A Community-Based Participatory Action Research for Roma Health Justice in a Deprived District in Spain

 ,
,  ,
, 
Abstract
:1. Introduction
1.1. Antigypsyism and Roma Health Inequities in Spain
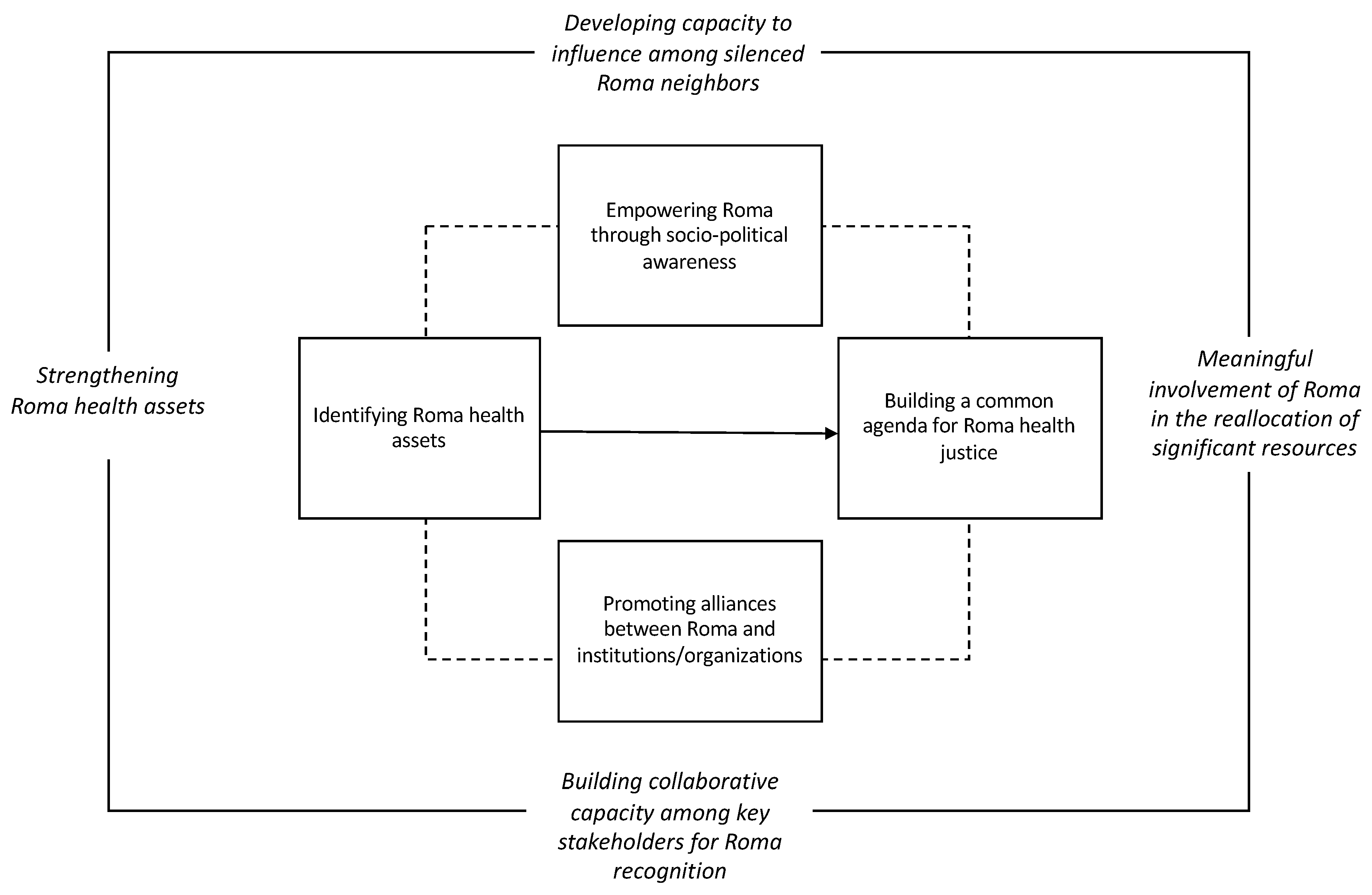
1.2. Roma Health Justice
1.2.1. Strengthening Roma Health Assets
1.2.2. Developing Capacity to Influence among Silenced Roma Neighbors
1.2.3. Building Collaborative Capacity among Key Stakeholders
1.2.4. Meaningful Involvement of Roma in the Reallocation of Significant Resources
1.3. Community-Based Participatory Action Reserach
2. Case Study
2.1. Background
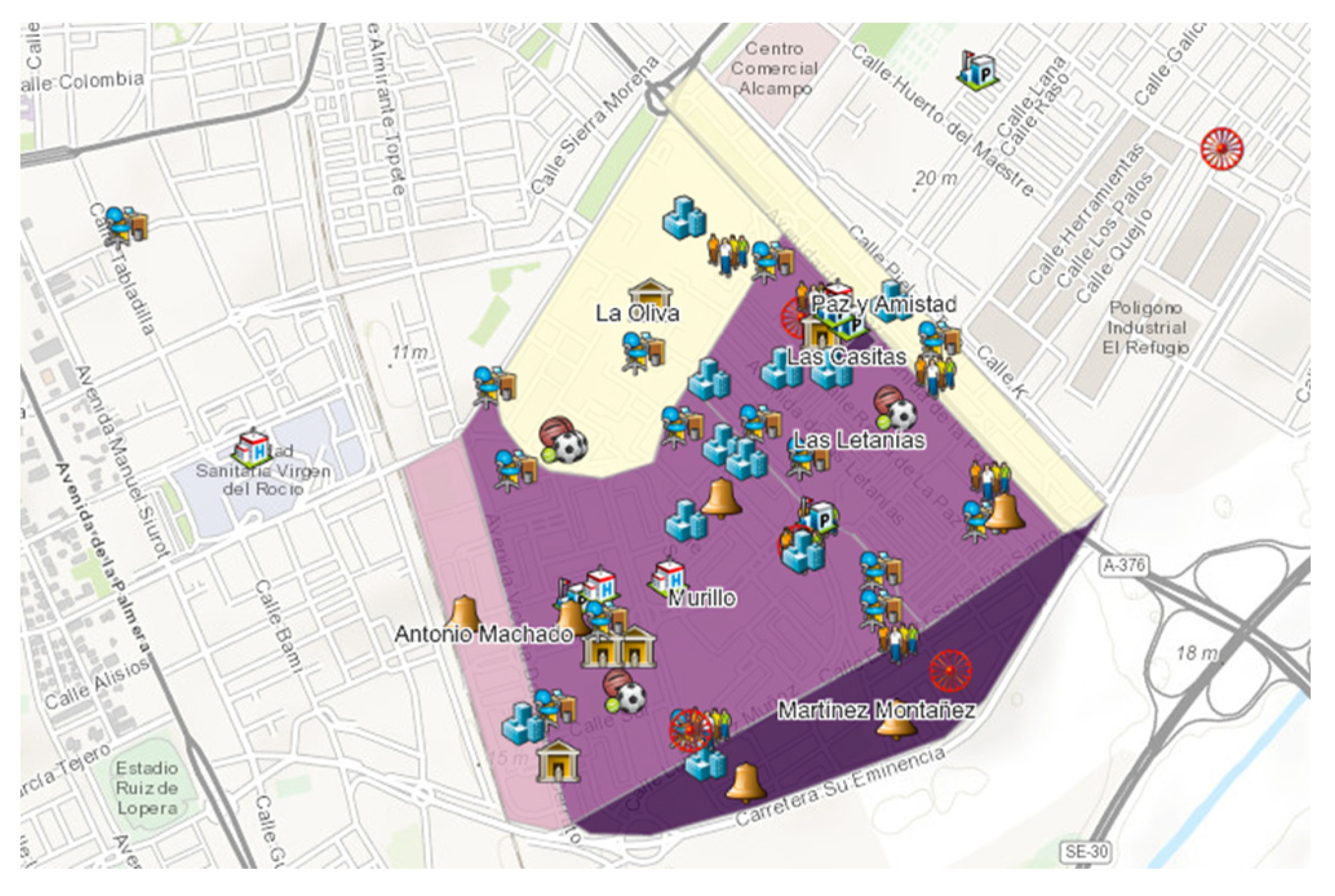
2.1.1. Community Context
2.1.2. The University-Community Partnership
2.2. Participants
2.3. Procedure
2.3.1. Identifying Roma Health Assets
2.3.2. Empowering Roma through Sociopolitical Awareness
2.3.3. Promoting Alliances between Roma and Community Resources/Institutions
2.3.4. Building a Common Agenda for Roma Health Justice
2.4. Results
2.4.1. Identifying Roma Health Assets
2.4.2. Empowering Roma through Sociopolitical Awareness
Unhealthy Public Spaces
Neglect from Public Services
Unlivable Housing Conditions
2.4.3. Promoting Alliances between Roma and Community Resources/Institutions
2.4.4. Building a Common Agenda for Roma Health Justice
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dimension | Questions |
|---|---|
| Use of community resources | How often do you attend these services (list of formal and informal services provided) |
| Level of satisfaction with services | I feel respected |
| My opinions are taken into consideration | |
| I have the opportunity to participate in activities | |
| Activities with Roma are organized | |
| I feel understood | |
| I have problems receiving services | |
| I am satisfied with the service I receive | |
| Professionals are ready to work with Roma community | |
| It is easy to commute to from Poligono Sur |
Appendix B
| Level | Dimension | Questions |
|---|---|---|
