Can Asset-Based Community Development with Children and Youth Enhance the Level of Participation in Health Promotion Projects? A Qualitative Meta-Synthesis

Abstract
:1. Introduction
ABCD Strategies
- Relationship oriented. There is a focus on building social networks.
- Asset-based. The process focusses on strengths, resources, and assets.
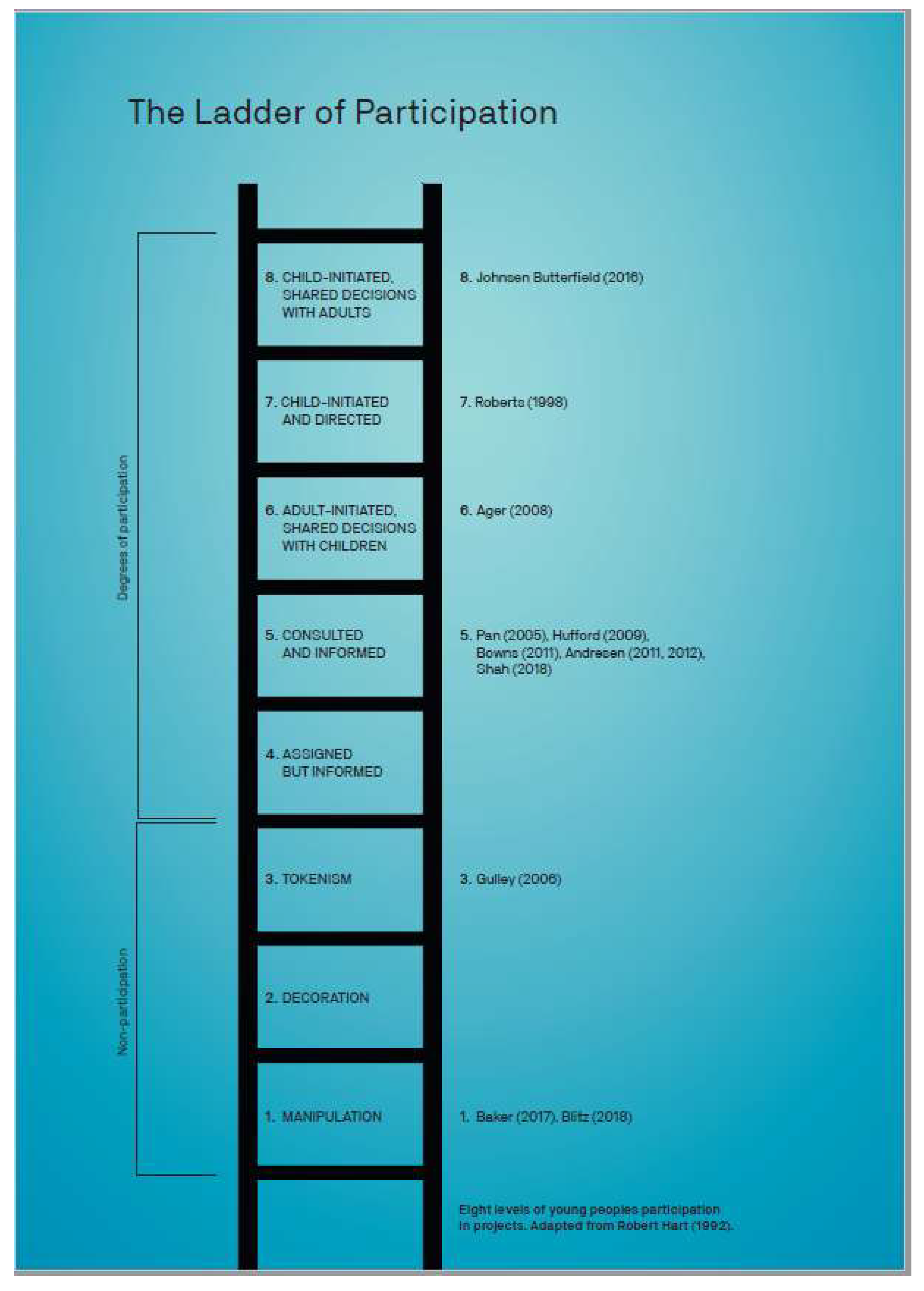
2. Classification of Participation
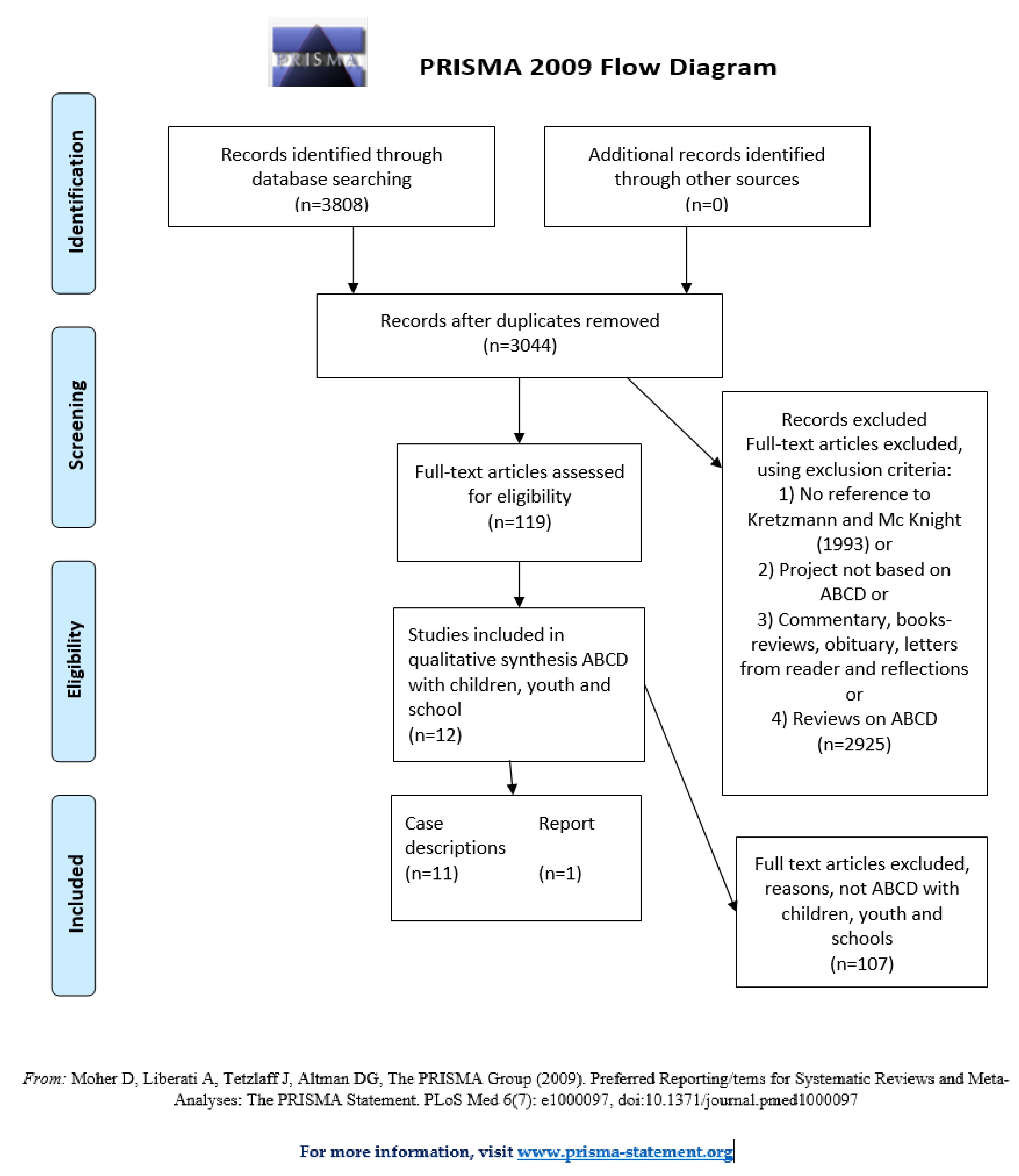
3. Methods and Materials
Some Methodological Challenges in the Included Texts
4. Results
4.1. Pre-School Children
4.2. Elementary School Children
4.3. High School Youth
4.4. Degrees of Adherence to ABCD Principles and Levels of Participation
4.5. Non-Participation and Low Degrees of Adherence to ABCD Principles
4.6. Informed Participation and Partial Adherence to ABCD Principles
4.7. High Level of Participation and Full Adherence to the ABCD Principles
5. Discussion
May the ABCD Approach Enhance Participation in Health Promotion Initiatives?
