Linkages between Respiratory Symptoms in Women and Biofuel Use: Regional Case Study of Rajasthan, India

 ,
, 
Abstract
:1. Introduction
1.1. Background on the Link between Cooking Fuel and Respiratory Symptoms Globally
1.2. Problem Statement: Biofuel Use and Respiratory Symptoms in Rajasthan
1.3. Study Objectives
2. Materials and Methods
2.1. Survey Overview
2.2. Sampling
2.3. Linkages and Associations to Explore
2.4. District Level Survey
3. Results
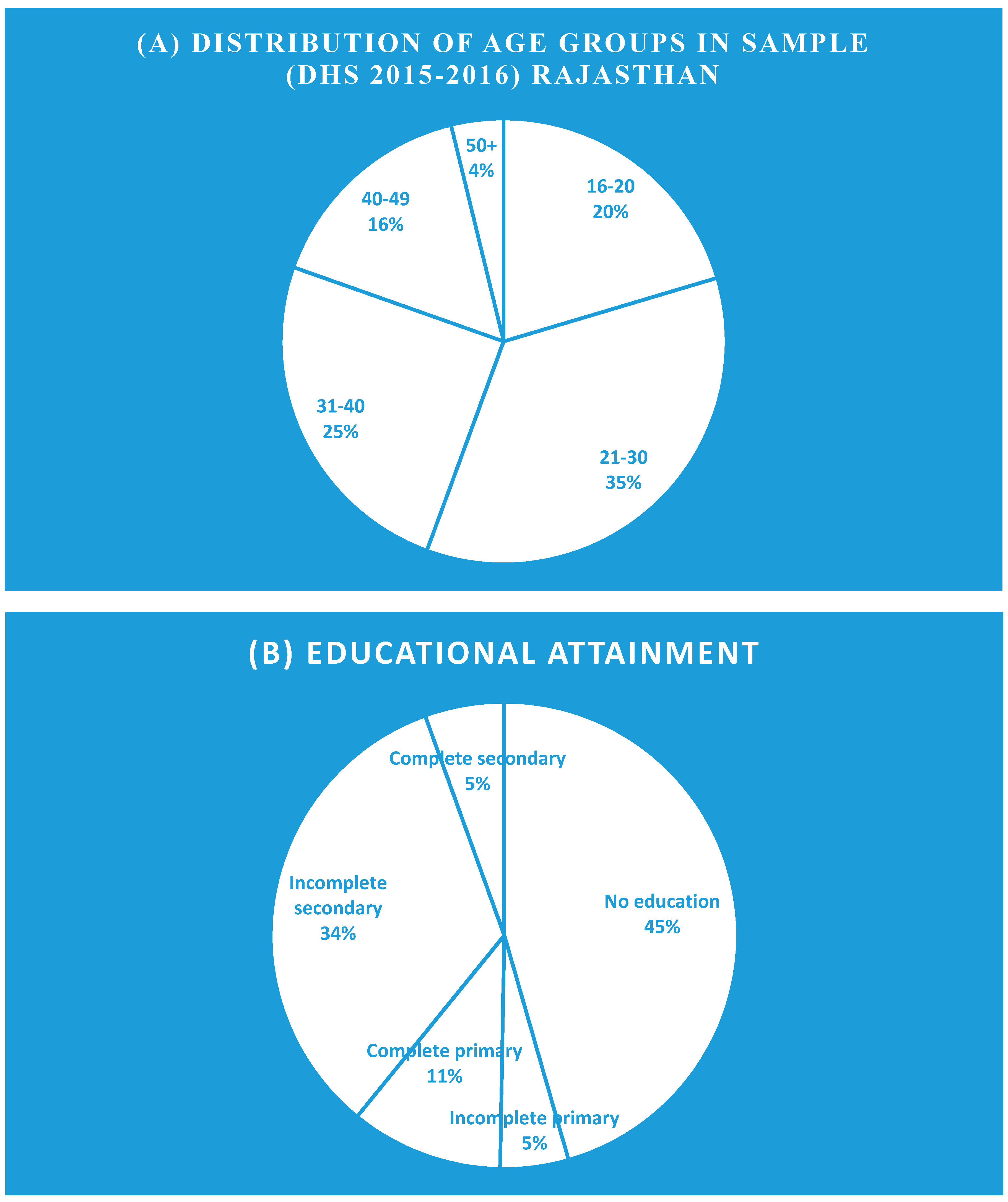
3.1. Demographic and Health Survey (DHS) Results
Descriptive for the Sample
3.2. Household Questionnaires
3.2.1. Socioeconomic Characteristics
3.2.2. Cooking Fuel Consumption Patterns
3.2.3. Cooking Fuel vs. Prevalence of Respiratory Symptoms
3.2.4. Cooking Fuel vs. Socioeconomic Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Singh, D.; Pachauri, S.; Zerriffi, H. Environmental payoffs of LPG cooking in India. Environ. Res. Lett. 2017, 12, 115003. Available online: https://iopscience.iop.org/article/10.1088/1748-9326/aa909d/meta (accessed on 27 October 2017). [CrossRef] [Green Version]
- Kar, A.; Zerriffi, H. From cookstove acquisition to cooking transition: Framing the behavioural aspects of cookstove interventions. Energy Res. Soc. Sci. 2018, 42, 23–33. [Google Scholar] [CrossRef]
- Behera, D.; Jindal, S.K. Respiratory Symptoms in Indian Women Using Domestic Cooking Fuels. Chest 1991, 100, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Tuladhar, B.; Bajracharya, K.; Pillarisetti, A. Assessment of effectiveness of improved cook stoves in reducing indoor air pollution and improving health in Nepal. Energy Sustain. Dev. 2012, 16, 406–414. [Google Scholar] [CrossRef]
- Saksena, S.; Singh, P.B.; Prasad, R.K.; Prasad, R.; Malhotra, P.; Joshi, V.; Patil, R.S. Exposure of infants to outdoor and indoor air pollution in low-income urban areas—A case study of Delhi. J. Expo. Sci. Environ. Epidemiol. 2003, 13, 219–230. [Google Scholar] [CrossRef] [PubMed]
- OECD/International Energy Agency. Global Energy Outlook 2018. Available online: https://webstore.iea.org/world-energy-outlook-2018 (accessed on 13 November 2018).
- Bansal, M.; Saini, R.P.; Khatod, D.K. Development of cooking sector in rural areas in India—A review. Renew. Sustain. Energy Rev. 2013, 17, 44–53. [Google Scholar] [CrossRef]
- The International Renewable Energy Agency (IRENA). Global Bioenergy: Supply and demand projections – A working paper for Remap 2030. 2014. Available online: https://www.irena.org/-/media/Files/IRENA/Agency/Publication/2014/IRENA_REmap_2030_Biomass_paper_2014.pdf (accessed on 2 May 2014).
- Prasad, R.; Garg, R.; Hosmane, G.B. Biomass fuel exposure and respiratory diseases in India. Biosci. trends. 2012, 6, 219–228. [Google Scholar] [CrossRef] [Green Version]
