Occurrence of Cortical Arousal at Recovery from Respiratory Disturbances during Deep Propofol Sedation

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approval and Study Subjects
2.2. Data Collection
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics, Details of the Sedation, and Frequency of Respiratory Disturbances
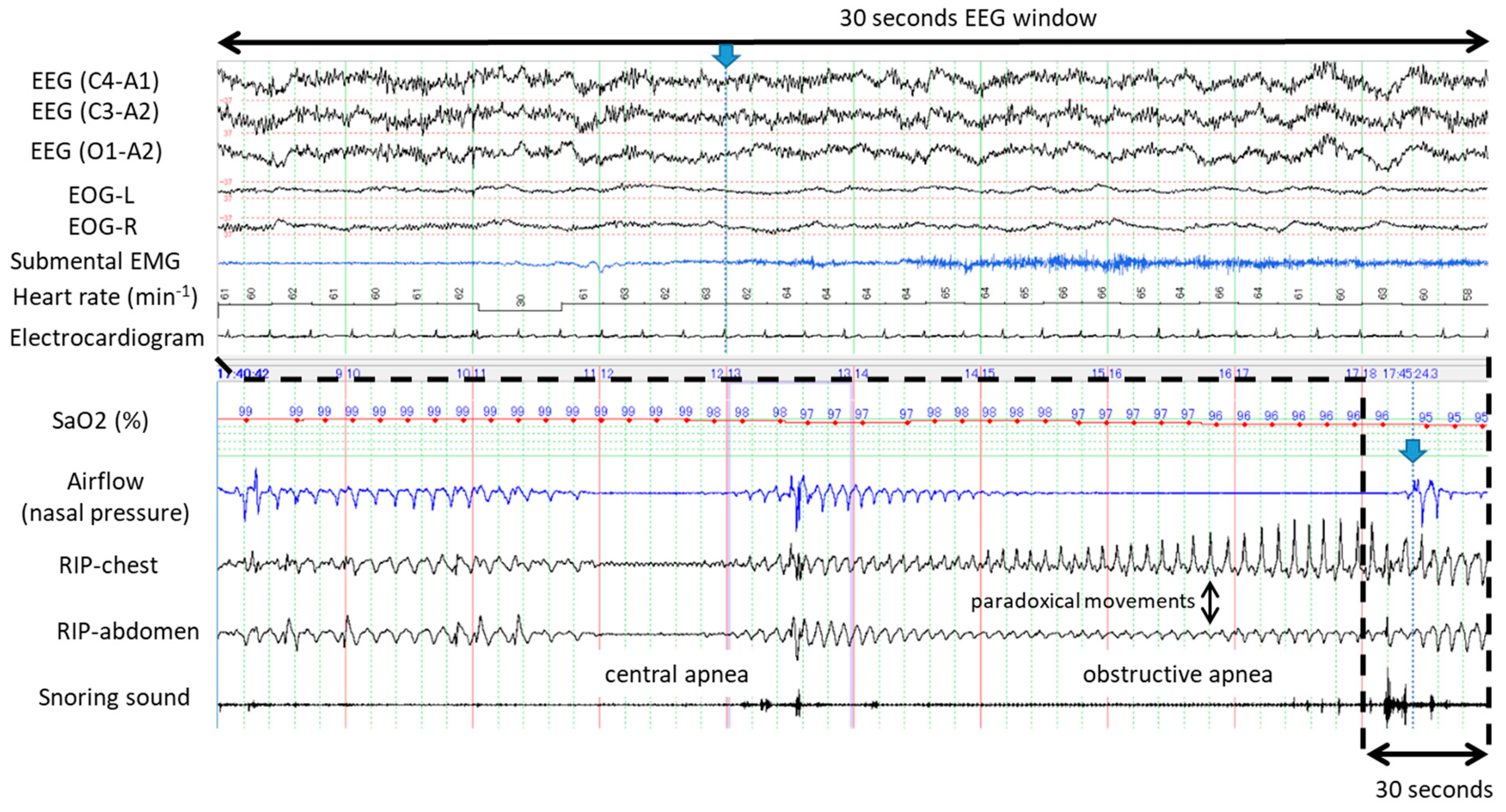
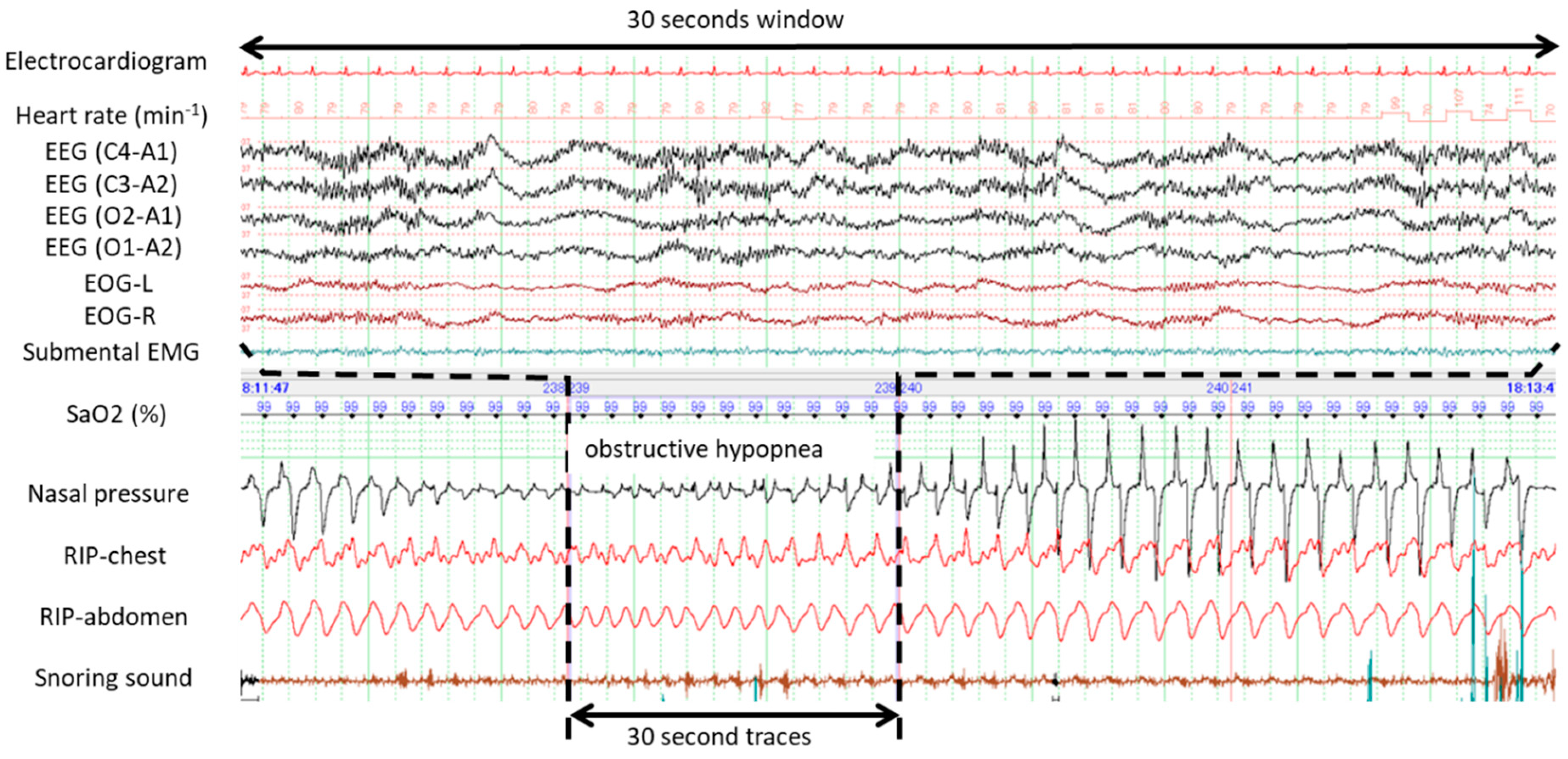
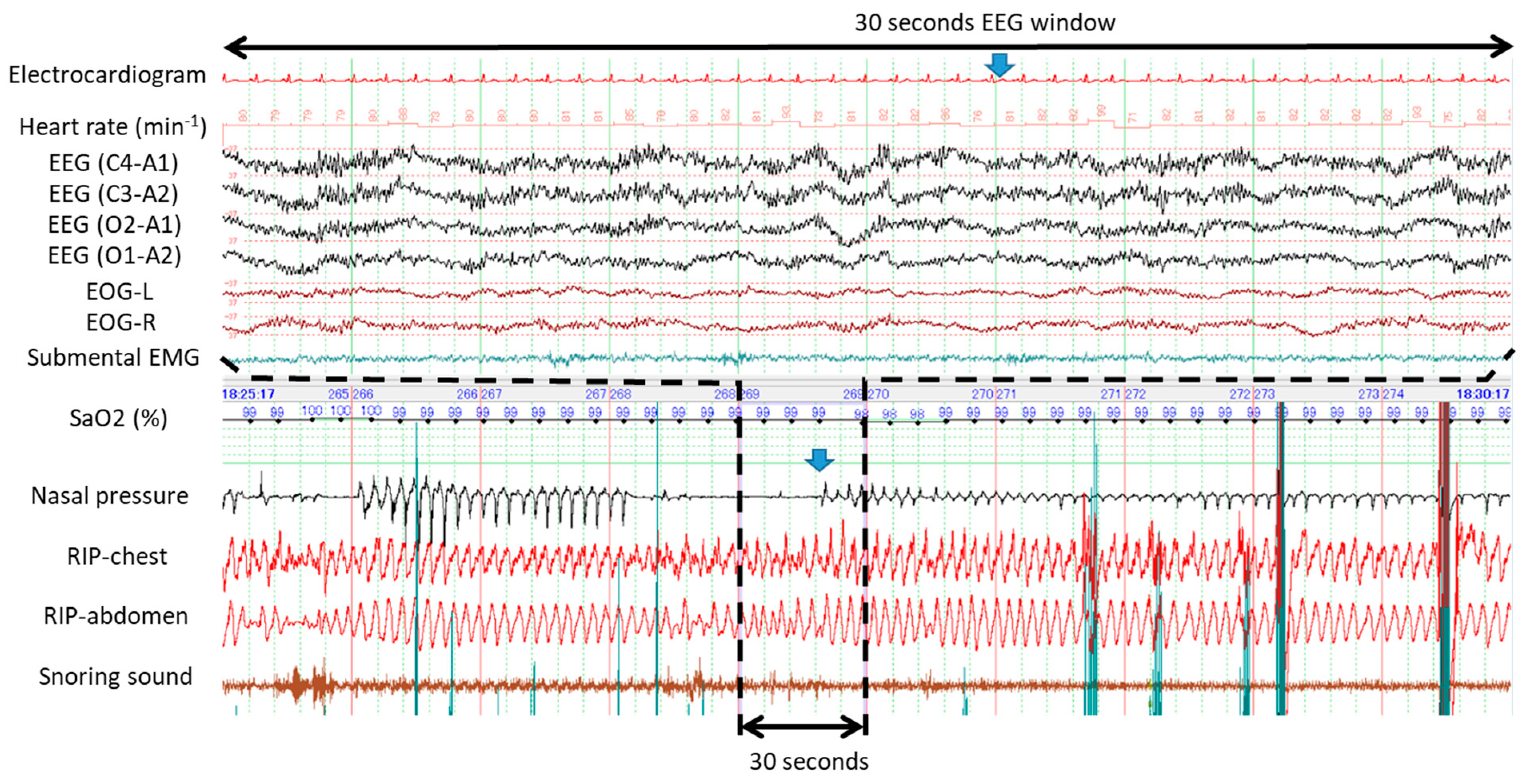
3.2. Typical Examples of Apneas and Hypopneas Without Cortical Arousal during Propofol-Induced Sleep
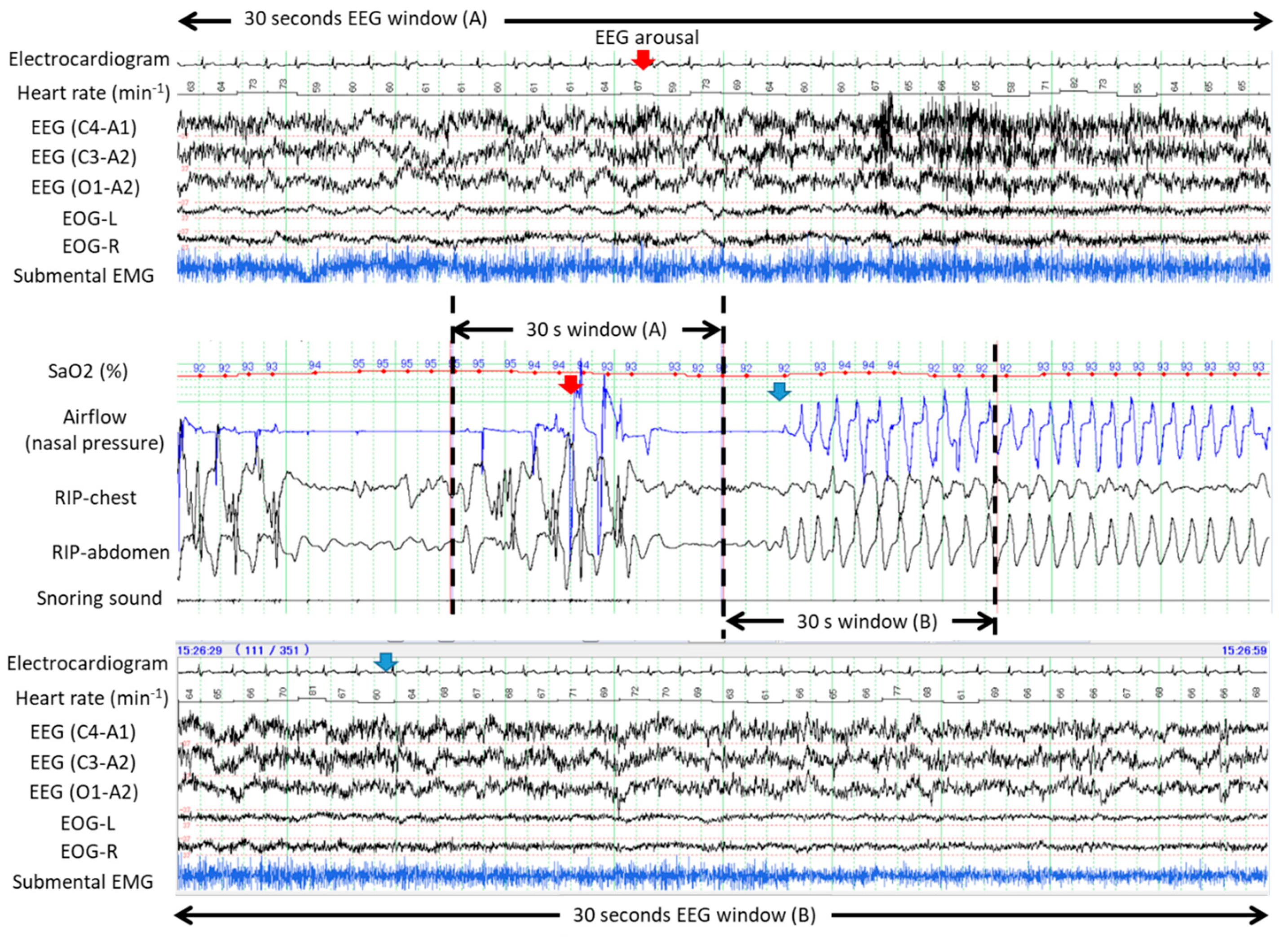
3.3. Arousal in Response to Apneas and Hypopneas with and without Desaturation
4. Discussion
4.1. Possible Mechanisms and Consequences of Spontaneous Recovery from Apnea and Hypopnea without Cortical Arousal during Propofol Sedation
4.2. Limitations of this Study
4.3. Clinical Implications of the Results of this Study
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Remmers, J.E.; de Groot, W.J.; Sauerland, E.K.; Anch, A.M. Pathogenesis of upper airway occlusion during sleep. J. Appl. Physiol. 1978, 44, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Phillipson, E.A.; Sullivan, C.E. Arousal: The forgotten response to respiratory stimuli. Am. Rev. Respir. Dis. 1978, 118, 807–809. [Google Scholar] [PubMed]
- McNamara, F.; Issa, F.G.; Sullivan, C.E. Arousal pattern following central and obstructive breathing abnormalities in infants and children. J. Appl. Physiol. 1996, 81, 2651–2657. [Google Scholar] [CrossRef] [PubMed]