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Morgan, A.; Ziglio, E.; Davies, M. Health Assets in a Global Context: Theory, Methods, Action; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Wong, N.; Zimmerman, M.; Parker, E. A Typology of Youth Participation and Empowerment for Child and Adolescent Health Promotion. Am. J. Community Psychol. 2010, 46, 100–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, A.; Ziglio, E. Revitalising the evidence base for public health: An assets model. Promot. Educ. 2007, 14, 17–22. [Google Scholar] [CrossRef]
- Department of Health. Real Involvement: Working with People to Improve Health Services; DH London: London, UK, 2008; p. 143.
- Macintyre, S.; Ellaway, A.; Cummins, S. Place effects on health: How can we conceptualise, operationalise and measure them? Soc. Sci. Med. 2002, 55, 125–139. [Google Scholar] [CrossRef]
- Roy, M.J. The assets-based approach: Furthering a neoliberal agenda or rediscovering the old public health? A critical examination of practitioner discourses. Crit. Public Health 2017, 27, 455–464. [Google Scholar] [CrossRef] [PubMed]
- WHO. The Ottawa Charter for Health Promotion. Available online: https://www.who.int/healthpromotion/conferences/previous/ottawa/en/ (accessed on 26 September 2019).
- Marmot, M.; Allen, J.; Goldblatt, P.; Boyce, T.; McNeish, D.; Grady, M.; Geddes, I. The Marmot review: Fair society, healthy lives. In The Strategic Review of Health Inequalities in England Post-2010; Institute of Health Equity: London, UK, 2010. [Google Scholar]
- O’Mara-Eves, A.; Brunton, G.; Mcdaid, D.; Oliver, S.; Kavanagh, J.; Jamal, F.; Matosevic, T.; Harden, A.; Thomas, J. Community engagement to reduce inequalities in health: A systematic review, meta-analysis and economic analysis. Public Health Res. 2013, 1. [Google Scholar] [CrossRef]
- Hauger, B. Styrkebasert Tilnærming i Lokalt Folkehelsearbeid, Innbyggerinvolvering, Myndiggjøring og Deltakelse; Helsedirektoratet: Oslo, Norway, 2018; p. 85. [Google Scholar]
- Foot, J.; Hopkins, T. A Glass Half-Full: How an Asset Approach Can Improve Community Health and Well-Being; Great Britain Improvement and Development Agency: London, UK, 2010. [Google Scholar]
- Dahl, K.A.; Holck-Christiansen, J. Ressourcebaseret Udvikling af Localområder—En Guide til Kortlægning of Mobilisering af Ressourcer i Udsatte Bydele; Socialministeriet: Copenhagen, Danmark, 2006. [Google Scholar]
- Caan, W.; Cassidy, J.; Coverdale, G.; Ha, M.A.; Nicholson, W.; Rao, M. The value of using schools as community assets for health. Public Health 2015, 129, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Johnson Butterfield, A.K.; Yeneabat, M.; Moxley, D.P. “Now I Know My ABCDs”: Asset-Based Community Development with School Children in Ethiopia. Child. Sch. 2016, 38, 199–208. [Google Scholar] [CrossRef]
- Kretzmann, J.P.; McKnight, J.L. Building Communities from the Inside Out: A Path toward Finding & Mobilizing a Community’s Assets; ACTA Publications: Evanston, IL, USA, 1993. [Google Scholar]
- Blickem, C.; Dawson, S.; Kirk, S.; Vassilev, I.; Mathieson, A.; Harrison, R.; Bower, P.; Lamb, J. What is asset-based community development and how might it improve the health of people with long-term conditions? A realist synthesis. SAGE Open 2018, 8. [Google Scholar] [CrossRef]
- Mathie, A.; Cameron, J.; Gibson, K. Asset-based and citizen-led development: Using a diffracted power lens to analyze the possibilities and challenges. Prog. Dev. Stud. 2017, 17, 54–66. [Google Scholar] [CrossRef]
- Rifkin, S.B. Examining the links between community participation and health outcomes: A review of the literature. Health Policy Plan. 2014, 29, ii98–ii106. [Google Scholar] [CrossRef]
- Friedli, L. ‘What we’ve tried, hasn’t worked’: The politics of assets based public health. Crit. Public Health 2013, 23, 131–145. [Google Scholar] [CrossRef]
- MacLeod, M.A.; Emejulu, A. Neoliberalism with a Community Face? A Critical Analysis of Asset-Based Community Development in Scotland. J. Community Pract. 2014, 22, 430–450. [Google Scholar] [CrossRef]
