The Hardness of Drinking Water Negatively while Socio-Economic Deprivation Positively Correlate with the Age-Adjusted Mortality Rates due to Cardiovascular Diseases in Hungarian Wine Regions


Abstract
:1. Introduction
The Dominant Types of Wines and the Settlements of Territories
2. Methods
2.1. Age-Adjusted Death Rate
2.2. The Measurement of the Indicators of Hardness of Drinking Water
2.3. Calculation of the Index of Socio-Economic Deprivation (ID)
2.4. Statistical Analysis
3. Results
3.1. The Number of Population, Age-Adjusted Death Rates Due to Cardiovascular Diseases, the Hardness of Drinking Water and Index of Deprivation in the Five Regions Between 2000 and 2010
3.2. The Indicators of Hardness of Drinking Water in the Five Territories
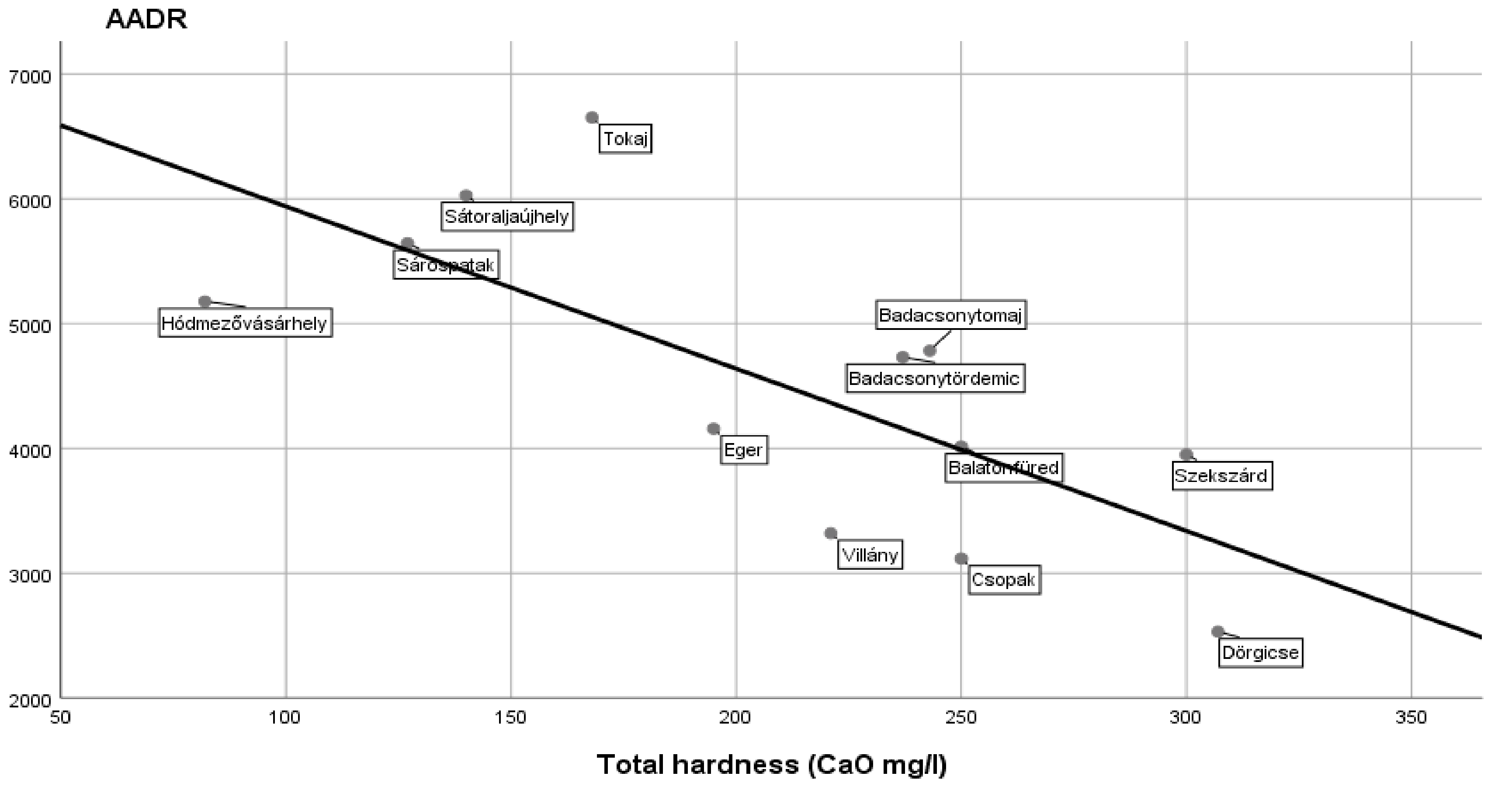
3.3. A Negative Correlation between the AADR Values Due to Cardiovascular Diseases and Total Hardness of Drinking Water in the Five Regions in a Population Larger than 200,000 Persons
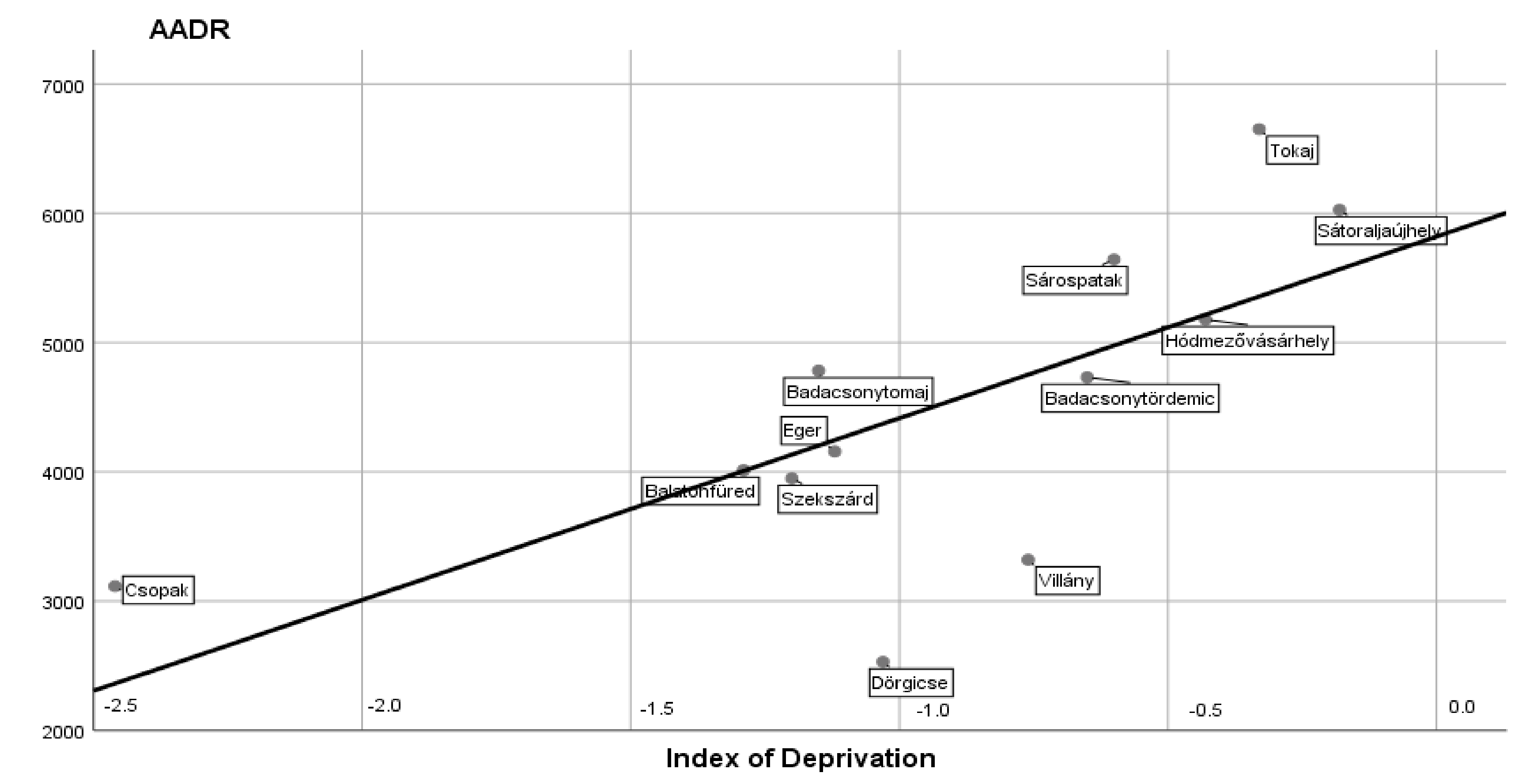
3.4. A Positive Correlation between the AADR Values Due to Cardiovascular Diseases and