Systematic Development of Materials for Inviting Low Health-Literate Individuals to Participate in Preconception Counseling

 and
and
Abstract
:1. Introduction
- -
- to analyze comprehension of the HP4All invitational material, perception of perinatal risk, attitude towards PCC, intention to participate in PCC, and actual participation in PCC (stage 1);
- -
- to adapt invitational material and assess acceptance, comprehensibility, and relevance of the adapted invitational material (stage 2);
- -
- to evaluate the final version of the adapted invitation in a new group of low health-literate women (stage 3).
2. Materials and Methods
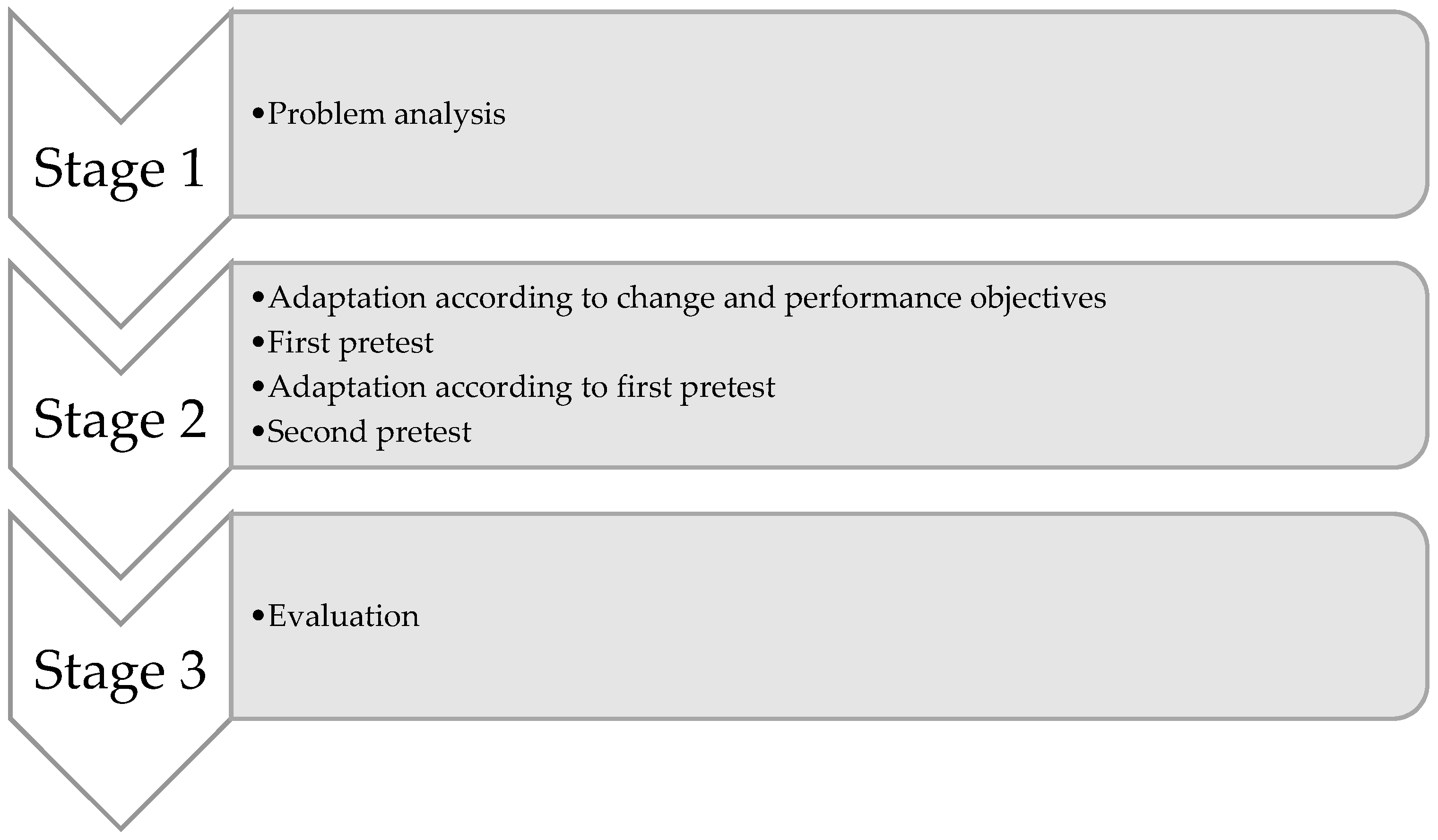
2.1. Study Design
2.2. Study Population and Recruitment
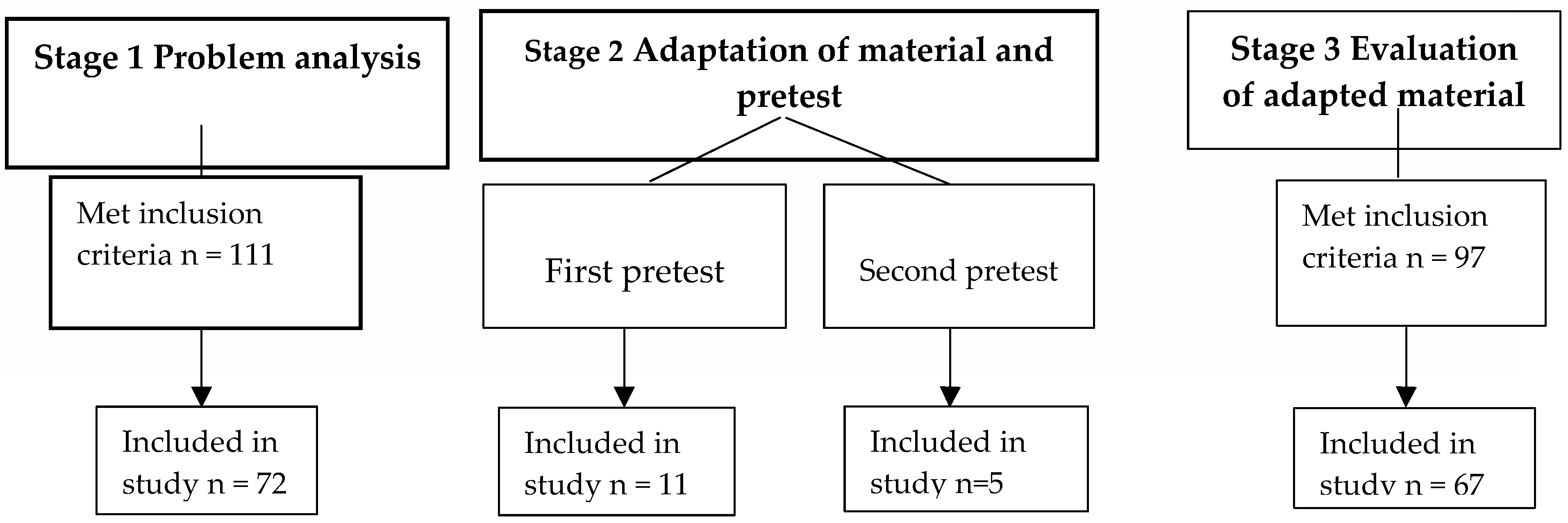
2.3. Stage 1: Problem Analysis
2.3.1. Conceptual Framework
2.3.2. Background Characteristics
2.3.3. Main Outcome Measures
2.4. Stage 2: Adaptation of Material and Pretest
2.4.1. Formulating Performance and Change Objectives Based on Outcomes Problem Analysis (Stage 1)
- -
- Is aware of written invitation for PCC
- -
- Makes an informed decision whether (or not) to participate in PCC
- -
- Participates in PCC
2.4.2. Adaptation and Pretesting of Invitational Material
2.5. Stage 3: Evaluation of Adapted Material
2.6. Analyses
2.6.1. Stage 1
2.6.2. Stage 2
2.6.3. Stage 3
2.7. Ethics Approval and Consent to Participate
3. Results
3.1. Response and Background Characteristics
3.2. Outcomes Stage 1: Problem Analysis
3.2.1. Subjective and Objective Comprehension
3.2.2. Risk Perception, Attitude and Intention
3.3. Outcomes Stage 2: Pretest and Adaptation of Material
3.4. Outcomes Stage 3: Evaluation of Adapted Material
3.4.1. Differences in Comprehension of Invitational Material
3.4.2. Differences in Risk Perception, Attitude and Intention
4. Discussion
4.1. Main Findings
4.2. Discussion of Main Findings
4.3. Strengths and Limitations
