A Correlational Analysis of the Relationships among Intolerance of Uncertainty, Anxiety Sensitivity, Subjective Sleep Quality, and Insomnia Symptoms

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Descriptive Analyses and Correlations
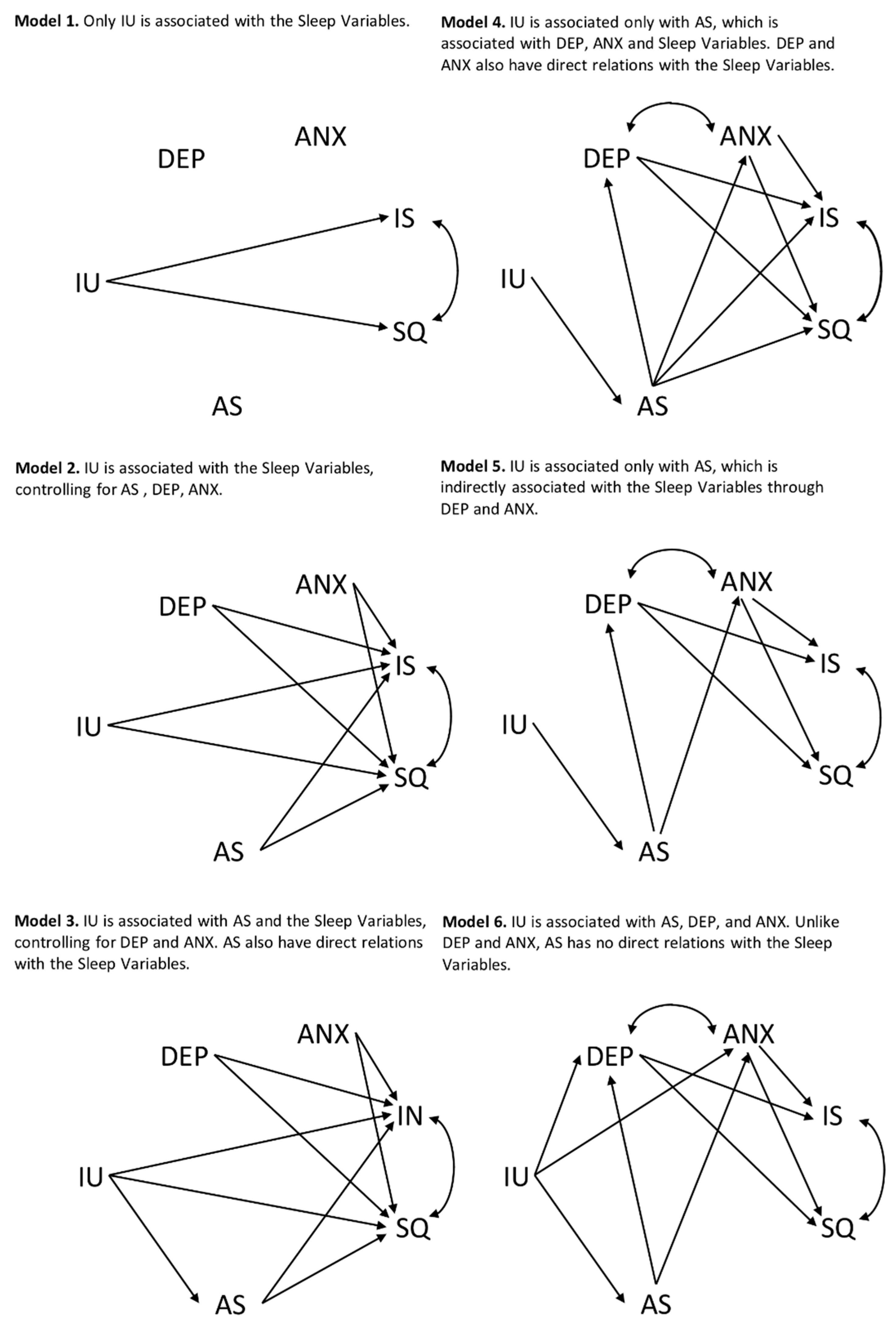
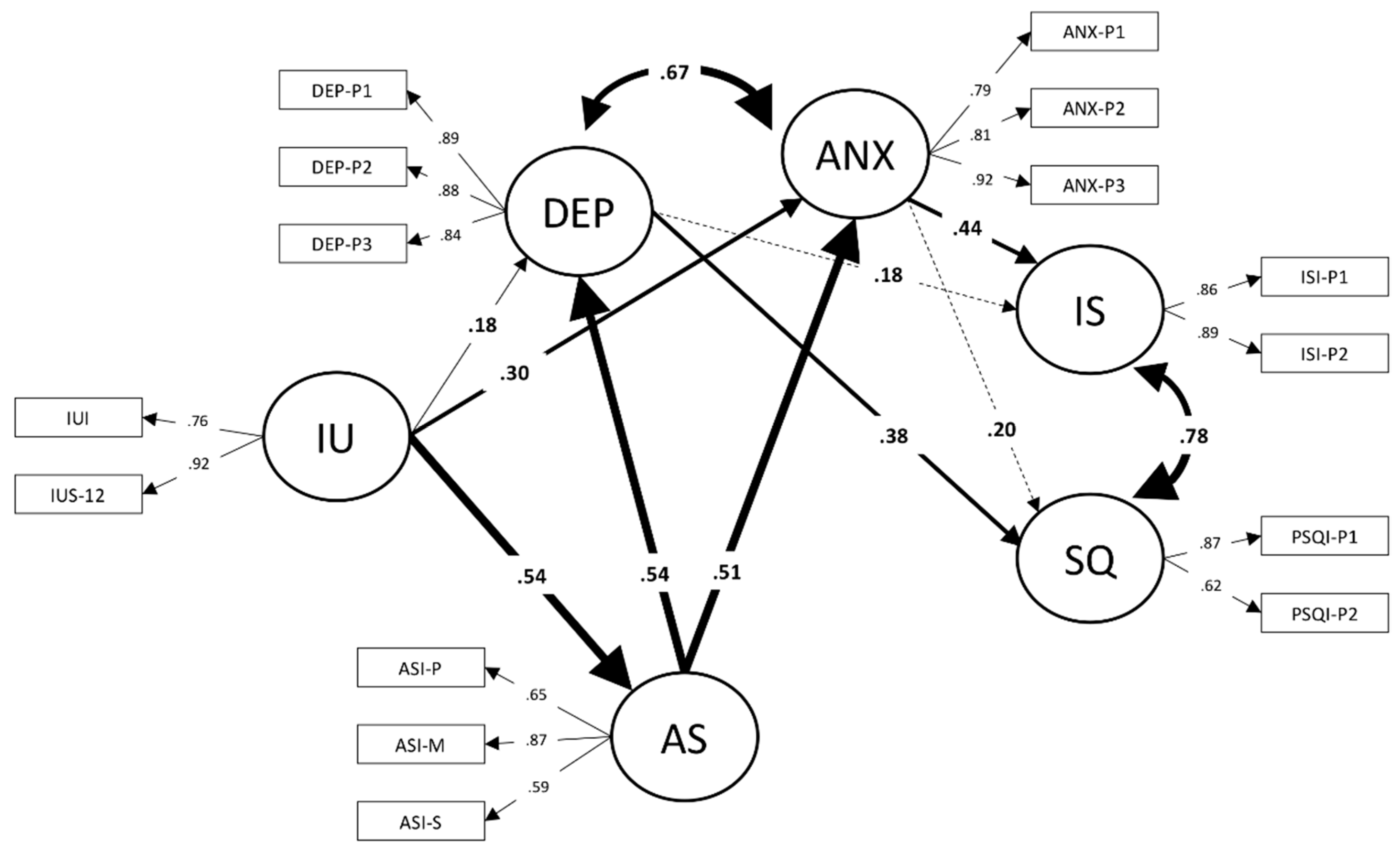
3.2. Structural Equations Modeling
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Domain | Parcel | Items | Parcel Mean | Parcel SD | PCA Eigenvalues | Items in the Parcel | Cronbach’s Alpha | Parcel-Domain Correlation * |
|---|---|---|---|---|---|---|---|---|
| BDI | 1 | 1, 4, 7, 10, 13, 16, 19 | 0.52 | 0.46 | 2.90; 0.86; 0.80; 0.75; 0.61; 0.59; 0.51 | 7 | 0.75 | 0.80 |
| 2 | 2, 5, 8, 11, 14, 17, 20 | 0.49 | 0.46 | 3.08; 0.86; 0.75; 0.68; 0.63; 0.54; 0.45 | 7 | 0.79 | 0.82 | |
| 3 | 3, 6, 9, 12, 15, 18, 21 | 0.40 | 0.38 | 2.67; 1.03; 0.85; 0.77; 0.63; 0.56; 0.49 | 7 | 0.72 | 0.80 | |
| STAI | 1 | 1R, 10R, 19R, 2, 5, 11, 15 | 2.03 | 0.49 | 2.85; 0.99; 0.92; 0.78; 0.71; 0.48; 0.23 | 7 | 0.73 | 0.79 |
| 2 | 7R, 13R, 3, 8, 12, 17, 20 | 2.16 | 0.60 | 3.23; 0.91; 0.89; 0.62; 0.49; 0.44; 0.43 | 7 | 0.82 | 0.78 | |
| 3 | 6R, 16R, 4, 9, 14, 18 | 2.22 | 0.55 | 2.41; 1.03; 0.92; 0.60; 0.56; 0.48 | 6 | 0.69 | 0.83 | |
| PSQI | 1 | 1, 3, 5, 7 | 1.01 | 0.70 | 1.71; 0.91; 0.81; 0.57 | 4 | 0.55 | 0.76 |
| 2 | 2, 4, 6 | 1.06 | 0.68 | 1.39, 0.84, 0.76 | 3 | 0.40 | 0.76 | |
| ISI | 1 | 1, 3, 5, 7 | 0.94 | 0.41 | 1.11; 0.82; 0.68; 0.38 | 4 | 0.68 | 0.47 |
| 2 | 2, 4, 6 | 0.74 | 0.50 | 1.77; 0.77; 0.46 | 3 | 0.65 | 0.47 |
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington DC, USA, 2013; ISBN 0-89042-555-8. [Google Scholar]
- Buboltz, W.C.; Brown, F.; Soper, B. Sleep habits and patterns of college students: A preliminary study. J. Am. Coll. Health 2001, 50, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Schlarb, A.A.; Kulessa, D.; Gulewitsch, M.D. Sleep characteristics, sleep problems, and associations of self-efficacy among German university students. Nat. Sci. Sleep 2012, 4, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lund, H.G.; Reider, B.D.; Whiting, A.B.; Prichard, J.R. Sleep Patterns and Predictors of Disturbed Sleep in a Large Population of College Students. J. Adolesc. Health 2010, 46, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Seun-Fadipe, C.T.; Mosaku, K.S. Sleep quality and psychological distress among undergraduate students of a Nigerian university. Sleep Health 2017, 3, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Peacey, V.; Wardle, J.; Population, S. Sleep Duration and Health in Young Adults. Arch. Intern. Med. 2006, 166, 1689–1692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curcio, G.; Ferrara, M.; De Gennaro, L. Sleep loss, learning capacity and academic performance. Sleep Med. Rev. 2006, 10, 323–337. [Google Scholar] [CrossRef] [PubMed]
