One Size Does Not Fit All: A Comprehensive Clinical Approach to Reducing Suicidal Ideation, Attempts, and Deaths


{kind=link}
{kind=link}
Abstract
:1. Introduction to the Problem
2. History of Mental Health and Suicidal Patients
2.1. Psychopharmacology for Suicidal Risk
2.2. Legacy of Mental Health
3. A Fixed Mindset about Suicidal Patient Care?
4. Key Developments That May Be Changing Our Mindset
4.1. Stabilization Planning
4.2. Caring Contact Follow Up
4.3. Lived Experience Perspective
Lived Experience Peer-Support Movement
4.4. Suicide-Specific Policy Developments
4.4.1. Joint Commission Sentinel Event Alerts
4.4.2. Zero Suicide
4.4.3. Recommended Standard Care
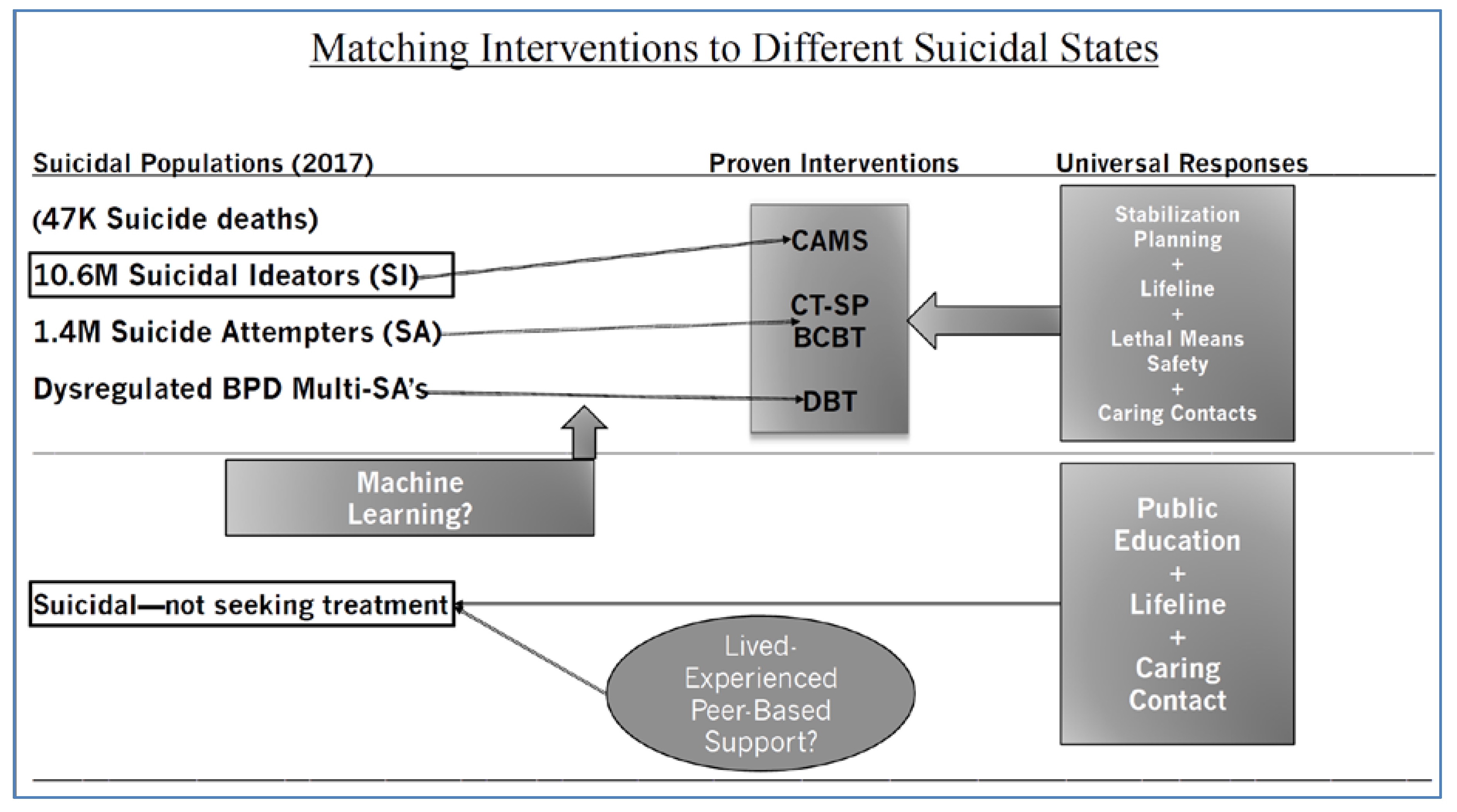
5. The Pursuit of Suicidal Typologies
Machine Learning
6. Effective Clinical Treatments for Suicidal Risk
6.1. Dialectical Behavior Therapy
6.2. Cognitive Therapy for Suicide Prevention
6.3. Brief Cognitive Behavior Therapy
6.4. The Collaborative Assessment and Management of Suicidality
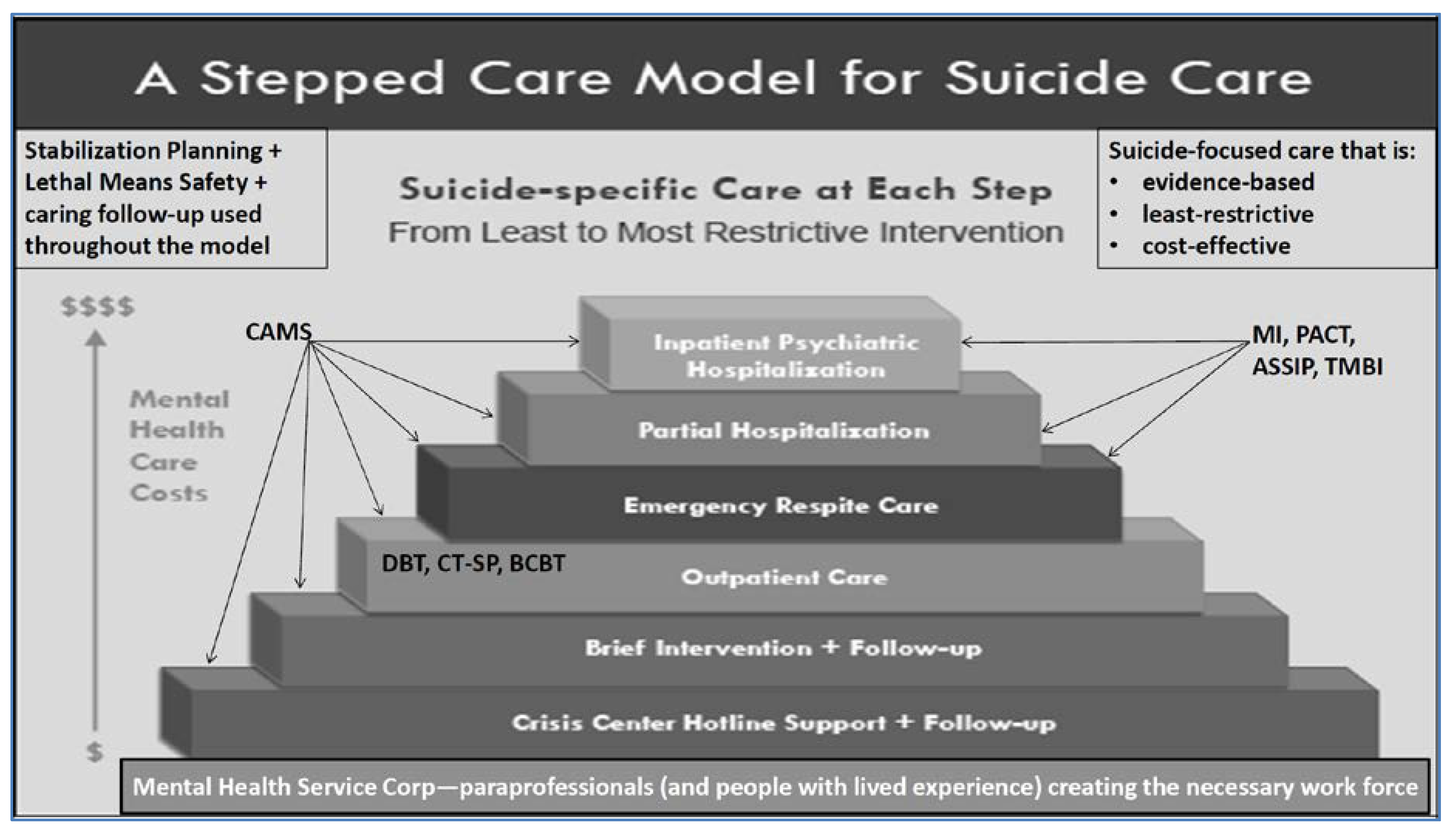
7. A Stepped Care Public Health Model
7.1. Suicidal People Who Do Not Seek Mental Health Care
7.2. Matching Different Treatments to Different Suicidal People
8. Summary and Conclusions
Conflicts of Interest
References
- World Health Organization. Suicide Rates (Per 100,000 Population); World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Drapeau, C.W.; McIntosh, J.L. USA Suicide 2017: Official Final Data; Official final data; American Association of Suicidology: Washington, DC, USA, 2018. [Google Scholar]
- Jobes, D.A.; Joiner, T.E. Reflections on suicidal ideation. Crisis J. Crisis Interv. Suicide Prev. 2019, 40, 227–230. [Google Scholar] [CrossRef] [PubMed]
- SAMHSA 2017 study (2018): Center for Behavioral Health Statistics and Quality. Key Substance Use and Mental Health Indicators in the United States: Results from the 2017 National Survey on Drug Use and Health; (HHS Pub. No. SMA 17-5068, NSDUH Series H-53); Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2018. [Google Scholar]
- Farreras, I.G. History of mental illness. In Noba Textbook Series: Psychology; Biswas-Diener, R., Diener, E., Eds.; DEF Publishers: Champaign, IL, USA, 2019. [Google Scholar]