Indices of Socio-Economic Deprivation in the Five Regions in a Population Larger than 200,000 Persons
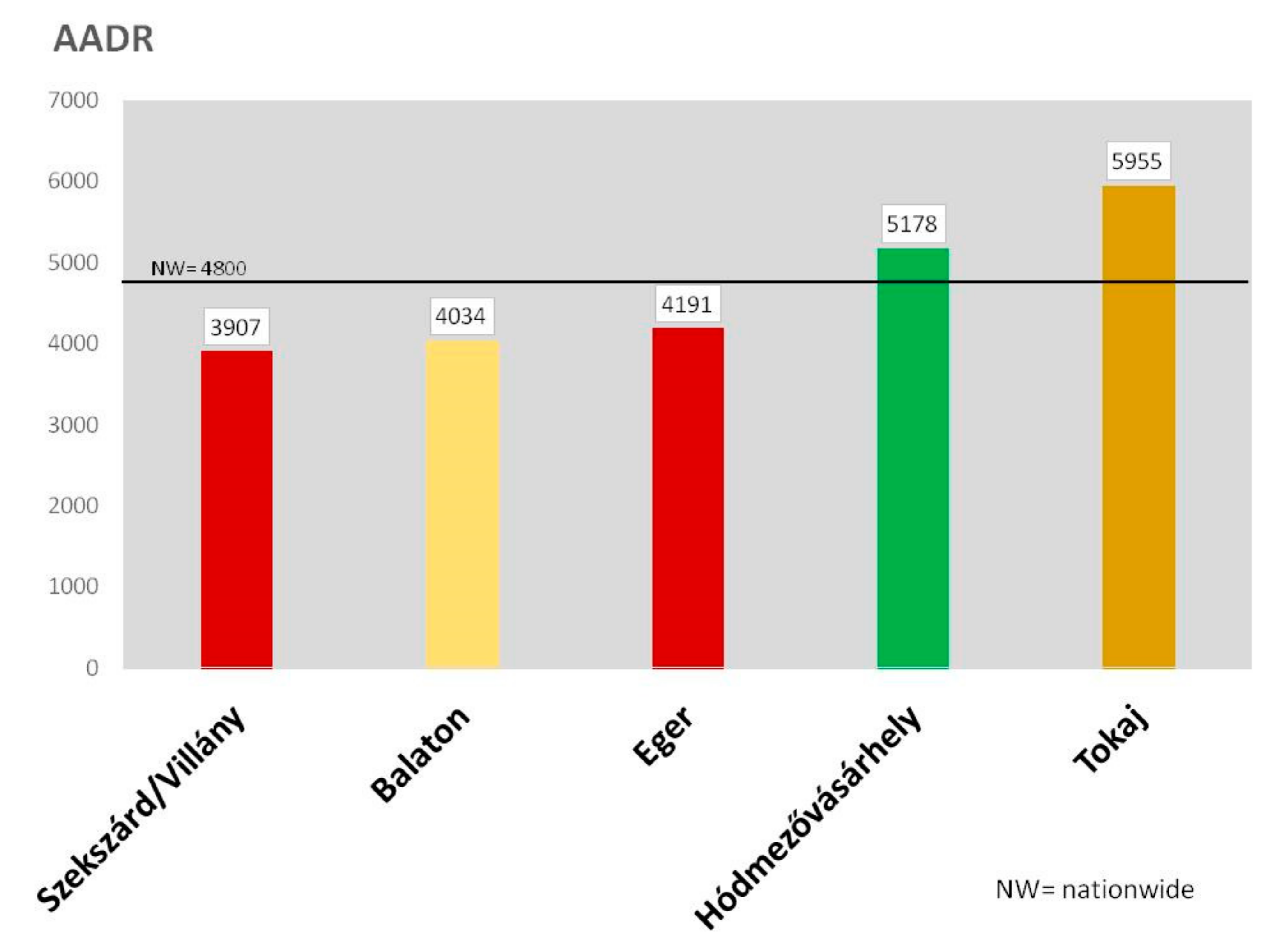
3.5. The AADR Values Due to Cardiovascular Diseases Presented from the Aspect of “Red” or “White” Dominant Types of Wines in the Regions
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- European Commission. Eurostat. Products Eurostat News. Causes and Occurrence of Deaths in the EU. 2019. Available online: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/DDN-20190716-1 (accessed on 31 July 2019).
