The Relationship between Scabies and Stroke: A Population-Based Nationwide Study

Abstract
:1. Introduction
2. Materials and Methods
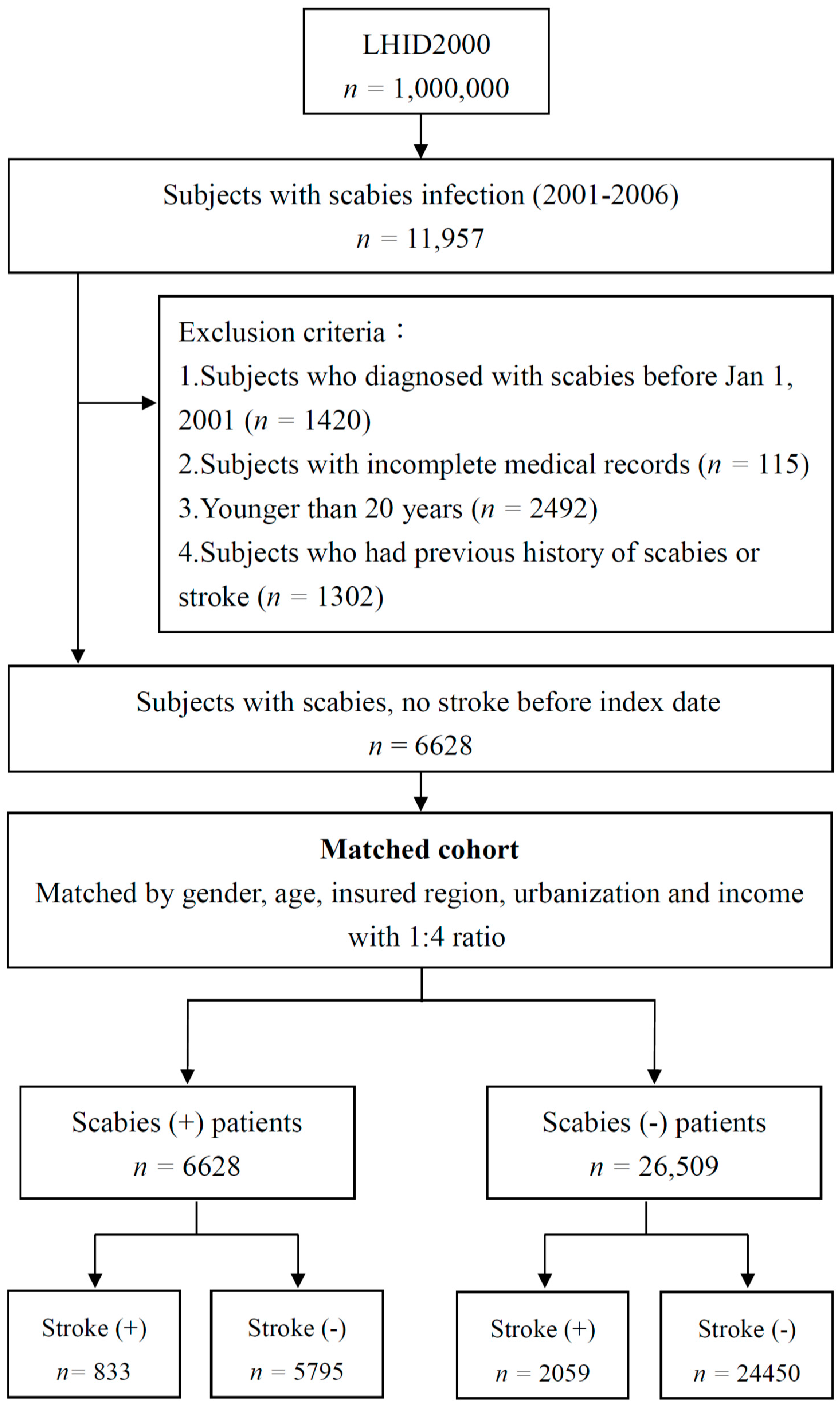
2.1. Database
2.2. Study Population
2.3. Covariates
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| aHR | Adjusted hazard ratio |
| CI | Confidence interval |
| HR | Hazard ratio |
| ICD-9-CM | The International Classification of Diseases, Ninth Revision, Clinical Modification |
| IL | Interleukin |
| NHIRD | National Health Insurance Research Database |
| LHID2000 | Longitudinal Health Insurance Database 2000 |
| Th17 | T helper 17 cells |
| PID | Pelvic Inflammation Disease |
References
- Chosidow, O. Scabies. N. Engl. J. Med. 2006, 354, 1718–1727. [Google Scholar] [CrossRef]
- Romani, L.; Steer, A.C.; Whitfeld, M.J.; Kaldor, J.M. Prevalence of scabies and impetigo worldwide: A systematic review. Lancet Infect. Dis. 2015, 15, 960–967. [Google Scholar] [CrossRef]
- Romani, L.; Koroivueta, J.; Steer, A.C.; Kama, M.; Kaldor, J.M.; Wand, H.; Hamid, M.; Whitfeld, M.J. Scabies and impetigo prevalence and risk factors in Fiji: A national survey. PLoS Negl. Trop. Dis. 2015, 9, e0003452. [Google Scholar] [CrossRef]
- Turkmen, K.; Erdur, M.F.; Kucuk, A. Risk factors that can affect the progression of chronic kidney disease in patients with poststreptecoccal glomerulonephritis history. Kidney Int. 2013, 83, 762. [Google Scholar] [CrossRef]
- Chung, S.D.; Wang, K.H.; Huang, C.C.; Lin, H.C. Scabies increased the risk of chronic kidney disease: A 5-year follow-up study. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 286–292. [Google Scholar] [CrossRef]
- Walton, S.F.; Oprescu, F.I. Immunology of scabies and translational outcomes: Identifying the missing links. Curr. Opin. Infect. Dis. 2013, 26, 116–122. [Google Scholar] [CrossRef]
- Donnan, G.A.; Fisher, M.; Macleod, M.; Davis, S.M. Stroke. Lancet 2008, 371, 1612–1623. [Google Scholar] [CrossRef]
- Ra, G.S.; Yoo, J.C.; Kang, C.J.; Kim, Y.S. Microfabricated in-channel structured polydimethylsiloxane microfluidic system for a lab-on-a-chip. J. Nanosci. Nanotechnol. 2008, 8, 4588–4592. [Google Scholar] [CrossRef]
- Jakovljevic, D.; Sarti, C.; Sivenius, J.; Torppa, J.; Mähönen, M.; Immonen-Räihä, P.; Kaarsalo, E.; Alhainen, K.; Kuulasmaa, K.; Tuomilehto, J.; et al. Socioeconomic status and ischemic stroke: The FINMONICA Stroke Register. Stroke 2001, 32, 1492–1498. [Google Scholar] [CrossRef]
- Lin, H.C.; Lin, Y.J.; Liu, T.C.; Chen, C.S.; Chiu, W.T. Urbanization and stroke prevalence in Taiwan: Analysis of a nationwide survey. J. Urban Health 2007, 84, 604–614. [Google Scholar] [CrossRef]