- Farrer, L.M.; Gulliver, A.; Bennet, K.; Fassnacht, D.B.; Griffiths, K.M. Demographic and psychosocial predictors of major depression and generalised anxiety disorder in Australian university students. BMC Psychiatry 2016, 16, 241. [Google Scholar] [CrossRef]
- Kang, J.-H.; Chen, S.-C. Effects of an irregular bedtime schedule on sleep quality, daytime sleepiness, and fatigue among university students in Taiwan. BMC Public Health 2009, 9, 248. [Google Scholar] [CrossRef]
- Harvey, A. A Transdiagnostic Approach to Treating Sleep Disturbance in Psychiatric Disorders. Cogn. Behav. Ther. 2009, 38, 35–42. [Google Scholar] [CrossRef]
- Taylor, D.J.; Lichstein, K.L.; Durrence, H.H. Insomnia as a health risk factor. Behav. Sleep Med. 2003, 1, 227–247. [Google Scholar] [CrossRef]
- Thompson, M.D.; Sakurai, T.; Rainero, I.; Maj, M.C.; Kukkonen, J.P. Orexin receptor multimerization versus functional interactions: Neuropharmacological implications for opioid and cannabinoid signalling and pharmacogenetics. Pharmaceuticals 2017, 10, 79. [Google Scholar] [CrossRef] [PubMed]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Jansson, M.; Linton, S.J. The role of anxiety and depression in the development of insomnia: Cross-sectional and prospective analyses. Psychol. Health 2006, 21, 383–397. [Google Scholar] [CrossRef]
- Morphy, H.; Dunn, K.M.; Lewis, M.; Boardman, H.F.; Croft, P.R. Epidemiology of insomnia: A longitudinal study in a UK population. Sleep 2007, 30, 274–280. [Google Scholar] [PubMed]
- Johnson, E.O.; Roth, T.; Breslau, N. The association of insomnia with anxiety disorders and depression: Exploration of the direction of risk. J. Psychiatr. Res. 2006, 40, 700–708. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Roth, T. Place of chronic insomnia in the course of depressive and anxiety disorders. PubMed Commons. J. Psychiatr. Res. 2003, 37, 9–15. [Google Scholar] [CrossRef]
- Jansson-Frojmark, M.; Lindblom, K. A bidirectional relationship between anxiety and depression, and insomnia? A prospective study in the general population. J. Psychosom. Res. 2008, 64, 443–449. [Google Scholar] [CrossRef]
- Alvaro, P.K.; Roberts, R.M.; Harris, J.K. A Systematic Review Assessing Bidirectionality between Sleep Disturbances, Anxiety, and Depression. Sleep 2013, 36, 1059–1068. [Google Scholar] [CrossRef]