- Harrison, R.; Blickem, C.; Lamb, J.; Kirk, S.; Vassilev, I. Asset-Based Community Development: Narratives, Practice, and Conditions of Possibility—A Qualitative Study with Community Practitioners. SAGE Open 2019, 9. [Google Scholar] [CrossRef]
- Caan, W. Mental health interventions in schools. Lancet Psychiatry 2014, 1, 500. [Google Scholar] [CrossRef]
- Boyd, C.P.; Hayes, L.; Wilson, R.L.; Bearsley-Smith, C. Harnessing the social capital of rural communities for youth mental health: An asset-based community development framework. Aust. J. Rural Health 2008, 16, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Frerichs, L.; Ataga, O.; Corbie-Smith, G.; Tessler Lindau, S. Child and youth participatory interventions for addressing lifestyle-related childhood obesity: A systematic review. Obes. Rev. 2016, 17, 1276–1286. [Google Scholar] [CrossRef] [PubMed]
- Hart, R.A. Stepping back from ‘the ladder’: Reflections on a model of participatory work with children. In Participation and Learning; Reid, A., Jensen, B.B., Nikel, J.V.S., Eds.; Springer: Dordrecht, The Netherlands, 2008; pp. 19–31. [Google Scholar]
- McKnight, J.; Russell, C. The Four Essensial Elements of an Asset-Based Community Development Process, What Is Distinctive about Asset-Based Community Process; Asset-Based Community Development Institute at DePaul University: Chicago, IL, USA, 2018; p. 15. [Google Scholar]
- Percy-Smith, B.; Thomas, N. A Handbook of Children and Young People’s Participation: Perspectives from Theory and Practice; Routledge: London, UK, 2010. [Google Scholar]
- Hart, R. Children’s Participation: From Tokenism to Citizenship; UNICEF International Child Development Centre: Florence, Italy, 1992. [Google Scholar]
- Treseder, P.; Smith, P.G.; Fund, S.T.C.; Office, C.S.R. Empowering Children & Young People: Training Manual: Promoting Involvement in Decision-Making; Save the Children: London, UK, 1997. [Google Scholar]
- Cahill, H.; Dadvand, B. Re-conseptualising youth participation: A framework to inform action. Child. Youth Serv. Rev. 2018, 95, 243–253. [Google Scholar] [CrossRef]
- Mathie, A.; Cunningham, G. Who is driving development? Reflections on the transformative potential of asset-based community development. Can. J. Dev. Stud. 2005, 26, 175–187. [Google Scholar] [CrossRef]
- Stige, B.; Malterud, K.; Midtgarden, T. Towards an Agenda for Evaliation of Qualitative Research. Qual. Health Res. 2009, 19, 1504–1516. [Google Scholar] [CrossRef]
- Ager, R.D.; Parquet, R.; Kreutzinger, S. The youth video project: An innovative program for substance abuse prevention. J. Soc. Work Pract. Addict. 2008, 8, 303–321. [Google Scholar] [CrossRef]
- Blitz, L.W.; Yull, D.; Kufeyani, P.; Wapinski-Mooradian, J. Akuluakulu? Sapasidwa Kanthu (Grown Ups? They Get Nothing): Informing an International Community-University-Partnership in Malawi. Soc. Dev. Issues 2018, 40, 5–16. [Google Scholar]
- Gulley, T. Building community capacity in southwest Virginia. Online J. Rural Nurs. Health Care 2006, 6, 17. [Google Scholar]
- Shah, R.W.; Troester, J.S.; Brooke, R.; Gatti, L.; Thomas, S.L.; Masterson, J. Fostering eABCD: Asset-Based Community Development in Digital Service-Learning. J. High. Educ. Outreach Engagem. 2018, 22, 189–221. [Google Scholar]
- Pan, R.J.; Littlefield, D.; Valladolid, S.G.; Tapping, P.J.; West, D.C. Building Healthier Communities for Children and Families: Applying Asset-Based Community Development to Community Pediatrics. Pediatrics 2005, 115, 1185–1187. [Google Scholar] [CrossRef] [PubMed]
- Baker, I.R.; Dennison, B.A.; Boyer, P.S.; Sellers, K.F.; Russo, T.J.; Sherwood, N.A. An asset-based community initiative to reduce television viewing in New York state. Prev. Med. 2007, 44, 437–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, S.; Dedrick, A.; Mitchell, G. Westlawn Keys to Community. Project Report; Community Building Resources: Spruce Grove, AB, Canada, 1998. [Google Scholar]