- Younes, M. Role of arousals in the pathogenesis of obstructive sleep apnea. Am. J. Respir. Crit. Care. Med. 2004, 169, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Younes, M.; Loewen, A.H.; Ostrowski, M.; Laprairie, J.; Maturino, F.; Hanly, P.J. Genioglossus activity available via non-arousal mechanisms vs. that required for opening the airway in obstructive apnea patients. J. Appl. Physiol. 2012, 112, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Eckert, D.J.; Younes, M.K. Arousal from sleep: Implications for obstructive sleep apnea pathogenesis and treatment. J. Appl. Physiol. 2014, 116, 302–313. [Google Scholar] [CrossRef] [PubMed]
- Younes, M.; Park, E.; Horner, R.L. Pentobarbital sedation increases genioglossus respiratory activity in sleeping rats. Sleep 2007, 30, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Eckert, D.J.; Owens, R.L.; Kehlmann, G.B.; Wellman, A.; Rahangdale, S.; Yim-Yeh, S.; White, D.P.; Malhotra, A. Eszopiclone increases the respiratory arousal threshold and lowers the apnoea/hypopnoea index in obstructive sleep apnoea patients with a low arousal threshold. Clin. Sci. (Lond.) 2011, 120, 505–514. [Google Scholar] [CrossRef] [Green Version]
- Eikermann, M.; Fassbender, P.; Zaremba, S.; Jordan, A.S.; Rosow, C.; Malhotra, A.; Chamberlin, N.L. Pentobarbital dose-dependently increases respiratory genioglossus muscle activity while impairing diaphragmatic function in anesthetized rats. Anesthesiology 2009, 110, 1327–1334. [Google Scholar] [CrossRef]
- Urahama, R.; Uesato, M.; Aikawa, M.; Yamaguchi, Y.; Hayano, K.; Matsumura, T.; Arai, M.; Kunii, R.; Isono, S.; Matsubara, H. Polysomnographic assessment of respiratory disturbance during deep propofol sedation for endoscopic submucosal dissection of gastric tumors. World. J. Gastrointest. Endosc. 2018, 10, 340–347. [Google Scholar] [CrossRef]