4.4. Implications for Further Research and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Denny, C.H.; Floyd, R.L.; Green, P.P.; Hayes, D.K. Racial and ethnic disparities in preconception risk factors and preconception care. J. Women Health. 2012, 21, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Temel, S.; Birnie, E.; Sonneveld, H.; Voorham, A.; Bonsel, G.; Steegers, E.; Denktaş, S. Determinants of the intention of preconception care use: Lessons from a multi-ethnic urban population in the Netherlands. Int. J. Public Health 2013, 58, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Hosli, E.J.; Elsinga, J.; Buitendijk, S.E.; Assendelft, W.J.; Van der Pal-de Bruin, K.M. Women’s motives for not participating in preconception counseling: Qualitative study. Commun. Genet. 2008, 11, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Shannon, G.D.; Alberg, C.; Nacul, L.; Pashayan, N. Preconception healthcare and congenital disorders: Systematic review of the effectiveness of preconception care programs in the prevention of congenital disorders. Matern. Child Health J. 2014, 18, 1354–1379. [Google Scholar] [CrossRef]
- Coonrod, D.V.; Bruce, N.C.; Malcolm, T.D.; Drachman, D.; Frey, K.A. Knowledge and attitudes regarding preconception care in a predominantly low-income Mexican American population. Am. J. Obstet. Gynecol. 2009, 200, 686.e1-7. [Google Scholar] [CrossRef]
- Elsinga, J.; de Jong-Potjer, L.C.; Van der Pal-de Bruin, K.M.; le Cessie, S.; Assendelft, W.J.; Buitendijk, S.E. The effect of preconception counselling on lifestyle and other behaviour before and during pregnancy. Womens Health Issues 2008, 18, S117–S125. [Google Scholar] [CrossRef]
- Fuehrer, L.; Buckler, E.; Bowman, E.; Gregory, T.; McDaniel, J. Promoting preconception health in primary care. J. Am. Acad. Phys. Assist. 2015, 28, 27–32. [Google Scholar] [CrossRef]
- Fowler, J.R.; Hughes, J. Preconception Counseling; StatPearls: St. Petersburg, FL, USA, 2017. [Google Scholar]
