, M.; Pedersen, M.; Raaschou-Nielsen, O.; Sørensen, M. Associations between maternal exposure to air pollution and traffic noise and newborn’s size at birth: A cohort study. Environ. Int. 2016, 95, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Vienneau, D.; Eze, I.C.; Probst-Hensch, N.; Rȍȍsli, M. Association between transportation noise and cardio-metabolic diseases: An update of the WHO meta-analysis. In Proceedings of the 23rd International Congress on Acoustics, Aachen, Germany, 9–13 September 2019. [Google Scholar]
- Brockwell, S.E.; Gordon, I.R. A simple method for inference on an overall effect in meta-analysis. Stat. Med. 2007, 26, 4531–4543. [Google Scholar] [CrossRef] [PubMed]
- Cornell, J.E.; Mulrow, C.D.; Localio, R.; Stack, C.B.; Meibohm, A.R.; Guallar, E.; Goodman, S.N. Random-effects meta-analysis of inconsistent effects: A time for change. Ann. Intern. Med. 2014, 160, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Doi, S.A.; Barendregt, J.J.; Khan, S.; Thalib, L.; Williams, G.M. Advances in the meta-analysis of heterogeneous clinical trials I: The inverse variance heterogeneity model. Contemp. Clin. Trials. 2015, 45, 130–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doi, S.A.; Barendregt, J.J.; Khan, S.; Thalib, L.; Williams, G.M. Simulation Comparison of the Quality Effects and Random Effects Methods of Meta-analysis. Epidemiology 2015, 26, e42–e44. [Google Scholar] [CrossRef] [PubMed]
