Tinnitus and Self-Perceived Hearing Handicap in Firefighters: A Cross-Sectional Study


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Prior Exposures Survey
2.3. Hearing Handicap Inventory for Adults (HHIA) Survey
2.4. Tinnitus Functional Index (TFI) Survey
2.5. Data Analyses
3. Results
3.1. Characteristics of Study Participants
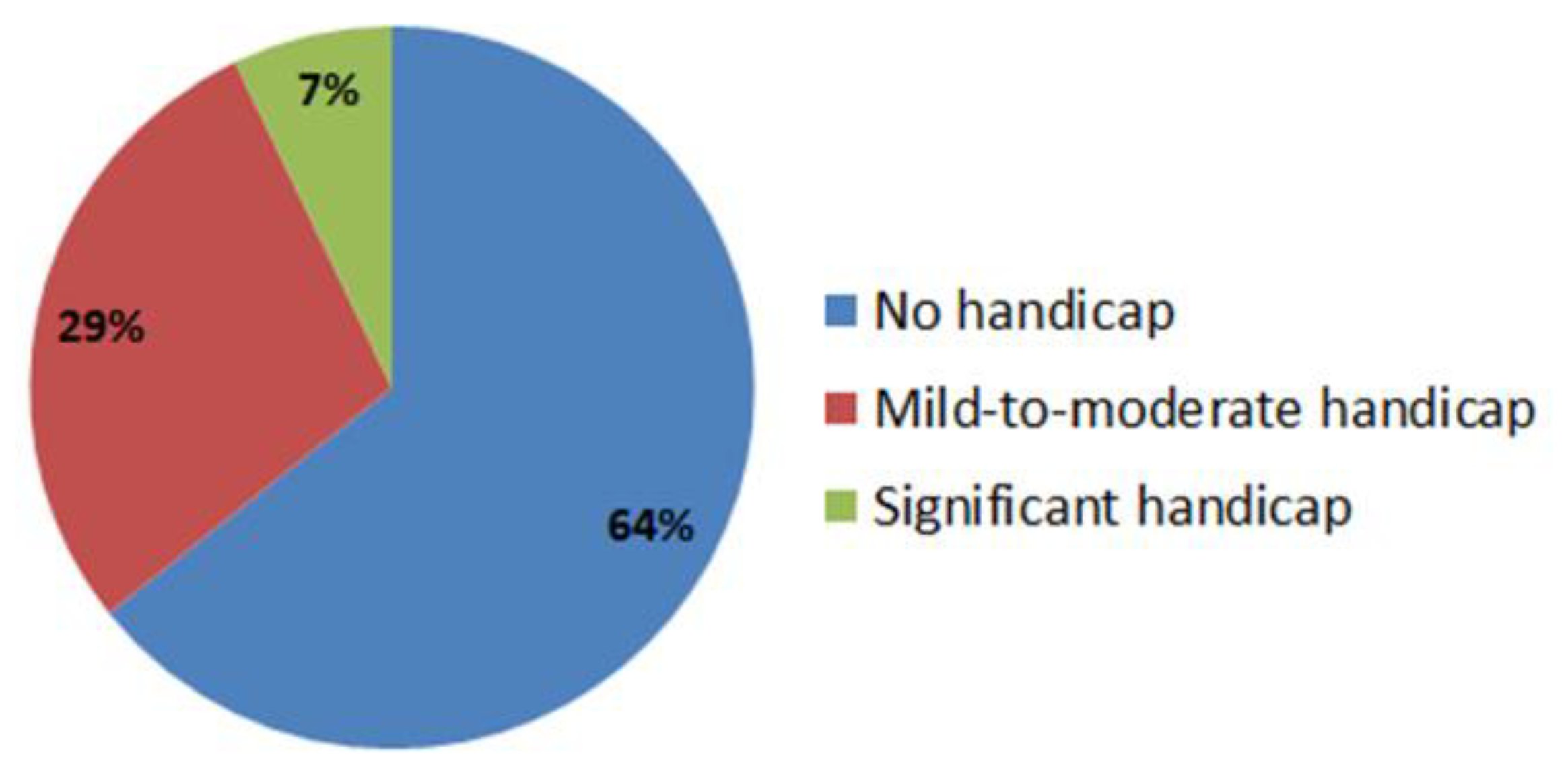
3.2. Hearing Handicap
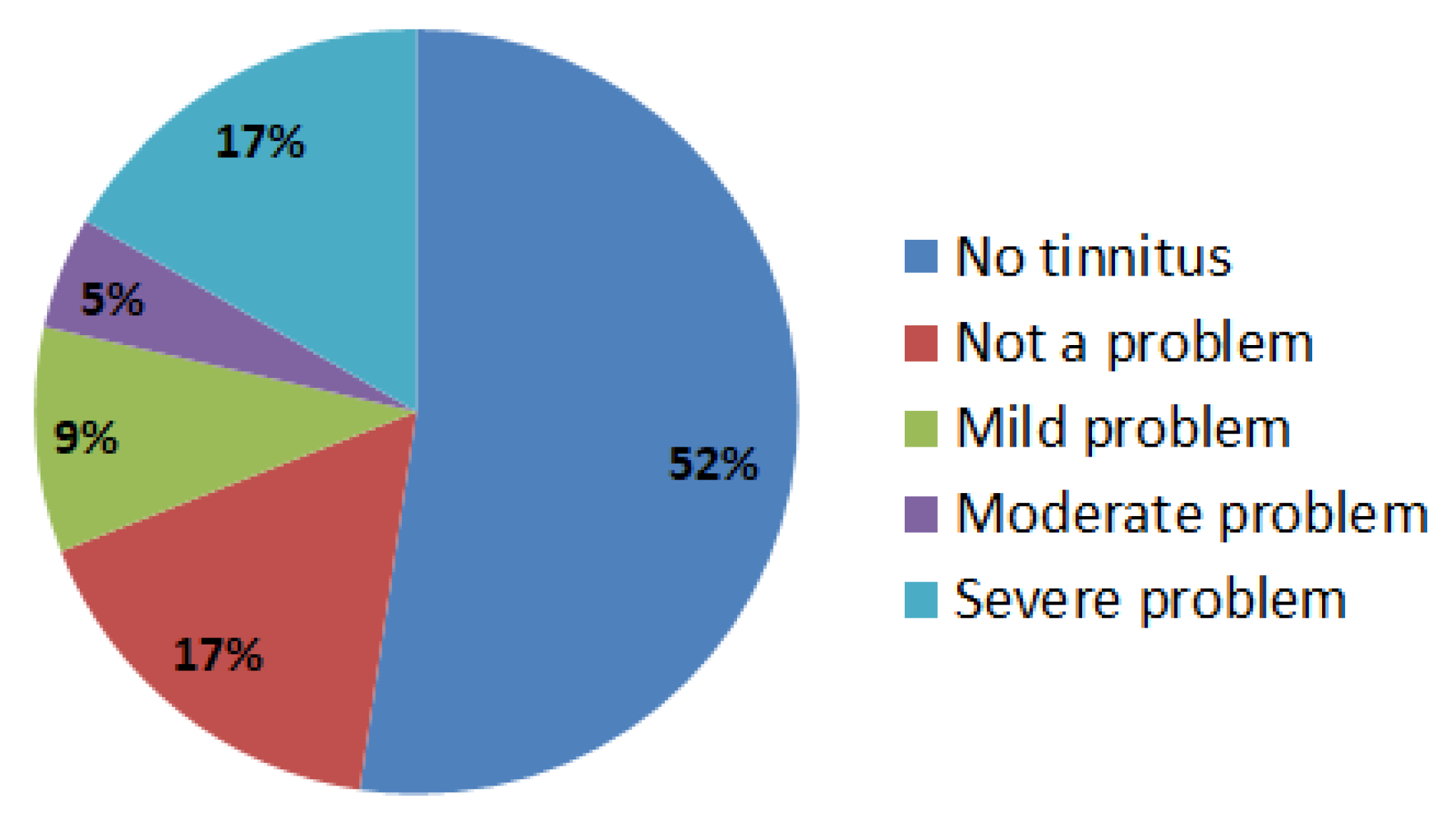
3.3. Tinnitus
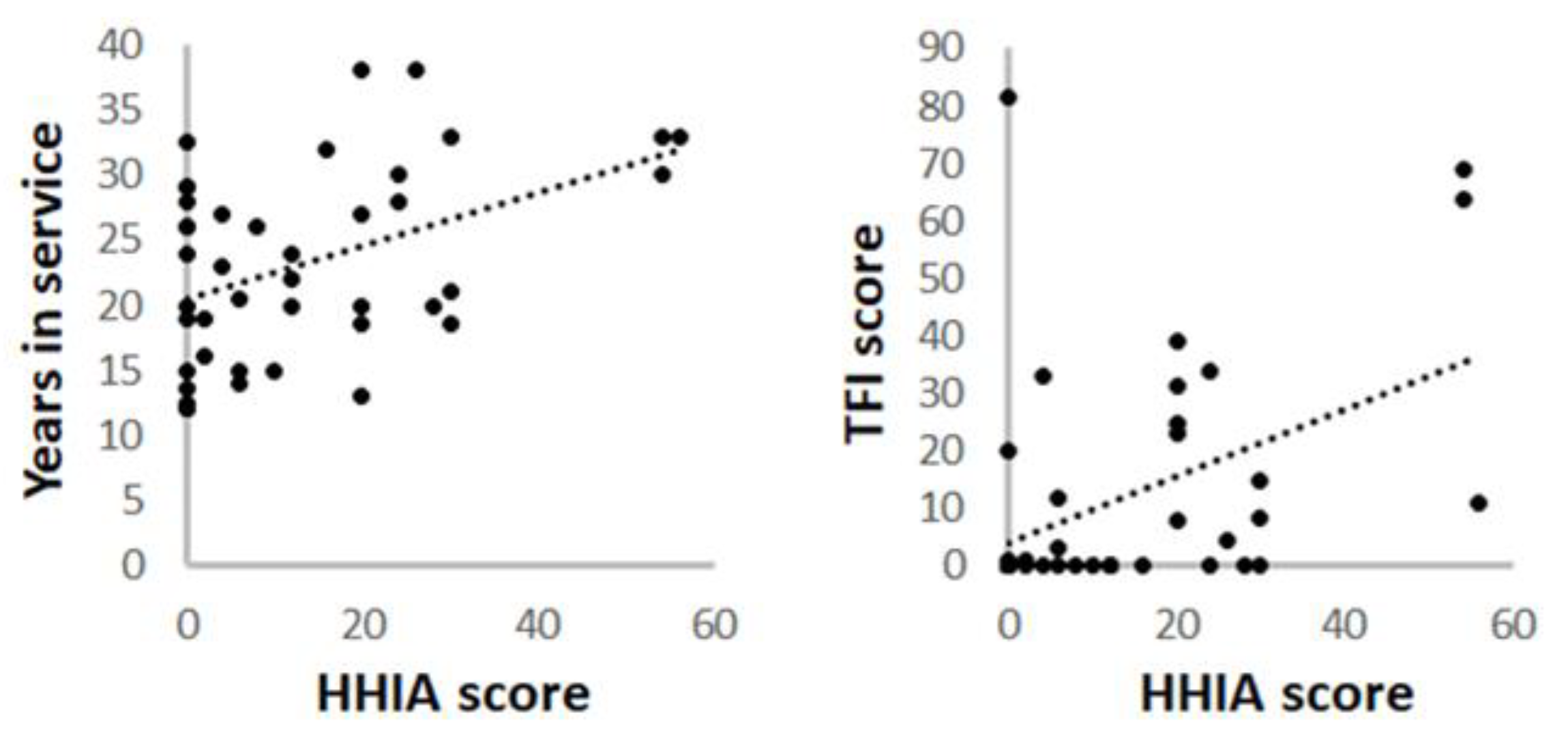
3.4. Association between Hearing Handicap and Tinnitus
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Blackwell, D.L.; Lucas, J.W.; Clarke, T.C. Summary health statistics for US adults: National Health Interview Survey, 2012. In Vital Health Statistics; National Center for Health Statistics, CDC: Atlanta, GA, USA, 2014. [Google Scholar]
- Hong, O.; Samo, D.; Hulea, R.; Eakin, B. Perception and attitudes of firefighters on noise exposure and hearing loss. J. Occup. Environ. Hyg. 2008, 5, 210–215. [Google Scholar] [CrossRef]
- Campo, P.; Morata, T.C.; Hong, O. Chemical exposure and hearing loss. Dis. Mon. 2013, 59, 119–138. [Google Scholar] [CrossRef] [Green Version]
- Henry, J.A.; Roberts, L.E.; Caspary, D.M.; Theodoroff, S.M.; Salvi, R.J. Underlying mechanisms of tinnitus: Review and clinical implications. J. Am. Acad. Audiol. 2014, 25, 5–22. [Google Scholar] [CrossRef] [PubMed]