- Ramsay, M.A.; Savege, T.M.; Simpson, B.R.; Goodwin, R. Controlled sedation with alphaxalone-alphadolone. Br. Med. J. 1974, 2, 656–659. [Google Scholar] [CrossRef] [PubMed]
- Rechtschaffen, A.; Kales, A. A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects; National Health Institute: Washington, DC, USA, 1968. [Google Scholar]
- Eichhorn, V.; Henzler, D.; Murphy, M.F. Standardizing care and monitoring for anesthesia or procedural sedation delivered outside the operating room. Curr. Opin. Anaesthesiol. 2010, 23, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Blouin, R.T.; Seifert, H.A.; Babenco, H.D.; Conard, P.F.; Gross, J.B. Propofol depresses the hypoxic ventilatory response during conscious sedation and isohypercapnia. Anesthesiology 1993, 79, 1177–1182. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuijs, D.; Sarton, E.; Teppema, L.J.; Kruyt, E.; Olievier, I.; van Kleef, J.; Dahan, A. Respiratory sites of action of propofol: Absence of depression of peripheral chemoreflex loop by low-dose propofol. Anesthesiology 2001, 95, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Eastwood, P.R.; Platt, P.R.; Shepherd, K.; Maddison, K.; Hillman, D.R. Collapsibility of the upper airway at different concentrations of propofol anesthesia. Anesthesiology 2005, 103, 470–477. [Google Scholar] [CrossRef]
- Eikermann, M.; Malhotra, A.; Fassbender, P.; Zaremba, S.; Jordan, A.S.; Gautam, S.; White, D.P.; Chamberlin, N.L. Differential effects of isoflurane and propofol on upper airway dilator muscle activity and breathing. Anesthesiology 2008, 108, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Wilson, S.L.; Thach, B.T.; Brouillette, R.T.; Abu-Osba, Y.K. Upper airway patency in the human infant: Influence of airway pressure and posture. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1980, 48, 500–504. [Google Scholar] [CrossRef]