- Harvey, A. A cognitive model of insomnia. Behav. Res. Ther. 2002, 40, 869–893. [Google Scholar] [CrossRef]
- Kaplan, K.A.; Talbot, L.S.; Harvey, A.G. Cognitive mechanisms in chronic insomnia: Processes and prospects. Sleep Med. Clin. 2009, 4, 541–548. [Google Scholar] [CrossRef]
- Carleton, R.N.; Sharpe, D.; Asmundson, G.J. Anxiety sensitivity and intolerance of uncertainty: Requisites of the fundamental fears? Behav. Res. Ther. 2007, 45, 2307–2316. [Google Scholar] [CrossRef] [PubMed]
- Greco, V.; Roger, D. Uncertainty, stress, and health. Personal. Individ. Differ. 2003, 34, 1057–1068. [Google Scholar] [CrossRef]
- Carleton, R.N. Into the unknown: A review and synthesis of contemporary models involving uncertainty. J. Anxiety Disord. 2016, 39, 30–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEvoy, P.M.; Erceg-Hurn, D.M. The search for universal transdiagnostic and trans-therapy change processes: Evidence for intolerance of uncertainty. J. Anxiety Disord. 2015, 41, 96–107. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Zvolensky, M.J.; Cox, B.J.; Deacon, B.J.; Heimberg, R.G.; Ledley, D.R.; Abramowitz, J.S.; Holaway, R.M.; Sandin, B.; Stewart, S.H.; et al. Robust dimensions of anxiety sensitivity: Development and initial validation of the Anxiety Sensitivity Index-3. Psychol. Assess. 2007, 19, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Ebesutani, C.; McLeish, A.C.; Luberto, C.M.; Young, J.; Maack, D.J. A Bifactor Model of Anxiety Sensitivity: Analysis of the Anxiety Sensitivity Index-3. J. Psychopathol. Behav. Assess. 2013, 36, 452–464. [Google Scholar] [CrossRef]
- Ghisi, M.; Bottesi, G.; Altoe, G.; Razzetti, E.; Melli, G.; Sica, C. Factor structure and psychometric properties of the anxiety sensitivity index-3 in an Italian community sample. Front. Psychol. 2016, 7, 160. [Google Scholar] [CrossRef]
- Fergus, T.A.; Bardeen, J.R. Anxiety sensitivity and intolerance of uncertainty: Evidence of incremental specificity in relation to health anxiety. Personal. Individ. Differ. 2013, 55, 640–644. [Google Scholar] [CrossRef]
- Sabouri, S.; Gerber, M.; Lemola, S.; Becker, S.P.; Shamsi, M.; Shakouri, Z.; Sadeghi Bahmani, D.; Kalak, N.; Holsboer-Trachsler, E.; Brand, S. Examining Dark Triad traits in relation to sleep disturbances, anxiety sensitivity and intolerance of uncertainty in young adults. Compr. Psychiatry 2016, 68, 103–110. [Google Scholar] [CrossRef]
- Hoge, E.; Bui, E.; Goetter, E.; Robinaugh, D.; Ojserkis, R.A.; Fresco, D.M.; Simon, N.M. Change in decentering mediates improvement in anxiety in mindfulness-based stress reduction for generalized anxiety disorder. Cogn. Ther. 2015, 39, 228–235. [Google Scholar] [CrossRef]