- Micale, M.S. The Salpêtrière in the age of Charcot: An institutional perspective on medical history in the late nineteenth century. J. Contemp. Hist. 1985, 20, 703–731. [Google Scholar] [CrossRef] [PubMed]
- Neustatter, W.L. Modern psychiatry in practice. Ment. Health 1948, 7, 105. [Google Scholar]
- Pagnin, D.; de Queiroz, V.; Pini, S.; Cassa, G.B. Efficacy of ECT in depression: A meta-analytic review. J. ECT 2004, 20, 13. [Google Scholar] [CrossRef]
- Jones, K. Insulin coma therapy in schizophrenia. J. R. Soc. Med. 2000, 93, 147–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, C.; Bschor, T.; Franklin, J.; Baethge, C. Suicides and suicide attempts during long-term treatment with antidepressants: A meta-analysis of 29 placebo-controlled studies including 6934 patients with major depressive disorder. PPS 2016, 85, 171–179. [Google Scholar]
- Cuijpers, P.; de Beurs, D.P.; van Spijker, B.A.; Berking, M.; Andersson, G.; Kerkhof, A.J. The effects of psychotherapy for adult depression on suicidality and hopelessness: A systematic review and meta-analysis. J. Affect. Disord. 2013, 144, 183–190. [Google Scholar] [CrossRef]
- Jakobsen, J.C.; Katakam, K.K.; Schou, A.; Hellmuth, S.G.; Stallknecht, S.E.; Leth-Møller, K.; Iversen, M.; Banke, M.B.; Petersen, I.J.; Klingenberg, S.L.; et al. Selective serotonin reuptake inhibitors versus placebo in patients with major depressive disorder. A systematic review with meta-analysis and Trial Sequential Analysis. BMC Psychiatry 2017, 17, 58. [Google Scholar]
- Zalsman, G.; Hawton, K.; Wasserman, D.; Van Heeringen, K.; Arensman, E.; Sarchiapone, M.; Carli, V.; Höschl, C.; Barzilay, R.; Balazs, J.; et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry 2016, 3, 646–659. [Google Scholar] [CrossRef]
- Murrough, J.W.; Soleimani, L.; DeWilde, K.E.; Collins, K.A.; Lapidus, K.A.; Iacoviello, B.M.; Lener, M.; Kautz, M.; Kim, J.; Stern, J.B.; et al. Ketamine for rapid reduction of suicidal ideation: A randomized controlled trial. Psychol. Med. 2015, 45, 3571–3580. [Google Scholar] [CrossRef]
- Cipriani, A.; Pretty, H.; Hawton, K.; Geddes, J.R. Lithium in the prevention of suicidal behavior and all-cause mortality in patients with mood disorders: A systematic review of randomized trials. Am. J. Psychiatry 2005, 162, 1805–1819. [Google Scholar] [CrossRef] [PubMed]