- Tough, S.; Tofflemire, K.; Clarke, M.; Newburn-Cook, C. Do women change their drinking behaviors while trying to conceive? An opportunity for preconception counseling. Clin. Med. Res. 2006, 4, 97–105. [Google Scholar] [CrossRef]
- Coffey, K.; Shorten, A. The challenge of preconception counseling: Using reproductive life planning in primary care. J. Am. Assoc. Nurse Pract. 2014, 26, 255–262. [Google Scholar] [CrossRef]
- Mazza, D.; Chapman, A. Improving the uptake of preconception care and periconceptional folate supplementation: What do women think? BMC Public Health 2010, 10, 786. [Google Scholar] [CrossRef]
- Temel, S.; Erdem, Ö.; Voorham, T.A.; Bonsel, G.J.; Steegers, E.A.; Denktaş, S. Knowledge on preconceptional folic acid supplementation and intention to seek for preconception care among men and women in an urban city: A population-based cross-sectional study. BMC Pregnancy Childbirth 2015, 15, 340. [Google Scholar] [CrossRef] [PubMed]
- Paasche-Orlow, M.K.; Wolf, M.S. The causal pathways linking health literacy to health outcomes. Am. J. Health Behav. 2007, 31, S19–S26. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, K.; van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Kilfoyle, K.A.; Vitko, M.; O’Conor, R.; Bailey, S.C. Health Literacy and Women’s Reproductive Health: A Systematic Review. J. Women Health 2016, 25, 1237–1255. [Google Scholar] [CrossRef] [PubMed]
- Heijmans, M.; Waverijn, G.; Rademakers, J.; van der Vaart, R.; Rijken, M. Functional, communicative and critical health literacy of chronic disease patients and their importance for self-management. Patient Educ. Couns. 2015, 98, 41–48. [Google Scholar] [CrossRef] [Green Version]
- Von Wagner, C.; Steptoe, A.; Wolf, M.S.; Wardle, J. Health literacy and health actions: A review and a framework from health psychology. Health Educ. Behav. 2009, 36, 860–877. [Google Scholar] [CrossRef]