- Leyro, T.; Babson, K.; Bonn-Miller, M.O. Anxiety sensitivity in relation to sleep quality among HIV-infected individuals. J. Assoc. Nurses AIDS Care 2014, 25, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.; Choi, H.; Lim, S.; Oh, K. The Relationship between Insomnia Severity and Depression, Anxiety and Anxiety Sensitivity in General Population. Sleep Med. Psychophysiol. 2006, 13, 59–66. [Google Scholar]
- Calkins, A.W.; Hearon, B.A.; Capozzoli, M.C.; Otto, M.W. Psychosocial Predictors of Sleep Dysfunction: The Role of Anxiety Sensitivity, Dysfunctional Beliefs, and Neuroticism. Behav. Sleep Med. 2013, 11, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.-M.; Xie, S.-S.; Yan, Y.-W.; Yan, W.-J. Intolerance of uncertainty and adolescent sleep quality: The mediating role of worry. Personal. Individ. Differ. 2017, 108, 168–173. [Google Scholar] [CrossRef]
- Riemann, D.; Spiegelhalder, K.; Feige, B.; Voderholzer, U.; Berger, M.; Perlis, M.; Nissen, C. The hyperarousal model of insomnia: A review of the concept and its evidence. Sleep Med. Rev. 2010, 14, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Carleton, R.N. Fear of the unknown: One fear to rule them all? J. Anxiety Disord. 2016, 41, 5–21. [Google Scholar] [CrossRef] [Green Version]
- Shihata, S.; McEvoy, P.M.; Mullan, B.A.; Carleton, R.N. Intolerance of uncertainty in emotional disorders: What uncertainties remain? J. Anxiety Disord. 2016, 41, 115–124. [Google Scholar] [CrossRef] [Green Version]
- Hong, R.Y.; Cheung, M.W.L. The structure of cognitive vulnerabilities to depression and anxiety: Evidence for a common core etiologic process based on a meta-analytic review. Clin. Psychol. Sci. 2015, 3, 892–912. [Google Scholar] [CrossRef]
- Lauriola, M.; Mosca, O.; Carleton, R.N. Hierarchical factor structure of the Intolerance of Uncertainty Scale short form (IUS-12) in the Italian version. TPM-Test. Psychom. Methodol. Appl. Psychol. 2016, 23, 377–394. [Google Scholar]
- Lauriola, M.; Mosca, O.; Trentini, C.; Foschi, R.; Tambelli, R.; Carleton, R.N. The intolerance of uncertainty inventory: Validity and comparison of scoring methods to assess individuals screening positive for anxiety and depression. Front. Psychol. 2018, 9, 388. [Google Scholar] [CrossRef]
- Ghisi, M.; Flebus, G.; Montano, A.; Sanavio, E.; Sica, C. Beck Depression Inventory-II: Edizione Italiana; Firenze Giunti: Florence, Italy, 2006. [Google Scholar]
