Occupational Health and Safety of Immigrant Workers in Italy and Spain: A Scoping Review

 , ,
, ,  ,
, 
Abstract
:1. Introduction
- were more often hired on precarious contracts and mainly employed in manual, low-skilled jobs;
- were concentrated in the most dangerous jobs;
- presented a higher risk of occupational injuries and diseases; and
- experienced a worsening of their working conditions during the international economic crisis of 2008–2014.
- to summarize the available literature through a scoping review;
- to identify research gaps; and
- to make recommendations for future research on occupational health and safety among immigrant workers in Italy and Spain.
2. Methods
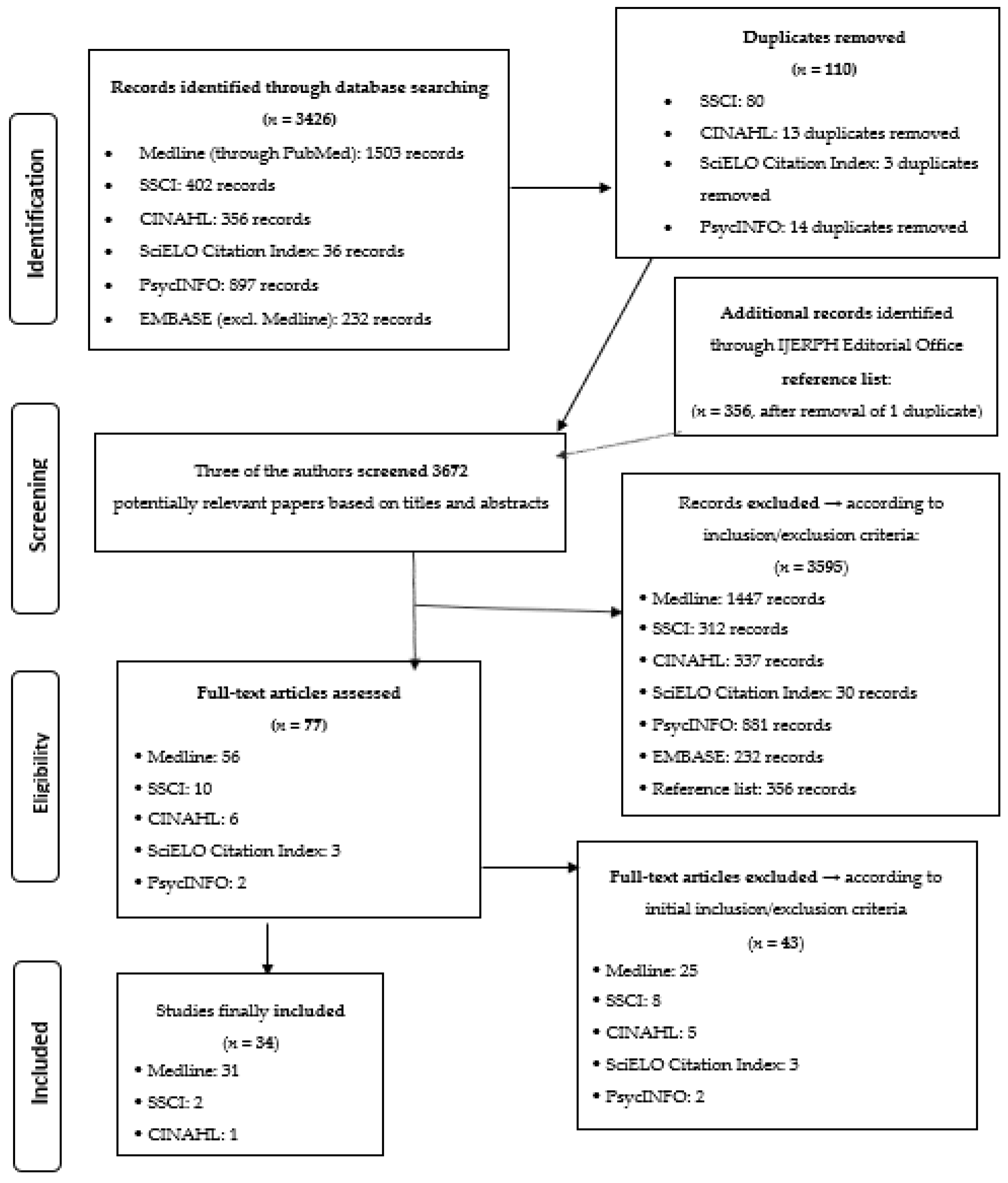
2.1. Search Strategy
2.2. Inclusion/Exclusion Criteria and Assessment
3. Results
3.1. Quantitative Studies
3.2. Qualitative Studies
4. Discussion
- Italy and Spain show similar occupational health and safety concerns and patterns of risk for fatal and non-fatal injuries; the overall numbers are impressive and demand interventions;
- the parallel economic crisis and the irregular status of many immigrant workers contributed to exacerbate occupational health and safety concerns in Italy and Spain;
- the uniqueness of the demographic migration process that happened in these two Mediterranean countries;
- compared to natives, immigrant workers in Italy and Spain showed [63,64,66,67,68,69,70,71,72,74,75,76,77,78,79,80,81,82,83,84,85,86,88,89,90,91,92,93] higher prevalence of manual work or low-skilled jobs, temporary or informal employment and low wages, perceived discrimination at work; higher physical demands, poorer environmental working conditions and more exposure to occupational risks, in particular ergonomic and psychosocial hazards; worse general and mental health and employment/working conditions, mainly due to the economic crisis [78,81,82];
- many problems have been highlighted, but scant solutions were proposed. No intervention studies are available, which could be very useful to build an evidence-based prevention of work-related injuries and diseases among immigrant workers in the workplaces, as well as to better inform health policy makers;
- more observational studies are needed with a longitudinal design, comparing the outcomes of interest in relationship to the different periods (i.e., before, during, and after) of the economic crisis. Such studies should be based on objective data and dealing preferably with occupational diseases instead of occupational injuries;
- more studies should analyze the potential role played by the migration status (i.e., documented vs undocumented) in exacerbating poor health and safety outcomes among migrant workers in Italy and Spain;
- the great majority of the included studies did not consider the heterogeneity of migrant workforce, with no sub-analyses for ethnic group and for length of stay in the host country; these are possible conditions of different vulnerability to occupational health and safety risks.