- Meltzer, H.Y.; Alphs, L.; Green, A.I.; Altamura, A.C.; Anand, R.; Bertoldi, A.; Bourgeois, M.; Chouinard, G.; Islam, M.Z.; et al. Clozapine treatment for suicidality in schizophrenia: International suicide prevention trial (InterSePT). Arch. Gen. Psychiatry 2003, 60, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Hoge, C.W. Suicide reduction and research efforts in service members and veterans—Sobering realities. JAMA Psychiatry 2019, 76, 464–466. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, M.; Farber, B.A. ‘It is never okay to talk about suicide’: Patients’ reasons for concealing suicidal ideation in psychotherapy. Psychother. Res. 2018, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Jobes, D.A.; Au, J.S.; Siegelman, A. Psychological approaches to suicide treatment and prevention. Curr. Treat. Options Psychiatry 2015, 2, 363–370. [Google Scholar] [CrossRef]
- Jobes, D.A. Clinical assessment and treatment of suicidal risk: A critique of contemporary care and CAMS as a possible remedy. Pract. Innov. 2017, 2, 207–220. [Google Scholar] [CrossRef]
- Jobes, D.A. One size does not fit all: Matching empirically proven interventions to different suicidal states. In Proceedings of the American Association of Suicidology, Denver, CO, USA, 24–27 April 2019. [Google Scholar]
- Dweck, C. Mindset: Changing the Way You Think to Fulfil Your Potential; Hachette UK: London, UK, 2012. [Google Scholar]
- Stanley, B.; Brown, G.K. Safety planning intervention: A brief intervention to mitigate suicide risk. Cogn. Behav. Pract. 2012, 19, 256–264. [Google Scholar] [CrossRef]
- Stanley, B.; Brown, G.K.; Brenner, L.A.; Galfalvy, H.C.; Currier, G.W.; Knox, K.L.; Chaudhury, S.R.; Bush, A.L.; Green, K.L. Comparison of the Safety Planning Intervention with Follow-up vs. Usual Care of Suicidal Patients Treated in the Emergency Department. JAMA Psychiatry 2018, 75, 894–900. [Google Scholar] [CrossRef]
- Rudd, M.D.; Joiner, T.E.; Rajab, M.H. Treating Suicidal Behavior: An Effective, Time-Limited Approach; Guilford Press: New York, NY, USA, 2004. [Google Scholar]