- Chen, P.C.; Tseng, T.C.; Hsieh, J.Y.; Lin, H.W. Association between stroke and patients with pelvic inflammatory disease: A nationwide population-based study in Taiwan. Stroke 2011, 42, 2074–2076. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.W.; Chao, P.Z.; Hao, W.R.; Liou, T.H.; Lin, H.W. Risk of stroke among patients with rhinosinusitis: A population-based study in Taiwan. Am. J. Rhinol. Allergy 2012, 26, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Aal, A.A.; Hassan, M.A.; Gawdat, H.I.; Ali, M.A.; Barakat, M. Immunomodulatory impression of anti and pro-inflammatory cytokines in relation to humoral immunity in human scabies. Int. J. Immunopathol. Pharmacol. 2016, 29, 188–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, X.; Walton, S.F.; Murray, H.C.; King, M.; Kelly, A.; Holt, D.C.; Currie, B.J.; McCarthy, J.S.; Mounsey, K.E. Crusted scabies is associated with increased IL-17 secretion by skin T cells. Parasite Immunol. 2014, 36, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Mounsey, K.E.; Murray, H.C.; Bielefeldt-Ohmann, H.; Pasay, C.; Holt, D.C.; Currie, B.J.; Walton, S.F.; McCarthy, J.S. Prospective study in a porcine model of Sarcoptes scabiei indicates the association of Th2 and Th17 pathways with the clinical severity of scabies. PLoS Negl. Trop. Dis. 2015, 9, e0003498. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis—An inflammatory disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Abou-Raya, A.; Abou-Raya, S. Inflammation: A pivotal link between autoimmune diseases and atherosclerosis. Autoimmun. Rev. 2006, 5, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Mullins, J.S.; Arlian, L.G.; Morgan, M.S. Extracts of Sarcoptes scabiei De Geer downmodulate secretion of IL-8 by skin keratinocytes and fibroblasts and of GM-CSF by fibroblasts in the presence of proinflammatory cytokines. J. Med. Entomol. 2009, 46, 845–851. [Google Scholar] [CrossRef]
- Hartman, J.; Frishman, W.H. Inflammation and atherosclerosis: A review of the role of interleukin-6 in the development of atherosclerosis and the potential for targeted drug therapy. Cardiol. Rev. 2014, 22, 147–151. [Google Scholar] [CrossRef]
- Tedgui, A.; Mallat, Z. Cytokines in atherosclerosis: Pathogenic and regulatory pathways. Physiol. Rev. 2006, 86, 515–581. [Google Scholar] [CrossRef]
- Huber, S.A.; Sakkinen, P.; Conze, D.; Hardin, N.; Tracy, R. Interleukin-6 exacerbates early atherosclerosis in mice. Arterioscler. Thromb. Vasc. Biol. 1999, 19, 2364–2367. [Google Scholar] [CrossRef] [PubMed]
- King, V.L.; Szilvassy, S.J.; Daugherty, A. Interleukin-4 deficiency decreases atherosclerotic lesion formation in a site-specific manner in female LDL receptor−/− mice. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Davenport, P.; Tipping, P.G. The role of interleukin-4 and interleukin-12 in the progression of atherosclerosis in apolipoprotein E-deficient mice. Am. J. Pathol. 2003, 163, 1117–1125. [Google Scholar] [CrossRef]