- Sijpkens, M.K.; van Voorst, S.F.; de Jong-Potjer, L.C.; Denktaş, S.; Verhoeff, A.P.; Bertens, L.C.; Rosman, A.N.; Steegers, E.A. The effect of a preconception care outreach strategy: The Healthy Pregnancy 4 All study. BMC Health Serv. Res. 2019, 19, 60. [Google Scholar] [CrossRef]
- Benson, J.G.; Forman, S.B. Comprehension of written health care information in an affluent geriatric retirement community: Use of the Test of Functional Health Literacy. Gerontology 2002, 48, 93–97. [Google Scholar] [CrossRef]
- Mullen, R.J.; Duhig, J.; Russell, A.; Scarazzini, L.; Lievano, F.; Wolf, M.S. Best-practices for the design and development of prescription medication information: A systematic review. Patient Educ. Couns. 2018, 101, 1351–1367. [Google Scholar] [CrossRef]
- Koops van‘t Jagt, R.; Hoeks, J.C.; Jansen, C.J.; de Winter, A.F.; Reijneveld, S.A. Comprehensibility of health-related documents for older adults with different levels of health literacy: A systematic review. J. Health Commun. 2016, 21, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Denktas, S.; Poeran, J.; van Voorst, S.F.; Vos, A.A.; de Jong-Potjer, L.C.; Waelput, A.J.; Steegers, E.A. Design and outline of the Healthy Pregnancy 4 All study. BMC Pregnancy Childbirth 2014, 14, 253. [Google Scholar] [CrossRef] [PubMed]
- Bartholomew, L.; Parcel, S.; Kok, G.; Gottlieb, N. Planning Health Promotion Programs: An Intervention Mapping Approach, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2006. [Google Scholar]
- Pander Maat, H.; Essink-Bot, M.L.; Leenaars, K.E.; Fransen, M.P. A short assessment of health literacy (SAHL) in the Netherlands. BMC Public Health 2014, 14, 990. [Google Scholar] [CrossRef] [PubMed]
- UNESCO. Revision of the International Standard Classification of Education; UNESCO: Paris, France, 2013. [Google Scholar]
- Rijksinstituut voor Volksgezondheid en Milieu. Etniciteit: Definitie en gegevens 2014. Available online: http://www.nationaalkompas.nl/bevolking/etniciteit/wat-is-etniciteit/ (accessed on 9 October 2014).