- Wang, D.; Chen, C.; Chen, J.; Xu, Y.; Wang, L.; Zhu, Z.; Deng, D.; Chen, J.; Long, A.; Tang, D.; et al. The use of propofol as a sedative agent in gastrointestinal endoscopy: A meta-analysis. PLoS ONE 2013, 8, e53311. [Google Scholar] [CrossRef]
- Goudra, B.; Nuzat, A.; Singh, P.M.; Gouda, G.B.; Carlin, A.; Manjunath, A.K. Cardiac arrests in patients undergoing gastrointestinal endoscopy: A retrospective analysis of 73,029 procedures. Saudi J. Gastroenterol. 2015, 21, 400–411. [Google Scholar] [CrossRef]
- Jordan, A.S.; Eckert, D.J.; Wellman, A.; Trinder, J.A.; Malhotra, A.; White, D.P. Termination of respiratory events with and without cortical arousal in obstructive sleep apnea. Am. J. Respir. Crit. Care. Med. 2011, 184, 1183–1191. [Google Scholar] [CrossRef]
- Isono, S.; Tanaka, A.; Nishino, T. Lateral position decreases collapsibility of the passive pharynx in patients with obstructive sleep apnea. Anesthesiology 2002, 97, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Andrade, C.M.; Patel, B.; Gill, J.; Amodeo, D.; Kulkarni, P.; Goldsmith, S.; Bachman, B.; Geerken, R.; Klein, M.; Anderson, W.; et al. Safety of gastrointestinal endoscopy with conscious sedation in patients with and without obstructive sleep apnea. J. Clin. Gastroenterol. 