- Government of India (GOI). Pradhan Mantri Ujjawala Yojana, Ministry of Petroleum and Natural Gas. 2016. Available online: https://pmuy.gov.in/ (accessed on 2 June 2016).
- Parikh, J.; Smith, K.; Laxmi, V. Indoor Air Pollution: A Reflection on Gender Bias. Econ. Political Wkly. 1999, 34, 539–544. [Google Scholar]
- Laxmi, V.; Parikh, J.; Karmakar, S.; Dabrase, P. Household energy, women’s hardship and health impacts in rural Rajasthan, India: Need for sustainable energy solutions. Energy Sustain. Dev. 2003, 7, 50–68. [Google Scholar] [CrossRef]
- Smith, K.R. Fuel combustion, air pollution exposure, and health: The situation in developing countries. Annu. Rev. Energy Environ. 1993, 18, 529–566. [Google Scholar] [CrossRef]
- Po, J.Y.; FitzGerald, J.M.; Carlsten, C. Respiratory disease associated with solid biomass fuel exposure in rural women and children: Systematic review and meta-analysis. Thorax 2011, 66, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Dutt, D.; Srinivasa, D.K.; Rotti, S.B.; Sahai, A.K. Effect of indoor air pollution on the respiratory system of women using different fuels for cooking in an urban slum of Pondicherry. Natl. Med J. India. 1996, 9, 113–117. [Google Scholar] [PubMed]
- IHME. The burden of chronic respiratory diseases and their heterogeneity across the state of India: The Global Burden of Disease Study 1990–2016. Lancet Glob. Health. 2018, 6, e1363–e1374. [Google Scholar] [CrossRef]
- Thurber, M.C.; Phadke, H.; Nagavarapu, S.; Shrimali, G.; Zerriffi, H. ‘Oorja’in India: Assessing a large-scale commercial distribution of advanced biomass stoves to households. Energy Sustain. Dev. 2014, 19, 138–150. [Google Scholar] [CrossRef] [PubMed]
- Gould, C.F.; Urpelainen, J. LPG as a clean cooking fuel: Adoption, use, and impact in rural India. Energy Policy 2018, 122, 395–408. [Google Scholar] [CrossRef]
- Menghwani, V.; Zerriffi, H.; Dwivedi, P.; Marshall, J.D.; Grieshop, A.; Bailis, R. Determinants of Cookstoves and Fuel Choice Among Rural Households in India. EcoHealth 2019, 16, 21–60. [Google Scholar] [CrossRef] [PubMed]
- Kaul, N.; Gupta, A.B.; Khandelwal, S.; Singh, G.; Singh, V. An International Impact of exposure to cooking—generated air pollution on human respiratory health: A case study of different microenvironments of India. Hum. Ecol. Risk Assess. 2017, 23, 1989–2001. [Google Scholar] [CrossRef]
- Padhi, B.K.; Adhikari, A.; Satapathy, P.; Patra, A.K.; Chandel, D.; Panigrahi, P. Predictors and respiratory depositions of airborne endotoxin in homes using biomass fuels and LPG gas for cooking. J. Expo. Sci. Environ. Epidemiol. 2017, 27, 112. [Google Scholar] [CrossRef]
- Kowsari, R.; Zerriffi, H. Three dimensional energy profile: A conceptual framework for assessing household energy use. Energy Policy 2011, 7505–7517. [Google Scholar] [CrossRef]