- Bryan, C.J.; Corso, K.A.; Neal-Walden, T.A.; Rudd, M.D. Managing suicide risk in primary care: Practice recommendations for behavioral health consultants. Prof. Psychol. Res. Pract. 2009, 40, 148. [Google Scholar] [CrossRef]
- Bryan, C.J.; Mintz, J.; Clemans, T.A.; Burch, T.S.; Leeson, B.; Williams, S.; Rudd, M.D. Effect of crisis response planning on patient mood and clinician decision making: A clinical trial with suicidal US soldiers. Psychiatr. Serv. 2017, 69, 108–111. [Google Scholar] [CrossRef]
- Bryan, C.J.; Mintz, J.; Clemans, T.A.; Leeson, B.; Burch, T.S.; Williams, S.R.; Maney, E.; Rudd, M.D. Effect of crisis response planning vs. contracts for safety on suicide risk in US Army Soldiers: A randomized clinical trial. J. Affect. Disord. 2017, 212, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Rudd, M.D.; Bryan, C.J.; Wertenberger, E.G.; Peterson, A.L.; Young-McCaughan, S.; Mintz, J.; Williams, S.R.; Arne, K.A.; Breitbach, J.; Delano, K.; et al. Brief cognitive-behavioral therapy effects on post-treatment suicide attempts in a military sample: Results of a randomized clinical trial with 2-year follow-up. Am. J. Psychiatry 2015, 172, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Rudd, M.D.; Mandrusiak, M.; Joiner, T.E. The case against no-suicide contracts: The commitment to treatment statement as a practice alternative. J. Clin. Psychol. 2006, 62, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Jobes, D.A. Managing Suicidal Risk: A Collaborative Approach; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Jobes, D.A. Managing Suicidal Risk: Second Edition: A Collaborative Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Motto, J.A.; Bostrom, A.G. A randomized controlled trial of post crisis suicide prevention. Psychiatr. Serv. 2001, 52, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Reger, M.A.; Luxton, D.D.; Tucker, R.P.; Comtois, K.A.; Keen, A.D.; Landes, S.J.; Matarazzo, B.B.; Thompson, C. Implementation methods for the caring contacts suicide prevention intervention. Prof. Psychol. Res. Pr. 2017, 48, 369–377. [Google Scholar] [CrossRef]
- Luxton, D.D.; June, J.D.; Comtois, K.A. Can post discharge follow-up contacts prevent suicide and suicidal behavior? Crisis 2012, 46–47. [Google Scholar] [CrossRef] [PubMed]