- Andresen, W.R. Using an asset-based community development initiative to attract and retain young people. J. Ext. 2011, 9, 1–5. [Google Scholar]
- Andresen, W.R. Evaluating an asset-based effort to attract and retain young people. Community Dev. 2012, 43, 49–62. [Google Scholar] [CrossRef]
- Hufford, L.; West, D.C.; Paterniti, D.A.; Pan, R.J. Community-based advocacy training: Applying asset-based community development in resident education. Acad. Med. 2009, 84, 765–770. [Google Scholar] [CrossRef]
- Bowns, C. Facilitating the Production of Place-Based Knowledge for Participatory Community Development in Rural Pennsylvania. Child. Youth Environ. 2011, 21, 275–292. [Google Scholar]
- Hancock, T.; Minkler, M. Community health assessment or healthy community assessment: Whose community? Whose health? Whose assessment? In Community Organizing and Community Building for Health, 2nd ed.; Minkler, M., Ed.; Rutgers University Press: New Brunswick, NJ, USA, 2011; p. 148. [Google Scholar]
- Ager, R.D.; Parquet, R. Public housing residents making their courtyard safe from drugs. J. Soc. Work Pract. Addict. 2008, 8, 95–115. [Google Scholar] [CrossRef]
- Mathie, A.; Cunningham, G. From clients to citizens: Asset-based Community Development as a strategy for community-driven development. Dev. Pract. 2003, 13, 474–486. [Google Scholar] [CrossRef]
- Raby, R. Children’s Participation as Neo-Liberal Governance? Discourse Stud. Cult. Politics Educ. 2014, 35, 77–89. [Google Scholar] [CrossRef]
- Wallerstein, N.; Duran, B.; Oetzel, J.G.; Minkler, M. Community-Based Participatory Research for Health: Advancing Social and Health Equity; John Wiley & Sons: Hoboken, NJ, USA, 2017. [Google Scholar]
- Forrester, G.; Kurth, J.; Vincent, P.; Oliver, M. Schools as community assets: An exploration of the merits of an Asset-Based Community Development (ABCD) approach. Educ. Rev. 2018, 1–16. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| # | Query |
|---|---|
| S3 | S1 AND S2 |
| S2 | (community or communities or city or cities or town* or village* or neighborhood* or neighborhood* or urban or rural) |
| S1 | (“asset*-based” or “asset* based” or “strength*-based” or “strength* based” or “asset* mapping” or “strength* mapping” or “appreciative inquiry” or “appreciative inquiries”) |
| First Author, Year, Title | Place | Project Aim | Results | Method |
|---|---|---|---|---|
| Ager, R.D. et al. (2008) [33] The Youth Video Project: An Innovative Program for Substance Abuse Prevention | New Orleans, USA | A pilot intervention to connect children with positive role models, enhance community ownership of drug issues, empower the community, use community capacities to lay the groundwork for a longer-term program sustained by the community. By developing a video, youth were to learn about healthy attitudes and behaviors related to substance abuse. | Six activities were identified as critical to the program’s success: Family involvement, community engagement, adapting drug education content to fit community characteristics, using a video camera as a vehicle for community field assignments, and evaluation-based learning. | Qualitative interviews and observation of processes relating to principles of capacity building and cognitive dissonance theory. The quantitative questionnaire, paired t-test with seven participants to test changes in drug attitudes, perceptions, behaviors and knowledge. |
| Andresen, W.R. (2011) [40] Using an Asset-based Community Development Initiative to Attract and Retain Young People | Northern Wisconsin and Michigan, USA | To use ABCD in a small community to attract and retain young people and reverse the region’s population decline. | During the asset mapping phase, few young people indicated that they planned to stay in the region. After their involvement in the project, 78% of participants (all ages) stated that their perception of the community had improved. The project led to a vision for, and steps towards, realizing a nature trail infrastructure, a promotional website and a social media campaign. Continued evaluations will assess population decline changes. | Quantitative survey to identify community features that respondents (668 teenagers and professionals under 40 years) considered to be assets. The author observes and describes the community-based initiative that followed to promote, strengthen and connect young people to the identified assets. |