5. Conclusions
- promotion of migrant workers’ wellbeing and prevention of migrant workers’ disorders in the workplaces, by means of focused and multidisciplinary risk assessments;
- concrete and timely responses to migrant workers’ health needs, through largely accessible and focused health surveillance, fitness for work, case management and health promotion performed by a qualified, accountable, and motivated occupational physician;
- more collaborative dialogue with general practitioners;
- more social protection and compensation opportunities for work-related disorders in migrant workers in general, and for female domestic workers and caregivers in particular;
- the already existing and protecting legislation about occupational health and safety of immigrant workers should be regularly and proactively applied in the workplaces;
- free access to public occupational health services should be provided to migrant workers, particularly undocumented ones.
Author Contributions
Funding
Conflicts of Interest
References
- International Labour Organization (ILO). Global Estimates on International Migrant Workers–Results and Methodology. 2018. Available online: https://www.ilo.org/global/publications/books/WCMS_652001/lang--en/index.htm (accessed on 8 August 2019).
- WHO Regional Office for Europe. Report on the Health of Refugees and Migrants in the WHO European Region. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/311347/9789289053846-eng.pdf?sequence=1&isAllowed=y (accessed on 8 August 2019).
- Bettin, G.; Cela, E. The evolution of migration flows in Europe and Italy. J. Appl. Econ. 2014, 33, 37–63. [Google Scholar]
- Larramona, G. Out-migration of immigrants in Spain. Population 2013, 68, 213–235. [Google Scholar] [CrossRef]
- Moyce, S.C.; Schenker, M. Migrant workers and their occupational health and safety. Annu. Rev. Public Health 2018, 39, 351–365. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Women on the Move-Migration, Care Work and Health. 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/259463/9789241513142-eng.pdf?sequence=1 (accessed on 13 October 2019).
- Sterud, T.; Tynes, T.; Sivesind Mehlum, I.; Veiersted, K.B.; Bergbom, B.; Airila, A.; Johansson, B.; Brendler-Lindqvist, M.; Hviid, K.; Flyvholm, M.-A. A systematic review of working conditions and occupational health among immigrants in Europe and Canada. BMC Public Health 2018, 18, 770. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe. Health Evidence Network Synthesis Report 43-Public Health Aspects of Migrant Health: A Review of the Evidence on Health Status for Labour Migrants in the European Region. 2015. Available online: http://www.euro.who.int/__data/assets/pdf_file/0004/289246/WHO-HEN-Report-A5-2-Refugees_FINAL.pdf (accessed on 8 August 2019).