- Comtois, K.A.; Kerbrat, A.H.; DeCou, C.R.; Atkins, D.C.; Majeres, J.J.; Baker, J.C.; Ries, R.K. Effect of augmenting standard care for military personnel with brief caring text messages for suicide prevention: A randomized clinical trial. JAMA Psychiatry 2019, 76, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Carey, B. Expert on mental illness reveals her own struggle. New York Times. Available online: http://www.sadag.org/images/pdf/expert%20own%20fight.pdf (accessed on 29 August 2019).
- Hogan, M.F.; Grumet, J.G. Suicide prevention: An emerging priority for health care. Health Aff. 2016, 35, 1084–1090. [Google Scholar] [CrossRef]
- Dimeff, L.A.; Jobes, D.A.; Chalker, S.A.; Piehl, B.M.; Duvivier, L.L.; Lok, B.C.; Zalake, M.S.; Chung, J.; Koerner, K. A novel engagement of suicidality in the emergency department: Virtual Collaborative Assessment and Management of Suicidality. Gen. Hosp. Psychiatry 2018. [Google Scholar] [CrossRef]
- Bruffaerts, R.; Demyttenaere, K.; Hwang, I.; Chiu, W.T.; Sampson, N.; Kessler, R.C.; Alonso, J.; Borges, G.; de Girolamo, G.; de Graaf, R.; et al. Treatment of suicidal people around the world. Br. J. Psychiatry 2011, 199, 64–70. [Google Scholar] [CrossRef] [Green Version]
- Alexander, M.J.; Haugland, G.; Ashenden, P.; Knight, E.; Brown, I. Coping with thoughts of suicide: Techniques used by consumers of mental health services. Psychiatr. Serv. 2009, 60, 1214–1221. [Google Scholar] [CrossRef]
- Allen, M.H.; Carpenter, D.; Sheets, J.L.; Miccio, S.; Ross, R. What do consumers say they want and need during a psychiatric emergency? J. Psychiatr. Pract. 2003, 9, 39–58. [Google Scholar] [CrossRef] [PubMed]
- Aguirre, R.T.P.; Slater, H.M. Suicide postvention as suicide prevention: Improvement and expansion in the United States. Death Stud. 2010, 34, 529–540. [Google Scholar] [CrossRef] [PubMed]
- Begley, M.; Quayle, E. The lived experience of adults bereaved by suicide: A phenomenological study. Crisis 2007, 28, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Force, S.A. The Way Forward: Pathways to Hope, Recovery, and Wellness with Insights from Lived Experience; National Action Alliance for Suicide Prevention: Washington, DC, USA, 2014. [Google Scholar]
- Crisis Now. 2019. Available online: https://crisisnow.com (accessed on 29 August 2019).
