How Attitudes toward Alcohol Policies Differ across European Countries: Evidence from the Standardized European Alcohol Survey (SEAS)

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Attitudes Toward Alcohol Policies
2.3. Country-Level Variables
2.4. Statistical Analyses
3. Results
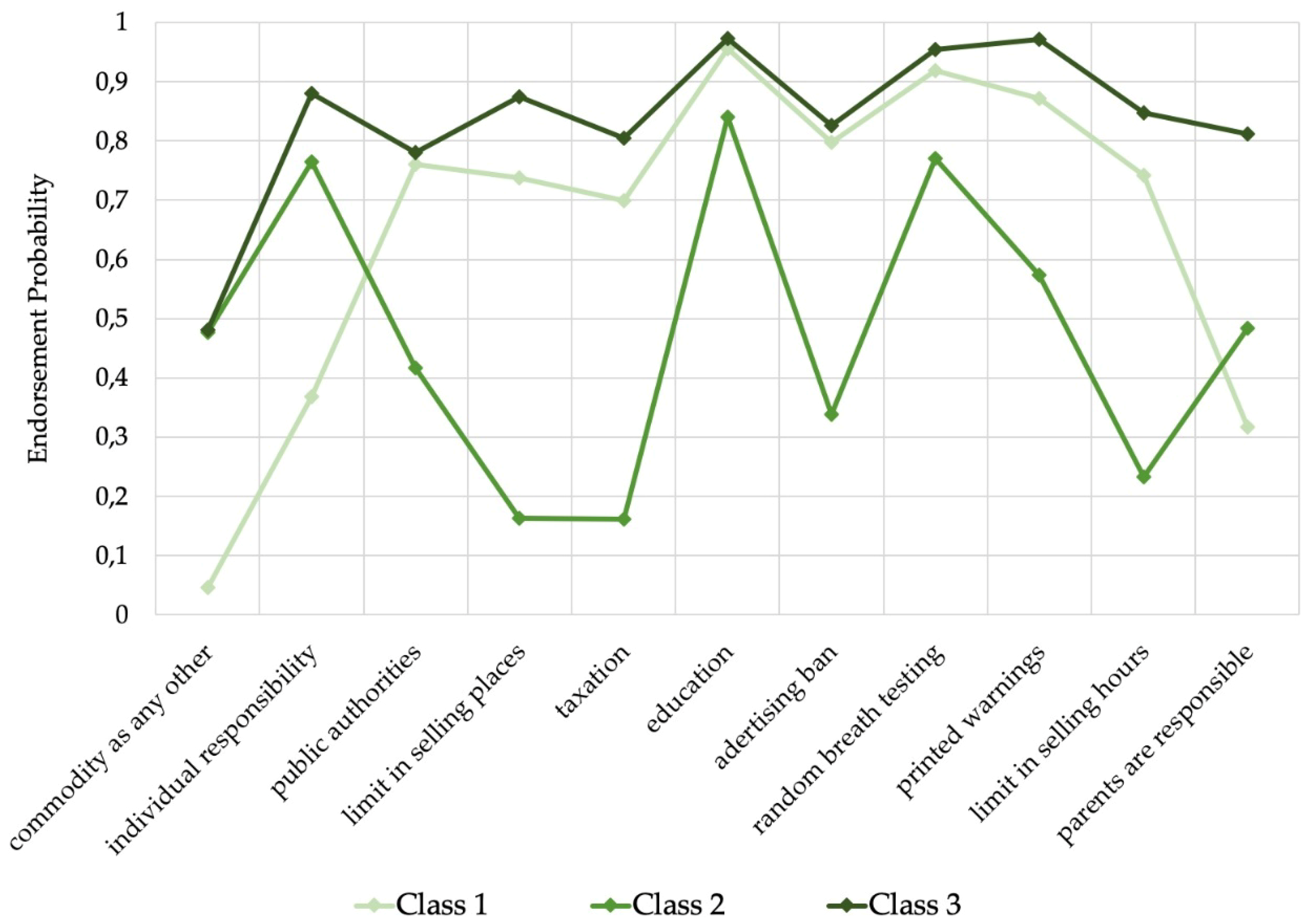
3.1. Results of the Latent Class Analysis
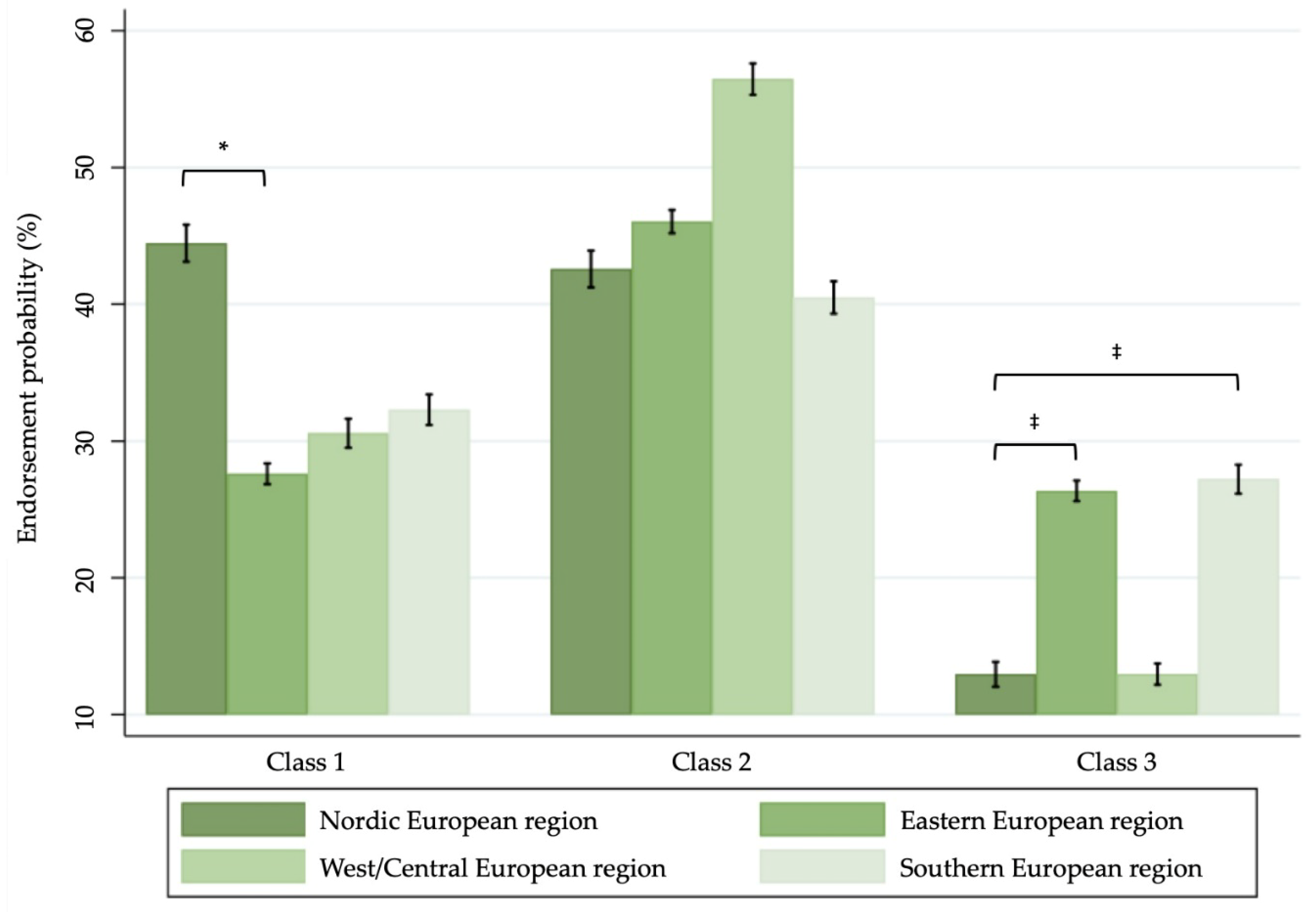
3.2. Regional Differences in Alcohol Policy Endorsement
3.3 Individual-Level Differences in Alcohol Policy Endorsement
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Status Report on Alcohol Consumption, Harm and Policy Responses in 30 European Countries; WHO European Region: Copenhagen, Denmark, 2019. [Google Scholar]
- Manthey, J.; Shield, K.D.; Rylett, M.; Hasan, O.; Probst, C.; Rehm, J. Alcohol exposure between 1990 and 2017 and forecasts until 2030: A global modelling study. Lancet 2019, 393, 2493–2502. [Google Scholar] [CrossRef]
- World Health Organization, Regional Office for Europe. European Action Plan to Reduce the Harmful Use of Alcohol, 2012–2020 [Internet]; WHO European Region: Copenhagen, Denmark, 2012; Available online: http://www.euro.who.int/data/assets/pdf_file/0008/178163/E96726.pdf (accessed on 25 March 2019).