- Ronda-Pérez, E.; Agudelo-Suárez, A.; López-Jacob, M.J.; García, A.M.; Benavides, F.G. Scoping review about working conditions and health of immigrant workers in Spain. Rev. Esp. Salud Pública 2014, 88, 703–714. [Google Scholar] [CrossRef] [PubMed]
- Bena, A.; Giraudo, M. The health of foreign workers: An Italian and international priority. Recenti Prog. Med. 2017, 108, 303–306. [Google Scholar] [PubMed]
- Ahonen, E.Q.; Benavides, F.G.; Benach, J. Immigrant populations, work and health—A systematic literature review. Scand. J. Work Environ. Health 2007, 33, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Villarroel, N.; Hannigan, A.; Severoni, S.; Puthoopparambil, S.; MacFarlane, A. Migrant health research in the Republic of Ireland: A scoping review. BMC Public Health 2019, 19, 324. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, S.; Rustage, K.; Nellums, L.B.; McAlpine, A.; Pocock, N.; Devakumar, D.; Aldridge, R.W.; Abubakar, I.; Kristensen, K.L.; Himmels, J.W.; et al. Occupational health outcomes among international migrant workers: A systematic review and meta-analysis. Lancet Glob. Health 2019, 7, e872–e882. [Google Scholar] [CrossRef]
- ISMU Foundation–Initiatives and Studies on Multi-Ethnicity; Twenty-fourth Italian Report on Migrations; Angeli, F. (Ed.) Milan, Italy, 2018. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Int. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Int. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Agudelo-Suárez, A.; Ronda-Pérez, E.; Gil-González, D.; Vives-Cases, C. A group of Colombian immigrants’ self-perception regarding working conditions and health in Alicante, Spain. Rev. Salud Publica 2008, 10, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Ahonen, E.Q.; Benavides, F.G. Risk of fatal and non-fatal occupational injury in foreign workers in Spain. J. Epidemiol. Community Health 2006, 60, 424–426. [Google Scholar] [CrossRef] [PubMed]
- Ahonen, E.Q.; Zanoni, J.; Forst, L.; Ochsner, M.; Kimmel, L.; Martino, C.; Ringholm, E.; Rodríguez, E.; Kader, A.; Sokas, R. Evaluating goals in worker health protection using a participatory design and an evaluation checklist. New Solut. J. Environ. Occup. Health Policy 2013, 23, 537–560. [Google Scholar] [CrossRef] [PubMed]
- Bacciconi, M.; Patussi, V.; Barbina, P.; Calabresi, C.; Gallieri, D.; Coppola, N.; Sarto, F.; Falasca, P.; Di Tommaso, F.; Falasca, G. Occupational accidents among immigrant women in the Italian North-Eastern regions (Veneto and Friuli Venezia Giulia). Epidemiol. Prev. 2006, 30, 33–39. [Google Scholar] [PubMed]
- Benach, J.; Julià, M.; Tarafa, G.; Mir, J.; Molinero, E.; Vives, A. Multidimensional measurement of precarious employment: Social distribution and its association with health in Catalonia (Spain). Gac. Sanit. 2015, 29, 375–378. [Google Scholar] [CrossRef] [PubMed]
- Benavides, F.G.; Ahonen, E.Q.; Bosch, C. Risk of occupational injury in foreign workers in Spain [2003 and 2004]. Gac. Sanit. 2008, 22, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Biggi, N. Fast food: An example of multi-ethnic service. G. Ital. Med. Lav. Ergon. 2011, 33, 37–40. [Google Scholar] [PubMed]
- Borrell, C.; Muntaner, C.; Solà, J.; Artazcoz, L.; Puigpinós, R.; Benach, J.; Noh, S. Immigration and self-reported health status by social class and gender: The importance of material deprivation, work organisation and household labour. J. Epidemiol. Community Health 2008, 62, e7. [Google Scholar] [CrossRef] [PubMed]
- Bottazzi, M.; Della Torre, L. Immigration, work and health-social, cultural and best practices in occupational medicine: The views of union patronage. G. Ital. Med. Lav. Ergon. 2011, 33, 29–32. [Google Scholar] [PubMed]
- Callejon-Ferre, A.J.; Montoya-Garcia, M.E.; Perez-Alonso, J.; Rojas-Sola, J.I. The psychosocial risks of farm workers in south-east Spain. Saf. Sci. 2015, 78, 77–90. [Google Scholar] [CrossRef]
- Capacci, F.; Carnevale, F.; Gazzano, N. The health of foreign workers in Italy. Int. J. Occup. Environ. Health 2005, 11, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Comba, P.; Merler, E.; Pasetto, R. Asbestos-related diseases in Italy: Epidemiologic evidences and public health issues. Int. J. Occup. Environ. Health 2005, 11, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Delclos, C.E.; Benavides, F.G.; García, A.M.; López-Jacob, M.J.; Ronda, E. From questionnaire to database: Field work experience in the “Immigration, work and health survey” (ITSAL Project). Gac. Sanit. 2011, 25, 419–422. [Google Scholar]
- Di Napoli, A.; Gatta, R.; Rossi, A.; Perez, M.; Costanzo, G.; Mirisola, C.; Petrelli, A. Perceived discrimination at work for being an immigrant: A study on self-perceived mental health status among immigrants in Italy. Epidemiol. Prev. 2017, 41, 33–40. [Google Scholar] [PubMed]
- Di Rosa, M.; Melchiorre, M.G.; Lucchetti, M.; Lamura, G. The impact of migrant work in the elder care sector: Recent trends and empirical evidence in Italy. Eur. J. Soc. Work 2012, 15, 9–27. [Google Scholar] [CrossRef]