- Doi, S.A.R.; Furuya-Kanamori, L.; Thalib, L.; Barendregt, J.J. Meta-analysis in evidence-based healthcare: A paradigm shift away from random effects is overdue. Int. J. Evid. Based Healthc. 2017, 15, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Furuya-Kanamori, L.; Barendregt, J.J.; Doi, S.A.R. A new improved graphical and quantitative method for detecting bias in meta-analysis. Int. J. Evid. Based Healthc. 2018, 16, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Barendregt, J.J.; Doi, S.A. MetaXL User Guide: Version 5.3.; EpiGear International Pty Ltd.: Queensland, Australia, 2016. [Google Scholar]
- Furuya-Kanamori, L.; Doi, S.A. Angry Birds, Angry Children, and Angry Meta-Analysts: A Reanalysis. Perspect. Psychol. Sci. 2016, 11, 408–414. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Hystad, P.; Davies, H.W.; Frank, L.; Van Loon, J.; Gehring, U.; Tamburic, L.; Brauer, M. Residential greenness and birth outcomes: Evaluating the influence of spatially correlated built-environment factors. Environ. Health Perspect. 2014, 122, 1095–1102. [Google Scholar] [CrossRef]
- Wu, T.N.; Chen, L.J.; Lai, J.S.; Ko, G.N.; Shen, C.Y.; Chang, P.Y. Prospective study of noise exposure during pregnancy on birth weight. Am. J. Epidemiol. 1996, 143, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Cusack, L.; Sbihi, H.; Larkin, A.; Chow, A.; Brook, J.R.; Moraes, T.; Mandhane, P.J.; Becker, A.B.; Azad, M.B.; Subbarao, P.; et al. CHILD Study Investigators. Residential green space and pathways to term birth weight in the Canadian Healthy Infant Longitudinal Development (CHILD) Study. Int. J. Health Geogr. 2018, 17, 43. [Google Scholar] [CrossRef] [PubMed]
- Weyde, K.V.; Krog, N.H.; Oftedal, B.; Magnus, P.; White, R.; Stansfeld, S.; Øverland, S.; Aasvang, G.M. A Longitudinal Study of Road Traffic Noise and Body Mass Index Trajectories from Birth to 8 Years. Epidemiology 2018, 29, 729–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ristovska, G.; Laszlo, H.E.; Hansell, A.L. Reproductive Outcomes Associated with Noise Exposure—A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2014, 11, 7931–7952. