Identifying Individual Stressors in Geriatric Nursing Staff—A Cross-Sectional Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
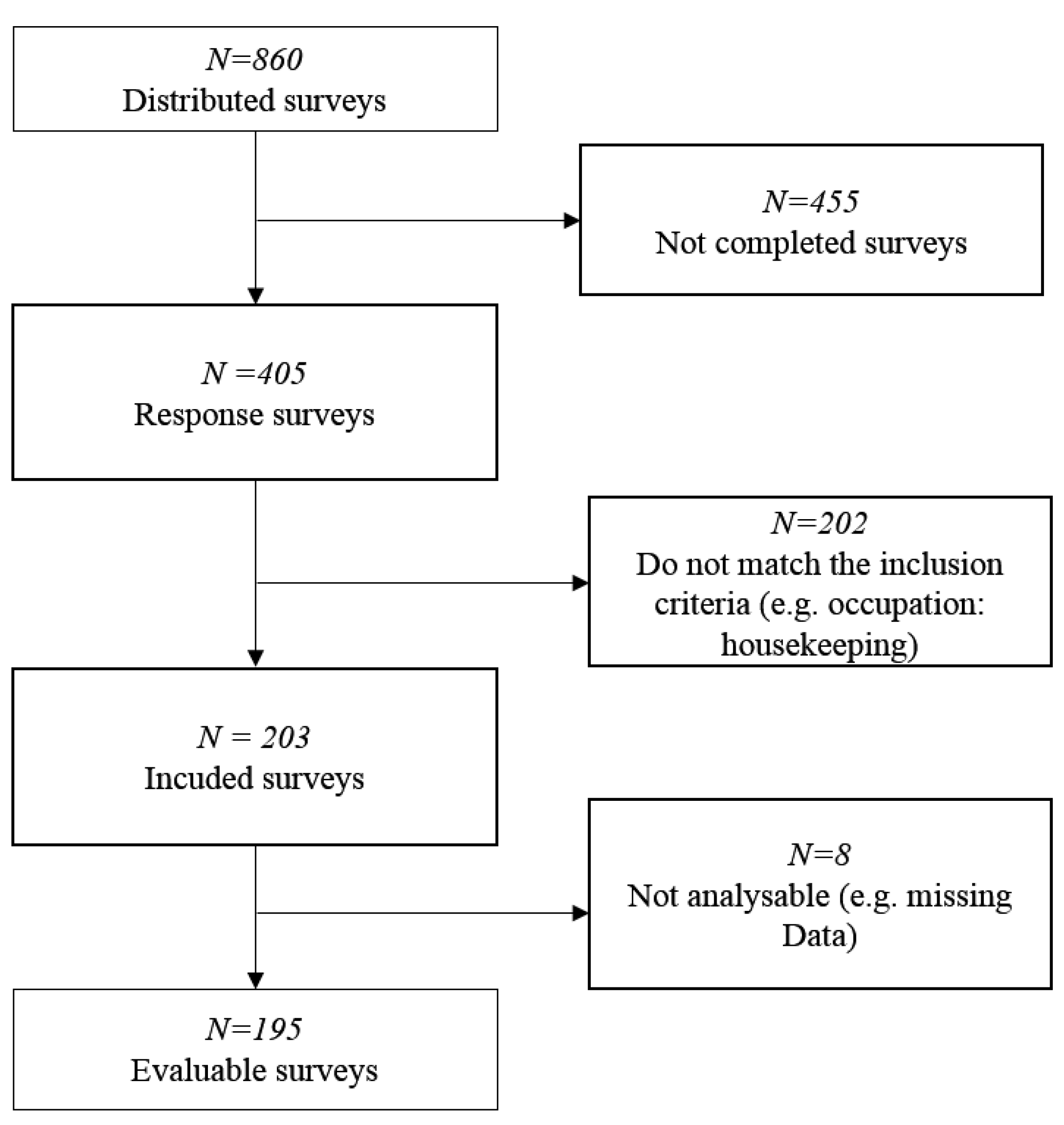
2.2. Sample and Setting
2.3. Measures
- (1)
- workplace exposure (Questionnaire for Subjective Assessment of Workplace Exposure- modified Slesina Questionnaire) [37];
- (2)
- musculoskeletal complaints (Questionnaire on Musculoskeletal Complaints-Nordic Questionnaire) [38];
- (3)
- physical and mental well-being (Health Survey SF-12): The SF-12 is an economic short form of the SF-36, consisting of twelve items, to measure the health-related quality of life. Its items are summarized in a sum score for mental and a sum score for physical well-being. The reliability and validity scales are considered established. Cronbachs Alpha ranged between 0.57 to 0.94 [39];
- (4)
- Trier Inventory for Chronic Stress (TICS): The twelve-item screening subscale (SSCS) of the TICS provides information about perceived stress within the last three months. Internal consistency (Cronbachs Alpha) with a range from 0.84 to 0.91 indicates good to very good reliability [36];
- (5)
- work-related behavior and experience patterns (Questionnaire on Work-Related Behavior and Experience Patterns (AVEM) [32];
- (6)
- questions regarding health-related resources due to WHO-criteria for e.g., physical activity and nutrition behavior.
