Increased Dementia Mortality in West Virginia Counties with Mountaintop Removal Mining?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Public Health and Socioeconomic Data
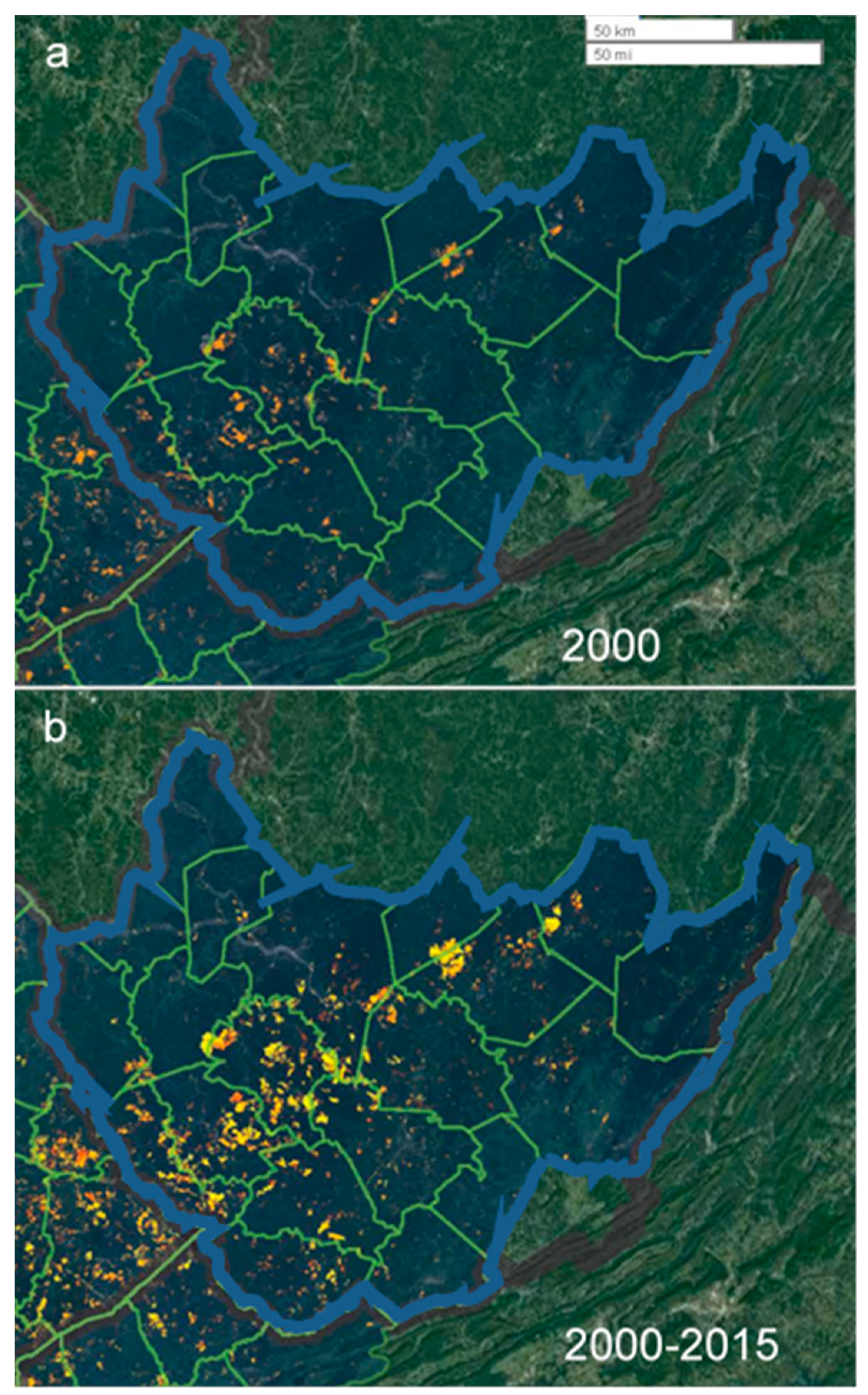
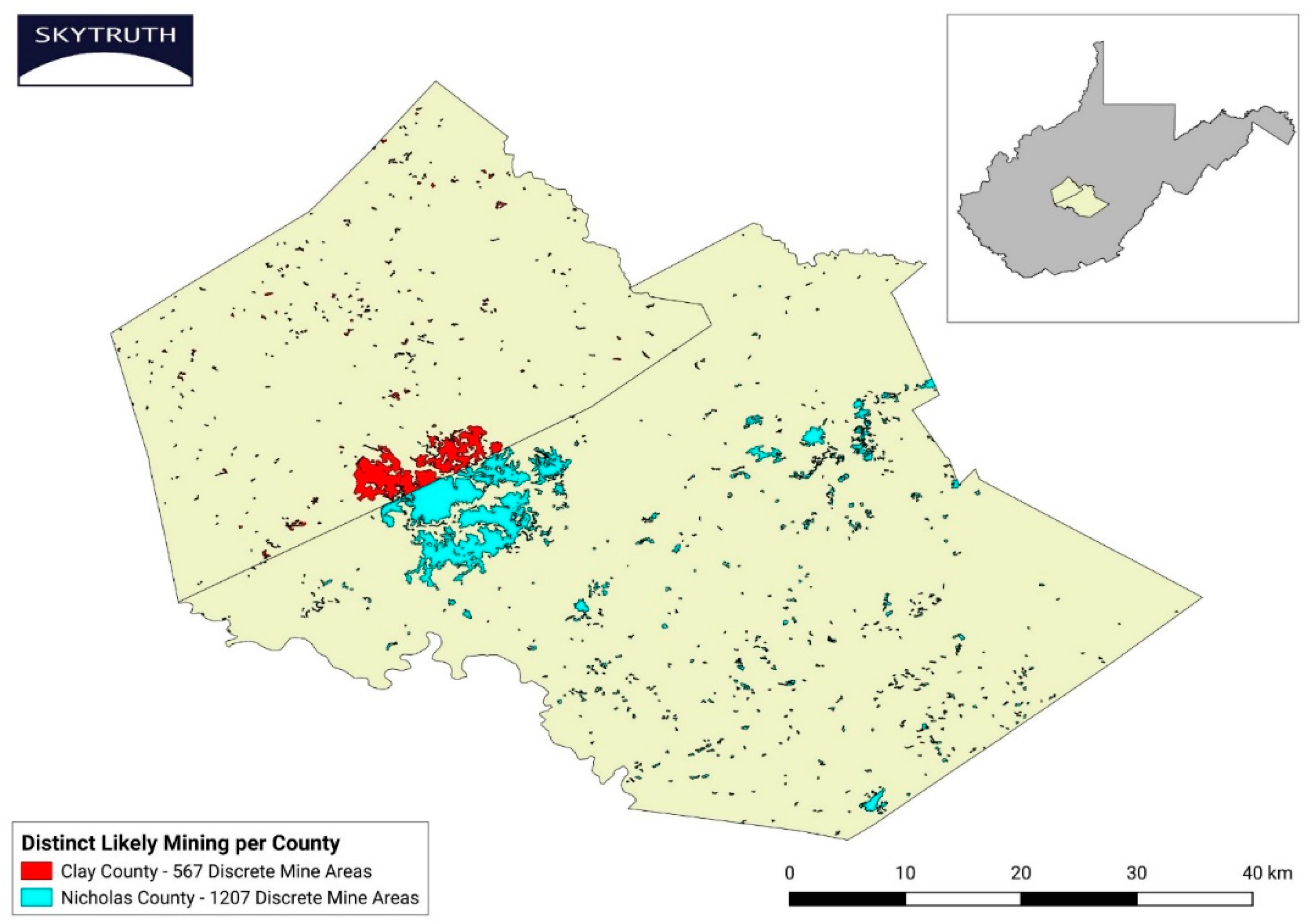
2.2. Location and Extent of MTM in West Virginia
2.3. Statistical Analyses
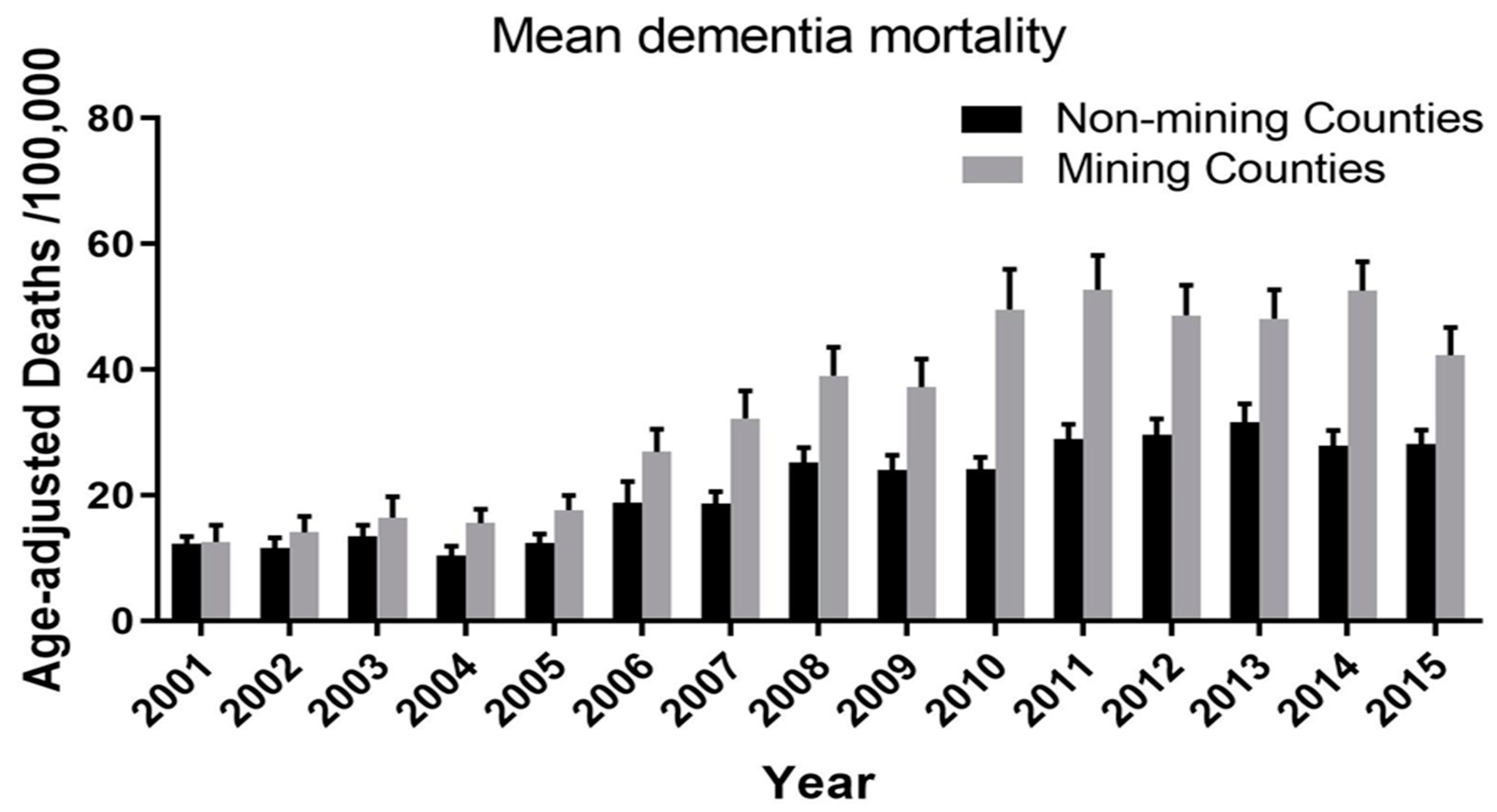
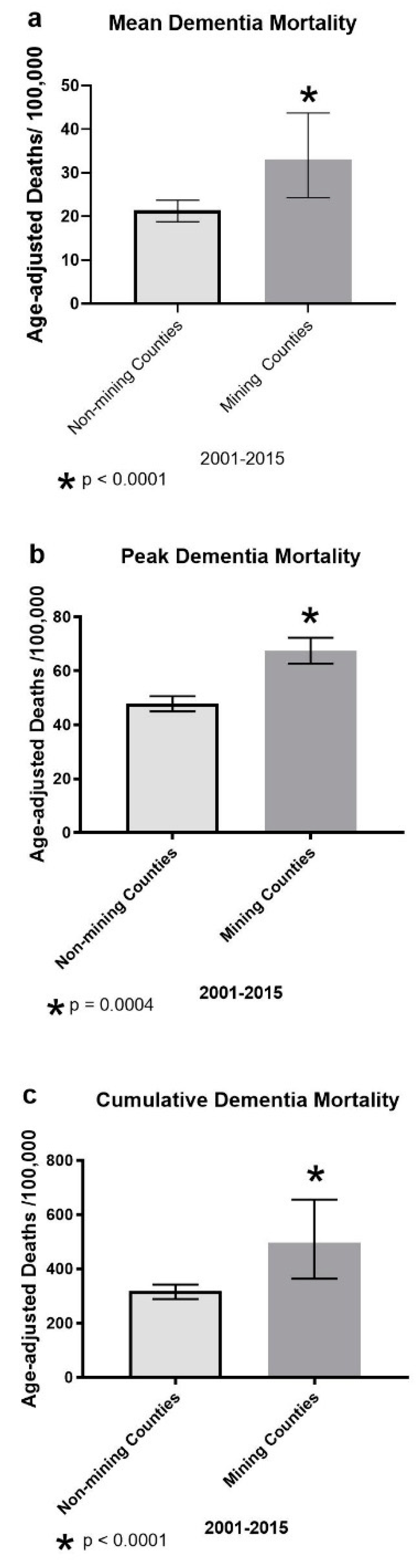