- Berry, J.W.; Phinney, J.S.; Sam, D.L.; Vedder, P. Immigrant youth: Acculturation, identity, and adaptation. Appl. Psychol. 2006, 55, 303–332. [Google Scholar] [CrossRef]
- Lee, S.Y.D.; Stucky, B.D.; Lee, J.Y.; Rozier, R.G.; Bender, D.E. Short assessment of health literacy—Spanish and English: A comparable test of health literacy for Spanish and English speakers. Health Serv. Res. 2010, 45, 1105–1120. [Google Scholar] [CrossRef]
- Marteau, T.M.; Dormandy, E.; Michie, S. A measure of informed choice. Health Expect. 2001, 4, 99–108. [Google Scholar] [CrossRef] [Green Version]
- Van den Berg, M.; Timmermans, D.R.; Ten Kate, L.P.; van Vugt, J.M.; van der Wal, G. Are pregnant women making informed choices about prenatal screening? J. Genet. Med. 2005, 7, 332–338. [Google Scholar] [CrossRef] [Green Version]
- Ooms, J.A.; Jansen, C.J.; Hoeks, J.C. The story against smoking: An exploratory study into the processing and perceived effectiveness of narrative visual smoking warnings. Health Educ. J. 2019. [Google Scholar] [CrossRef]
- Damman, O.C.; Timmermans, D.R. Educating health consumers about cardio-metabolic health risk: What can we learn from lay mental models of risk? Patient Educ. Couns. 2012, 89, 300–308. [Google Scholar] [CrossRef]
- Poels, M.; Koster, M.P.; Boeije, H.R.; Franx, A.; van Stel, H.F. Why do women not use preconception care? A systematic review on barriers and Facilitators. Obstet. Gynecol. Surv. 2016, 71, 603–612. [Google Scholar] [CrossRef]
- Aldridge, M.D. Writing and designing readable patient education materials. Nephrol. Nurs. J. 2004, 31, 373. [Google Scholar] [PubMed]
- Meppelink, C.S.; Smit, E.G.; Buurman, B.M.; van Weert, J.C. Should we be afraid of simple messages? The effects of text difficulty and illustrations in people with low or high health literacy. Health Commun. 2015, 30, 1181–1189. [Google Scholar] [CrossRef] [PubMed]
- Rutherford, J.; Taylor, A.; Holman, R.; MacDonald, J.; Jarrett, D.; Bigrigg, A. Low literacy: A hidden problem in family planning clinics. BMJ Sex. Reprod. Health 2006, 32, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.E.; Sanson-Fisher, R.W.; Lynagh, M.C.; Threlfall, T.; D’Este, C.A. Format and readability of an enhanced invitation letter did not affect participation rates in a cancer registry-based study: A randomized controlled trial. J. Clin. Epidemiol. 2013, 66, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Davis, T.C.; Williams, M.V.; Marin, E.; Parker, R.M.; Glass, J. Health literacy and cancer communication. CA Cancer J. Clin. 2002, 52, 134–149. [Google Scholar] [CrossRef] [PubMed]
- Fransen, M.P.; Hopman, M.E.; Murugesu, L.; Rosman, A.N.; Smith, S.K. Preconception counselling for low health literate women: An exploration of determinants in the Netherlands. Reprod. Health 2018, 15, 192. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Performance Objectives | Determinants | |||
|---|---|---|---|---|
| Risk Perception | Knowledge Level | Attitude | Coping Skills | |
| Is aware of written invitation for PCC. | Knows that she is invited by the written invitation material of PCC. | |||
| Makes an informed decision whether (or not) to participate in PCC. | Is aware of the fact that she belongs to a high risk group. | Knows what PCC entails. | Has a positive attitude towards participation in PCC. The decision whether or not to participate in PCC corresponds with attitude. Weighs the advantages and disadvantages and assigns value to these advantages and disadvantages. | |
| Participates in PCC. | Is able to cope with practical barriers. | |||
| Performance Objectives | Change Objectives | Theoretical Models | Methods | Strategy |
|---|---|---|---|---|