- Live Through This. 2019. Available online: https://livethroughthis.org (accessed on 29 August 2019).
- Now Matters Now. 2019. Available online: https://www.nowmattersnow.org (accessed on 29 August 2019).
- MacLean, S.; MacKie, C.; Hatcher, S. Involving people with lived experience in research on suicide prevention. CMAJ 2018, 190, S13–S14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Joint Commission. Sentinel Event Alert: Detecting and treating suicide ideation in all settings. Jt. Comm. 2016, 56, 1–7. [Google Scholar]
- Brodsky, B.S.; Spruch-Feiner, A.; Stanley, B. The zero suicide model: Applying evidence-based suicide prevention practices to clinical care. Front. Psychiatry 2018, 9, 33. [Google Scholar] [CrossRef] [PubMed]
- Zero Suicide. 2019. Available online: https://zerosuicide.sprc.org (accessed on 29 August 2019).
- National Suicide Action Alliance for Suicide Prevention: Transforming Health Systems Initiative Work Group. Recommended Standard Care for People with Suicide Risk: Making Health Care Suicide Safe; Education Development Center, Inc.: Washington, DC, USA, 2018. [Google Scholar]
- Durkheim, E. Suicide: A Study in Sociology, 1987; Spaulding, J.A.; Simpson, G., Translators; Free Press: Glencoe, IL, USA, 1951. [Google Scholar]
- Conrad, A.K.; Jacoby, A.M.; Jobes, D.A.; Lineberry, T.W.; Shea, C.E.; Arnold Ewing, T.D.; Schmid, P.J.; Ellenbecker, S.M.; Lee, J.L.; Fritsche, K.; et al. A psychometric investigation of the suicide status form II with a psychiatric inpatient sample. Suicide Life Threat. Behav. 2009, 39, 307–320. [Google Scholar] [CrossRef] [PubMed]
- Kleiman, E.M.; Turner, B.J.; Fedor, S.; Beale, E.E.; Huffman, J.C.; Nock, M.K. Examination of real-time fluctuations in suicidal ideation and its risk factors: Results from two ecological momentary assessment studies. J. Abnorm. Psychol. 2017, 126, 726. [Google Scholar] [CrossRef] [PubMed]
- Au, J.S. Typologies of Suicidal Patients Based on Suicide Status Form Data. Ph.D. Thesis, The Catholic University of America, Washington, DC, USA, 2019. [Google Scholar]
- Stanley, I.H.; Rufino, K.A.; Rogers, M.L.; Ellis, T.E.; Joiner, T.E. Acute suicidal affective disturbance (ASAD): A confirmatory factor analysis with 1442 psychiatric inpatients. J. Psychiatr. Res. 2016, 80, 97–104. [Google Scholar] [CrossRef]
- Galynker, I.; Yaseen, Z.S.; Cohen, A.; Benhamou, O.; Hawes, M.; Briggs, J. Prediction of suicidal behavior in high risk psychiatric patients using an assessment of acute suicidal state: The suicide crisis inventory. Depress. Anxiety 2017, 34, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Jobes, D.A. The challenge and the promise of clinical suicidology. Suicide Life Threat. Behav. 1995, 25, 437–449. [Google Scholar] [PubMed]
- Kessler, R.C.; Chalker, S.A.; Luedtke, A.R.; Sadikova, E.; Jobes, D.A. A preliminary precision treatment rule for collaborative assessment and management of suicidality relative to enhanced care-as-usual in prompting rapid remission of suicide ideation. Behav. Res. Ther. 2019. [Google Scholar] [CrossRef]