- Shargorodsky, J.; Curhan, G.C.; Farwell, W.R. Prevalence and characteristics of tinnitus among US adults. Am. J. Med. 2010, 123, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Pross, S.E.; Allen, C.A.; Hong, O.S.; Cheung, S.W. Willingness-to-accept Gamma knife radiosurgery for tinnitus among career San Francisco firefighters. Otol. Neurotol. 2014, 35, 1026–1032. [Google Scholar] [CrossRef]
- Murray, K.S.; Rogers, D.T.; Kaufman, M.M. Heavy metals in an urban watershed in southeastern Michigan. J. Environ. Qual. 2004, 33, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Newman, C.W.; Weinstein, B.E.; Jacobson, G.P.; Hug, G.A. The Hearing Handicap Inventory for Adults: Psychometric adequacy and audiometric correlates. Ear Hear 1990, 11, 430–433. [Google Scholar] [CrossRef] [PubMed]
- Newman, C.W.; Weinstein, B.E.; Jacobson, G.P.; Hug, G.A. Test-retest reliability of the hearing handicap inventory for adults. Ear Hear 1991, 12, 355–357. [Google Scholar] [CrossRef]
- Meikle, M.B.; Henry, J.A.; Griest, S.E.; Stewart, B.J.; Abrams, H.B.; McArdle, R.; Myers, P.J.; Newman, C.W.; Sandridge, S.; Turk, D.C.; et al. The tinnitus functional index: Development of a new clinical measure for chronic, intrusive tinnitus. Ear Hear 2012, 33, 153–176. [Google Scholar] [CrossRef]
- Henry, J.A.; Griest, S.; Thielman, E.; McMillan, G.; Kaelin, C.; Carlson, K.F. Tinnitus Functional Index: Development, validation, outcomes research, and clinical application. Hear Res. 2016, 334, 58–64. [Google Scholar] [CrossRef]
- Lopez-Escamez, J.A.; Bibas, T.; Cima, R.F.; Van de Heyning, P.; Knipper, M.; Mazurek, B.; Szczepek, A.J.; Cederroth, C.R. Genetics of Tinnitus: An Emerging Area for Molecular Diagnosis and Drug Development. Front. Neurosci. 2016, 10, 377. [Google Scholar] [CrossRef] [PubMed]