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.S. The epidemiology of adverse pregnancy outcomes: An overview. J. Nutr. 2003, 133, 1592S–1596S. [Google Scholar] [CrossRef] [PubMed]
- De Bernabé, J.V.; Soriano, T.; Albaladejo, R.; Juarranz, M.; Calle, M.E.; Marti’nez, D.; Domi´nguez-Rojas, V. Risk factors for low birth weight: A review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 116, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Skrivankova, V.; Zwahlen, M.; Adams, M.; Low, N.; Kuehni, C.; Egger, M. Spatial epidemiology of gestational age and birth weight in Switzerland: Census-based linkage study. BioRxiv 2018, 466854. [Google Scholar] [CrossRef] [Green Version]
- Wakefield, J. Ecologic studies revisited. Annu. Rev. Public Health 2008, 29, 75–90. [Google Scholar] [CrossRef]
- Greenland, S. Ecologic versus individual-level sources of bias in ecologic estimates of contextual health effects. Int. J. Epidemiol. 2001, 30, 1343–1350. [Google Scholar] [CrossRef]
- Greenland, S. Divergent biases in ecologic and individual-level studies. Stat. Med. 1992, 11, 1209–1223. [Google Scholar] [CrossRef]
- Teixeira, L.R.; Azevedo, T.M.; Bortkiewicz, A.; da Silva, D.T.C.; de Abreu, W.; de Almeida, M.S.; de Araujo, M.A.N.; Gadzicka, E.; Ivanov, I.D.; Leppink, N.; et al. WHO/ILO work-related burden of disease and injury: Protocol for systematic reviews of exposure to occupational noise and of the effect of exposure to occupational noise on cardiovascular disease. Environ. Int. 2019, 125, 567–578. [Google Scholar] [CrossRef] [PubMed]