- Chisholm, D.; Moro, D.; Bertram, M.; Pretorius, C.; Gmel, G.; Shield, K.D.; Rehm, J. Are the “best buys” for alcohol control still valid? An update on the comparative cost-effectiveness of alcohol control strategies at the global level. J. Stud. Alcohol Drugs 2018, 79, 514–522. [Google Scholar] [PubMed]
- WHO Regional Office for Europe. Policy in action. In A Tool for Measuring Alcohol Policy Implementation; WHO Regional Office for Europe: Copenhagen, Denmark, 2017. [Google Scholar]
- Anderson, P.; Chisholm, D.; Fuhr, D.C. Effectiveness and cost-effectiveness of policies and programmes to reduce the harm caused by alcohol. Lancet 2009, 373, 2234–2246. [Google Scholar] [CrossRef]
- Burton, R.; Henn, C.; Lavoie, D.; O’Connor, R.; Perkins, C.; Sweeney, K.; Greaves, F.; Ferguson, B.; Beynon, C.; Belloni, A.; et al. A rapid evidence review of the effectiveness and cost-effectiveness of alcohol control policies: An English Perspective. Lancet 2017, 389, 1558–1580. [Google Scholar] [CrossRef]
- Burstein, P. The Impact of Public Opinion on Public Policy: A Review and an Agenda. Political Res. Q. 2003, 56, 29–40. [Google Scholar] [CrossRef]
- Giesbrecht, N.; Livingston, M. Public perceptions and alcohol policies: Six case studies that examine trends and interactions. Drug Alcohol Rev. 2014, 33, 217–219. [Google Scholar] [CrossRef]
- Moskalewicz, J.; Wieczorek, Ł.; Karlsson, T.; Österberg, E. Social support for alcohol policy: Literature review. Drugs Edu. Prev. Policy 2013, 20, 361–374. [Google Scholar] [CrossRef]
- Storvoll, E.E.; Rossow, I.; Rise, J. Changes in attitudes towards restrictive alcohol policy measures: The mediating role of changes in beliefs. J. Subst. Use 2014, 19, 38–43. [Google Scholar] [CrossRef]
- Österberg, E.; Lindeman, M.; Karlsson, T. Changes in alcohol policies and public opinions in Finland 2003–2013. Drug Alcohol Rev. 2014, 33, 242–248. [Google Scholar] [CrossRef]
- Leimar, P.; Ramstedt, M.; Weibull, L. Public opinion and alcohol plicy in Sweden, 1990–2012. Nordic Stud. Alcohol Drug 2013, 30, 473–490. [Google Scholar] [CrossRef]
- Rossow, I.; Storvoll, E.E. Long-term trends in alcohol policy attitudes in Norway. Drug Alcohol Rev. 2014, 33, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Pechey, R.; Burge, P.; Mentzakis, E.; Suhrcke, M.; Marteau, T.M. Public acceptability of population-level interventions to reduce alcohol consumption: A discrete choice experiment. Soc. Sci. Med. 2014, 113, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Lovatt, M.; Eadie, D.; Dobbie, F.; Meier, P.; Holmes, J.; Hastings, G.; MacKintosh, A.M. Public attitudes towards alcohol control policies in Scotland and England: Results from a mixed-methods study. Soc. Sci. Med. 2017, 177, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Storvoll, E.E.; Moan, I.S.; Rise, J. Predicting Attitudes Toward a Restrictive Alcohol Policy: Using a Model of Distal and Proximal Predictors. Psychol. Addict. Behav. 2015, 29, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Hemström, Ö. Attitudes toward alcohol policy in six EU countries. Contemp. Drug Prob. 2002, 29, 605–618. [Google Scholar] [CrossRef]
- Elekes, Z.; Moskalewicz, J.; Tsereteli, Z. Opinions on and attitudes towards alcohol. In Comparative Monitoring of Alcohol Epidemiology Across the EU Baseline Assessment and Suggestions for Future Action Synthesis Report; Moskalewicz, J., Room, R., Thom, B., Eds.; Reducing Alcohol Related Harm (RARHA): Warszawa, Poland, 2016; pp. 209–230. [Google Scholar]
- Masyn, K.E. Latent Class Analysis and Finite Mixture Modeling. In The Oxford Handbook of Quantitative Methods Volume 2: Statistical Analysis; Little, T.D., Ed.; Oxford University Press: New York, NY, USA, 2013; Volume 2, pp. 551–611. [Google Scholar]
- Karlsson, T.; Lindeman, E.; Österberg, E. Does alcohol policy make any difference? Scales and consumption. In Alcohol Policy in Europe: Evidence from AMPHORA, 2nd ed.; Anderson, P., Braddick, F., Eds.; EU: Brussels, Belgium, 2012; pp. 17–25. Available online: http://amphoraproject.net/ (accessed on 17 April 2019).