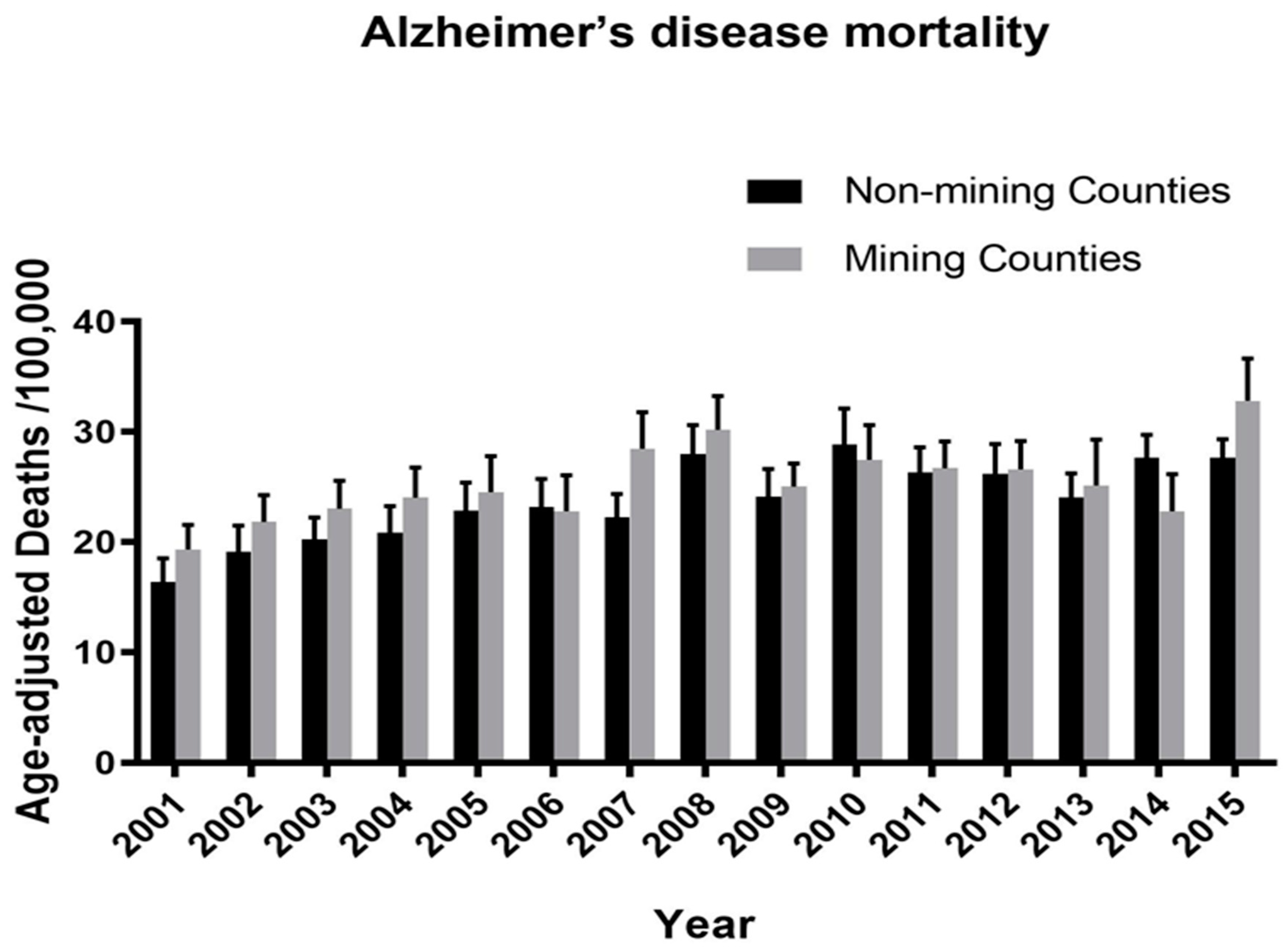
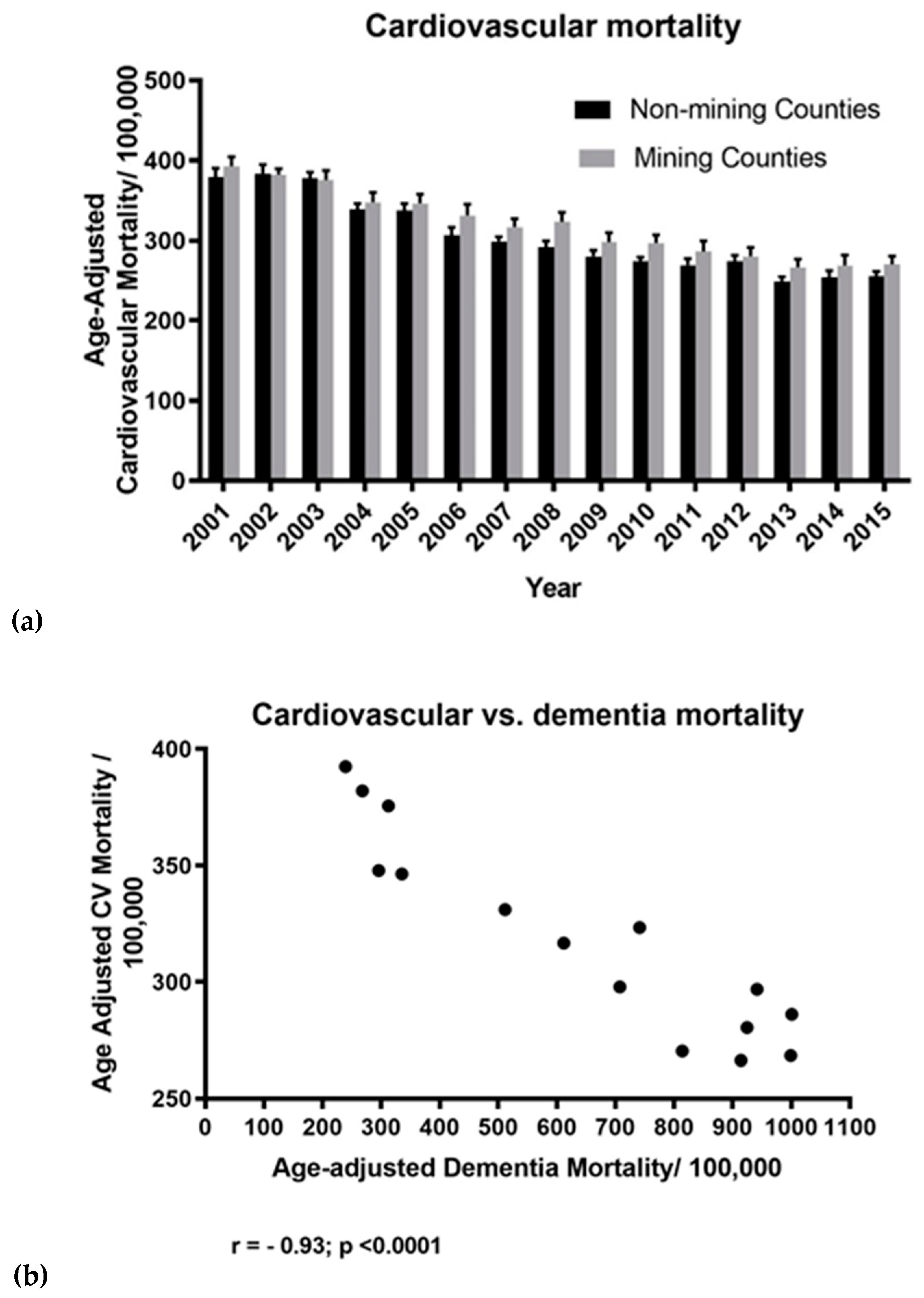
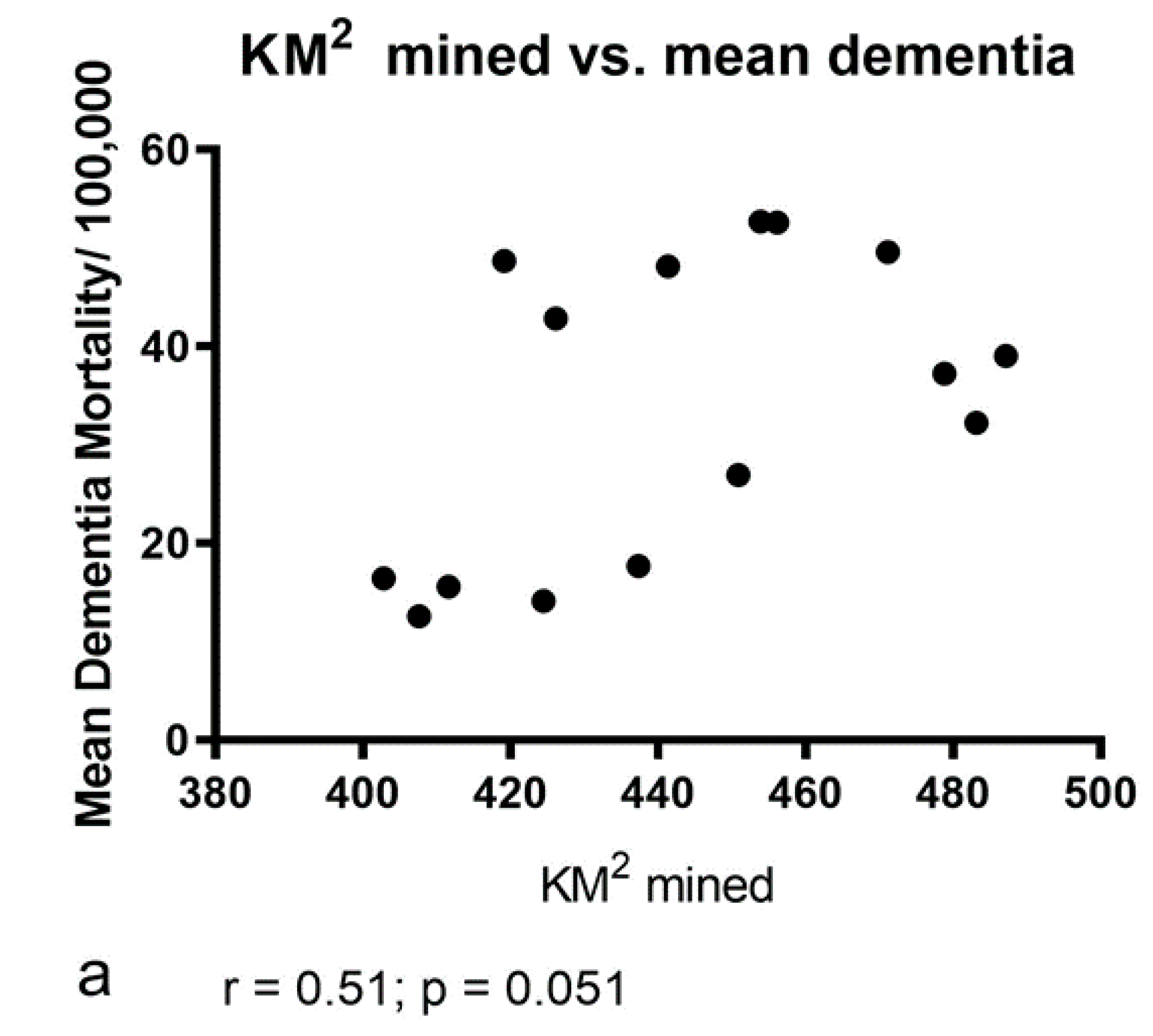
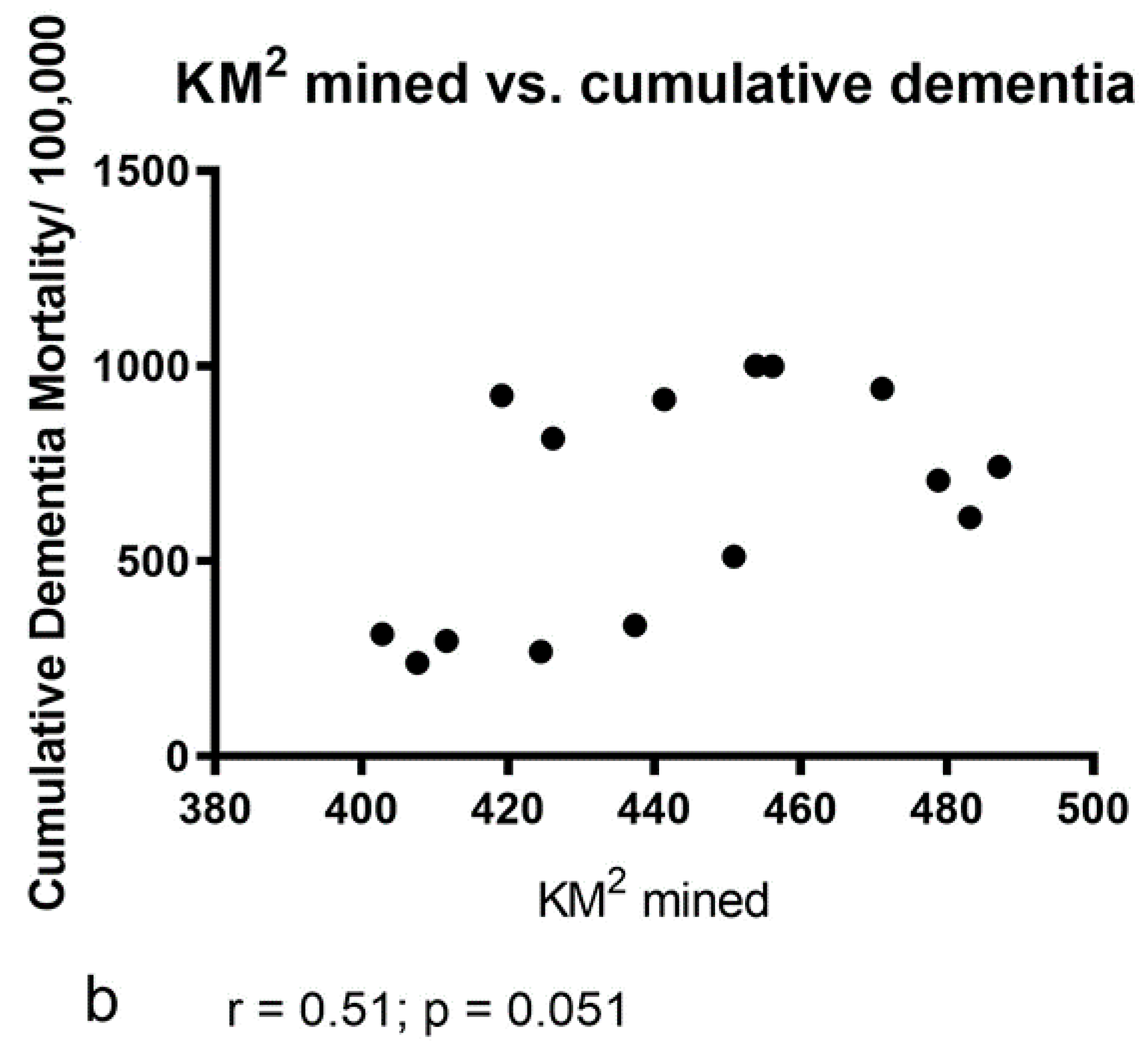
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ahern, M.M.; Hendryx, M.; Conley, J.; Fedorko, E.; Ducatman, A.; Zullig, K.J. The association between mountaintop mining and birth defects among live births in central Appalachia, 1996–2003. Environ. Res. 2011, 111, 838–846. [Google Scholar] [CrossRef] [PubMed]
- Esch, L.; Hendryx, M. Chronic cardiovascular disease mortality in mountaintop mining areas of central Appalachian states. J. Rural Health 2011, 27, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Hendryx, M.; Wolfe, L.; Luo, J.; Webb, B. Self-reported cancer rates in two rural areas of West Virginia with and without mountaintop coal mining. J. Community Health 2012, 37, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Zullig, K.J.; Hendryx, M. Health-related quality of life among central Appalachian residents in mountaintop mining counties. Am. J. Public Health 2011, 101, 848–853. [Google Scholar] [CrossRef] [PubMed]
- Boyles, A.L.; Blain, R.B.; Rochester, J.R.; Avanasi, R.; Goldhaber, S.B.; McComb, S.; Holmgren, S.D.; Masten, S.A.; Thayer, K.A. Systematic review of community health impacts of mountaintop removal mining. Environ. Int. 2017, 107, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Cama, T. Trump Administration Halts Research on Mountaintop Removal Coal Mining. The Hill 2017. Available online: https://thehill.com/policy/energy-environment/347374-trump-administration-halts-research-on-mountaintop-removal-coal (accessed on 18 December 2018).