- Davey, J.; Turner, R.M.; Clarke, M.J.; Higgins, J.P.T. Characteristics of meta-analyses and their component studies in the Cochrane Database of Systematic Reviews: A cross-sectional, descriptive analysis. BMC Med. Res. Methodol. 2011, 11, 160. [Google Scholar] [CrossRef] [PubMed]
- Stone, J.; Gurunathan, U.; Glass, K.; Munn, Z.; Tugwell, P.; Doi, S.A.R. Stratification by quality induced selection bias in a meta-analysis of clinical trials. J. Clin. Epidemiol. 2019, 107, 51–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]









| Study | Country | Design | Sample | Birth Outcomes | Noise Exposure | Adjustments in Main Model |
|---|---|---|---|---|---|---|
| Gehring et al. [18] | Canada | Cohort (1999/02) | 68,238 singleton live births | Term BW, term LBW, SGA, PTB; Medical records | Modelled road traffic Lden at post code-level; Entire pregnancy; 60.2 ± 5.3 dB (6.2–89) | Sex, parity, nationality, maternal age, smoking, education, income, year and month, gestational week (for BW) |
| Dadvand et al. [19] | Spain | Cohort (2001/05) | 6438 singleton term live births | Term LBW, SGA; Medical records | Modelled road traffic Lden within 50 m of the residence; Entire pregnancy; 68.7 ± 6.7 dB | Area-level SES, ethnicity, maternal education, marital status, age, smoking, alcohol, BMI, diabetes, infection, parity, infant sex, season and year |
| Markevych et al. [15] | Germany | Cross-sectional (1996/99) | 1818 singleton term live births with normal BW | Term BW; Medical records | Modelled road traffic Lden at most exposed façade (noise barriers considered); Data available after delivery (2007); 53.8 ± 9 dB | Maternal age, education, smoking, infant sex, season and year, study area |