2.4. Procedures
2.5. Analysis
- The whole group descriptive analysis and frequencies of relevant physical and psychological work-related stressors and main musculoskeletal disorders as well as resilience factors were done with Chi2-tests.
- The resulting factors from step one were analyzed by comparing groups with chronic and non-chronic stress. In addition to the Chi2-tests, a one-way Analysis of Variance (one-way ANOVA) was conducted (e.g., Scores of SF-12).
- To further analyze the potential influential factors, a Pearson product moment correlation was computed in order to prepare a four-step hierarchical regression analysis: the regression analysis was conducted to identify which variables determine stress scores of the TICS. The potential stressors identified from step 1 were divided into the following blocks for the regression analysis:
- Block I:
- physical strains (heavy physical tasks, awkward posture, holding heavy loads, lifting heavy loads, physical well-being and standing);
- Block II:
- psychological strains (pressure to perform, time pressure, shift-work, deadline pressure and psychological well-being);
- Block III:
- pattern (G, S, A and B);
- Block IV:
- resilience factors (satisfaction of health condition, frequency of being calm and relaxed in the past seven days, importance to improve the state of health, days of being full of energy, nutritional behavior, frequency of having breakfast and stress level).
3. Results
3.1. Participants
3.2. Prevalence of Potential Stressors in Geriatric Nurses
3.3. Comparison of the Geriatric Nurses with Chronic and Non-Chronic Stress
3.4. Analysis of Correlation
3.5. Results of the Regression Model
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. heavy physical tasks | 1 | |||||||||
| 2. awkward posture | 0.46 ** | 1 | ||||||||
| 3. standing | 0.24 ** | 035 ** | 1 | |||||||
| 4. holding heavy loads | 0.55 ** | 0.38 ** | 0.15 | 1 | ||||||
| 5. lifting heavy loads | 0.56 ** | 0.45 ** | 0.17 * | 0.69 ** | 1 | |||||
| 6. pressure to perform | 0.42 ** | 0.23 * | 0.13 | 0.24 * | 0.35 ** | 1 | ||||
| 7. deadline pressure | 0.37 ** | 0.18 | 0.26 ** | 0.23 * | 0.29 ** | 0.52 ** | 1 | |||
| 8. time pressure | 0.46 ** | 0.25 ** | 0.38 ** | 0.20 * | 0.19 | 0.52 ** | 0.55 ** | 1 | ||
| 9. shift work | 0.40 ** | 0.36 ** | 0.30 ** | 0.30 ** | 0.27 ** | 0.30 ** | 0.23 * | 0.18 | 1 | |
| 10. SSCS | −0.39 ** | −0.30 ** | −0.14 | −0.34 ** | −0.33 ** | −0.38 ** | −0.34 | −0.35 ** | −0.25 ** | 1 |
Appendix B
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1. mental well-being | 1 | ||||||
| 2. physical well-being | 0.17 * | 1 | |||||
| 3. pattern G | 0.33 ** | 0.74 | 1 | ||||
| 4. pattern S | 0.22 * | 0.12 | −0.23 * | 1 | |||
| 5. pattern A | −0.24 * | −0.06 | 0.13 | −0.66 ** | 1 | ||
| 6. pattern B | −0.50 ** | −0.09 | −0.50 ** | −0.22 * | 0.43 ** | 1 | |
| 7. SSCS | −0.64 ** | −0.42 ** | −0.23 * | −0.39 ** | 0.41 ** | 0.55 ** | 1 |
Appendix C