2016, 50, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Jordan, A.S.; O’Donoghue, F.J.; Cori, J.M.; Trinder, J. Physiology of Arousal in Obstructive Sleep Apnea and Potential Impacts for Sedative Treatment. Am. J. Respir. Crit. Care. Med. 2017, 196, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Kohzuka, Y.; Isono, S.; Ohara, S.; Kawabata, K.; Kitamura, A.; Suzuki, T.; Almeida, F.R.; Sato, Y.; Iijima, T. Nasopharyngeal Tube Effects on Breathing during Sedation for Dental Procedures: A Randomized Controlled Trial. Anesthesiology 2019, 130, 946–957. [Google Scholar] [CrossRef] [PubMed]
- Lewandowska, K.; Mędrzycka‑Dąbrowska, W.; Kwiecień‑Jaguś, K.; Czyż‑Szypenbejl, K. Factors determining sleep in patients hospitalised in ICUs in a hospital in Northern Poland. Sleep Biol. Rhythms 2019, 17, 243–250. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Zhuge, P.; Jiang, Y.; Shao, K.; Hu, L.; Feng, G. Correlation between nasopharyngoscopy and magnetic resonance imaging (MRI) in locating the upper airway obstruction plane in male obstructive sleep apnea hypopnea syndrome (OSAHS) patients. Sleep Biol. Rhythms 2017, 15, 269–276. [Google Scholar] [CrossRef]
- Rex, D.K.; Deenadayalu, V.P.; Eid, E.; Imperiale, T.F.; Walker, J.A.; Sandhu, K.; Clarke, A.C.; Hillman, L.C.; Horiuchi, A.; Cohen, L.B.; et al. Endoscopist-directed administration of propofol: A worldwide safety experience. Gastroenterology 2009, 137, 1229–1237. [Google Scholar] [CrossRef] [PubMed]
- Ballester, E.; Badia, J.R.; Hernández, L.; Farré, R.; Navajas, D.; Montserrat, J.M. Nasal prongs in the detection of sleep-related disordered breathing in the sleep apnoea/hypopnoea syndrome. Eur. Respir. J. 1998, 11, 880–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cacho, G.; Pérez-Calle, J.L.; Barbado, A.; Lledó, J.L.; Ojea, R.; Fernández-Rodríguez, C.M. Capnography is superior to pulse oximetry for the detection of respiratory depression during colonoscopy. Rev. Esp. Enferm. Dig. 2010, 102, 86–89. [Google Scholar] [CrossRef] [Green Version]