| Hjortebjerg et al. [22] | Denmark | Cohort (1996/02) | 75,166 singleton term live births | Term BW; Medical records | Modelled road traffic Lden at most exposed façade; Entire pregnancy; 57.6 dB (49.4 – 69.7) | Gestational age, maternal age, BMI, height, parity, education, income, smoking, alcohol, city, other noise sources, NO2, infant sex, season |
| Barba-Vasseur et al. [9] | France | Case-control, 4:1 (2005/09) | 1191 singleton births | PTB; Medical records | Modelled all-source Lden at each floor and façade; Data available at delivery; ≈ 55 dB (40–70) | Maternal age, parity, smoking |
| Smith et al. [10] | United Kingdom | Cohort (2006/10) | 540,365/471,489 singleton term births | Term BW, Term SGA, Term LBW; Medical records | Modelled road traffic LAeq,16hr at most exposed façade; Data available at delivery; 58.1 ± 5.2 dB (54.7–86) | Infant sex, maternal age, ethnicity, birth registration type, area-level tobacco expenditure, Carstairs quintile, gestational age (for BW/LBW), season of birth, year, area |
| Wallas et al. [11] | Sweden | Cohort (1994/96) | 4089 live births | LBW, PTB; Medical records | Modelled road traffic Lden at most exposed façade; Entire pregnancy; 52.1 dB (25–77.4) | Parental occupation, maternal smoking, BMI, municipality |
| Nieuwenhuijsen et al. [12] | United Kingdom, France, Spain, Lithuania, Norway, Greece | Cohort | 31,458 singleton live term births | Term BW; Medical records | Modelled road traffic Lden; Data available at delivery; 45% imputed values; 54.4 ± 7.2 dB | City, gestational age, infant sex, maternal age, education, parity, height and weight, smoking, season |