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| 1. satisfaction with health status | 1 | |||||||
| 2. importance to improve status of health | −0.06 | 1 | ||||||
| 3. nutritional behaviour | 0.142 | 0.07 | 1 | |||||
| 4. frequency of having breakfast | 0.02 | 0.19 * | 0.23 ** | 1 | ||||
| 5. frequency of being calm and relaxed | 0.40 ** | 0.05 | 0.25 ** | 0.10 | 1 | |||
| 6. frequency of full energy | 0.44 ** | 0.06 | 0.15 * | 0.08 | 0.50 ** | 1 | ||
| 7. stress level | 0.47 ** | −0.03 | 0.27 ** | 0.11 | 0.31 ** | 0.32 ** | 1 | |
| 8. SSCS | 0.49 ** | −0.19 | 0.16 | 0.00 | 0.49 ** | 0.41 | 0.44 | 1 |
Appendix D
| Variables | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. neck complaints | 1 | ||||
| 2. shoulder complaints | 0.68 | 1 | |||
| 3. upper back complaints/thoracic spine | 0.45 | 0.44 | 1 | ||
| 4. lower back/lumbar complaints | 0.46 | 0.42 * | 0.61 | 1 | |
| 5. SSCS | −0.35 | −0.33 | −0.21 | −0.35 | 1 |
References
- McVicar, A. Workplace stress in nursing: A literature review. J. Adv. Nurs. 2003, 44, 633–642. [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; Williams, S. Reducing work related psychological ill health and sickness absence: A systematic literature review. Occup. Environ. Med. 2003, 60, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Pélissier, C.; Vohito, M.; Fort, E.; Sellier, B.; Agard, J.P.; Fontana, L.; Charbotel, B. Risk factors for work-related stress and subjective hardship in health-care staff in nursing homes for the elderly: A cross-sectional study. J. Occup. Health 2015, 57, 285–296. [Google Scholar] [CrossRef] [PubMed]
- Ruotsalainen, J.H.; Verbeek, J.H.; Mariné, A.; Serra, C. Preventing occupational stress in healthcare workers (Review). Cochrane Database Syst. Rev. 2015, 4, CD002892. [Google Scholar]
- WHO. Data and Statistics [WHO Web Side]. 2018. Available online: http://www.euro.who.int/en/health-topics/Health-systems/nursing-and-midwifery/data-and-statistics (accessed on 26 February 2019).
- Burmeister, E.A.; Kalisch, B.J.; Xie, B.; Doumit, M.A.; Lee, E.; Ferraresion, A.; Terzioglu, F.; Bragadóttir, H. Determinants of nurse absenteeism and intent to leave: An international study. J. Nurs. Manag. 2019, 27, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Farquharson, B.; Bell, C.; Johnston, D.; Jones, M.; Schofield, P.; Allan, J.; Ricketts, I.; Morrison, K.; Johnston, M. Nursing stress and patient care: Real-time investigation of the effect of nursing tasks and demands on psychological stress, physiological stress, and job performance: Study protocol. J. Adv. Nurs. 2013, 69, 2327–2335. [Google Scholar] [CrossRef]
- Maresso, A.; Mladovsky, P.; Thomson, S.; Sagan, A.; Karanikolos, M.; Richardson, E.; Cylus, J.; Evetovits, T.; Jowett, M.; Figueras, J.; et al. Economic Crisis, Health Systems and Health in Europe. Country Experiences. [WHO PDF web site]. 2015. Available online: http://www.euro.who.int/__data/assets/pdf_file/0010/279820/Web-economic-crisis-health-systems-and-health-web.pdf?ua=1 (accessed on 12 March 2019).