- Dominguez-Mujica, J.; Guerra-Talavera, R.; Parreno-Castellano, J.M. Migration at a time of global economic crisis: The situation in Spain. Int. Migr. 2014, 52, 113–127. [Google Scholar] [CrossRef]
- Font, A.; Moncada, S.; Llorens, C.; Benavides, F.G. Psychosocial factor exposures in the workplace: Differences between immigrants and Spaniards. Eur. J. Public Health 2012, 22, 688–693. [Google Scholar] [CrossRef] [PubMed]
- Fullin, G. Unemployment trap or high job turnover? Ethnic penalties and labour market transitions in Italy. Int. J. Comp. Sociol. 2011, 52, 284–305. [Google Scholar] [CrossRef]
- Fullin, G.; Reyneri, E. Low unemployment and bad jobs for new immigrants in Italy. Int. Migr. 2011, 49, 118–147. [Google Scholar] [CrossRef]
- Gotsens, M.; Malmusi, D.; Villarroel, N.; Vives-Cases, C.; Garcia-Subirats, I.; Hernando, C.; Borrell, C. Health inequality between immigrants and natives in Spain: The loss of the healthy immigrant effect in times of economic crisis. Eur. J. Public Health 2015, 25, 923–929. [Google Scholar] [CrossRef] [PubMed]
- Hoggart, K.; Mendoza, C. African immigrant workers in Spanish agriculture. Sociol. Rural. 1999, 39, 538–562. [Google Scholar] [CrossRef]
- López-Jacob, M.J.; Safont, E.C.; García, A.M.; Garí, A.; Agudelo-Suárez, A.; Gil, A.; Benavides, F.G. Participation and influence of migrant workers on working conditions: A qualitative approach. New Solut. 2010, 20, 225–238. [Google Scholar] [CrossRef] [PubMed]
- Marcacci, T.; Chierzi, F.; Ferretti, M.; Allegri, F.; Storbini, V.; Menchetti, M.; Berardi, D.; Tarricone, I. Comunicazione, competenza culturale e sicurezza nei luoghi di lavoro: Una ricerca-intervento per I’applicazione del modello C.I.A.O. Minerva Psichiatr. 2013, 54, 221–232. [Google Scholar]
- Martinez-Brawley, E.; Gualda, E. US/Spanish comparisons on temporary immigrant workers: Implications for policy development and community practice. Eur. J. Soc. Work 2006, 9, 59–84. [Google Scholar] [CrossRef]
- Meardi, G.; Martin, A.; Riera, M.L. Constructing uncertainty: Unions and migrant labour in construction in Spain and the UK. J. Ind. Relat. 2012, 54, 5–21. [Google Scholar] [CrossRef]
- Moreno-Jimenez, M.P.; Hidalgo, M.C. Measurement and prediction of satisfaction with life in immigrant workers in Spain. Differences according to their administrative status. An. Psicol. 2011, 27, 179–185. [Google Scholar]
- Mosconi, G.; Riva, M.M. Immigrants and health in construction industry: Results of a health survey of a sample of construction workers in the province of Bergamo. G. Ital. Med. Lav. Ergon. 2011, 33, 33–36. [Google Scholar] [PubMed]
- Motellon, E.; Lopez-Bazo, E. Job loss among immigrant and native workers: Evidence from Spain’s economic downturn. Soc. Indic. Res. 2015, 120, 345–371. [Google Scholar] [CrossRef] [Green Version]
- Mousaid, S.; De Moortel, D.; Malmusi, D.; Vanroelen, C. New perspectives on occupational health and safety in immigrant populations: Studying the intersection between immigrant background and gender. Ethn. Health 2016, 21, 251–267. [Google Scholar] [CrossRef] [PubMed]
- Parra, A.; Fernández Baraibar, J.; García López, V.; Ayestarán, J.R.; Extremiana, E. Labour market, occupational health and immigration. An. Sist. Sanit. Navar. 2006, 29, 77–95. [Google Scholar] [PubMed]
- Parra Osés, Á.; García López, V.; Fernández Baraibar, J.; Ayestarán Ruiz Bazán, J.R. La siniestralidad laboral en la población inmigrante de Navarra en el 2006: Una aproximación a sus causas. Med. Segur. Trab. 2008, 54, 55–78. [Google Scholar] [CrossRef]
- Pérez, E.R.; Benavides, F.G.; Levecque, K.; Love, J.G.; Felt, E.; Van Rossem, R. Differences in working conditions and employment arrangements among migrant and non-migrant workers in Europe. Ethn. Health 2012, 17, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, A.; Di Napoli, A.; Rossi, A.; Costanzo, G.; Mirisola, C.; Gargiulo, L. The variation in the health status of immigrants and italians during the global crisis and the role of socioeconomic factors. Int. J. Equity Health 2017, 16, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porru, S.; Arici, C. Immigration and work. Roles and opportunities for occupational medicine in the health and safety of migrant workers. Med. Lav. 2010, 101, 70–77. [Google Scholar] [PubMed]
- Porru, S.; Arici, C. Occupational health and immigration: Skills, perspectives and areas of intervention. G. Ital. Med. Lav. Ergon. 2011, 33, 16–21. [Google Scholar] [PubMed]