- Office of the Registrar and Census Commissioner, Government of India. 2011 Census of India. Available online: https://censusindia.gov.in (accessed on 12 April 2019).
- Nerini, F.F.; Tomei, J.; To, L.S.; Bisaga, I.; Parikh, P.; Black, M.; Borrion, A.; Spataru, C.; Broto, V.C.; Anandarajah, G.; et al. Mapping synergies and trade-offs between energy and the Sustainable Development Goals. Nature Energy 2018, 3, 10–15. [Google Scholar] [CrossRef]
- Vart, P.; Jaglan, A.; Shafique, K. Caste-based social inequalities and childhood anemia in India: Results from the National Family Health Survey (NFHS) 2005–2006. BMC Public Health 2015, 15. Available online: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-015-1881-4 (accessed on 5 June 2015). [CrossRef] [PubMed]
- NSSO, National Sample Survey Office (NSSO). Energy Sources of Indian Households for Cooking and Lighting. 2010. Available online: http://www.mospi.gov.in/sites/default/files/publication_reports/nss_Report-542.pdf (accessed on 30 September 2012).
- Balakrishnan, K.; Ghosh, S.; Ganguli, B.; Sambandam, S.; Bruce, N.; Barnes, D.; Smith, K. State and national household concentrations of PM2.5 from solid cookfuel use: Results from measurements and modeling in India for estimation of the global burden of disease. Environ. Health 2013, 12. Available online: https://ehjournal.biomedcentral.com/articles/10.1186/1476-069X-12-77 (accessed on 11 September 2013). [CrossRef] [PubMed]
- Sehjpal, R.; Ramji, A.; Soni, A.; Kumar, A. Going beyond incomes: Dimensions of cooking energy transitions in rural India. Energy 2014, 68, 470–477. [Google Scholar] [CrossRef]
- Demographic Health Survey (DHS). India National Family Health Survey (NFHS-4), 2015–2016; DHS: Mumbai, India, 2015. [Google Scholar]
- Balakrishnan, K.; Sankar, S.; Parikh, J.; Padmavathi, R.; Srividya, K.; Venugopal, V.; Pandey, V.L. Daily average exposures to respirable particulate matter from combustion of biomass fuels in rural households of Southern India. Environ. Health Perspect. 2002, 110, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- Hobson, M.; Thistlethwaite, G. Emission factors program task 7—Review of residential and small-scale commercial combustion sources. In Report to the Department for Environment; Food and Rural Affairs; the National Assembly of Wales; The Scottish Executive and the Department of Environment in Northern Ireland: London, UK, 2003. [Google Scholar]
- Puzzolo, E.; Pope, D.; Stanistreet, D.; Rehfuess, E.A.; Bruce, N.G. Clean fuels for resource-poor settings: A systematic review of barriers and enablers to adoption and sustained use. Environ. Res. 2016, 146, 218–234. [Google Scholar] [CrossRef] [PubMed]
- Medical Research Council (MRC). Questionnaire on Respiratory Symptoms. Available online: https://mrc.ukri.org/documents/pdf/questionnaire-on-respiratory-symptoms-1986 (accessed on 1 September 2018).