- Mantovani, A.; Bussolino, F.; Dejana, E. Cytokine regulation of endothelial cell function. FASEB J. 1992, 6, 2591–2599. [Google Scholar] [CrossRef] [PubMed]
- Boysen, G.; Nyboe, J.; Appleyard, M.; Sørensen, P.S.; Boas, J.; Somnier, F.; Jensen, G.; Schnohr, P. Stroke incidence and risk factors for stroke in Copenhagen, Denmark. Stroke 1988, 19, 1345–1353. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.D.; Whisnant, J.P.; Sicks, R.D.; O’Fallon, W.M.; Wiebers, D.O. Stroke incidence, prevalence, and survival: Secular trends in Rochester, Minnesota, through 1989. Stroke 1996, 27, 373–380. [Google Scholar]
- Wolf, P.A.; D’Agostino, R.B.; O’Neal, M.A.; Sytkowski, P.; Kase, C.S.; Belanger, A.J.; Kannel, W.B. Secular trends in stroke incidence and mortality: The Framingham Study. Stroke 1992, 23, 1551–1555. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Number of (%) Individuals | ||
|---|---|---|---|
| With Scabies n = 6628 | Without Scabies n = 26,509 | p-Value | |
| Gender | 0.998 | ||
| Female | 3196 (48.2%) | 12,783 (48.2%) | |
| Male | 3432 (51.8%) | 13,726 (51.8%) | |
| Age_Group | 1 | ||
| 20–29 | 1797 (27.1%) | 7188 (27.1%) | |
| 30–39 | 1227 (18.5%) | 4908 (18.5%) | |
| 40–49 | 1236 (18.6%) | 4944 (18.7%) | |
| 50–59 | 869 (13.1%) | 3476 (13.1%) | |
| 60–69 | 552 (8.3%) | 2208 (8.3%) | |
| ≥70 | 947 (14.3%) | 3785 (14.3%) | |
| Income_Group | 0.001 | ||
| <20,000 | 5039 (76%) | 19,697 (74.3%) | |
| 20,000–39,999 | 1027 (15.5%) | 4287 (16.2%) | |
| 40,000–59,999 | 433 (6.5%) | 1817 (6.9%) | |
| ≥60,000 | 129 (1.9%) | 708 (2.7%) | |
| Geography | <0.001 | ||
| North | 3053 (46.1%) | 13,893 (52.4%) | |
| Central | 1260 (19%) | 4598 (17.3%) | |
| South | 1993 (30.1%) | 7308 (27.6%) | |
| Other (East+ Penghu) | 322 (4.9%) | 710 (2.7%) | |
| Urbanization | <0.001 | ||
| 1 (highest) | 1564 (23.6%) | 8017 (30.2%) | |
| 2 | 2051 (30.9%) | 7929 (29.9%) | |
| 3 | 1144 (17.3%) | 4870 (18.4%) | |
| 4 | 1051 (15.9%) | 3440 (13%) | |
| 5 | 144 (2.2%) | 466 (1.8%) | |
| 6 | 362 (5.5%) | 947 (3.6%) | |
| 7 (lowest) | 312 (4.7%) | 840 (3.2%) | |
| Comorbidity | |||
| DM | 1372 (20.7%) | 3499 (13.2%) | <0.001 |
| Hypertension | 2274 (34.3%) | 6540 (24.7%) | <0.001 |
| CHD | 1239 (18.7%) | 3211 (12.1%) | <0.001 |
| Hyperlipidemia | 1645 (24.8%) | 5261 (19.8%) | <0.001 |
| CKD | 464 (7%) | 935 (3.5%) | <0.001 |
| Atrial_fibrillation | 176 (2.7%) | 375 (1.4%) | <0.001 |
| Variable | Number of (%) Individuals | |
|---|---|---|
| With Scabies n = 6628 | Without Scabies n = 26,509 | |
| With stroke | 833 (12.6) | 2059 (7.8) |