- Porthé, V.; Ahonen, E.; Vázquez, M.L.; Pope, C.; Agudelo, A.A.; García, A.M.; Amable, M.; Benavides, F.G.; Benach, J. ITSAL project extending a model of precarious employment: A qualitative study of immigrant workers in Spain. Am. J. Ind. Med. 2010, 53, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Porthé, V.; Benavides, F.G.; Vázquez, M.L.; Ruiz-Frutos, C.; García, A.M.; Ahonen, E.; Agudelo-Suárez, A.A.; Benach, J.; por el proyecto ITSAL. Precarious employment in undocumented immigrants in Spain and its relationship with health. Gac. Sanit. 2009, 23, 107–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes-Uruena, J.M.; Noori, T.; Pharris, A.; Jansà, J.M. New times for migrants’ health in Europe. Rev. Esp. Sanid. Penit. 2014, 16, 48–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarcella, C.; Benedetti, L.; Comincini, F.; El Hamad, I.; Magoni, M.; Provasi, M.; Sottini, D. The role of the ASL of Brescia in the health and safety of immigrant workers. G. Ital. Med. Lav. Ergon. 2011, 33, 22–25. [Google Scholar] [PubMed]
- Solé, M.; Rodríguez, M. Disparities in the effect of working conditions on health between immigrant and native-born populations in Spain. Gac. Sanit. 2010, 24, 145–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soler-González, J.; Serna, M.C.; Bosch, A.; Ruiz, M.C.; Huertas, E.; Rué, M. Sick leave among native and immigrant workers in Spain-a 6-month follow-up study. Scand. J. Work Environ. Health 2008, 34, 438–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somaruga, C.; Troja Martinazzoli, M.G.; Brambilla, G.; Colosio, C. Migrant workers in agriculture and animal husbandry: Experiences of health surveillance. G. Ital. Med. Lav. Ergon. 2011, 33, 41–43. [Google Scholar] [PubMed]
- Vázquez, M.L.; Vargas, I.; Aller, M.B. The impact of the economic crisis on the health and healthcare of the immigrant population. SESPAS report 2014. Gac. Sanit. 2014, 28, 142–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agudelo-Suárez, A.A.; Benavides, F.G.; Felt, E.; Ronda-Pérez, E.; Vives-Cases, C.; García, A.M. Sickness presenteeism in Spanish-born and immigrant workers in Spain. BMC Public Health 2010, 10, 791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agudelo-Suárez, A.A.; Ronda-Pérez, E.; Gil-González, D.; Vives-Cases, C.; García, A.M.; García-Benavides, F.; Ruiz-Frutos, C.; López-Jacob, M.J.; Porthé, V.; Sousa, E. The migratory process, working conditions and health in immigrant workers in Spain (the ITSAL project). Gac. Sanit. 2009, 23, 115–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agudelo-Suárez, A.A.; Ronda-Pérez, E.; Gil-González, D.; Vives-Cases, C.; García, A.M.; Ruiz-Frutos, C.; Felt, E.; Benavides, F.G. The effect of perceived discrimination on the health of immigrant workers in Spain. BMC Public Health 2011, 11, 652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agudelo-Suárez, A.A.; Ronda, E.; Vázquez-Navarrete, M.L.; García, A.M.; Martínez, J.M.; Benavides, F.G. Impact of economic crisis on mental health of migrant workers: What happened with migrants who came to Spain to work? Int. J. Public Health 2013, 58, 627–631. [Google Scholar] [CrossRef] [PubMed]
- Benazizi, I.; Ronda-Pérez, E.; Ortíz-Moncada, R.; Martínez-Martínez, J.M. Influence of employment conditions and length of residence on adherence to dietary recommendations in immigrant workers in Spain. Int. J. Environ. Res. Public Health 2018, 15, 2488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cayuela, A.; Malmusi, D.; López-Jacob, M.J.; Gotsens, M.; Ronda, E. The impact of education and socioeconomic and occupational conditions on self-perceived and mental health inequalities among immigrants and native workers in Spain. J. Immigr. Minor. Health 2015, 17, 1906–1910. [Google Scholar] [CrossRef] [PubMed]
- Cayuela, A.; Martínez, J.M.; Ronda, E.; Delclos, G.L.; Conway, S. Assessing the influence of working hours on general health by migrant status and family structure: The case of Ecuadorian-, Colombian-, and Spanish-born workers in Spain. Public Health 2018, 163, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Conway, S.H.; Cayuela, A.; Delclos, G.L.; Pompeii, L.A.; Ronda, E. Association between long work hours and poor self-reported general health among Latin American immigrant and native workers in the United States and Spain. Am. J. Ind. Med. 2016, 59, 1105–1111. [Google Scholar] [CrossRef] [PubMed]
- Del Amo, J.; Jarrín, I.; García-Fulgueiras, A.; Ibáñez-Rojo, V.; Alvarez, D.; Rodríguez-Arenas, M.A.; García-Pina, R.; Fernández-Liria, A.; García-Ortúzar, V.; Díaz, D.; et al. Mental health in Ecuadorian migrants from a population-based survey: The importance of social determinants and gender roles. Soc. Psychiatr. Psychiatr. Epidemiol. 2011, 46, 1143–1152. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Serrano, L. Immigrants, natives and job quality: Evidence from Spain. Int. J. Manpow. 2013, 34, 753–775. [Google Scholar] [CrossRef]
- Font, A.; Moncada, S.; Benavides, F.G. The relationship between immigration and mental health: What is the role of workplace psychosocial factors. Int. Arch. Occup. Environ. Health 2012, 85, 801–806. [Google Scholar] [CrossRef] [PubMed]