- Pedrabissi, L.; Santinello, M. Inventario per L’ansia di «Stato» e di «Tratto»: Nuova Versione Italiana Dello STAI Forma Y: Manuale; Organ Specification: Firenze, Italy, 1989; p. 44. [Google Scholar]
- Fisher, P.L.; Durham, R.C. Recovery rates in generalized anxiety disorder following psychological therapy: An analysis of clinically significant change in the {STAI}-{T} across outcome studies since 1990. Psychol. Med. 1999, 29, 1425–1434. [Google Scholar] [CrossRef] [PubMed]
- Curcio, G.; Tempesta, D.; Scarlata, S.; Marzano, C.; Moroni, F.; Rossini, P.M.; Ferrara, M.; De Gennaro, L. Validity of the Italian Version of the Pittsburgh Sleep Quality Index (PSQI). Neurol. Sci. 2013, 34, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Castronovo, V.; Galbiati, A.; Marelli, S.; Brombin, C.; Cugnata, F.; Giarolli, L.; Anelli, M.M.; Rinaldi, F.; Ferini-Strambi, L. Validation study of the Italian version of the Insomnia Severity Index (ISI). Neurol. Sci. 2016, 37, 1517–1524. [Google Scholar] [CrossRef] [PubMed]
- Macho, S.; Ledermann, T. Estimating, Testing, and Comparing Specific Effects in Structural Equation Models: The Phantom Model Approach. Psychol. Methods 2011, 16, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Little, T.D.; Cunningham, W.A.; Shahar, G.; Widaman, K.F. To parcel or not to parcel: Exploring the question, weighing the merits. Struct. Equ. Model. Multidiscip. J. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Satorra, A.; Bentler, P.M. A scaled difference chi-square test statistic for moment structure analysis. Psychometrika 2001, 66, 507–514. [Google Scholar] [CrossRef] [Green Version]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Bryant, F.B.; Satorra, A. Principles and Practice of Scaled Difference Chi-Square Testing. Struct. Equ. Model. Multidiscip. J. 2012, 19, 372–398. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA, 2012; Volume 3, ISBN 978-1-60623-876-9. [Google Scholar]
- Maassen, G.H.; Bakker, A.B. Suppressor Variables in Path Models: Definitions and Interpretations. Sociol. Methods Res. 2001, 30, 241–270. [Google Scholar] [CrossRef]
- Alamir, Y.A.; Zullig, K.J.; Wen, S.; Montgomery-Downs, H.; Kristjansson, A.L.; Misra, R.; Zhang, J. Association Between Nonmedical Use of Prescription Drugs and Sleep Quality in a Large College Student Sample. Behav. Sleep Med. 2019, 17, 470–480. [Google Scholar] [CrossRef]
- Smith, M.T.; Wegener, S.T. Measures of sleep: The Insomnia Severity Index, Medical Outcomes Study (MOS) Sleep Scale, Pittsburgh Sleep Diary (PSD), and Pittsburgh Sleep Quality Index (PSQI). Arthritis Rheum. 2003, 49, S184–S196. [Google Scholar] [CrossRef]