| Without stroke | 5795 (87.4) | 24,450 (92.2) |
| Crude HR | 1.67 (1.54–1.81) ‡ | - |
| Variable | Crude | Adjusted |
|---|---|---|
| HR (95% CI) | HR * (95% CI) | |
| Scabies | 1.67 (1.54–1.81) ‡ | 1.32 (1.21–1.43) ‡ |
| Gender | ||
| Female | 1 | - |
| Male | 1.06 (0.99–1.14) | - |
| Age_Group | ||
| 20–29 | 1 | 1 |
| 30–39 | 2.01 (1.58–2.57) ‡ | 1.69 (1.32–2.16) ‡ |
| 40–49 | 4.4 (3.56–5.46) ‡ | 2.63 (2.11–3.28) ‡ |
| 50–59 | 9.51 (7.74–11.68) ‡ | 3.74 (3.01–4.65) ‡ |
| 60–69 | 18.49 (15.1–22.64) ‡ | 5.53 (4.46–6.87) ‡ |
| ≥70 | 24.32 (20.05–29.52) ‡ | 7.99 (6.49–9.83) ‡ |
| Income_Group | ||
| <20,000 | 1 | 1 |
| 20,000–39,999 | 0.54 (0.47–0.6) ‡ | 1.02 (0.9–1.17) |
| 40,000–59,999 | 0.44 (0.36–0.54) ‡ | 0.77 (0.62–0.94) † |
| ≥60,000 | 0.58 (0.43–0.76) ‡ | 0.72 (0.54–0.96) † |
| Geography | ||
| North | 1 | 1 |
| Central | 1.13 (1.02–1.25) ‡ | 0.94 (0.84–1.05) |
| South | 1.23 (1.13–1.34) ‡ | 0.96 (0.87–1.05) |
| Other (East+ Penghu) | 1.73 (1.45–2.06) ‡ | 1.03 (0.86–1.25) |
| Urbanization | ||
| 1 (highest) | 1 | 1 |
| 2 | 1.07 (0.97–1.19) | 1.04 (0.94–1.16) |
| 3 | 1.2 (1.07–1.35) † | 1.14 (1.01–1.28) † |
| 4 | 1.61 (1.44–1.81) ‡ | 1.15 (1.01–1.29) † |
| 5 | 2.31 (1.86–2.86) ‡ | 1.18 (0.94–1.47) |
| 6 | 1.84 (1.55–2.17) ‡ | 1.07 (0.9–1.29) |
| 7 (lowest) | 1.85 (1.55–2.21) ‡ | 1.13 (0.94–1.37) |
| Comorbidity | ||
| DM | 4.44 (4.12–4.78) ‡ | 1.36 (1.25–1.47) ‡ |
| Hypertension | 9.4 (8.64–10.23) ‡ | 3.19 (2.88–3.54) ‡ |
| CHD | 6.25 (5.81–6.73) ‡ | 1.63 (1.5–1.77) ‡ |
| Hyperlipidemia | 3.09 (2.87–3.32) ‡ | 1.16 (1.07–1.26) ‡ |
| CKD | 4.89 (4.42–5.41) ‡ | 1.25 (1.13–1.39) ‡ |
| Atrial_fibrillation | 7.36 (6.47–8.38) ‡ | 1.61 (1.4–1.84) ‡ |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, M.-H.; Li, C.-Y.; Pan, H.; Lin, Y.-C. The Relationship between Scabies and Stroke: A Population-Based Nationwide Study. Int. J. Environ. Res. Public Health 2019, 16, 3491. https://doi.org/10.3390/ijerph16183491
Wu M-H, Li C-Y, Pan H, Lin Y-C. The Relationship between Scabies and Stroke: A Population-Based Nationwide Study. International Journal of Environmental Research and Public Health. 2019; 16(18):3491. https://doi.org/10.3390/ijerph16183491
Chicago/Turabian StyleWu, Meng-Huan, Chien-Yu Li, Huichin Pan, and Yu-Chieh Lin. 2019. "The Relationship between Scabies and Stroke: A Population-Based Nationwide Study" International Journal of Environmental Research and Public Health 16, no. 18: 3491. https://doi.org/10.3390/ijerph16183491
APA StyleWu, M. -H., Li, C. -Y., Pan, H., & Lin, Y. -C. (2019). The Relationship between Scabies and Stroke: A Population-Based Nationwide Study. International Journal of Environmental Research and Public Health, 16(18), 3491. https://doi.org/10.3390/ijerph16183491