| Dzhambov et al. UIT [13] | Austria | Cross-sectional (1985/89) | 573 live births | BW, LBW, SGA, PTB; Medical records | Modelled road traffic Ldn (calibration measurements); Data available after delivery (1997); 46.36 ± 13.8 dB | Infant sex, maternal age, marital status, education, smoking, gestational age (for LBW and BW), duration of residence before conception, house type |
| Dzhambov et al. BBT [13] | Austria, Italy | Cross-sectional (1992/98) | 518 live births | BW, LBW, SGA, PTB; Medical records | Modelled road traffic Lden (calibration measurements); Data available after delivery (2003/04); 49.66 ± 14.3 dB | Infant sex, maternal age, education, smoking, gestational age (for LBW and BW), duration of residence before conception, house type |
| Study | Publication Type | Study Design | Noise Exposure | Birth Outcomes | Confounding Factors | Statistics | Bias | Overall Bias |
|---|---|---|---|---|---|---|---|---|
| Gehring et al. [18] | 1 | 2 | 3 | 2 | 3 | 1 | 1 | 13 (low) |
| Dadvand et al. [19] | 1 | 2 | 3 | 2 | 3 | 1 | 1 | 13 (low) |
| Markevych et al. [15] | 1 | 0 | 3 | 2 | 1 | 1 | 0 1 | 8 (unclear) |
| Hjortebjerg et al. [22] | 1 | 2 | 3 | 2 | 3 | 1 | 1 | 13 (low) |
| Barba-Vasseur et al. [9] | 1 | 2 | 3 | 2 | 1 | 1 | 0 2 | 10 (low) |
| Smith et al. [10] | 1 | 2 | 3 | 2 | 3 | 1 | 0 2,3 | 12 (low) |
| Wallas et al. [11] | 1 | 2 | 3 | 2 | 1 | 1 | 1 | 11 (low) |
| Nieuwenhuijsen et al. [12] | 1 | 2 | 3 | 2 | 3 | 1 | 0 2,4 | 12 (low) |
| Dzhambov et al. UIT [13] | 1 | 0 | 3 | 2 | 1 | 1 | 0 1 | 8 (unclear) |
| Dzhambov et al. BBT [13] | 1 | 0 | 3 | 2 | 1 | 1 | 0 1 | 8 (unclear) |
| Outcome (Model) | N | β/OR | 95% CI | I2 (%) |
|---|---|---|---|---|