- Bridge, J.A.; Iyengar, S.; Salary, C.B.; Barbe, R.P.; Birmaher, B.; Pincus, H.A.; Ren, L.; Brent, D.A. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: A meta-analysis of randomized controlled trials. JAMA 2007, 297, 1683–1696. [Google Scholar] [CrossRef] [PubMed]
- Gysin-Maillart, A.; Schwab, S.; Soravia, L.; Megert, M.; Michel, K. A novel brief therapy for patients who attempt suicide: A 24-months follow-up randomized controlled study of the attempted suicide short intervention program (ASSIP). PLoS Med. 2016, 13, e1001968. [Google Scholar] [CrossRef] [PubMed]
- Bateman, A.; Fonagy, P. 8-year follow-up of patients treated for borderline personality disorder: Mentalization-based treatment versus treatment as usual. Am. J. Psychiatry 2008, 165, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Linehan, M. Cognitive-Behavioral Treatment for Borderline Personality Disorder; Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- Linehan, M.M.; Comtois, K.A.; Murray, A.M.; Brown, M.Z.; Gallop, R.J.; Heard, H.L.; Korslund, K.E.; Tutek, D.A.; Reynolds, S.K.; Lindenboim, N. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch. Psychiatry 2006, 63, 757–766. [Google Scholar] [CrossRef]
- Linehan, M.M.; Korslund, K.E.; Harned, M.S.; Gallop, R.J.; Lungu, A.; Neacsiu, A.D.; McDavid, J.; Comtois, K.A.; Murray-Gregory, A.M. Dialectical behavior therapy for high suicide risk in individuals with borderline personality disorder: A randomized clinical trial and component analysis. JAMA Psychiatry 2015, 72, 475–482. [Google Scholar] [CrossRef]
- Goldstein, T.R.; Fersch-Podrat, R.K.; Rivera, M.; Axelson, D.A.; Merranko, J.; Yu, H.; Brent, D.A.; Birmaher, B. Dialectical behavior therapy for adolescents with bipolar disorder: Results from a pilot randomized trial. J. Child Adole. Psychopharm. 2015, 25, 140–149. [Google Scholar] [CrossRef]
- Mehlum, L.; Ramberg, M.; Tørmoen, A.J.; Haga, E.; Diep, L.M.; Stanley, B.H.; Miller, A.L.; Sund, A.M.; Grøholt, B. Dialectical behavior therapy compared with enhanced usual care for adolescents with repeated suicidal and self-harming behavior: Outcomes over a one-year follow-up. J. Am. Acad. Child Adole. Psychiatry 2016, 55, 295–300. [Google Scholar] [CrossRef]
- DeCou, C.R.; Comtois, K.A.; Landes, S.J. Dialectical behavior therapy is effective for the treatment of suicidal behavior: A meta-analysis. Behav. Ther. 2019, 50, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.K.; Have, T.T.; Henriques, G.R.; Xie, S.X.; Hollander, J.E.; Beck, A.T. Cognitive therapy for the prevention of suicide attempts: A randomized controlled trial. JAMA 2005, 294, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Kovacs, M.; Weissman, A. Hopelessness and suicidal behavior: An overview. JAMA 1975, 234, 1146–1149. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T. The current state of cognitive therapy: A 40-year retrospective. Arch. Gen. Psychiatry 2005, 62, 953. [Google Scholar] [CrossRef] [PubMed]