- Ford, M.M.; Highfield, L.D. Exploring the spatial association between social deprivation and cardiovascular disease mortality at the neighborhood level. PLoS ONE 2016, 11, e0146085. [Google Scholar] [CrossRef] [PubMed]
- Riccioni, G.; Speranzy, L.; Pesce, M.; Cusenza, S.; D’ Orazio, N.; Glade, M.J. Novel phytonutrient contributors to antioxidant protection against cardiovascular disease. Nutrition 2012, 28, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Van Bussel, B.C.T.; Henry, R.M.A.; Schalkwijk, C.; Dekker, J.M.; Nijjzels, G.; Feskens, E.J.M.; Stehouwere, C.D.A. Alcohol and red wine consumption, but not fruit, vegetables, fish or dairy products are associated with less endothelial dysfunction and less low-grade inflammation: the Hoorn Study. Eur. J. Nutr. 2018, 57, 1409–1419. [Google Scholar] [CrossRef] [PubMed]
- Rubenowitz, E.; Axelsson, G.; Rylander, R. Magnesium and calcium in drinking water and death from acute myocardial infarction in women. Epidemiology 1999, 10, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Gianfredi, V.; Bragazzi, N.L.; Nucci, D.; Villarini, M.; Moretti, M. Cardiovascular diseases and hard drinking waters: Implications from a systemic review with meta-analysis of case-control studies. J. Water Health 2017, 15, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Rapant, S.; Fajciková, K.; Cvecková, V.; Durza, A.; Stehliková, D.; Zenisová, Z. Chemical composition of groundwater and relative mortality for cardiovascular diseases in the Slovak Republic. Environ. Geochem. Health 2015, 37, 745–756. [Google Scholar] [CrossRef] [PubMed]
- Rapant, S.; Cvecková, V.; Fajcikivá, K.; Hajdúk, I.; Hiller, E.; Stehliková, B. Hard water, more elastic arteries: A Case Study from Krupina District, Slovakia. Int. J. Environ. Res. Public Health 2019, 16, 1521. [Google Scholar] [CrossRef] [PubMed]
- Széles, G.; Vokó, Z.; Jenei, T.; Kardos, L.; Pocsai, Zs.; Bajtay, A. A preliminary evaluation of health monitoring program in Hungary. Eur. J. Public Health 2005, 15, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Juhász, A.; Nagy, C.; Páldy, A.; Beale, L. Development of Deprivation Index and its relation to premature mortality due to diseases of the circulatory system in Hungary, 1998-2004. Soc. Sci. Med. 2010, 70, 1342–1349. [Google Scholar] [CrossRef] [PubMed]
- Elekes, Zs.; Paksi, B. Drinking Customs of the Hungarian Population 1994. Available online: https://nfsz.munka.hu/Lapok/archivum_programok/mhelyi_alk_es_drogm/alkdrogprev_mellekletek/content/alkdrogprev_mellekletek_20.doc (accessed on 31 July 2019).