| Organizational | Values and goals of the organization | Social justice is an important value in my organization My organization provides opportunities for Roma well-being |
| Accessibility of services | My organization actively identifies accessibility barriers specific to Roma community My organization provides mechanisms to overcome these barriers | |
| Sensitivity towards Roma community | My organization evaluates if its practices are Roma-sensitive My organization registers Roma-specific information My organization provides Roma-specific training My organization adapts its practices to Roma needs My organization evaluates Roma-user satisfaction My organization provides its providers with Roma-specific resources | |
| Participation | My organization includes participatory mechanism for Roma Providers can influence within the organization My organization responds to Roma complaints and/or proposals My organization participates in Roma community activities My organization provides health mediation/mediation services My organization has formal relations with other organizations (if so, which ones) | |
| Personal | Personal value of work | My work is important to me My role is important for organizational functioning |
| Personal level of adaptation | I can adapt my work for Roma needs My organization provides me with information specific for adapting work with Roma My organization provides me with Roma-specific training I am competent when providing services to Roma I have support of other community resources I show appreciation towards Roma when providing services | |
| Sensitivity towards Roma | I value and respect Roma and/or other groups I effectively communicate with Roma users |
References
- European Union Agency for Fundamental Rights. A Persisting Concern: Anti-Gypsyism as a Barrier to Roma Inclusion; Publications Office of the European Union: Luxembourg, 2018. [Google Scholar]
- Council of Europe. Human Rights of Roma and Travellers in Europe; Council of Europe Publications: Strasbourg, France, 2012. [Google Scholar]