- Nolting, H.D.; Berger, J.; Niemann, D.; Schiffhorst, G.; Genz, H.O.; Kordt, M. BGW-DAK Stress-Monitoring. [BGW-DAK PDF web site]. 2001. Available online: http://people.f3.htw-berlin.de/Professoren/Pruemper/instrumente/KFZA-BGW-DAK-StressMonitoring_UEBERBLICK.pdf (accessed on 28 October 2018).
- Kaluza, G. Gelassenheit und Sicher im Stress. Das Stresskompetenz-Buch: Stress Erkennen, Verstehen, Bewältigen; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Duxbury, L.; Higgins, C.; Smart, R. Elder care and the impact of caregiver strain on the health of employed caregivers. Work 2009, 40, 29–40. [Google Scholar]
- Saarnio, R.; Sarvimäki, A.; Laukkala, H.; Isola, A. Stress of conscience among staff caring for older persons. Nurs. Ethics 2012, 19, 104–115. [Google Scholar] [CrossRef]
- Cocco, E.; Gatti, M.; de Mendonça Lima, C.A.; Camus, V. A comparative study of stress and burnout among staff caregivers in nursing homes and acute geriatric wards. Int. J. Geriatr. Psychiatry 2003, 18, 78–85. [Google Scholar] [CrossRef]
- Eley, R.; Hegney, D.; Buikstra, E.; Fallon, T.; Plank, A.; Parker, V. Aged care nursing in queensland—The nurses’ view. J. Clin. Nurs. 2007, 16, 860–872. [Google Scholar] [CrossRef]
- Cope, V.C.; Jones, B.; Hendricks, J. Residential aged care nurses: Portraits of resilience. Contemp. Nurse 2016, 52, 736–752. [Google Scholar] [CrossRef] [PubMed]
- Hasson, H.; Arnetz, J. Nursing staff competence, work strain, stress and satisfaction in elderly care: A comparison of home-based care and nursing homes. J. Clin. Nurs. 2006, 17, 468–481. [Google Scholar] [CrossRef] [PubMed]
- Nübling, M.; Vomstein, M.; Schmidt, S.G.; Gregersen, S.; Dulon, M.; Nienhaus, A. Psychosocial work load and stress in the geriatric care. BMC Public Health 2010, 10, 428. [Google Scholar] [CrossRef] [PubMed]
- Alexandrova-Karamanova, A.; Todorova, I.; Montgomery, A.; Panagopoulou, E.; Costa, P.; Baban, A.; Davas, A.; Milosevic, M.; Mijakoski, D. Burnout and health behaviors in health professionals from seven European countries. Int. Arch. Occup. Environ. Health 2016, 89, 1059–1075. [Google Scholar] [CrossRef]
- Hall, L.H.; Johnson, J.; Watt, I.; Tsipa, A.; O’Connor, D.B. Healthcare staff wellbeing, burnout, and patient safety: A systematic review. PLoS ONE 2016, 11, e0159015. [Google Scholar] [CrossRef]
- Steptoe, A.; Kivimäki, M. Stress and cardiovascular disease. Nat. Rev. Cardiol. 2012, 9, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Stansfeld, S.; Candy, B. Psychosocial work environment and mental health-a meta-analytic review. Scand. J. Work Environ. Health 2006, 32, 443–462. [Google Scholar] [CrossRef] [PubMed]
- Landsbergis, P.A.; Dobson, M.; Koutsouras, G.; Schnall, P. Job strain and ambulatory blood pressure: A meta-analysis and systematic review. Am. J. Public Health 2013, 103, e61–e71. [Google Scholar] [CrossRef]
- Bhatia, V.; Tandon, R.K. Stress and the gastrointestinal tract. J. Gastroenterol. Hepatol. 2005, 20, 332–339. [Google Scholar] [CrossRef]
- Poghosyan, L.; Clarke, S.P.; Finlayson, M.; Aiken, L.H. Nurse burnout and quality of care: Cross-national investigation in six countries. Res. Nurs. Health 2010, 33, 288–298. [Google Scholar] [CrossRef] [Green Version]