- López-Jacob, M.J.; Ahonen, E.; García, A.M.; Gil, A.; Benavides, F.G. Occupational injury in foreign workers by economic activity and autonomous community (Spain 2005). Rev. Esp. Salud Publica 2008, 82, 179–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Carceles, M.D.; Medina, M.D.; Perez-Flores, D.; Noguera, J.A.; Pereniguez, J.E.; Madrigal, M.; Luna, A. Screening for hazardous drinking in migrant workers in southeastern Spain. J. Occup. Health 2014, 56, 39–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robert, G.; Martínez, J.M.; García, A.M.; Benavides, F.G.; Ronda, E. From the boom to the crisis: Changes in employment conditions of immigrants in Spain and their effects on mental health. Eur. J. Public Health 2014, 24, 404–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronda, E.; Agudelo-Suárez, A.A.; García, A.M.; López-Jacob, M.J.; Ruiz-Frutos, C.; Benavides, F.G. Differences in exposure to occupational health risks in Spanish and foreign-born workers in Spain (ITSAL Project). J. Immigr. Minor. Health 2013, 15, 64–171. [Google Scholar] [CrossRef] [PubMed]
- Rubiales-Gutiérrez, E.; Agudelo-Suárez, A.A.; López-Jacob, M.J.; Ronda-Pérez, E. Differences in occupational accidents in Spain according to the worker’s country of origin. Salud Publica Mex. 2010, 52, 199–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solé, M.; Diaz-Serrano, L.; Rodríguez, M. Disparities in work, risk and health between immigrants and native-born Spaniards. Soc. Sci. Med. 2013, 76, 179–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa, E.; Agudelo-Suarez, A.; Benavides, F.G.; Schenker, M.; Garcia, A.M.; Benach, J.; Delclos, C.; Lopez-Jacob, M.J.; Ruiz-Frutos, C.; Ronda-Perez, E.; et al. Project, itsal immigration, work and health in Spain: The influence of legal status and employment contract on reported health indicators. Int. J. Public Health 2010, 55, 443–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torá, I.; Martínez, J.M.; Benavides, F.G.; Leveque, K.; Ronda, E. Effect of economic recession on psychosocial working conditions by workers’ nationality. Int. J. Occup. Environ. Health 2015, 21, 328–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agudelo-Suárez, A.A.; Gil-González, D.; Ronda-Pérez, E.; Porthé, V.; Paramio-Pérez, G.; García, A.M.; Garí, A. Discrimination, work and health in immigrant populations in Spain. Soc. Sci. Med. 2009, 68, 1866–1874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahonen, E.Q.; López-Jacob, M.J.; Vázquez, M.L.; Porthé, V.; Gil-González, D.; García, A.M.; Ruiz-Frutos, C.; Benach, J.; Benavides, F.G. ITSAL Project Invisible work, unseen hazards: The health of women immigrant household service workers in Spain. Am. J. Ind. Med. 2010, 53, 405–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahonen, E.Q.; Porthé, V.; Vázquez, M.L.; García, A.M.; López-Jacob, M.J.; Ruiz-Frutos, C.; Ronda-Pérez, E.; Benach, J.; Benavides, F.G. ITSAL Project. A qualitative study about immigrant workers’ perceptions of their working conditions in Spain. J. Epidemiol. Community Health 2009, 63, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Galon, T.; Briones-Vozmediano, E.; Agudelo-Suárez, A.A.; Felt, E.B.; Benavides, F.G.; Ronda, E. Understanding sickness presenteeism through the experience of immigrant workers in a context of economic crisis. Am. J. Ind. Med. 2014, 57, 950–959. [Google Scholar] [CrossRef] [PubMed]
- García, A.M.; López-Jacob, M.J.; Agudelo-Suárez, A.A.; Ruiz-Frutos, C.; Ahonen, E.Q.; Porthé, V. Occupational health of immigrant workers in Spain [ITSAL Project]: Key informants survey. Gac. Sanit. 2009, 23, 91–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronda, E.; Briones-Vozmediano, E.; Galon, T.; García, A.M.; Benavides, F.G.; Agudelo-Suárez, A.A. A qualitative exploration of the impact of the economic recession in Spain on working, living and health conditions: Reflections based on immigrant workers’ experiences. Health Expect. 2016, 19, 416–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capasso, R.; Zurlo, M.C.; Smith, A.P. Ethnicity, work-related stress and subjective reports of health by migrant workers: A multi-dimensional model. Ethn. Health 2018, 23, 174–193. [Google Scholar] [CrossRef] [PubMed]
- Cediel, N.; Conte, V.; Tomassone, L.; Tiberti, D.; Guiso, P.; Romero, J.; Villamil, L.C.; De Meneghi, D. Risk perception about zoonoses in immigrants and Italian workers in Northwestern Italy. Rev. Saude Publica 2012, 46, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Colao, A.M.; Pisciottano, V.; Giampaoletti, C.; Cenci, G. Occupational accidents among immigrant workers in the Fabriano areas. Med. Lav. 2006, 97, 787–798. [Google Scholar] [PubMed]
- Giraudo, M.; Bena, A.; Costa, G. Migrant workers in Italy: An analysis of injury risk taking into account occupational characteristics and job tenure. BMC Public Health 2017, 17, 351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patussi, V.; Barbina, P.; Barbone, F.; Valent, F.; Bubbi, R.; Caffau, C.; Driussi, C.; Munafò, G.; Rosolen, V.; Venturini, C.; et al. Comparison of the incidence rate of occupational injuries among permanent, temporary and immigrant workers in Friuli-Venezia Giulia. Epidemiol. Prev. 2008, 32, 35–38. [Google Scholar] [PubMed]