- Furukawa, T.; Nakano, H.; Yoshihara, K.; Sudo, N. Predictors of objectively measured snoring in a working population. Sleep Biol. Rhythms 2019, 17, 349–354. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n = 10 |
|---|---|
| Mean ± SD or N | |
| Demographics | |
| Age (years) | 71 ± 7 |
| Males, Females | 6, 4 |
| Height (cm) | 159 ± 9 |
| Body weight (kg) | 59 ± 8 |
| Body mass index (kg/m2) | 23.6 ± 3.5 |
| Sedation drug | |
| Initial injection dose of propofol (mg/kg) | 1.2 ± 0.4 |
| Total dose of propofol (mg/kg/hour) | 5.1 ± 0.8 |
| Variables | n = 10 |
|---|---|
| Mean ± SD | |
| Sedation quality | |
| Sedation period (min) | 114 ± 36 |
| Total sleep time (min) | 93 ± 34 |
| Sedation efficacy (%) | 81 ± 7 |
| Sedation efficacy (%) | 15.4 ± 9.2 |
| Nature of respiratory disturbances during sedation | |
| Apnea hypopnea index with desaturation (h−1) | 4.0 ± 5.3 |
| Apnea hypopnea index without desaturation (h−1) | 11.4 ± 7.1 |
| Mean duration of apnea hypopnea (seconds) | 26 ± 2 |
| Longest apnea and hypopnea (seconds) | 62 ± 18 |
| Mean nadir SaO2 of desaturation events (%) | 89.6 ± 5.1 |
| Lowest SaO2 of desaturation events (%) | 82.0 ± 11.7 |
| Types of Respiratory Disturbances | Arousal | Desaturation Events: N (%) | No Desaturation Events: N (%) | Total Events N (%) | Chi-Sqaure p Value |
|---|---|---|---|---|---|
| Apnea and hypopneas (n = 245) | yes | 24 (9.8) | 31 (12.7) | 55 (22.4) | <0.001 |
| no | 29 (11.8) | 161 (65.7) | 190 (77.6) | ||
| Obstructive apnea (n = 134) | yes | 16 (11.9) | 16 (11.9) | 32 (23.8) | <0.001 |