- Murányi, Z. New Results on the Trace Element Contents of Wines. Ph.D. Thesis, Hungarian University of Debrecen, Debrecen, Hungary, March 2002. [Google Scholar]
- Poursafa, P.; Kelishadi, R.; Amin, M.M.; Hashemi, M.; Amin, M. First report on the association of drinking water hardness and endothelial function in children and adolescents. Arch. Med. Sci. 2014, 29, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Wodschow, K.; Hansen, B.; Schullehner, J.; Ersball, A.K. Stability of major geogenic cations in drinking water—an issue of public health importance. A Danish study, 1980–2017. Int. J. Environ. Res. Public Health 2018, 15, 1212. [Google Scholar] [CrossRef] [PubMed]
- Klevay, L.M. Some bottled water may be salubrious. J. Trace Elem. Med. Biol. 2018, 48, 188–189. [Google Scholar] [CrossRef] [PubMed]
- Toxqui, L.; Vaquer, M.P. An intervention with mineral water decreases cardio-metabolic risk biomarkers. A crossover, randomized, controlled trial with two mineral waters in moderately hypercholesterolaemic adults. Nutrients 2016, 7, E400. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Tokaj | Eger | Balaton | Szekszárd/Villány | Hódmezővásárhely |
|---|---|---|---|---|---|
| Population | 33,917 | 56,981 | 30,833 | 37,268 | 47,160 |
| Cardiovascular mortality (AADR) | 5955 | 4191 | 4034 | 3907 | 5178 |
| Drinking water total hardness (CaO mg/L) | 138.60 | 194.90 | 249.20 | 294.20 | 81.90 |
| Index of deprivation | −0.36 | −1.1 | −1.22 | −1.17 | −0.43 |
| Element/Compound | Unit | Tokaj | Eger | Balaton | Szekszárd/Villány | Hódmező-Vásárhely |
|---|---|---|---|---|---|---|
| Magnesium | mg/L | 24.50 | 26.80 | 46.20 | 39.70 | 14.50 |
| Average ± SD | ± 4.4 | ± 5.3 | ± 5.1 | ± 6.2 | ± 7.7 | |
| Calcium | mg/L | 2.40 | 86.20 | 115.40 | 8.20 | 27.60 |
| Average ± SD | ± 0.35 | ± 1.13 | ± 17.6 | ± 7.8 | ± 15.1 | |
| Total hardness | CaO mg/L | 138.60 | 194.90 | 249.20 | 294.20 | 81.90 |
| Average ± SD | ± 31.3 | ± 30.8 | ± 33.7 | ± 40.6 | ± 37.3 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagy, J.; Sipka, S.; Sipka, S., Jr.; Kocsis, J.; Horváth, Z. The Hardness of Drinking Water Negatively while Socio-Economic Deprivation Positively Correlate with the Age-Adjusted Mortality Rates due to Cardiovascular Diseases in Hungarian Wine Regions. Int. J. Environ. Res. Public Health 2019, 16, 3437. https://doi.org/10.3390/ijerph16183437
Nagy J, Sipka S, Sipka S Jr., Kocsis J, Horváth Z. The Hardness of Drinking Water Negatively while Socio-Economic Deprivation Positively Correlate with the Age-Adjusted Mortality Rates due to Cardiovascular Diseases in Hungarian Wine Regions. International Journal of Environmental Research and Public Health. 2019; 16(18):3437. https://doi.org/10.3390/ijerph16183437
Chicago/Turabian StyleNagy, János, Sándor Sipka, Sándor Sipka, Jr., Judit Kocsis, and Zsolt Horváth. 2019. "The Hardness of Drinking Water Negatively while Socio-Economic Deprivation Positively Correlate with the Age-Adjusted Mortality Rates due to Cardiovascular Diseases in Hungarian Wine Regions" International Journal of Environmental Research and Public Health 16, no. 18: 3437. https://doi.org/10.3390/ijerph16183437
APA StyleNagy, J., Sipka, S., Sipka, S., Jr., Kocsis, J., & Horváth, Z. (2019). The Hardness of Drinking Water Negatively while Socio-Economic Deprivation Positively Correlate with the Age-Adjusted Mortality Rates due to Cardiovascular Diseases in Hungarian Wine Regions. International Journal of Environmental Research and Public Health, 16(18), 3437. https://doi.org/10.3390/ijerph16183437