- Cook, B.; Wayne, G.F.; Valentine, A.; Lessios, A.; Yeh, E. Revisiting the evidence on health and health care disparities among the Roma: A systematic review 2003–2012. Int. J. Public Health 2013, 58, 885–911. [Google Scholar] [CrossRef] [PubMed]
- Alliance against Antigypsyism. Antigypsyism—A Reference Paper. Available online: http://antigypsyism.eu/wp-content/uploads/2017/07/Antigypsyism-reference-paper-16.06.2017.pdf (accessed on 30 September 2019).
- Brüggemann, C.; Friedman, E. The Decade of Roma Inclusion: Origins, Actors, and Legacies. Eur. Educ. 2017, 49, 1–9. [Google Scholar] [CrossRef]
- Mirga-Kruszelnicka, A. Revisting the EU Roma Framework: Assessing the European Dimension for the Post-2020 Future; Open Society Foundations: Brussels, Belgium, 2017. [Google Scholar]
- Sándor, J.; Kósa, Z.; Boruzs, K.; Boros, J.; Tokaji, I.; McKee, M.; Ádány, R. The decade of Roma Inclusion: Did it make a difference to health and use of health care services? Int. J. Public Health 2017, 62, 803–815. [Google Scholar] [CrossRef] [PubMed]
- Stronks, K.; Toebes, B.; Hendricks, A.; Umar, I.; Sridhard, V. Social Justice and Human Rights as a Framework for Addressing Social Determinants of Health; World Health Organization: Copenhagen, Denmark, 2017. [Google Scholar]
- Marmot, M.; Allen, J.; Bell, R.; Bloomer, E.; Goldblatt, P. WHO European review of social determinants of health and the health divide. Lancet 2012, 380, 1011–1029. [Google Scholar] [CrossRef]
- Van Tongeren, C. Distinctive culture: Framing flamenco artistry in Polígono Sur: El arte de Las Tres Mil by Dominique Abel. J. Span. Cult. Stud. 2017, 18, 169–189. [Google Scholar] [CrossRef]
- Council of Europe. Descriptive Glossary of Terms Relating to Roma Issues; Council of Europe Publications: Strasbourg, France, 2012. [Google Scholar]
- Strochlic, N. Unravelling the Gypsy myth. Ethos Magazine. 2011. Available online: https://www.dailyemerald.com/ethos/archives/unraveling-the-gypsy-myth/article_c0330c1a-effc-5425-b647-95b0ee8d960c.html. (accessed on 30 September 2019).