- Folmer, R.L.; Griest, S.E. Tinnitus and insomnia. Am. J. Otolaryngol. 2000, 21, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Pattyn, T.; Van Den Eede, F.; Vanneste, S.; Cassiers, L.; Veltman, D.J.; Van De Heyning, P.; Sabbe, B.C.G. Tinnitus and anxiety disorders: A review. Hear Res. 2016, 333, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Hoekstra, C.E.; Wesdorp, F.M.; van Zanten, G.A. Socio-demographic, health, and tinnitus related variables affecting tinnitus severity. Ear Hear 2014, 35, 544–554. [Google Scholar] [CrossRef]
- Castellanos, M.J.; Fuente, A. The Adverse Effects of Heavy Metals with and without Noise Exposure on the Human Peripheral and Central Auditory System: A Literature Review. Int J. Environ. Res. Public Health 2016, 13, 1223. [Google Scholar] [CrossRef]
- Kirk, K.M.; McGuire, A.; Nielsen, L.; Cosgrove, T.; McClintock, C.; Nasveld, P.E.; Treloar, S.A. Self-reported tinnitus and ototoxic exposures among deployed Australian Defence Force personnel. Mil. Med. 2011, 176, 461–467. [Google Scholar] [CrossRef]
- Choi, Y.H.; Hu, H.; Mukherjee, B.; Miller, J.; Park, S.K. Environmental cadmium and lead exposures and hearing loss in US adults: The National Health and Nutrition Examination Survey, 1999 to 2004. Environ. Health Perspect. 2012, 120, 1544–1550. [Google Scholar] [CrossRef]