- Fears, D. Trump administration halted a study of mountaintop coal mining’s health effects. The Washington Post, 21 August 2017. [Google Scholar]
- Associated Press. Groups Warn of Potential Risks for Those Living Close to Mines. The Dominion Post, 29 May 2017. [Google Scholar]
- Anandwala, R.; The National Academy News Division, Washington, DC, USA; Salm, A.K.; West Virginia University School of Medicine, Morgantown, WV, USA. Personal communication, 2018.
- Kurth, L.M.; McCawley, M.; Hendryx, M.; Lusk, S. Atmospheric particulate matter size distribution and concentration in West Virginia coal mining and non-mining areas. J. Exposure Sci. Environ. 2014, 24, 405–411. [Google Scholar] [CrossRef]
- Ayers, H.; Boyer, J.; Feeney, P.; McGrath, L.; Owen, S.; Rodgers, K.; Wasson, M. Appalachian Coalfield Delegation Position Paper on Sustainable Energy. In Proceedings of the United Nations Commission on Sustainable Development 15th Session, New York, NY, USA, 30 April–11 May 2007; pp. 1–22. [Google Scholar]
- MSHA (Mine Safety and Health Administration). Arlington, VA. U.S. Dept. of Labor, Effects of Blasting on Air Quality. 2013. Available online: http://www.msha.gov/illness prevention/healthtopics/blasting.htm (accessed on 9 December 2017).
- Kurth, L.; Kolker, A.; Engle, M.; Geboy, N.; Hendryx, M.; Orem, W.; McCawley, M.; Crosby, L.; Tatu, C.; Varonka, M.; et al. Atmospheric particulate matter in proximity to mountaintop coal mines: Sources and potential environmental and human health impacts. Environ. Geochem. Health 2015, 37, 529–544. [Google Scholar] [CrossRef]
- Ghose, M.K. Generation and quantification of hazardous dusts from coal mining in the Indian context. Environ. Monitor. Assess. 2007, 130, 35–45. [Google Scholar] [CrossRef]
- Shrey, K.; Suchit, A.; Deepika, D.; Shruti, K.; Vibha, R. Air pollutants: The key stages in the pathway towards the development of cardiovascular disorders. Environ. Toxicol. Pharmacol. 2011, 31, 1–9. [Google Scholar] [CrossRef]
- Favarato, G.; Anderson, H.R.; Atkinson, R.; Fuller, G.; Mills, I.; Walton, H. Traffic-related pollution and asthma prevalence in children. Quantification of associations with nitrogen dioxide. Air Qual. Atmos. Health 2014, 7, 459–466. [Google Scholar] [CrossRef] [Green Version]
- Aneja, V.P.; Pillai, P.R.; Isherwood, A.; Morgan, P.; Aneja, S.P. Particulate matter pollution in the coal-producing regions of the Appalachian Mountains: Integrated ground-based measurements and satellite analysis. J. Air Waste Manag. Assoc. 2017, 67, 421–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCawley, M.; Knuckles, T. Toxicology of Nano- and Ultrafine Particles. In Toxicology Principles for the Industrial Hygienist, 2nd ed.; Lutrell, W.E., Jederberg, W.W., Still, K.R., Eds.; American Industrial Hygiene Association: Falls Church, VA, USA, 2019; Chapter 24. [Google Scholar]
- Chen, H.; Kwong, J.C.; Copes, R.; Tu, K.; Villeneuve, P.J.; van Donkelaar, A.; Hystad, P.; Martin, R.V.; Murray, B.J.; Jessiman, B.; et al. Living near major roads and the incidence of dementia, Parkinson’s disease, and multiple sclerosis: A population-based cohort study. Lancet 2017, 389, 718–726. [Google Scholar] [CrossRef]
- Kioumourtzoglou, M.A.; Schwartz, J.D.; Weisskopf, M.G.; Melly, S.J.; Wang, Y.; Dominici, F.; Zanobetti, A. Long-term PM2.5 Exposure and neurological hospital admissions in the northeastern United States. Environ. Health Perspect 2016, 124, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Hendryx, M. Personal and family health in rural areas of Kentucky with and without mountaintop coal mining. J. Rural Health 2013, 29 (Suppl. 1), s79–s88. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Saffari, A.; Sioutas, C.; Forman, H.J.; Morgan, T.E.; Finch, C.E. Nanoscale particulate matter from urban traffic rapidly induces oxidative stress and inflammation in olfactory epithelium with concomitant effects on brain. Environ. Health Perspect. 2016, 124, 1537–1546. [Google Scholar] [CrossRef] [PubMed]
- Oberdorster, G.; Sharp, Z.; Atudorei, V.; Elder, A.; Gelein, R.; Kreyling, W.; Cox, C. Translocation of inhaled ultrafine particles to the brain. Inhal. Toxicol. 2004, 16, 437–445. [Google Scholar] [CrossRef]
- Heusinkveld, H.J.; Wahle, T.; Campbell, A.; Westerink, R.H.; Tran, L.; Johnston, H.; Stone, V.; Cassee, F.R.; Schins, R.P. Neurodegenerative and neurological disorders by small inhaled particles. Neurotoxicology 2016, 56, 94–106. [Google Scholar] [CrossRef]
- Power, M.C.; Adar, S.D.; Yanosky, J.D.; Weuve, J. Exposure to air pollution as a potential contributor to cognitive function, cognitive decline, brain imaging, and dementia: A systematic review of epidemiologic research. Neurotoxicology 2016, 56, 235–253. [Google Scholar] [CrossRef] [Green Version]
- Allen, J.L.; Klocke, C.; Morris-Schaffer, K.; Conrad, K.; Sobolewski, M.; Cory-Slechta, D.A. Cognitive effects of air pollution exposures and potential mechanistic underpinnings. Curr. Environ. Health Rep. 2017, 4, 180–191. [Google Scholar] [CrossRef]
- Xu, X.; Ha, S.U.; Basnet, R. A review of epidemiological research on adverse neurological effects of exposure to ambient air pollution. Front. Public Health 2016, 4, 157. [Google Scholar] [CrossRef]