- Eatough, E.M.; Way, J.D.; Chang, C.H. Understanding the link between psychosocial work stressors and work-related musculoskeletal complaints. Appl. Ergon. 2012, 43, 554–563. [Google Scholar] [CrossRef] [PubMed]
- Carayon, P.; Smith, M.J.; Haims, M.C. Work organization, job stress, and work-related musculoskeletal disorders. Hum. Factors 1999, 41, 644–663. [Google Scholar] [CrossRef] [PubMed]
- Cameron, F.; Brownie, S. Enhancing resilience in registered aged care nurses. Australas. J. Ageing 2010, 29, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Mauno, S.; Ruokolainen, M.; Kinnunen, U.; De Bloom, J. Emotional labour and work engagement among nurses: Examining perceived compassion, leadership and work ethic as stress buffers. J. Adv. Nurs. 2016, 72, 169–1181. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, K.H.; Diestel, S. Job demands and personal resources in their relations to indicators of job strain among nurses for older people. J. Adv. Nurs. 2013, 69, 2185–2195. [Google Scholar] [CrossRef] [PubMed]
- Zapf, D.; Semmer, N. Stress und Gesundheit in Organisationen: Enzyklopädie Der Psychologie, Themenbereich, D., 2nd ed.; Serie III, Band 3 Organisationspsychologie; Hogrefe: Göttingen, Germany, 2004. [Google Scholar]
- Carver, C.S.; Connor-Smith, J. Personality and coping. Ann. Rev. Psychol. 2010, 61, 679–704. [Google Scholar] [CrossRef]
- Schaarschmidt, U.; Fischer, A.W. Arbeitsbezogenes Verhaltens-und Erlebensmuster: AVEM (Standardform). AVEM-44 (Kurzform); Manual Pearson: Frankfurt, Germany, 2010. [Google Scholar]
- Grundmann, J.; Sude, K.; Löwe, B.; Wingenfeld, K. Arbeitsbezogene Stressbelastung und psychische Gesundheit: Eine Befragung von Psychotherapeutinnen und therapeuten in Ausbildung. Psychother. Psychosom. Med. Psychol. 2013, 63, 145–149. [Google Scholar] [CrossRef]
- Bamberg, E.; Keller, M.; Wohlert, C.; Zeh, A. BGW-Stresskonzept. Das Arbeitspsychologische Stressmodell; Berufsgenossenschaft für Gesundheitsdienst und Wohlfahrtspflege (Hg.): Hamburg, Germany, 2006. [Google Scholar]
- Dackert, I. The impact of team climate for innovation on well-being and stress in elderly care. J. Nurs. Manag. 2010, 18, 302–310. [Google Scholar] [CrossRef]
- Schulz, P.; Schlotz, W. Trierer Inventar zur Erfassung von chronischem Streß (TICS): Skalenkonstruktion, teststatistische Überprüfung und Validierung der Skala Arbeitsüberlastung. Diagnostica 1999, 45, 8–19. [Google Scholar] [CrossRef]
- Slesina, W. Fragebogen zur subjektiven Einschätzung der Belastungen am Arbeitsplatz (FEBA) [Bundesanstalt für Arbeitsschutz und Arbeitsmedizin PDF Rückenkompass Web Site]. 1987. Available online: www rueckenkompass. de/cd/doc/Fragen-Slesina pdf (accessed on 25 January 2019).
- Caffier, G.; Steinberg, U.; Liebers, F. Praxisorientiertes Methodeninventar zur Belastungs-und Beanspruchungsbeurteilung im Zusammenhang mit Arbeitsbedingten Muskel-Skelett-Erkrankungen [Bundesanstalt für Arbeitsschutz und Arbeitsmedizin PDF Web Site]. Available online: https://www.baua.de/DE/Angebote/Publikationen/Schriftenreihe/Forschungsberichte/1999/Fb850.pdf?__blob=publicationFile&v=1 (accessed on 23 January 2019).