- Bildirici, M.E. Economic growth and biomass energy. Biomass Bioenergy 2012, 50, 19–24. [Google Scholar] [CrossRef]
- Fullerton, D.G.; Bruce, N.; Gordon, S.B. Indoor air pollution from biomass fuel smoke is a major health concern in the developing world. Trans. R. Soc. Trop. Med. Hyg. 2008, 102, 843–851. [Google Scholar] [CrossRef] [Green Version]
- Pandey, V.L.; Chaubal, A. Comprehending household cooking energy choice in rural India. Biomass Bioenergy 2011, 35, 4724–4731. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| State/Union Territory | With Electricity | Using Solid Fuel for Cooking |
|---|---|---|
| Punjab | 99.6 | 92.9 |
| Rajasthan | 91.0 | 67.8 |
| Himachal Pradesh | 99.5 | 62.5 |
| Uttarakhand | 97.5 | 48.1 |
| Haryana | 98.8 | 47.4 |
| Delhi | 99.8 | 1.6 |
| Jammu and Kashmir | 97.4 | 41.5 |
| Chandigarh | 99.6 | 4.1 |
| Source | df1 | df2 | Wald F | Sig. |
|---|---|---|---|---|
| Model | 12.000 | 1491.000 | 892.557 | 0.001 |
| (Intercept) | 1.000 | 1502.000 | 290.149 | 0.001 |
| Fuel (Z-score) | 1.000 | 1502.000 | 18.621 | 0.001 |
| Edu (Z-score) | 5.000 | 1498.000 | 54.716 | 0.001 |
| Age (Z-score) | 6.000 | 1497.000 | 1659.738 | 0.001 |
| R Square | 0.253 | |||
| Cough = (Intercept) + Fuel + Education + Age | ||||
| Disease Symptoms | Cooking Fuels | ||||
|---|---|---|---|---|---|
| All (N = 26) | Clean Fuel (N = 6) | Wood (N = 18) | Crop Residues (N = 2) | ||
| Duration time | Less than 5 days | 3 (11.5%) | 0 | 3 (11.5%) | 0 |
| 5–10 days | 3 (11.5%) | 1(3.8%) | 1 (3.8%) | 1 (3.8%) | |
| 10–30 days | 6 (23.1%) | 2 (7.7%) | 3 (11.5%) | 1 (3.8%) | |
| 1–3 months | 10 (38.5%) | 3 (11.5%) | 7 (27.0%) | 0 | |
| 3–6 months | 4 (15.4%) | 0 | 4 (15.4%) | 0 | |
| Cough in one day (%) | Less than 25% | 15 (57.7%) | 4 (15.4%) | 11(42.3%) | 0 |
| 25–50% | 5 (19.2%) | 0 | 3 (11.5%) | 2 (7.7%) | |
| More than 50% | 4 (15.4%) | 1 (3.8%) | 3 (11.5%) | 0 | |
| All day | 2 (7.7%) | 1 (3.8%) | 1 (3.8%) | 0 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parikh, P.; Kwami, C.S.; Vivekanand, V.; Paritosh, K.; Lakhanpaul, M. Linkages between Respiratory Symptoms in Women and Biofuel Use: Regional Case Study of Rajasthan, India. Int. J. Environ. Res. Public Health 2019, 16, 3594. https://doi.org/10.3390/ijerph16193594
Parikh P, Kwami CS, Vivekanand V, Paritosh K, Lakhanpaul M. Linkages between Respiratory Symptoms in Women and Biofuel Use: Regional Case Study of Rajasthan, India. International Journal of Environmental Research and Public Health. 2019; 16(19):3594. https://doi.org/10.3390/ijerph16193594
Chicago/Turabian StyleParikh, Priti, Corina Shika Kwami, Vivekanand Vivekanand, Kunwar Paritosh, and Monica Lakhanpaul. 2019. "Linkages between Respiratory Symptoms in Women and Biofuel Use: Regional Case Study of Rajasthan, India" International Journal of Environmental Research and Public Health 16, no. 19: 3594. https://doi.org/10.3390/ijerph16193594
APA StyleParikh, P., Kwami, C. S., Vivekanand, V., Paritosh, K., & Lakhanpaul, M. (2019). Linkages between Respiratory Symptoms in Women and Biofuel Use: Regional Case Study of Rajasthan, India. International Journal of Environmental Research and Public Health, 16(19), 3594. https://doi.org/10.3390/ijerph16193594