| Birth weight | ||||
| Crude | 5 | −18.18 | −44.53, 8.18 | 91 |
| Main | 6 | −8.72 | −25.20, 7.76 | 89 |
| Air pollution-adjusted | 6 | −6.41 | −24.11, 11.29 | 91 |
| Low birth weight | ||||
| Crude | 4 | 1.28 | 1.13, 1.46 | 48 |
| Main | 7 | 1.06 | 0.91, 1.23 | 49 |
| Air pollution-adjusted | 5 | 1.01 | 0.89, 1.14 | 37 |
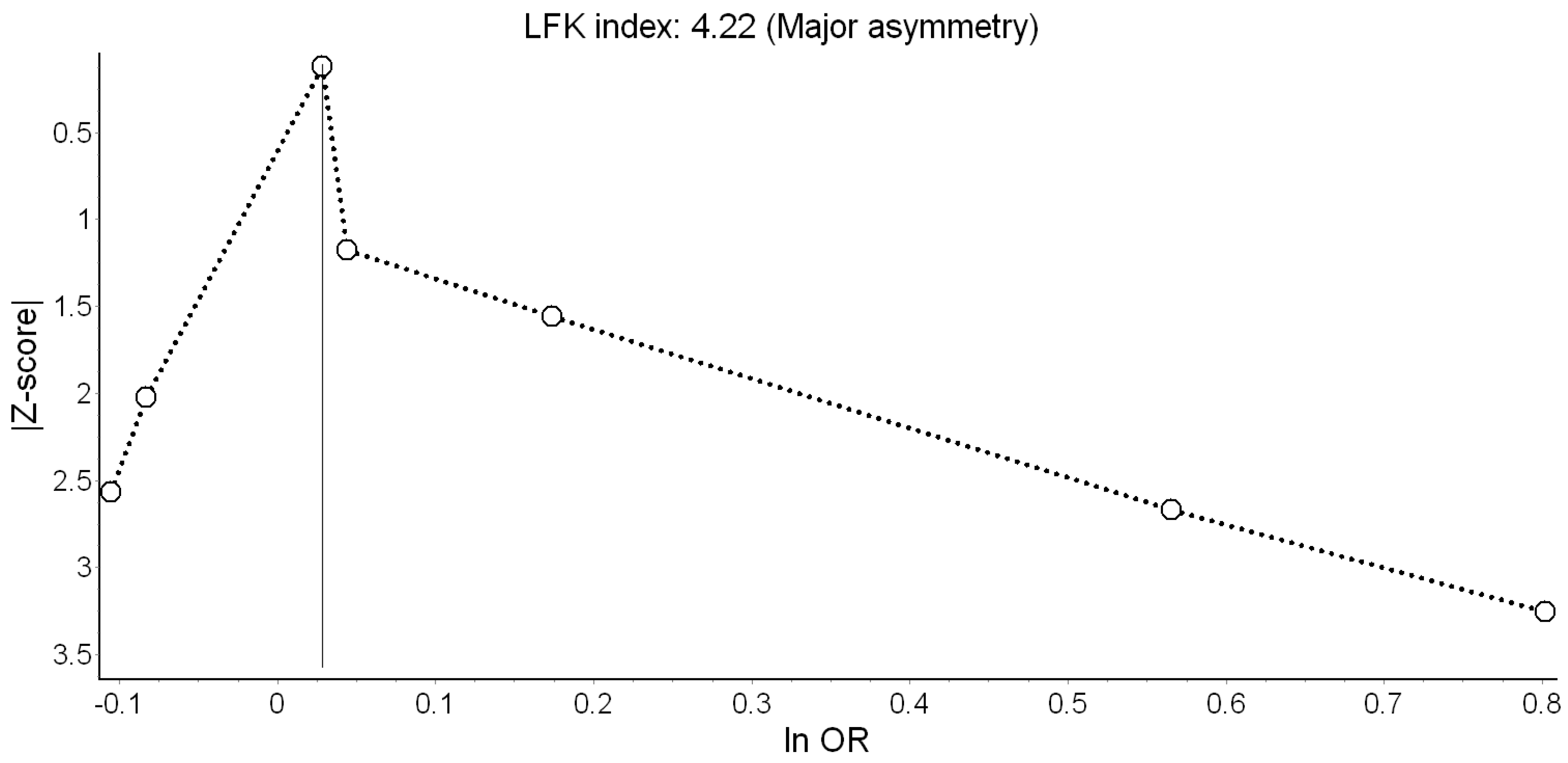
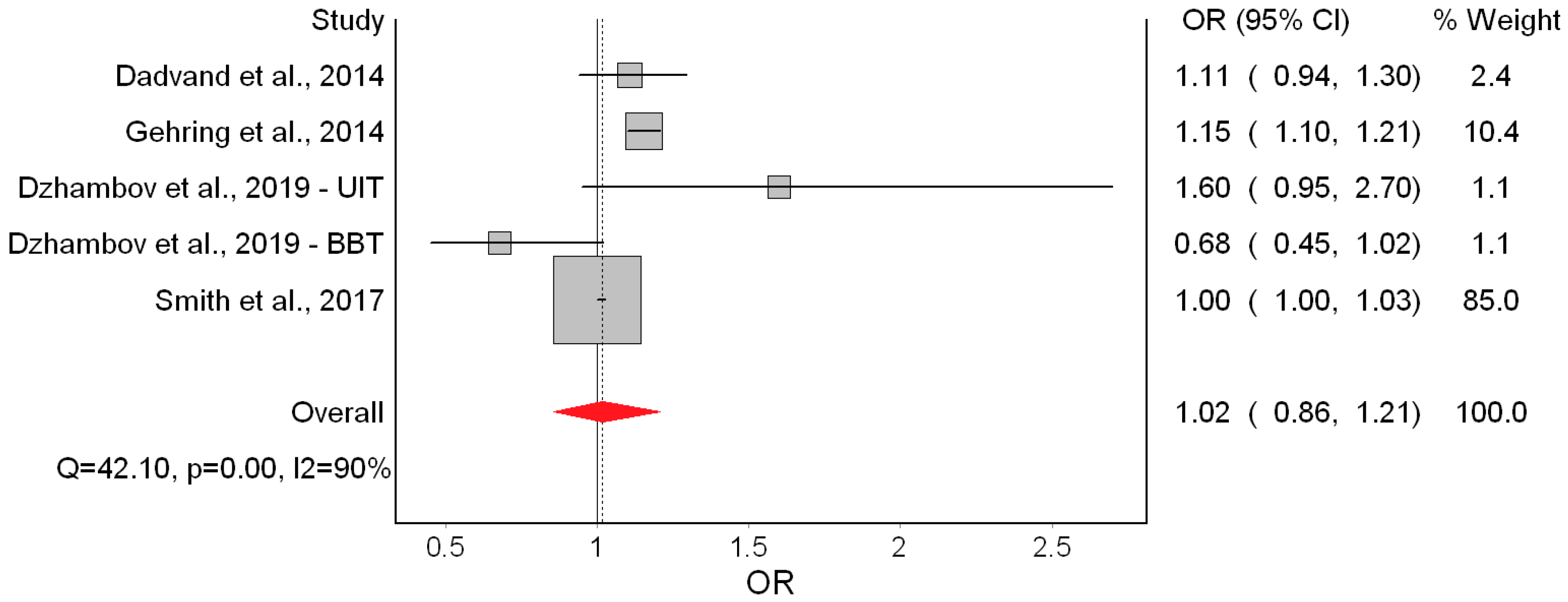
| Small for gestational age | ||||
| Crude | 4 | 1.04 | 0.89, 1.22 | 91 |
| Main | 5 | 1.02 | 0.86, 1.21 | 90 |
| Air pollution-adjusted | 4 | 1.01 | 0.90, 1.15 | 84 |
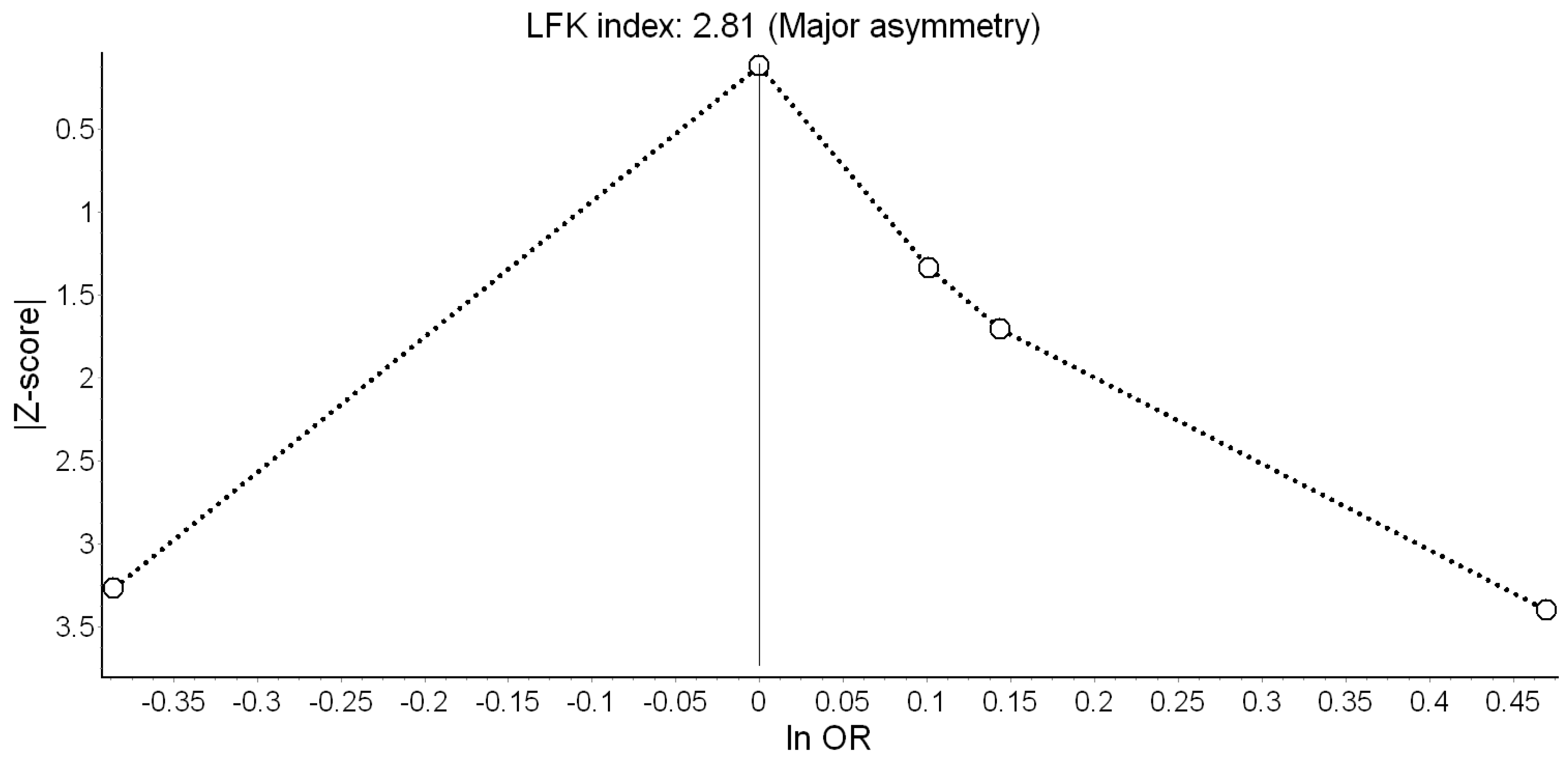
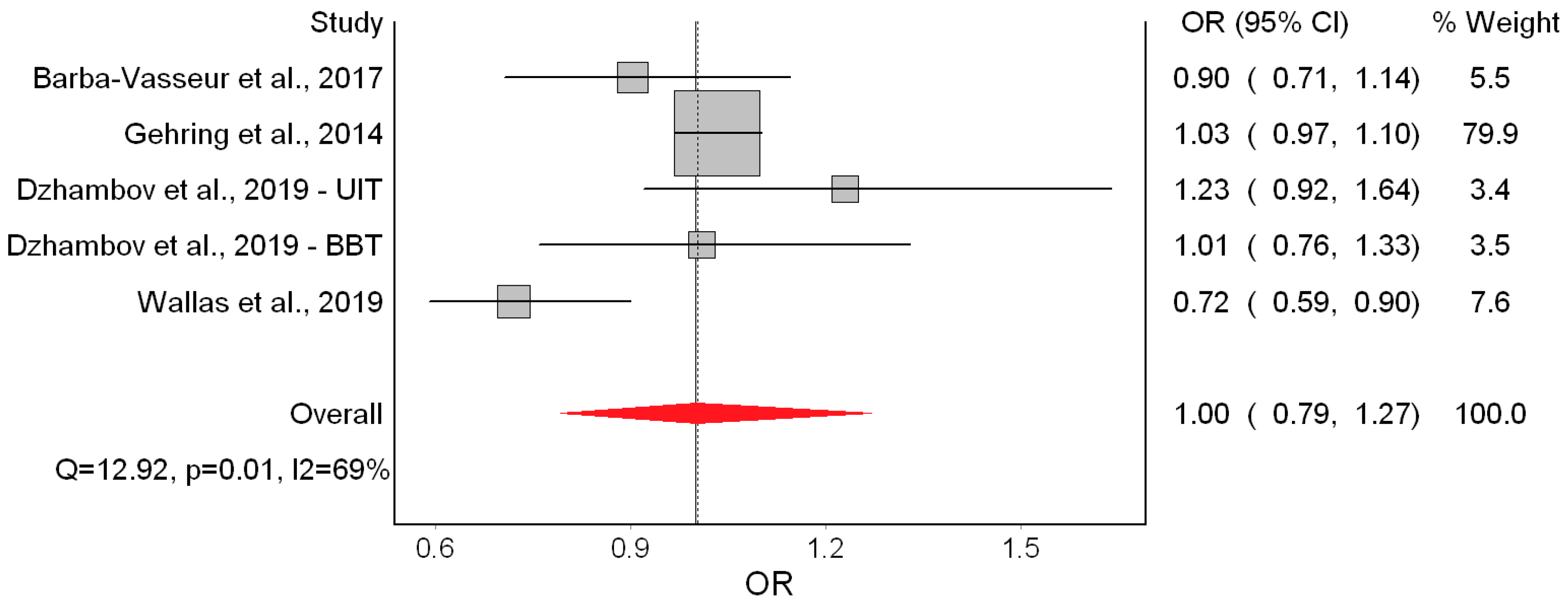
| Preterm birth | ||||
| Crude | 4 | 1.02 | 0.96, 1.09 | 0 |
| Main | 5 | 1.00 | 0.79, 1.27 | 69 |
| Air pollution-adjusted | 3 | 1.00 | 0.79, 1.26 | 39 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dzhambov, A.M.; Lercher, P. Road Traffic Noise Exposure and Birth Outcomes: An Updated Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 2522. https://doi.org/10.3390/ijerph16142522
Dzhambov AM, Lercher P. Road Traffic Noise Exposure and Birth Outcomes: An Updated Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2019; 16(14):2522. https://doi.org/10.3390/ijerph16142522
Chicago/Turabian StyleDzhambov, Angel M., and Peter Lercher. 2019. "Road Traffic Noise Exposure and Birth Outcomes: An Updated Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 16, no. 14: 2522. https://doi.org/10.3390/ijerph16142522
APA StyleDzhambov, A. M., & Lercher, P. (2019). Road Traffic Noise Exposure and Birth Outcomes: An Updated Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 16(14), 2522. https://doi.org/10.3390/ijerph16142522