| Andresen, W.R. (2012) [41] Evaluating an asset-based effort to attract and retain young people. | Northern Wisconsin and Michigan, USA | Evaluation of the use of ABCD in a small community to attract and retain young people and reverse the region’s population decline. | A heightened understanding of local assets led to momentum for their further development, including investments in nature trails and information promotion. These short- and mid-term program results may positively influence long-term population numbers. | Evaluation of the effectiveness of a community-based initiative by qualitative and quantitative methods. Measurement of short-term changes in learning and mid-term changes in action. |
| Baker, I.R. et al. (2007) [38] An asset-based community initiative to reduce television viewing in New York state. | Rural upstate New York, USA | Catalyzing an established asset-based community partnership to support efforts to reduce television viewing. Part of a broader 3-year study to reduce childhood obesity among rural preschool-aged children. | Asset mapping and focus groups led to identifying desirable actions before planning and implementation of activities in two TV turn-off weeks in 2004 and 2005. Forty indoor and outdoor activities for pre-schoolers and families were provided in public venues. A community-sourced action plan can lend strength to childhood obesity interventions and other public health initiatives. | Case study. Observation and documentation of asset mapping of individual and community strengths followed by focus groups to identify desirable actions. The project engaged childcare staff, administrators and directors from 10 childcare facilities serving on average 276 pre-schoolers. |
| Hufford, L. (2009) [42] Applying asset-based community development in resident education | Sacramento, California, USA | Communities and Physicians Together (CPT) at the University of California, has developed a service-learning program teaching ABCD since 1999. Their aim has been to establish collaboration with local communities and enable residents (pediatricians) to become effective community advocates. CPT aims to emphasize identifying and utilizing strengths and building capacity, in contrast to the traditional medical model, which emphasizes deficits and needs. | CPT became a well-established partnership between a pediatric residency program, five community collaboratives located in diverse neighborhoods, and a grassroots child advocacy organization. The CPT curriculum teaches residents to build partnerships with their assigned community throughout three years of training, following the ABCD principles. Residents perform activities designed to provide them with a community member’s perspective and partner with communities to implement a project to improve the health of children in that community. The article provides examples of successful community projects. | Case reports and description of the development of the service-learning program teaching ABCD. Refers to reports from students (resident pediatricians) who participated in the program and a qualitative evaluation that demonstrated residents’ attitudes of their role as pediatricians in the community changed with CPT. |