- Jamesdaniel, S.; Rosati, R.; Westrick, J.; Ruden, D.M. Chronic lead exposure induces cochlear oxidative stress and potentiates noise-induced hearing loss. Toxicol. Lett. 2018, 292, 175–180. [Google Scholar] [CrossRef]
- Kang, T.; Hong, O.; Kim, K.; Yoon, C. Hearing among male firefighters: A comparison with hearing data from screened and unscreened male population. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 106–112. [Google Scholar] [CrossRef]
- Roberts, L.E.; Salvi, R. Overview: Hearing loss, tinnitus, hyperacusis, and the role of central gain. Neuroscience 2019, 407, 1–7. [Google Scholar] [CrossRef]
- Hong, O.; Chin, D.L.; Phelps, S.; Joo, Y. Double Jeopardy: Hearing Loss and Tinnitus Among Noise-Exposed Workers. Workplace Health Saf. 2016, 64, 235–242. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | Firefighters (n = 42) |
|---|---|
| Sex | |
| Male | 40 (95.2%) |
| Female | 2 (4.8%) |
| Race/ethnicity | |
| African American or Black | 15 (33.7%) |
| Caucasian | 27 (64.3%) |
| Age (year) | |
| Mean ± SD | 47.95 ± 6.77 |
| Median | 48.5 |
| Years as firefighter | |
| Mean ± SD | 23.16 ± 7.30 |
| Median | 22.5 |
| Hearing Handicap Inventory for Adults (HHIA) | Firefighters (n = 42) |
|---|---|
| Mean ± SD | 13.24 ± 15.55 |
| Range | 0–56 |
| Subscales | |
| Social | |
| Mean ± SD | 12.50 ± 15.37 |
| Range | 0–58.33 |
| Emotional | |
| Mean ± SD | 13.74 ± 16.97 |
| Range | 0–57.69 |
| Tinnitus Functional Index (TFI) | Firefighters (n = 42) |
|---|---|
| Mean ± SD | 11.47 ± 20.24 |
| Range | 0–81.6 |
| Subscales | |
| Intrusive | |
| Mean ± SD | 14.09 ± 24.86 |
| Range | 0–93.33 |
| Sense of control | |