- Bullinger, M.; Kirchberger, I. SF-36: Fragebogen Zum Gesundheitszustand; Handanweisung; Hogrefe: Göttingen, Germany, 1998. [Google Scholar]
- Simon, M.; Tackenberg, P.; Hasselhorn, H.M.; Kümmerling, A.; Büscher, A.; Müller, B.H. Auswertung Der Ersten Befragung Der NEXT-Studie in Deutschland; Universität Wuppertal: Wuppertal, Germany, 2005. [Google Scholar]
- Gelsema, T.I.; Van Der Doef, M.; Maes, S.; Janssen, M.; Akerboom, S.; Verhoeven, C. A longitudinal study of job stress in the nursing profession: Causes and consequences. J. Nurs. Manag. 2006, 14, 289–299. [Google Scholar] [CrossRef]

| Variables | Stressed N (%) | Non-stressed N (%) | Total N (%) |
|---|---|---|---|
| Gender (N) (%) | 124 (64%) 1 | 71 (36%) 2 | 195 (100%) |
| Male Sex | 14 | 10 | 24 |
| Female Sex | 107 | 60 | 167 |
| Age | 40.76 (11.7 SD) | 38.97(13.1 SD) | 40.1(12.2 SD) |
| Burden at workplace | |||
| heavy physical tasks | 100 (55.2) | 32 (17.7) | 132 (100) |
| awkward posture | 80 (46.2) | 32 (18.5) | 112 (64.7) |
| standing | 41 (24.0) | 20 (11.7) | 61 (35.7) |
| holding heavy loads | 71 (41.3) | 24 (14.0) | 95 (55.2) |
| lifting heavy loads | 82 (47.7) | 32 (18.6) | 114 (66.3) |
| pressure to perform | 50 (43.9) | 16 (14.0) | 66 (57.9) |
| deadline pressure | 25 (37.8) | 15 (12.6) | 40 (50.4) |
| time pressure | 57 (49.6) | 25 (21.7) | 82 (71.3) |
| Shift work | 42 (36.2) | 18 (15.5) | 60 (51.7) |
| Burden at the locomotor system during the last 7 days | |||
| neck complaints | 67 (41.9) | 18 (11.3) | 85 (53.1) |
| thoracic spine | 47 (54.0) | 17 (38.6) | 64 (48.9) |
| lumbar spine | 59 (39.3) | 17 (11.3) | 76 (50.7) |
| shoulder complaints | 67 (41.6) | 20 (12.4) | 87 (54.0) |
| Resilience-Factors (resources) | Stressed mean (SD) | Non-stressed mean (SD) | Total mean (SD) |
| satisfaction of health status | 3.31 (0.98) | 2.45 (1.02) | 3.0 (1.08) |
| Importance to improve status of health | 1.85 (1.05) | 2.27 (1.32) | 2.0 (1.17) |
| nutritional behavior | 2.90 (0.90) | 2.75 (1.10) | 2.84 (1.0) |
| frequency of breakfast | 2.40 (1.38) | 2.39 (1.54) | 2.39 (1.42) |
| frequency of being calm and relaxed | 3.20 (1.12) | 2.33 (1.04) | 2.89 (1.15) |
| frequency of being full of energy | 3.33 (1.01) | 2.70 (0.93) | 3.10 (1.02) |
| stress level | 3.72(1.10) | 2.83 (1.16) | 3.41 (1.20) |
| Psychological factors | |||
| physical well-being | 46.41 (9.36) | 51.75 (6.14) | 48.38 (8.68) |
| psychological well-being | 41.49 (10,72) | 53.47 (5,53) | 45.92 (10.81) |
| SSCS-value | 24.93 (7.37) | 7.99 (4.06) | 18.76 (10.36) |
| pattern G | 19.67 (29.63) | 40.08(40.59) | 27.49 (35.47) |
| pattern S | 29.36 (36.17) | 43.33 (41.95) | 34.71 (28.87) |
| pattern A | 23.67 (32.29) | 11.54 (25.20) | 19.03 (30.22) |
| pattern B | 27.26 (35.18) | 5.03 (14.48) | 18.74 (30.90) |
| Variables | Step 1 | Step 2 | Step 3 | Step 4 | ||||
|---|---|---|---|---|---|---|---|---|
| B | ß | B | ß | B | ß | B | ß | |
| 1. Block I: Physical burdens | ||||||||