- Coveney, C.M. Managing sleep and wakefulness in a 24-hour world. Sociol. Health Illn. 2014, 36, 123–136. [Google Scholar] [CrossRef] [PubMed]
- Saulnier, K.G.; Allan, N.P.; Raines, A.M.; Schmidt, N.B. Anxiety sensitivity cognitive concerns drive the relation between anxiety sensitivity and symptoms of depression. Cogn. Behav. Ther. 2018, 47, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Olthuis, J.V.; Watt, M.C.; Stewart, S.H. Anxiety Sensitivity Index (ASI-3) subscales predict unique variance in anxiety and depressive symptoms. J. Anxiety Disord. 2014, 28, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Edéll-Gustafsson, U.; Carstensen, J.; Regestein, Q.; Swahn, E.; Svanborg, E. Hyperarousal, depression and quality of life—Validity and reliability of the Swedish version of the Hyperarousal Scale. Scand. J. Caring Sci. 2006, 20, 58–67. [Google Scholar] [CrossRef] [PubMed]
- Krystal, A.D. Psychiatric Disorders and Sleep. Neurol. Clin. 2012, 30, 1389–1413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tull, M.T.; Gratz, K.L. Further examination of the relationship between anxiety sensitivity and depression: The mediating role of experiential avoidance and difficulties engaging in goal-directed behavior when distressed. J. Anxiety Disord. 2008, 22, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Balsamo, M.; Lauriola, M.; Saggino, A. Work values and college major choice. Learn. Individ. Differ. 2013, 24, 110–116. [Google Scholar] [CrossRef]
- Dugas, M.J.; Robichaud, M. Cognitive-Behavioral Treatment for Generalized Anxiety Disorder: From Science to Practice; Routledge: New York, NY, USA, 2012; ISBN 1135928355. [Google Scholar]
- Stewart, S.; Watt, M. Overcoming the Fear of Fear: How to Reduce Anxiety Sensitivity; New Harbinger Publications: Oakland, CA, USA, 2007. [Google Scholar]


| Variables | M | SD | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Intolerance of Uncertainty (IUS-12) | 27.70 | 8.63 | 1 | |||||||
| 2. Intolerance of Uncertainty (IUI-A) | 25.90 | 8.08 | 0.70 *** | 1 | ||||||
| 3. Anxiety Sensitivity Physical (ASI-3) | 4.06 | 4.61 | 0.27 *** | 0.30 *** | 1 | |||||
| 4. Anxiety Sensitivity Social (ASI-3) | 6.87 | 4.84 | 0.33 *** | 0.31 *** | 0.43 *** | 1 | ||||
| 5. Anxiety Sensitivity Mental (ASI-3) | 4.26 | 4.22 | 0.43 *** | 0.35 *** | 0.57 *** | 0.50 *** | 1 | |||
| 6. Depression (BDI-II) | 9.86 | 8.30 | 0.41 *** | 0.35 *** | 0.38 *** | 0.34 *** | 0.53 *** | 1 | ||
| 7. Trait Anxiety (STAI-Y) | 40.12 | 9.29 | 0.50 *** | 0.40 *** | 0.40 *** | 0.37 *** | 0.57 *** | 0.73 *** | 1 | |