- Ferrer, F. El estado de salud del pueblo gitano en España. Una revisión de la bibliografía. Gac. Sanit. 2003, 17 (Suppl. 3), 2–8. [Google Scholar] [CrossRef] [PubMed]
- La Parra, D.; Gil-González, D.; Jiménez, A. Los procesos de exclusión social y la salud del pueblo gitano en España. Gac. Sanit. 2013, 27, 385–386. [Google Scholar] [CrossRef]
- Junta de Andalucia. Plan Integral para la Inclusión de la Comunidade Gitana de Andalucia 2017–2020; Junta de Andalucia: Sevilla, Spain, 2017. [Google Scholar]
- Centro de Investigaciones Sociologicios. Percepción de la Discriminación en España; Centro de Investigaciones Sociologicos: Madrid, Spain, 2013. [Google Scholar]
- Blasco, P.G.Y. “It’s the best place for them”: Normalising Roma segregation in Madrid: “It’s the Best Place for them”. Soc. Anthropol. 2016, 24, 446–461. [Google Scholar] [CrossRef]
- Rodríguez-Bailón, R.; Ruiz, J.; Moya, M. The Impact of Music on Automatically Activated Attitudes: Flamenco and Gypsy People. Group Process. Intergroup Relat. 2009, 12, 381–396. [Google Scholar] [CrossRef]
- Escobar-Ballesta, M.; García-Ramírez, M.; de Freitas, C. Taking stock of Roma health policies in Spain: Lessons for health governance. Health Policy 2018, 122, 444–451. [Google Scholar] [CrossRef]
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Segunda Encuesta Nacional de Salud a Población Gitana 2014; Ministerio de Sanidad, Servicios Sociales e Igualdad: Madrid, Spain, 2016. [Google Scholar]
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Estrategia Nacional para la Inclusión Social de la Población Gitana Plan Operativo 2012–2020; Ministerio de Sanidad, Servicios Sociales e Igualdad: Madrid, Spain, 2014. [Google Scholar]
- Legido-Quigley, H.; Otero, L.; Parra, D.L.; Alvarez-Dardet, C.; Martin-Moreno, J.M.; McKee, M. Will austerity cuts dismantle the Spanish healthcare system? BMJ 2013, 346, f2363. [Google Scholar] [CrossRef] [PubMed]
- Sardelić, J. The position and agency of the “irregularized”: Romani migrants as European semi-citizens. Politics 2017, 37, 332–346. [Google Scholar] [CrossRef]
- Aiello, E.; Flecha, A.; Serradell, O. Exploring the Barriers: A Qualitative Study about the Experiences of Mid-SES Roma Navigating the Spanish Healthcare System. Int. J. Environ. Res. Public Health 2018, 15, 377. [Google Scholar] [CrossRef] [PubMed]
- Briones-Vozmediano, E.; la Parra-Casado, D.; Vives-Cases, C. Health Providers’ Narratives on Intimate Partner Violence Against Roma Women in Spain. Am. J. Community Psychol. 2018, 61, 411–420. [Google Scholar] [CrossRef] [PubMed]
- European Union Agency for Fundamental Rights. Poverty and Unemployment: The Case of Roma in 11 EU Member States; Publications Office of the European Union: Luxembourg, 2014. [Google Scholar]
- European Commission. An EU Framework for National Roma Integration Strategies Up to 2020; European Commission: Brussels, Belgium, 2011. [Google Scholar]
- Escobar-Ballesta, M.; García-Ramírez, M.; Albar-Marín, M.J.; Paloma, V. Salud sexual y reproductiva en mujeres gitanas: El programa de planificación familiar del Polígono Sur. Gac. Sanit. 2019, 33, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Vincze, E. The racialization of Roma in the ‘new’ Europe and the political potential of Romani women. Eur. J. Women’s Stud. 2014, 21, 435–442. [Google Scholar] [CrossRef]
- Crowley, N.; Genova, A.; Sansonetti, S. Empowerment of Roma Women within the European Framework for National Roma Integration Strategies; European Parliament: Brussels, Belgium, 2013. [Google Scholar]
- European Commission. 12th Meeting of the European Platform for Roma Inclusion; European Commission: Brussels, Belgium, 2018. [Google Scholar]
- Clavé-Mercier, A.; Olivera, M. Inclusion and the “Arts of Resistance”. Intersections 2018, 4, 2. [Google Scholar] [CrossRef]
- Lewis, S.; Bambra, C.; Barnes, A.; Collins, M.; Egan, M.; Halliday, E.; Orton, L.; Ponsford, R.; Powell, K.; Salway, S.; et al. Reframing ‘participation’ and ‘inclusion’ in public health policy and practice to address health inequalities: Evidence from a major resident led neighbourhood improvement initiative. Health Soc. Care Community 2019, 27, 199–206. [Google Scholar] [CrossRef]