| 1.1 heavy physical tasks | −4.629 | −0.204 | 0.977 | 0.043 | 2.528 | 0.112 | 4.925 | 0.217 |
| 1.2 awkward posture | −1.036 | −0.048 | −1.647 | −0.076 | −2.050 | −0.094 | −0.887 | −0.041 |
| 1.3 lifting heavy loads | −4.028 | −0.185 | −5.404 | −0.249 | −2.762 | −0.127 | −3.582 | −0.15 |
| 1.4 holding heavy loads | −0.627 | −0.030 | 0.678 | 0.033 | −1.294 | −0.062 | −3.928 | −0.189 |
| 1.5 standing | 0.916. | 0.043 | 3.212 | 0.150 | 3.148 | 0.147 | 6.381 * | 0.297 |
| 1.6 physical well-being | −0.461 ** | −0.352 | −0.372 ** | −0.285 | −0.354 ** | −0.271 | 0.128 | 0.098 |
| 2. Block II: Psychological burdens | ||||||||
| 2.1 mental well-being | −0.437 *** | −0.285 | −0.341 *** | −0.360 | 0.117 | 0.123 | ||
| 2.2 pressure of time | −3.690 | −0.153 | −2.464 | −0.10 | −7.619 ** | −0.316 | ||
| 2.3 pressure to perform | 0.937 | 0.044 | 1.095 | −0.05 | 5.279 * | 0.246 | ||
| 2.4 deadline pressure | −1.857 | −0.088 | −2.679 | −0.128 | −2.770 | −0.132 | ||
| 2.5 shift work | −2.908 | −0.139 | −1.963 | −0.094 | −3.728 | −0.178 | ||
| 3. Block III: Patterns of work-related behavior and experience | ||||||||
| 3.1 pattern A | 0.080 * | 0.220 | 0.062 | 0.170 | ||||
| 3.2 pattern B | 0.121 ** | 0.361 | 0.122 * | 0.3363 | ||||
| 3.3 pattern S | excluded | excluded | ||||||
| 3.4 pattern G | 0.051 | 0.168 | 0.039 | 0.127 | ||||
| 4. Block IV: Resilience factors | ||||||||
| 4.1 satisfaction of health condition | 3.463 | 0.37 | ||||||
| 4.2 frequency of being calm and relaxed | 2.162 | 0.250 | ||||||
| 4.3 stress-level | 0.859 | 0.01 | ||||||
| 4.4 frequency of having breakfast | 2.32 | 0.202 | ||||||
| 4.5 nutritional behavior | −0.94 | −0.029 | ||||||
| 4.6 frequency of being full of energy | 0.295 | 0030 | ||||||
| R2 | 0.376 ** | 0.553 *** | 0.631 * | 0.759 ** | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wollesen, B.; Hagemann, D.; Pabst, K.; Schlüter, R.; Bischoff, L.L.; Otto, A.-K.; Hold, C.; Fenger, A. Identifying Individual Stressors in Geriatric Nursing Staff—A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 3587. https://doi.org/10.3390/ijerph16193587
Wollesen B, Hagemann D, Pabst K, Schlüter R, Bischoff LL, Otto A-K, Hold C, Fenger A. Identifying Individual Stressors in Geriatric Nursing Staff—A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2019; 16(19):3587. https://doi.org/10.3390/ijerph16193587
Chicago/Turabian StyleWollesen, Bettina, Diane Hagemann, Katharina Pabst, Ramona Schlüter, Laura L. Bischoff, Ann-Kathrin Otto, Carolin Hold, and Annika Fenger. 2019. "Identifying Individual Stressors in Geriatric Nursing Staff—A Cross-Sectional Study" International Journal of Environmental Research and Public Health 16, no. 19: 3587. https://doi.org/10.3390/ijerph16193587
APA StyleWollesen, B., Hagemann, D., Pabst, K., Schlüter, R., Bischoff, L. L., Otto, A. -K., Hold, C., & Fenger, A. (2019). Identifying Individual Stressors in Geriatric Nursing Staff—A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 16(19), 3587. https://doi.org/10.3390/ijerph16193587