| 8. Sleep Quality (PSQI) | 6.00 | 2.74 | 0.06 | 0.03 | 0.18 ** | 0.11 | 0.21 *** | 0.42 *** | 0.41 *** | 1 |
| 9. Insomnia Severity (ISI) | 7.14 | 4.51 | 0.22 *** | 0.19 *** | 0.24 *** | 0.15 *** | 0.33 *** | 0.48 *** | 0.51 *** | 0.67 *** |
| Model | ML χ2 | DF | MLR χ2 | NNFI * | CFI * | SRMR | RMSEA * | 95% CI | AIC * | CAIC * |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 714.56 | 87 | 612.88 | 0.638 | 0.697 | 0.323 | 0.142 | 0.131–0.153 | 438.9 | 29.7 |
| 2 | 601.35 | 81 | 521.00 | 0.672 | 0.747 | 0.290 | 0.135 | 0.124–0.146 | 359.0 | −22.0 |
| 3 | 534.56 | 80 | 468.41 | 0.707 | 0.777 | 0.283 | 0.127 | 0.116–0.138 | 308.4 | −67.9 |
| 4 | 164.84 | 79 | 149.88 | 0.946 | 0.959 | 0.050 | 0.055 | 0.041–0.068 | −8.1 | −379.7 |
| 5 | 169.29 | 81 | 153.91 | 0.946 | 0.958 | 0.056 | 0.055 | 0.041–0.068 | −8.1 | −389.1 |
| 6 | 150.16 | 79 | 138.17 | 0.955 | 0.966 | 0.050 | 0.050 | 0.036–0.063 | −19.8 | −391.4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lauriola, M.; Carleton, R.N.; Tempesta, D.; Calanna, P.; Socci, V.; Mosca, O.; Salfi, F.; De Gennaro, L.; Ferrara, M. A Correlational Analysis of the Relationships among Intolerance of Uncertainty, Anxiety Sensitivity, Subjective Sleep Quality, and Insomnia Symptoms. Int. J. Environ. Res. Public Health 2019, 16, 3253. https://doi.org/10.3390/ijerph16183253
Lauriola M, Carleton RN, Tempesta D, Calanna P, Socci V, Mosca O, Salfi F, De Gennaro L, Ferrara M. A Correlational Analysis of the Relationships among Intolerance of Uncertainty, Anxiety Sensitivity, Subjective Sleep Quality, and Insomnia Symptoms. International Journal of Environmental Research and Public Health. 2019; 16(18):3253. https://doi.org/10.3390/ijerph16183253
Chicago/Turabian StyleLauriola, Marco, R. Nicholas Carleton, Daniela Tempesta, Pierpaolo Calanna, Valentina Socci, Oriana Mosca, Federico Salfi, Luigi De Gennaro, and Michele Ferrara. 2019. "A Correlational Analysis of the Relationships among Intolerance of Uncertainty, Anxiety Sensitivity, Subjective Sleep Quality, and Insomnia Symptoms" International Journal of Environmental Research and Public Health 16, no. 18: 3253. https://doi.org/10.3390/ijerph16183253
APA StyleLauriola, M., Carleton, R. N., Tempesta, D., Calanna, P., Socci, V., Mosca, O., Salfi, F., De Gennaro, L., & Ferrara, M. (2019). A Correlational Analysis of the Relationships among Intolerance of Uncertainty, Anxiety Sensitivity, Subjective Sleep Quality, and Insomnia Symptoms. International Journal of Environmental Research and Public Health, 16(18), 3253. https://doi.org/10.3390/ijerph16183253