- Wolff, T.; Minkler, M.; Wolfe, S.M.; Berkowitz, B.; Bowen, L.; Dunn Butterfoss, F.; Christens, B.D.; Francisco, V.T.; Himmelman, A.T.; Lee, K.S. Collaborating for equity and justice: Moving beyond collective impact. NPQ 2016, 9, 42–53. [Google Scholar]
- Morgan, A.; Ziglio, E. Revistalising the evidence base for public health: An assets model. Promot. Educ. 2007, 2, 17–22. [Google Scholar] [CrossRef]
- Kretzmann, J.; McKnight, J. Discovering Community Power: Guide to Mobilizing Local Assets and Your Orgazniation’s Capacity; ABCD Institute: Evanston, IL, USA, 2005. [Google Scholar]
- Mathie, A.; Cunningham, G. From clients to citizens: Asset-based Community Development as a strategy for community-driven development. Dev. Pract. 2003, 13, 474–486. [Google Scholar] [CrossRef]
- López, J.; García, R.; Martí, T. Drugs and Mental Health Problems among the Roma: Protective Factors Promoted by the Iglesia Evangélica Filadelfia. Int. J. Environ. Res. Public Health 2018, 15, 335. [Google Scholar] [CrossRef] [PubMed]
- McFadden, A.; Siebelt, L.; Gavine, A.; Atkin, K.; Bell, K.; Innes, N.; Jones, H.; Jackson, C.; Haggi, H.; MacGillivray, S. Gypsy, Roma and Traveller access to and engagement with health services: A systematic review. Eur. J. Public Health 2018, 28, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Roy, M.J. The assets-based approach: Furthering a neoliberal agenda or rediscovering the old public health? A critical examination of practitioner discourses. Crit. Public Health 2017, 27, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Hankivsky, O.; Reid, C.; Cormier, R.; Varcoe, C.; Clark, N.; Benoit, C.; Brotman, S. Exploring the promises of intersectionality for advancing women’s health research. Int. J. Equity Health 2010, 9, 5. [Google Scholar] [CrossRef] [PubMed]
- Crenshaw, K. Mapping the Margins: Intersectionality, Identity Politics, and Violence against Women of Color. Stanford Law Rev. 1991, 43, 1241. [Google Scholar] [CrossRef]
- De Freitas, C.; Martin, G. Inclusive public participation in health: Policy, practice and theoretical contributions to promote the involvement of marginalised groups in healthcare. Soc. Sci. Med. 2015, 135, 31–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fésüs, G.; Östlin, P.; McKee, M.; Ádány, R. Policies to improve the health and well-being of Roma people: The European experience. Health Policy 2012, 105, 25–32. [Google Scholar] [CrossRef]
- Hujo, K. Policy Innovations for Transformative Change; United Nations Research Institute for Social Development: Geneva, Switzerland, 2016. [Google Scholar]
- Tremlett, A.; McGarry, A. Challenges Facing Researchers on Roma Minorities in Contemporary Europe: Notes towards a Research Program; European Centre for Minority Issues: Flensburg, Germany, 2013. [Google Scholar]
- Boyce, T.; Brown, C. Engagement and Participation for Health Equity; World Health Organization: Copenhagen, Denmark, 2017. [Google Scholar]
- Bruner, J. A Narrative Model of Self-Construction. Ann. N. Y. Acad. Sci. 1997, 818, 145–161. [Google Scholar] [CrossRef]
- García-Ramírez, M.; de la Mata, M.L.; Paloma, V.; Hernández-Plaza, S. A Liberation Psychology Approach to Acculturative Integration of Migrant Populations. Am. J. Community Psychol. 2011, 47, 86–97. [Google Scholar] [CrossRef]
- Watts, R.J.; Williams, N.C.; Jagers, R.J. Sociopolitical Development. Am. J. Community Psychol. 2003, 31, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Griffith, D.M.; Mason, M.; Yonas, M.; Eng, E.; Jeffries, V.; Plihcik, S.; Parks, B. Dismantling institutional racism: Theory and action. Am. J. Community Psychol. 2007, 39, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Paloma, V.; Lenzi, M.; Furlanis, N.; Vieno, A.; García-Ramírez, M. Sociopolitical Control for Immigrants: The Role of Receiving Local Contexts. Am. J. Community Psychol. 2018, 62, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Garrido, R.; García-Ramírez, M.; Balcazar, F.E. Community Context in Cultural Competence: Moving towards Community Cultural Competence. Int. J. Intercult. Relat. 2019. (Accepted for Publishing). [Google Scholar]