| Blitz, L.V. et al. (2018) [34] Akuluakulu? Sapasidwa Kanthu (Grown-ups? They Get Nothing): Informing an International Community-University Partnership in Malawi | Rural Malawi | To apply ABCD to establish a university-assisted component of the Malawi Children’s Mission. | ABCD was used as an engagement approach and a set of strategies to identify and mobilize community assets to support guardian that supported orphaned children. Whereas, the project is still in an early stage, an independent network of adults who are invested in the healthy growth of their communities is taking form, and children are, so far, a target group. | Case study—150 orphan children at the Malawi Children’s Mission and their guardians from three rural villages. Interviews and group meetings with community members, village chiefs and staff at the Malawi Children’s Mission. |
| Johnson Butterfield, A.K. et al. (2016) [14] “Now I know my ABCDs”: Asset-Based Community Development with School Children in Ethiopia. | Addis Ababa, Ethiopia | An adult facilitator aimed to assist children who explored how they could advance the quality of life in their communities. The children had participated in an adult-led ABCD project requested their own ABCD process for their low-income community. The project aimed to explore how ABCD methods can address gaps in community assets for children, to produce knowledge for social work educators, students, and practitioners working to involve children in community partnerships. | The children elected their own facilitators, came to appreciate their own and their community’s strengths and formed communities of learning. Using drawings, flip charts, narratives, sociodrama, poems, art and songs, they presented their findings, including local government and school officials. They pinpointed strengths, assets, gaps and solutions, and gained support for initiatives, including a children’s theatre group that enacts sensitive and challenging themes, and outreach to poverty-struck elderly residents. | Case study. The project process was observed and documented, throughout the three-year period, where the number of participants doubled to 100 children aged 7–14. The study documented the process of various subprojects, i.e., involving language development, performing arts and community service. |
| Gulley, T. (2006) [35] Building community capacity in southwest Virginia. | Southwest Virginia, USA | The project aimed to increase social capital in a neighborhood after “Ms. G”, who led the project, introduced the idea and wanted to beautify a wall. The project aims to illustrate how community assets can be recognized, and social capital can be increased. | Children aged 4 to 17 participated in painting elements from community history on a wall, with support from the fire department (wall cleaning), parents (snacks, transport), the town council (funds), a student (mural painting experience). The author concludes that the rural community residents achieved their goal, with the painted mural as a reminder of a positive experience. Implications for nursing education and community partnerships are discussed. | Description of a case intervention. |
| Bowns, C. (2011) [43] Facilitating the Production of Place-Based Knowledge for Participatory Community Development in Rural Pennsylvania | Rural Pennsylvania, USA | Research questions: “How can local communities contribute to place-sensitive development in rural places?” and “What are the outcomes of adult and child participation in community-based projects?”. | Local communities were engaged in identifying and prioritizing local opportunities for revitalization and invited to comment on proposals. Place-based knowledge can benefit community improvement through participatory processes. | Case study. Description of service-learning projects in three rural communities, delivered by landscape architecture students. |