- Porru, S.; Elmetti, S.; Arici, C. Psychosocial risk among migrant workers: What we can learn from literature and field experiences. Med. Lav. 2014, 105, 109–129. [Google Scholar] [PubMed]
- Salvatore, M.A.; Baglio, G.; Cacciani, L.; Spagnolo, A.; Rosano, A. Discrimination at the workplace among immigrants in Italy. Med. Lav. 2012, 103, 249–258. [Google Scholar] [PubMed]
- Salvatore, M.A.; Baglio, G.; Cacciani, L.; Spagnolo, A.; Rosano, A. Work-related injuries among immigrant workers in Italy. J. Immigr. Minor. Health 2013, 15, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Tarricone, I.; Morgan, C.; Boydell, J.; Panigada, S.; Morigi, R.; Braca, M.; Sutti, E.; Boldri, P.; Di Forti, M.; Murray, R.M.; et al. Occupation and first episode psychosis in Northern Italy: Better outcomes for migrants. Early Interv. Psychiatry 2017, 11, 522–525. [Google Scholar]
- International Labour Organization (ILO): Integrating Labour Migration into the 2013 UN High-Level Dialogue on International Migration and Development, and the Post-2015 UN Development Agenda/ILO Position Paper. 2013. Available online: https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---migrant/documents/briefingnote/wcms_222913.pdf (accessed on 6 November 2019).


{kind=link}
| Variable | n (%) |
|---|---|
| Country | |
| Spain | 25 (74%) |
| Italy | 9 (26%) |
| Type of the study | |
| Quantitative | 28 (82%) |
| Qualitative | 6 (18%) |
| Design of the study | |
| Cross-sectional | 25 (74%) |
| Longitudinal | 9 (26%) |
| Study period (range 2000–2017) | |
| Before economic crisis (2000–2007) | 14 (41%) |
| During economic crisis (2008–2014) | 16 (47%) |
| After economic crisis (2015–2017) | 4 (12%) |
| Methods of data collection | |
| Surveys, personal interviews, focus groups | 28 (82%) |
| Objective data (i.e. occupational injury data, case series) | 6 (18%) |
| Author (Ref Number), Country, Study Period | Aim/Objectives | Method, Sample | Main Results |
|---|---|---|---|
| Before economic crisis (2000–2007) | |||
| Del Amo et al. [69], Spain, 2006–2007 | To describe the prevalence of and the risk factors for poor mental health in female and male Ecuadorian migrants in Spain. |
|
|
| Diaz-Serrano et al. [70], Spain, 2006 | To determine which of the working conditions are perceived as (dis)amenities by the different groups of workers. |
|
|
| Font et al. [71], Spain, 2004-2005 | To examine the relationship between immigration and mental health, taking into account the psychosocial factors in the workplace. |
|
|
| Solé et al. [77], Spain, 2006 | To assess disparities between immigrants and natives in the role played by working conditions in determining the occurrence of disability. |
|
|
| Patussi et al. [90], Italy, 2003 | To evaluate the difference in the frequency of occupational injuries between between permanent and temporary workers and between Italian and immigrant workers. |
|
|
| Salvatore et al. [92], Italy, 2007 | To compare the occurrence of episodes of arrogance or discrimination perceived at the workplace between documented immigrants and Italians. |
|
|
| Salvatore et al. [93], Italy, 2007 | To compare the occurrence of work-related injuries between legally residing immigrants and Italians. |
|
|
| During economic crisis (2008–2014) | |||
| Agudelo-Suárez et al. [61], Spain, 2008–2009 | To assess the extent of sickness presenteeism in a sample of Spanish-born and foreign-born workers. |
|
|
| Agudelo-Suárez et al. [62], Spain, 2008 | To describe the migratory process (reasons for migrating, time of residence), legal status and personal, working and health characteristics of immigrants with work experience in Spain. |
|
|
| Agudelo-Suárez et al. [63], Spain, 2008 | To analyze the relationship between immigrants’ perceived discrimination and various self-reported health indicators. |
|
|
| Cayuela et al. [67], Spain, 2011-2012 | To examine differences between workers related to migrant-status, self-perceived and mental health. |
|
|
| Conway et al. [68], Spain, 2011 | To assess the relationship between long work hours (LWH) and self-reported general health (SRGH). |
|
|
| Perez-Carceles et al. [73], Spain, 2010–2012 | To identify migrant workers with a hazardous drinking problem by means of a self-reported questionnaire and a biomarker and to ascertain associated risk factors. |
|
|
| Ronda et al. [75], Spain, 2008 | To compare self-reported exposure to occupational health risks in foreign-born and Spanish-born workers in Spain. |
|
|
| Rubiales-Gutiérrez et al. [76], Spain, 2008 | To compare the occupational accidents between autochthonous and immigrant workers in Spain. |
|
|
| Sousa et al. [78], Spain, 2008-2009 | To analyze the relationship of legal status and employment conditions with health indicators in foreign-born and Spanish-born workers in Spain. |