- Cacciottolo, M.; Wang, X.; Driscoll, I.; Woodward, N.; Saffari, A.; Reyes, J.; Serre, M.L.; Vizuete, W.; Sioutas, C.; Morgan, T.E.; et al. Particulate air pollutants, APOE alleles and their contributions to cognitive impairment in older women and to amyloidogenesis in experimental models. Translat. Psychiat. 2017, 7, e1022. [Google Scholar] [CrossRef] [PubMed]
- Calderon-Garciduenas, L.; Franco-Lira, M.; Henriquez-Roldan, C.; Osnaya, N.; Gonzalez-Maciel, A.; Reynoso-Robles, R.; Villarreal-Calderon, R.; Herritt, L.; Brooks, D.; Keefe, S.; et al. Urban air pollution: Influences on olfactory function and pathology in exposed children and young adults. Exp. Toxicol. Pathol. 2010, 62, 91–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calderon-Garciduenas, L.; Solt, A.C.; Henriquez-Roldan, C.; Torres-Jardon, R.; Nuse, B.; Herritt, L.; Villarreal-Calderon, R.; Osnaya, N.; Stone, I.; Garcia, R.; et al. Long-term air pollution exposure is associated with neuroinflammation, an altered innate immune response, disruption of the blood-brain barrier, ultrafine particulate deposition, and accumulation of amyloid beta-42 and alpha-synuclein in children and young adults. Toxicol. Pathol. 2008, 36, 289–310. [Google Scholar] [PubMed]
- Block, M.L.; Calderon-Garciduenas, L. Air pollution: Mechanisms of neuroinflammation and CNS disease. Trends Neurosc. 2009, 32, 506–516. [Google Scholar] [CrossRef]
- Pearce, N. The ecological fallacy strikes back. J. Epidemiol. Community Health 2000, 54, 326–327. [Google Scholar] [CrossRef] [Green Version]
- Anderson, R. Coding and Classifying Causes of Death: Trends and International Differences. In International Handbook of Adult Mortality, 2nd ed.; Rogers, R., Crimmins, E., Eds.; Springer Science and Business Media: Berlin, Germany, 2011; pp. 467–488. [Google Scholar]
- De Roos, A.; van der Grond, J.; Mitchell, G.; Westenberg, J. Magnetic resonance imaging of cardiovascular function and the brain: Is dementia a cardiovascular-driven disease? Circulation 2017, 135, 2178–2195. [Google Scholar] [CrossRef]
- Exalto, L.G.; Biessels, G.J.; Karter, A.J.; Huang, E.S.; Katon, W.J.; Minkoff, J.R.; Whitmer, R.A. Risk score for prediction of 10 year dementia risk in individuals with type 2 diabetes: A cohort study. Lancet Diabetes Endocrinol. 2013, 1, 183–190. [Google Scholar] [CrossRef]
- CDC WONDER Database, Centers for Disease Control and Prevention, National Center for Health Statistics. Underlying Cause of Death 1999–2016 on CDC WONDER Online Database, Released December 2017. Available online: http://wonder.cdc.gov/ucd-icd10.html (accessed on 4 April 2018).
- Ngandu, T.; von Strauss, E.; Helkala, E.L.; Winblad, B.; Nissinen, A.; Tuomilehto, J.; Soininen, H.; Kivipelto, M. Education and dementia: What lies behind the association? Neurology 2007, 69, 1442–1450. [Google Scholar] [CrossRef]
- Marden, J.R.; Tchetgen Tchetgen, E.J.; Kawachi, I.; Glymour, M.M. Contribution of socioeconomic status at 3 life-course periods to late-life memory function and decline: Early and late predictors of dementia risk. Am. J. Epidemiol. 2017, 186, 805–814. [Google Scholar] [CrossRef]
- Pericak, A.A.; Thomas, C.J.; Kroodsma, D.A.; Wasson, M.F.; Ross MR, V.; Clinton, N.E.; Campagna, D.J.; Franklin, Y.; Bernhardt, E.S.; Amos, J.F. Mapping the yearly extent of surface coal mining in Central Appalachia using Landsat and Google Earth Engine. PLoS ONE 2018, 13, e0197758. [Google Scholar] [CrossRef]
- Taylor, C.A.; Greenlund, S.F.; McGuire, L.C.; Lu, H.; Croft, J.B. Deaths from Alzheimer’s Disease—United States, 1999–2014. Morbid. Mortal. Wkly. Rep. 2017, 66, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, C.; Rosenorn-Lanng, E. Neurological deaths of American adults (55–74) and the over 75’s by sex compared with 20 Western countries 1989–2010: Cause for concern. Surg. Neurol. Int. 2015, 6, 123. [Google Scholar] [CrossRef] [PubMed]
- Blakely, T.A.; Woodward, A.J. Ecological effects in multi-level studies. J. Epidemiol. Community Health 2000, 54, 367–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanobetti, A.; Dominici, F.; Wang, Y.; Schwartz, J.D. A national case-crossover analysis of the short-term effect of PM2.5 on hospitalizations and mortality in subjects with diabetes and neurological disorders. Environ. Health 2014, 13, 38. [Google Scholar] [CrossRef] [PubMed]
- Sperling, R.A.; Aisen, P.S.; Beckett, L.A.; Bennett, D.A.; Craft, S.; Fagan, A.M.; Iwatsubo, T.; Jack, C.R., Jr.; Kaye, J.; Montine, T.J.; et al. Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 280–292. [Google Scholar] [CrossRef] [PubMed]
- Moulton, P.V.; Yang, W. Air pollution, oxidative stress, and Alzheimer’s disease. J. Environ. Public Health 2012, 2012, 472751. [Google Scholar] [CrossRef]
- Woodward, N.C.; Levine, M.C.; Haghani, A.; Shirmohammadi, F.; Saffari, A.; Sioutas, C.; Morgan, T.E.; Finch, C.E. Toll-like receptor 4 in glial inflammatory responses to air pollution in vitro and in vivo. J. Neuroinflam. 2017, 14, 84. [Google Scholar] [CrossRef]
- Kuhn, S.; Duzel, S.; Eibich, P.; Krekel, C.; Wustemann, H.; Kolbe, J.; Martensson, J.; Goebel, J.; Gallinat, J.; Wagner, G.G.; et al. In search of features that constitute an “enriched environment” in humans: Associations between geographical properties and brain structure. Sci. Rep. 2017, 7, 11920. [Google Scholar] [CrossRef]
- Vogt, J.T.; Smith, W.B. Forest Inventory and Analysis. Fiscal Year 2016 Business Report; FS-1075; United States Department of Agriculture (USDA): Washington, DC, USA, 2017; p. 84.