- Albar-Marín, M.J.; Miranda, D.E. Advocacy for Roma health: In-service training of professionals from the Health District Sevilla. Gac Sanit. 2019. In press 2019. [Google Scholar]
- Dimova, A.; Rohova, M.; Hasardzhiev, S.; Spranger, A. An innovative approach to participatory health policy development in Bulgaria: The conception and first achievements of the Partnership for Health. Health Policy 2018, 122, 81–86. [Google Scholar] [CrossRef]
- Kirwan, G.; Jacob, D. Addressing barriers to healthcare access for Roma: A community development approach. Administration 2016, 64, 157–177. [Google Scholar] [CrossRef] [Green Version]
- McGarry, A.; Agarin, T. Unpacking the Roma Participation Puzzle: Presence, Voice and Influence. J. Ethn. Migr. Stud. 2014, 40, 1972–1990. [Google Scholar] [CrossRef]
- Paloma, V.; García-Ramírez, M.; de la Mata, M. Acculturative integration, self and citizenship construction: The experience of Amal-Andaluza, a grassroots organization of Moroccan women in Andalusia. Int. J. Intercult. Relat. 2010, 34, 101–113. [Google Scholar] [CrossRef]
- Selener, D. Participatory Action Research for Social Change; The Cornell Participatory Action Research Network: Ithaca, NY, USA, 1997; p. 17. [Google Scholar]
- Greenwood, D.; Levin, M. Introduction to Action Research: Social Research for Social Change; SAGE Publishing, Inc.: Thousand Oaks, CA, USA, 2006. [Google Scholar]
- Lykes, M.B. Community-based and participatory action research: Community psychology collaborations within and across borders. In APA Handbook of Community Psychology: Methods for Community Research and Action for Diverse Groups and Issues; Bond, M.A., Serrano-García, I., Keys, C.B., Shinn, M., Eds.; American Psychological Association: Washington, DC, USA, 2017; pp. 43–58. [Google Scholar]
- Suarez-Balcazar, Y.; Early, A.; Maldonado, A.; Garcia, C.P.; Arias, D.; Zeidman, A.; Agudelo-Orozco, A. Community-based participatory research to promote healthy lifestyles among Latino immigrant families with youth with disabilities. Scand. J. Occup. Ther. 2018, 25, 396–406. [Google Scholar] [CrossRef]
- Kovacic, M.; Stigler, S.; Smith, A.; Kidd, A.; Vaughn, L. Beginning a Partnership with PhotoVoice to Explore Environmental Health and Health Inequities in Minority Communities. Int. J. Environ. Res. Public Health 2014, 11, 11132–11151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.; Burris, M.A. Photovoice: Concept, Methodology, and Use for Participatory Needs Assessment. Health Educ. Behav. 1997, 24, 369–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallerstein, N.; Duran, B. Community-Based Participatory Research Contributions to Intervention Research: The Intersection of Science and Practice to Improve Health Equity. Am. J. Public Health 2010, 100, S40–S46. [Google Scholar] [CrossRef] [PubMed]
- Ayuntamiento de Sevilla. Plan Local de Salud de Sevilla 2019/2023; Ayuntamiento de Sevilla: Seville, Spain, 2019. [Google Scholar]
- Casado, D.L.; González, D.G.; Esteve, M.D. The social class gradient in health in Spain and the health status of the Spanish Roma. Ethn. Health 2016, 21, 468–479. [Google Scholar] [CrossRef] [PubMed]
- Maeztu, J. Plan Integral del Polígono Sur; Junta de Andalucia: Seville, Spain, 2006. [Google Scholar]
- Instituto Nacional de Estadisticas. Indicadores Urbanos; Instituto Nacional de Estadisticas: Madrid, Spain, 2017. [Google Scholar]
- García-Ramírez, M. Follow-Up Case Study on the NRIS Spain: Strengthening Roma Engagement in Polígono Sur Through Roma Health Governance; International Organization for Migrations: Brussels, Belgium, 2016. [Google Scholar]
- Suarez-Balcazar, Y.; Harper, G.W.; Lewis, R. An Interactive and Contextual Model of Community-University Collaborations for Research and Action. Health Educ. Behav. 2005, 32, 84–101. [Google Scholar] [CrossRef] [PubMed]
- García-Ramírez, M.; Escobar-Ballesta, M.; Lizana, T. Implementation of the Assessment of the National Roma Integration Strategy and Other National Commitments in the Field of Health in Spain; International Organization for Migrations: Brussels, Belgium, 2015. [Google Scholar]