| Is aware of written invitation for PCC. | Knows that she is invited by the written invitation material of PCC. | Dual-process model (William James, 1890). Systemic functional linguistics (Halliday et al., 1994). | Stimulating women’s intuitive and automatic cognitive processes. Adjusting text attributes. | Strengthen association letter with an invitation. Adjusting text attributes. |
| Makes an informed decision whether (or not) to participate in PCC. | Is aware of the fact that she belongs to a high-risk group. | Social Cognitive Theory, (Bandura, 1986.) Theory of Heuristics (Herbert Simon, 1957). Systemic functional linguistics (Halliday et al., 1994). | Modeling. Adjusting text attributes. | Role model story. Using narratives. Adjusting text attributes. |
| Makes an informed decision whether (or not) to participate in PCC. | Knows what PCC entails. | Dual process model (William James, 1890). Systemic functional linguistics (Halliday et al., 1994). | Stimulating women’s working memory and deliberative, logical and analytical cognitive processes. Adjusting text attributes. | Role model story.Using narratives. Adjusting text attributes. |
| Makes an informed decision whether (or not) to participate in PCC. | Weighs the advantages and disadvantages and assigns value to these advantages and disadvantages. | Social Cognitive Theory, (Bandura 1986). Theory of Heuristics (Herbert Simon, 1957). Systemic functional linguistics (Halliday et al., 1994). Dual-process model (William James, 1890). | Modelling. Adjusting text attributes. Using International Patient Decision Aids Standards (IPDAS) criteria. | Role model story.Adjusting text attributes. Apply IPDAS criteria in narrative. |
| Makes an informed decision whether (or not) to participate in PCC. | The decision whether or not to participate in PCC corresponds with attitude. | Dual process model (William James, 1890). Systemic functional linguistics (Halliday et al., 1994). | Using IPDAS criteria. Adjusting text attributes. | Apply IPDAS criteria in narrative. Adjusting text attributes. |
| Women participate in PCC. | Is able to cope with practical barriers. | Social Cognitive Theory, (Bandura 1986). Theory of Heuristics (Herbert Simon, 1957). Systemic functional linguistics (Halliday et al., 1994). | Modelling. Adjusting text attributes. | Clearly stating how women should deal with practical problems. Adjusting text attributes. |
| Background Characteristics | Stage 1 (n = 72) | Stage 3 (n = 67) | Stage 1 and 3 (n = 139) | |||
|---|---|---|---|---|---|---|
| Mean (SD; Range) | N (%) | Mean (SD; Range) | N (%) | Mean (SD; Range) | N (%) | |
| Age (years) | 29 (7; 18–42) | 30 (6; 18–42) | ||||
| Educational level 1 | ||||||
| Low | 9 (13) | 1 (2) | 10 (7) | |||
| Intermediate | 37 (51) | 44 (66) | 81 (58) | |||
| High | 26 (36) | 22 (33) | 48 (35) | |||
| Occupational status | ||||||
| Employed | 37 (51) | 39 (58) | 76 (55) | |||
| Student | 13 (18) | 17 (25) | 30 (22) | |||
| Unemployed | 22 (31) | 11 (16) | 33 (24) | |||
| Ethnic background 2 | ||||||
| Dutch | 13 (18) | 41 (61) | 54 (39) | |||
| Other western (non-Dutch) | 13 (18) | 10 (15) | 23 (17) | |||
| Non-western | 46 (64) | 16 (24) | 62 (45) | |||
| Health literacy score | 35 (13; 9–53) | 47 (7; 20–54) | 41 (12; 9–54) | |||
| Difficulty understanding Dutch | ||||||
| Sometimes | 29 (40) | 3 (5) | 32 (23) | |||
| Never | 42 (58) | 64 (96) | 106 (76) | |||
| Relationship status | ||||||
| Married/Living together with partner | 46 (64) | 43 (64) | 89 (64) | |||
| Single/Not living together with partner | 26 (36) | 24 (36) | 50 (36) | |||
| Perinatal experiences | ||||||
| Was pregnant before | 66 (92) | 45 (67) | 111 (80) | |||
| Ever had an unplanned pregnancy | 38 (53) | 16 (24) | 54 (39) | |||