| Pan, R. et al. (2005) [37] Building Healthier Communities for Children and Families: Applying ABCD to Community Pediatrics | Sacramento, California, USA | The service-learning program aimed to apply ABCD to community pediatrics. In this concrete case, the aim was to involve community partners through ABCD to address the problem of a high frequency of children arriving at the emergency ward bitten by dogs. | The chosen case illustrates that ABCD can be used successfully in the service-learning program. In this case, the asset mapping exercise involved dog owners, crossing guards, children, a neighborhoods association, an elementary school and a city park. The resident and community partners organized a dog-safety fair, where dog owners allowed children to practice dog-safety behavior. New social networks and social norms were created in the community. The authors observe that this approach is likely to reduce dog bites. | Case study on the application of ABCD based on the report from a pediatric resident. |
| Roberts, S. et al. (1998) [39] | Edmonton, Canada | The Community Development Office of Capital Health (CDO) Westlawn Junior High School aimed to involve students and community groups in development processes by the use of ABCD. They aimed to discover, connect, and mobilize students’ assets and gifts and connect these with those of people and groups in the communities, and to evaluate the project. | Fifteen grade 9 students met for two full-day workshops and 14 afternoons, in addition to some full days spent on special events and projects. Assisted by facilitators the youth made two projects: Flower planting with the community and carnival for daycare children. The children developed their participatory skills. The evaluation recommended: (1) Securing funding for continuation. (2) Pre and post-test to measure changes in students’ self-esteem and leadership abilities. (3) Include business plans as part of the projects. (4) Increase the involvement of external partners. (5) and of the parents and staff. (6) Modify daily plans. (7) Daily reflections and evaluations. (8) Keep records of expenses and human resources. | Project description and evaluation-based on objectives set before the project started, followed by observations documented by the participants. Unpublished report. |
| Shah, R.W. et al. (2018) [36] Fostering eABCD: Asset-based community development in digital service-learning | Lincoln, Nebraska, USA | To explore how aspects of asset-based com-munity development can be enacted in online asset-based community development (eABCD). | The study of a digital writing partnership between college students and rural youth in the ninth grade. It illustrates how students can be supported in asset-based, relationship-driven, and internally focused interactions in online service-learning collaborations. | Case study based on online text dialogues. Texts from one term were coded using Dedoose to identify aspects of the three ABCD principles. Community partners and youth participants also answered questions geared towards the ABCD principles. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agdal, R.; Midtgård, I.H.; Meidell, V. Can Asset-Based Community Development with Children and Youth Enhance the Level of Participation in Health Promotion Projects? A Qualitative Meta-Synthesis. Int. J. Environ. Res. Public Health 2019, 16, 3778. https://doi.org/10.3390/ijerph16193778
Agdal R, Midtgård IH, Meidell V. Can Asset-Based Community Development with Children and Youth Enhance the Level of Participation in Health Promotion Projects? A Qualitative Meta-Synthesis. International Journal of Environmental Research and Public Health. 2019; 16(19):3778. https://doi.org/10.3390/ijerph16193778
Chicago/Turabian StyleAgdal, Rita, Inger Helen Midtgård, and Vigdis Meidell. 2019. "Can Asset-Based Community Development with Children and Youth Enhance the Level of Participation in Health Promotion Projects? A Qualitative Meta-Synthesis" International Journal of Environmental Research and Public Health 16, no. 19: 3778. https://doi.org/10.3390/ijerph16193778
APA StyleAgdal, R., Midtgård, I. H., & Meidell, V. (2019). Can Asset-Based Community Development with Children and Youth Enhance the Level of Participation in Health Promotion Projects? A Qualitative Meta-Synthesis. International Journal of Environmental Research and Public Health, 16(19), 3778. https://doi.org/10.3390/ijerph16193778