- García-Ramírez, M.; Paloma, V.; Suarez-Balcazar, Y.; Balcazar, F. Building International Collaborative Capacity: Contributions of Community Psychologists to a European Network. Am. J. Community Psychol. 2009, 44, 116–122. [Google Scholar] [CrossRef] [PubMed]
- McNall, M.; Foster-Fishman, P.G. Methods of Rapid Evaluation, Assessment, and Appraisal. Am. J. Eval. 2007, 28, 151–168. [Google Scholar] [CrossRef]
- Goldman, K.D.; Schmalz, K.J. “Accentuate the Positive!” Using an Asset-Mapping Tool as Part of a Community-Health Needs Assessment. Health Promot. Pract. 2005, 6, 125–128. [Google Scholar] [CrossRef]
- Balcazar, F.E.; Suarez-Balcazar, Y.; Adames, S.B.; Keys, C.B.; García-Ramírez, M.; Paloma, V. A Case Study of Liberation Among Latino Immigrant Families Who Have Children with Disabilities. Am. J. Community Psychol. 2012, 49, 283–293. [Google Scholar] [CrossRef]
- Catalani, C.; Minkler, M. Photovoice: A Review of the Literature in Health and Public Health. Health Educ. Behav. 2010, 37, 424–451. [Google Scholar] [CrossRef]
- Foster-Fishman, P.G.; Law, K.M.; Lichty, L.F.; Aoun, C. Youth ReACT for Social Change: A Method for Youth Participatory Action Research. Am. J. Community Psychol. 2010, 46, 67–83. [Google Scholar] [CrossRef] [PubMed]
- Hmelo, C.E.; Ferrari, M. The Problem-Based Learning Tutorial: Cultivating Higher Order Thinking Skills. J. Educ. Gift. 1997, 20, 401–422. [Google Scholar] [CrossRef]
- Maton, K.I. Empowering Community Settings: Agents of Individual Development, Community Betterment, and Positive Social Change. Am. J. Community Psychol. 2008, 41, 4–21. [Google Scholar] [CrossRef] [PubMed]
- Red Equisastipen. Manual para la Promoción de la Salud en la Comunidad Gitana; Ministerio de Sanidad, Servicios Sociales e Igualdad: Madrid, Spain, 2015. [Google Scholar]
- International Organization for Migrations, Migration Health Division. Equi Health Final Report; International Organization for Migrations: Brussels, Belgium, 2017. [Google Scholar]
- Joshi, A. Legal Empowerment and Social Accountability: Complementary Strategies toward Rights-based Development in Health? World Dev. 2017, 99, 160–172. [Google Scholar] [CrossRef]
- Maton, K.I.; Humphreys, K.; Jason, L.A.; Shinn, M. Community psychology in the policy arena. In APA Handbook of Community Psychology: Methods for Community Research and Action for Diverse Groups and Issues; Bond, M.A., Serrano-García, I., Keys, C.B., Shinn, M., Eds.; American Psychological Association: Washington, DC, USA, 2017; pp. 275–295. [Google Scholar]
- Kegler, M.C.; Rigler, J.; Honeycutt, S. How does community context influence coalitions in the formation stage? A multiple case study based on the Community Coalition Action Theory. BMC Public Health 2010, 10, 90. [Google Scholar] [CrossRef]
- Sprague, C.; Scanlon, M.L.; Pantalone, D.W. Qualitative Research Methods to Advance Research on Health Inequities Among Previously Incarcerated Women Living with HIV in Alabama. Health Educ. Behav. 2017, 44, 716–727. [Google Scholar] [CrossRef] [PubMed]





| Question | Quotes |
|---|---|
| What experiences do you have working with the local Roma population? | “We try to work with the Roma community because it is a priority in the Poligono Sur, and we understand that they have particular needs […] we are conscious that we lack mediation to better understand them, it is challenging.” “The ‘I am a social victim’ is a persistent problem of the population here. ‘By being a gypsy I have a right to everything’, and this is not the reality. Because there are non-Roma people who have much greater needs and we have to be provider in a wide spectrum. We are familiar with the Roma handicaps and obviously need to help […]” |
| Are their Roma-specific services? | “There are many local Roma non-governmental organizations however they are exclusive to only part of the Roma community so their services are not accessible to everyone who could be taking advantage of them” “[…] coordination is good with all community-based organizations, but many Roma organizations do mediation. When there is a real problem [with Roma] there is a lot of personal involvement then there can be no impartiality” |