| Mean ± SD | 11.94 ± 22.68 |
| Range | 0–76.67 |
| Cognitive | |
| Mean ± SD | 12.3 ± 25.27 |
| Range | 0–100 |
| Sleep | |
| Mean ± SD | 11.59 ± 23.40 |
| Range | 0–80 |
| Auditory | |
| Mean ± SD | 15.79 ± 27.21 |
| Range | 0–80 |
| Relaxation | |
| Mean ± SD | 13.17 ± 25.81 |
| Range | 0–100 |
| Quality of life | |
| Mean ± SD | 8.15 ± 18.46 |
| Range | 0–70 |
| Emotional | |
| Mean ± SD | 5.24 ± 13.19 |
| Range | 0–63.33 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jamesdaniel, S.; Elhage, K.G.; Rosati, R.; Ghosh, S.; Arnetz, B.; Blessman, J. Tinnitus and Self-Perceived Hearing Handicap in Firefighters: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2019, 16, 3958. https://doi.org/10.3390/ijerph16203958
Jamesdaniel S, Elhage KG, Rosati R, Ghosh S, Arnetz B, Blessman J. Tinnitus and Self-Perceived Hearing Handicap in Firefighters: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2019; 16(20):3958. https://doi.org/10.3390/ijerph16203958
Chicago/Turabian StyleJamesdaniel, Samson, Kareem G. Elhage, Rita Rosati, Samiran Ghosh, Bengt Arnetz, and James Blessman. 2019. "Tinnitus and Self-Perceived Hearing Handicap in Firefighters: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 16, no. 20: 3958. https://doi.org/10.3390/ijerph16203958
APA StyleJamesdaniel, S., Elhage, K. G., Rosati, R., Ghosh, S., Arnetz, B., & Blessman, J. (2019). Tinnitus and Self-Perceived Hearing Handicap in Firefighters: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 16(20), 3958. https://doi.org/10.3390/ijerph16203958