|
|
| Cediel et al. [87], Italy, 2008-2009 | To assess factors associated with a low risk perception of zoonoses in immigrant and Italian workers. |
|
|
| After economic crisis (2015–2017) | |||
| Cayuela et al. [66], Spain, 2015 | To analyze the relationship between working hours (WHs) and the likelihood of poor self-reported general health (SRGH). |
|
|
| Capasso et al. [86], Italy, 2015 | To test a multi-dimensional model in the prediction of subjectives reports of health by workers differing in ethnicity. |
|
|
| Author (Ref Number), Country, Study Period | Aim/Objectives | Method, Sample | Main Results |
|---|---|---|---|
| Before economic crisis (2000–2007) | |||
| López-Jacob et al. [72], Spain, 2005 | To compare the incidences for both fatal and non-fatal injuries in foreign workers to that of Spanish workers. |
|
|
| Colao et al. [88], Italy, 2000–2003 | To describe the trend of work accidents in the Local Health Area of Fabriano (Marche Region), during the period 2000–2003. |
|
|
| Tarricone et al. [94], Italy, 2002–2009 | To evaluate the occupational outcomes of a first episode psychosis (FEP) sample in Bologna (Northern Italy). |
|
|
| During economic crisis (2008–2014) | |||
| Agudelo-Suárez et al. [64], Spain, 2008 and 2011 | To assess changes in mental health in a sample of migrant workers after the eruption of the economic crisis in Spain. |
|
|
| Robert et al. [74], Spain, 2008 and 2011 | To evaluate the influence of changes in employment conditions on the incidence of poor mental health of immigrant workers in Spain, after a period of 3 years, in context of economic crisis. |
|
|
| Torá et al. [79], Spain, 2007 and 2011 | To assess whether the prevalence of adverse psychosocial working conditions changed for Spanish and foreign workers between 2007 (pre-economic recession) and 2011 (post-economic recession). |
|
|
| Porru et al. [91], Italy, 2001–2013 | To present data from a clinical case list of workers assessed for psychosocial issues at a Northern Italy public occupational health unit. |
|
|
| After economic crisis (2015–2017) | |||
| Benazizi et al. [65], Spain, 2015–2017 | To analyze the influence of employment conditions on adherence to dietary recommendations. |
|
|
| Giraudo et al. [89], Italy, 2017 | To study the injury risk differentials between migrants and natives. |
|
|
| Author (Ref Number), Country, Study Period | Aim/Objectives | Method, Sample | Main Results |
|---|---|---|---|
| Before economic crisis (2000–2007) | |||
| Agudelo-Suárez et al. [80], Spain, 2006–2007 | To research perceptions of discrimination and the specific relationship between discrimination in the workplace and health among Spain’s immigrant population. |
|
|
| Ahonen et al. [81], Spain, 2006–2007 | To examine the environmental, ergonomic, and psychosocial hazards and health effects identified by immigrant women working in household service in five Spanish cities. |
|
|
| Ahonen et al. [82], Spain, 2006–2007 | To explore the perceptions that immigrant workers in Spain had of their working conditions. |
|
|
| García et al. [84], Spain, 2006 | To describe the characteristics, working conditions, and occupational health situation of immigrant workers in Spain through key informants. |
|
|
| During economic crisis (2008–2014) | |||
| Galon et al. [83], Spain, 2012 | To explore perceptions about the factors that lead to presenteeism in immigrant workers considering the context of economic crisis. |
|
|
| Ronda et al. [85], Spain, 2012 | To analyse how immigrant workers in Spain experienced changes in their working and employment conditions brought about Spain’s economic recession and the impact of these changes on their living conditions and health status. |
| Participants experienced:
|
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arici, C.; Ronda-Pérez, E.; Tamhid, T.; Absekava, K.; Porru, S. Occupational Health and Safety of Immigrant Workers in Italy and Spain: A Scoping Review. Int. J. Environ. Res. Public Health 2019, 16, 4416. https://doi.org/10.3390/ijerph16224416
Arici C, Ronda-Pérez E, Tamhid T, Absekava K, Porru S. Occupational Health and Safety of Immigrant Workers in Italy and Spain: A Scoping Review. International Journal of Environmental Research and Public Health. 2019; 16(22):4416. https://doi.org/10.3390/ijerph16224416
Chicago/Turabian StyleArici, Cecilia, Elena Ronda-Pérez, Tishad Tamhid, Katsiaryna Absekava, and Stefano Porru. 2019. "Occupational Health and Safety of Immigrant Workers in Italy and Spain: A Scoping Review" International Journal of Environmental Research and Public Health 16, no. 22: 4416. https://doi.org/10.3390/ijerph16224416
APA StyleArici, C., Ronda-Pérez, E., Tamhid, T., Absekava, K., & Porru, S. (2019). Occupational Health and Safety of Immigrant Workers in Italy and Spain: A Scoping Review. International Journal of Environmental Research and Public Health, 16(22), 4416. https://doi.org/10.3390/ijerph16224416