| Ever had problems in previous pregnancy | 35 (49) | 26 (39) | 61 (44) | |||
| Wish to conceive 3 | ||||||
| In next 2 years | 30 (42) | 11 (16) | 41 (30) | |||
| In 2–5 years | 31 (43) | 30 (45) | 61 (44) | |||
| Undecided | 11 (15) | 26 (39) | 37 (27) | |||
| Comprehension of HP4All Invitation | N (%) | Correct N (%) |
|---|---|---|
| Subjective comprehension letter | ||
| Easy/very easy | 67 (93) | |
| Neutral | 5 (7) | |
| Difficult/very difficult | ||
| Subjective comprehension referral | ||
| Easy/very easy | 64 (89) | |
| Neutral | 8 (11) | |
| Difficult/very difficult | ||
| Objective comprehension letter | ||
| Target audience | 67 (93) | |
| Content counseling | 65 (90) | |
| Aim counseling | 53 (74) | |
| Application procedure | 46 (64) | |
| Objective comprehension referral | ||
| Content counseling | 64 (89) | |
| Aim counseling | 70 (97) | |
| Application procedure | 63 (88) |
| Background Characteristics | First Pretest (n = 11) | Second Pretest (n = 5) |
|---|---|---|
| Age mean (range) | 30 (19–39) | 32 (28–37) |
| Ethnic background | ||
| Dutch | 7 (64%) | 1 (20%) |
| Western (other than Dutch) | 0 (0%) | 1 (20%) |
| Non-Western | 4 (32%) | 3 (60%) |
| Number children | ||
| mean (range) | 2 (1–7) | 1 (0–2) |
| Comprehension | Stage 1 (n = 72) | Stage 3 (n = 67) | Difference Stage 1 and 3 |
|---|---|---|---|
| N (%) | N (%) | Beta (95% CI) | |
| Subjective comprehension letter * | 0.05 (−0.02–0.12) | ||
| Easy/very easy | 67 (93) | 64 (96) | |
| Neutral | 5 (7) | 1 (2) | |
| Difficult/very difficult | 0 (0) | 0 (0) | |
| Objective comprehension letter | 0.09 (−0.13–0.31) *** | ||
| Correct answers ‘target audience’ | 67 (93) | 63 (94) | |
| Correct answers ‘content counseling’ | 65 (90) | 65 (97) | |
| Correct answers ‘aim ‘counseling | 53 (74) | 62 (93) | |
| Correct answers ‘application procedure’ ** | 46 (64) | 65 (97) |
| Risk Perception, Attitude and Intention | Stage 1 (n = 72) | Stage 3 (n = 67) | Difference Stage 1 and 3 |
|---|---|---|---|
| Mean (SD; range) | Mean (SD; range) | Beta (95% CI) | |
| Risk perception | 2.6 (0.9; 2–4) | 2.7 (1.1; 1–5) | 0.14 (−0.19–0.47) |
| Attitude towards preconception counseling | 3.7 (0.4; 2–4) | 4.3 (0.6; 3–5) | 0.71 (0.48–0.93) * |
| Intention to participate | 3.1 (1,5; 1–5) | 3.0 (1.1; 1–5) | −0.13 (−0.57–0.31) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murugesu, L.; Hopman, M.E.; Van Voorst, S.F.; Rosman, A.N.; Fransen, M.P. Systematic Development of Materials for Inviting Low Health-Literate Individuals to Participate in Preconception Counseling. Int. J. Environ. Res. Public Health 2019, 16, 4223. https://doi.org/10.3390/ijerph16214223
Murugesu L, Hopman ME, Van Voorst SF, Rosman AN, Fransen MP. Systematic Development of Materials for Inviting Low Health-Literate Individuals to Participate in Preconception Counseling. International Journal of Environmental Research and Public Health. 2019; 16(21):4223. https://doi.org/10.3390/ijerph16214223
Chicago/Turabian StyleMurugesu, Laxsini, Miriam E. Hopman, Sabine F. Van Voorst, Ageeth N. Rosman, and Mirjam P. Fransen. 2019. "Systematic Development of Materials for Inviting Low Health-Literate Individuals to Participate in Preconception Counseling" International Journal of Environmental Research and Public Health 16, no. 21: 4223. https://doi.org/10.3390/ijerph16214223
APA StyleMurugesu, L., Hopman, M. E., Van Voorst, S. F., Rosman, A. N., & Fransen, M. P. (2019). Systematic Development of Materials for Inviting Low Health-Literate Individuals to Participate in Preconception Counseling. International Journal of Environmental Research and Public Health, 16(21), 4223. https://doi.org/10.3390/ijerph16214223