| How would you describe the living conditions of local Roma population? | “There are many houses that are overcrowded, meaning that 3 or 4 generations are living together. They have done extensions to the original house […] they are looking for, as it is logical and normal, a way to survive.” “And here that happens very often […] many children with substance abuse problems use the pension [of elderly family member] for consumption.” “Because although these are apartment building, we consider them as vertical settlements […]” |
| Modules | Topics | Field Notes of Provider Discussion |
|---|---|---|
| History and culture of Roma population | Roma history Cultural identity Social demographics | Providers attribute Roma health problems to culture and health practices, homogenizing group needs. |
| Roma health | Health diagnostics Health inequities | Providers begin to discuss marginalization as the main problem, questioning initial attribution to culture. Neglect of public spaces as a general concern for health issues. |
| Roma health and Spanish healthcare system | Cultural differences between Roma and healthcare system Structure and coverage of the healthcare system National Roma integration strategies health component | Blaming individualized habits of Roma. Structural issues are identified (e.g., lack of provider continuity in healthcare center) and no available resources to improve services for Roma. Providers did not have knowledge about Roma health policies. |
| Strategies to facilitate intervention | Peer mentoring Mediation Cultural competences* | Providers identified their own good practices when responding to local Roma needs. Identified frustrations due to lack of organizational support and the need to adapt their practices to local needs. |
| Health promotion with Roma community | Health education for Roma community Health accompaniment Intersectoral work Community networking Roma participation | Agreed that collaboration with Roma organizations and Roma neighbors was an action that could help improve local health outcomes. |
| Content | Neighbor Proposal | Agreement/Recommendations |
|---|---|---|
| (1) Share evidence (resource map and Photovoice) | Increase number of trash bins Raise awareness among others regarding clean spaces Improve frequency and quality of public service | Develop plan to meet with waste management representatives Providers offering navigational support of different institutions and resources within the community |
| (2) Identify allies | Commit to working with health providers and other Roma | Exchange of contact information between Roma and providers |
| (3) Identify opportunities for Roma engagement | Open channels for collaboration with local institutions | Invitation to participate in local health working groups by local policymaker |
| (4) Plan for implementation and sustainability actions | Offer support as Roma advocates within institutions and organizations | Follow-up meeting Continued funding from the Open Society Foundations Roma Initiatives Office |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miranda, D.E.; Garcia-Ramirez, M.; Balcazar, F.E.; Suarez-Balcazar, Y. A Community-Based Participatory Action Research for Roma Health Justice in a Deprived District in Spain. Int. J. Environ. Res. Public Health 2019, 16, 3722. https://doi.org/10.3390/ijerph16193722
Miranda DE, Garcia-Ramirez M, Balcazar FE, Suarez-Balcazar Y. A Community-Based Participatory Action Research for Roma Health Justice in a Deprived District in Spain. International Journal of Environmental Research and Public Health. 2019; 16(19):3722. https://doi.org/10.3390/ijerph16193722
Chicago/Turabian StyleMiranda, Daniela E., Manuel Garcia-Ramirez, Fabricio E. Balcazar, and Yolanda Suarez-Balcazar. 2019. "A Community-Based Participatory Action Research for Roma Health Justice in a Deprived District in Spain" International Journal of Environmental Research and Public Health 16, no. 19: 3722. https://doi.org/10.3390/ijerph16193722
APA StyleMiranda, D. E., Garcia-Ramirez, M., Balcazar, F. E., & Suarez-Balcazar, Y. (2019). A Community-Based Participatory Action Research for Roma Health Justice in a Deprived District in Spain. International Journal of Environmental Research and Public Health, 16(19), 3722. https://doi.org/10.3390/ijerph16193722