| no | 19 (14.2) | 83 (61.9) | 102 (76.2) | ||
| Obstructive hypopnea (n = 61) | yes | 8 (13.1) | 5 (8.2) | 13 (21.3) | 0.012 |
| no | 10 (16.4) | 38 (62.3) | 48 (78.7) | ||
| Central apnea (n = 19) | yes | 0 | 1 (5.3) | 1 (5.3) | NA |
| no | 0 | 18 (94.7) | 18 (94.7) | ||
| Central hypopnea (n = 31) | yes | 0 | 9 (29.0) | 9 (29.0) | NA |
| no | 0 | 22 (71.0) | 22 (71.0) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urahama, R.; Uesato, M.; Aikawa, M.; Kunii, R.; Isono, S.; Matsubara, H. Occurrence of Cortical Arousal at Recovery from Respiratory Disturbances during Deep Propofol Sedation. Int. J. Environ. Res. Public Health 2019, 16, 3482. https://doi.org/10.3390/ijerph16183482
Urahama R, Uesato M, Aikawa M, Kunii R, Isono S, Matsubara H. Occurrence of Cortical Arousal at Recovery from Respiratory Disturbances during Deep Propofol Sedation. International Journal of Environmental Research and Public Health. 2019; 16(18):3482. https://doi.org/10.3390/ijerph16183482
Chicago/Turabian StyleUrahama, Ryuma, Masaya Uesato, Mizuho Aikawa, Reiko Kunii, Shiroh Isono, and Hisahiro Matsubara. 2019. "Occurrence of Cortical Arousal at Recovery from Respiratory Disturbances during Deep Propofol Sedation" International Journal of Environmental Research and Public Health 16, no. 18: 3482. https://doi.org/10.3390/ijerph16183482
APA StyleUrahama, R., Uesato, M., Aikawa, M., Kunii, R., Isono, S., & Matsubara, H. (2019). Occurrence of Cortical Arousal at Recovery from Respiratory Disturbances during Deep Propofol Sedation. International Journal of Environmental Research and Public Health, 16(18), 3482. https://doi.org/10.3390/ijerph16183482