- Johnson, K.A.; Fox, N.C.; Sperling, R.A.; Klunk, W.E. Brain imaging in Alzheimer disease. Cold Spring Harb. Perspect. Med. 2012, 2, a006213. [Google Scholar] [CrossRef]
- O’Neil, S.G. Superfund: Evaluating the impact of executive order 12898. Environ. Health Perspect. 2007, 115, 1087–1093. [Google Scholar] [CrossRef]
- Lewis, M.J. An Overview of Dementia: The Growing Crisis in West Virginia; West Virginia Department of Health and Human Resources: Charleston, WV, USA, 2011; pp. 1–31. [Google Scholar]
- Calderon-Garciduenas, L.; Franco-Lira, M.; Mora-Tiscareno, A.; Medina-Cortina, H.; Torres-Jardon, R.; Kavanaugh, M. Early Alzheimer’s and Parkinson’s disease pathology in urban children: Friend versus foe responses—It is time to face the evidence. BioMed Res. Internat. 2013, 2013, 161687. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Zhao, Z.; Sabirzhanov, B.; Stoica, B.A.; Kumar, A.; Luo, T.; Skovira, J.; Faden, A.I. Spinal cord injury causes brain inflammation associated with cognitive and affective changes: Role of cell cycle pathways. J. Neurosci. 2014, 34, 10989–11006. [Google Scholar] [CrossRef] [PubMed]
- Kua, E.H.; Ho, E.; Tan, H.H.; Tsoi, C.; Thng, C.; Mahendran, R. The natural history of dementia. Psychogeriatry 2014, 14, 196–201. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| County | Minimum Distinct Sites | Maximum Distinct Sites | Mean Distinct Sites | Cumulative Distinct Sites | Cumulative Dementia Deaths/100,000 |
|---|---|---|---|---|---|
| Boone | 1364 | 1556 | 1481 | 22,221 | 884.8 |
| Cabell | 277 | 390 | 335 | 5024 | 642.6 |
| Clay | 590 | 792 | 686 | 11,027 | 566.3 |
| Fayette | 1109 | 1677 | 1418 | 21,272 | 546.3 |
| Greenbrier | 1238 | 1978 | 1577 | 23,654 | 409.8 |
| Kanawha | 1393 | 1968 | 1696 | 25,437 | 711.2 |
| Lincoln | 725 | 970 | 854 | 12,810 | 788.5 |
| Logan | 1124 | 1237 | 1179 | 17,682 | 364.6 |
| Mason | 250 | 357 | 309 | 4637 | 320.6 |
| McDowell | 147 | 1236 | 1031 | 15,461 | 385.6 |
| Mercer | 338 | 486 | 417 | 6251 | 655.8 |
| Mingo | 1142 | 1321 | 1260 | 18,897 | 227.8 |
| Nicholas | 1135 | 1687 | 1426 | 21,396 | 438.3 |
| Pocahontas | 1288 | 1858 | 1562 | 23,430 | 179.7 |
| Putnam | 176 | 2058 | 358 | 5372 | 705.0 |
| Raleigh | 772 | 2579 | 1036 | 15,544 | 345.1 |
| Summers | 422 | 602 | 521 | 7823 | 435.8 |
| Wayne | 712 | 1633 | 879 | 13,189 | 496.1 |
| Wyoming | 785 | 1118 | 954 | 14,315 | 514.1 |
| Totals | 14,987 | 25,503 | 18,979 | 285,415 | 9618.00 |
| Effect | Estimate | Standard Error | DF | t Value | Pr > |t| | Alpha | Lower | Upper |
|---|---|---|---|---|---|---|---|---|
| Intercept | −26.75 | 37.71 | 49 | −0.71 | 0.481 | 0.05 | −102.55 | 49.02 |
| Mining | 15.60 | 3.14 | 49 | 4.96 | <0.0001 | 0.05 | 9.28 | 21.91 |
| Non−Mining | 0 | |||||||
| Hs | −0.031 | 0.39 | 49 | −0.08 | 0.93 | 0.05 | −0.83 | 0.77 |
| Income | 0.0007 | 0.0003 | 49 | 2.31 | 0.025 | 0.05 | 0.0001 | 0.0014 |
| Poverty | 0.93 | 0.56 | 49 | 1.64 | 0.107 | 0.05 | −0.21 | 2.0759 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salm, A.K.; Benson, M.J. Increased Dementia Mortality in West Virginia Counties with Mountaintop Removal Mining? Int. J. Environ. Res. Public Health 2019, 16, 4278. https://doi.org/10.3390/ijerph16214278
Salm AK, Benson MJ. Increased Dementia Mortality in West Virginia Counties with Mountaintop Removal Mining? International Journal of Environmental Research and Public Health. 2019; 16(21):4278. https://doi.org/10.3390/ijerph16214278
Chicago/Turabian StyleSalm, A. K., and Michael J. Benson. 2019. "Increased Dementia Mortality in West Virginia Counties with Mountaintop Removal Mining?" International Journal of Environmental Research and Public Health 16, no. 21: 4278. https://doi.org/10.3390/ijerph16214278
APA StyleSalm, A. K., & Benson, M. J. (2019). Increased Dementia Mortality in West Virginia Counties with Mountaintop Removal Mining? International Journal of Environmental Research and Public Health, 16(21), 4278. https://doi.org/10.3390/ijerph16214278