- Comtois, K.A.; Jobes, D.A.; O’Connor, S.; Atkins, D.C.; Janis, K.; Chessen, C.; Landes, S.J.; Holen, A.; Yuodelis-Flores, C. Collaborative assessment and management of suicidality (CAMS): Feasibility trial for next-day appointment services. Depress. Anxiety 2011, 28, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Jobes, D.A.; Comtois, K.A.; Gutierrez, P.M.; Brenner, L.A.; Huh, D.; Chalker, S.A.; Ruhe, G.; Kerbrat, A.H.; Atkins, D.C.; Jennings, K.; et al. A randomized controlled trial of the collaborative assessment and management of suicidality versus enhanced care as usual with suicidal soldiers. Psychiatry 2017, 80, 339–356. [Google Scholar] [CrossRef] [PubMed]
- Ryberg, W.; Zahl, P.H.; Diep, L.M.; Landrø, N.I.; Fosse, R. Managing suicidality within specialized care: A randomized controlled trial. J. Affect. Disord. 2019, 249, 112–120. [Google Scholar] [CrossRef]
- Andreasson, K.; Krogh, J.; Wenneberg, C.; Jessen, H.K.L.; Krakauer, K.; Gluud, C.; Thomsen, R.R.; Randers, L.; Nordentoft, M. Effectiveness of dialectical behavior therapy versus collaborative assessment and management of suicidality treatment for reduction of self-harm in adults with borderline personality traits and disorder: A randomized observer-blinded clinical trial. Depress. Anxiety 2016, 33, 520–530. [Google Scholar] [CrossRef] [PubMed]
- Luoma, J.B.; Martin, C.E.; Pearson, J.L. Contact with mental health and primary care providers before suicide: A review of the evidence. Am. J. Psychiatry 2002, 159, 909–916. [Google Scholar] [CrossRef]
- Niederkrotenthaler, T.; Logan, J.E.; Karch, D.L.; Crosby, A. Characteristics of US suicide decedents in 2005–2010 who had received mental health treatment. Psychiatr. Serv. 2014, 65, 387–390. [Google Scholar] [CrossRef]
- Pitman, A.; Osborn, D.P.J. Cross-cultural attitudes to help-seeking among individuals who are suicidal: New perspective for policymakers. Br. J. Psychiatry 2011, 199, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Jobes, D.A.; Gregorian, M.J.; Colborn, V.A. A stepped care approach to clinical suicide prevention. Psychol. Serv. 2018, 15, 243. [Google Scholar] [CrossRef] [PubMed]
- Jobes, D.A.; Kelly, C.A. Growing up in AAS. Presented at the American Association of Suicidology, Phoenix, AZ, USA, 21 April 2017. [Google Scholar]


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jobes, D.A.; Chalker, S.A. One Size Does Not Fit All: A Comprehensive Clinical Approach to Reducing Suicidal Ideation, Attempts, and Deaths. Int. J. Environ. Res. Public Health 2019, 16, 3606. https://doi.org/10.3390/ijerph16193606
Jobes DA, Chalker SA. One Size Does Not Fit All: A Comprehensive Clinical Approach to Reducing Suicidal Ideation, Attempts, and Deaths. International Journal of Environmental Research and Public Health. 2019; 16(19):3606. https://doi.org/10.3390/ijerph16193606
Chicago/Turabian StyleJobes, David A., and Samantha A. Chalker. 2019. "One Size Does Not Fit All: A Comprehensive Clinical Approach to Reducing Suicidal Ideation, Attempts, and Deaths" International Journal of Environmental Research and Public Health 16, no. 19: 3606. https://doi.org/10.3390/ijerph16193606
APA StyleJobes, D. A., & Chalker, S. A. (2019). One Size Does Not Fit All: A Comprehensive Clinical Approach to Reducing Suicidal Ideation, Attempts, and Deaths. International Journal of Environmental Research and Public Health, 16(19), 3606. https://doi.org/10.3390/ijerph16193606