- Papke, L.E.; Wooldridge, J.M. Econometric methods for fractional response variablies with an application to 401 (K) plan participation rates. J. Appl. Eco. 1996, 11, 619–632. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 15; StataCorp LLC: Texas, TX, USA, 2017. [Google Scholar]
- R Core Team. R: A language and environment for statistical computing. Vienna, Austria, 2019. Available online: https://www.R-project.org/ (accessed on 10 September 2019).
- Rammstedt, B.; Danner, D.; Bosnjak, M. Acquiescence response styles: A multilevel model explaining individual-level and country-level differences. Pers. Individual Differ. 2017, 107, 190–194. [Google Scholar] [CrossRef]
- Van Vaerenbergh, Y.; Thomas, T.D. Response Styles in Survey Research: A Literature Review of Antecedents, Consequences, and Remedies. Int. J. Pub. Opin. Res. 2013, 25, 195–2017. [Google Scholar] [CrossRef]
- Van Herk, H.; Poortinga, Y.H.; Verhallen, T.M.M. Response Styles In Rating Scales. Evidence of Method Bias in Data From Six EU Countries. J. Cross-Cult. Psychol. 2004, 35, 346–360. [Google Scholar] [CrossRef]
- Shield, K.D.; Rehm, J. Difficulties with telephone-based surveys on alcohol consumption in high-income countries: the Canadian example: Difficulties with telephone-based surveys on alcohol consumption. Int. J. Meth. Psychiatr. Res. 2012, 21, 17–28. [Google Scholar] [CrossRef]
- Zhao, J.; Stockwell, T.; Macdonald, S. Non-response bias in alcohol and drug population surveys. Drug Alcohol Rev. 2009, 28, 648–657. [Google Scholar] [CrossRef]
- Midanik, L. The Validity of Self-Reported Alcohol Consumption and Alcohol Problems: A Literature Review. Br. J. Addict. 1982, 77, 357–382. [Google Scholar] [CrossRef] [PubMed]
- Probst, C.; Shuper, P.A.; Rehm, J. Coverage of alcohol consumption by national surveys in South Africa: Coverage of alcohol use in South Africa. Addiction 2017, 112, 705–710. [Google Scholar] [CrossRef] [PubMed]
- Storvoll, E.E.; Halkjelsvik, T. Changes in Norwegian public opinion on alcohol policy, 2005–2012. Nordic Stud. Alcohol Drugs 2013, 30, 491–509. [Google Scholar] [CrossRef]
- Holmila, M.; Mustonen, H.; Österberg, E.; Raitasalo, K. Public opinion and community-based prevention of alcohol-related harms. Add. Res. Theor. 2009, 17, 360–371. [Google Scholar] [CrossRef]
- Ramstedt, M. Change and stability? Trends in alcohol consumption, harms and poicy: Sweden 1990–2010. Nordic Stud. Alcohol Drugs 2010, 27, 409–423. [Google Scholar] [CrossRef]
- Rossow, I. Challenges in an affluent society. Trends in alcohol consumption, harms and policy: Norway 1990–2010. Nordic Stud. Alcohol Drugs 2010, 27, 449–464. [Google Scholar] [CrossRef]
- Karlsson, T.; Mäkelä, P.; Österberg, E. A new alcohol environment. Trends in alcohol consumption, harms and policy: Finland 1990–2010. Nordic Stud Alcohol Drugs 2010, 37, 497–513. [Google Scholar] [CrossRef]
- Moskalewicz, J.; Österberg, E. Changes in Alcohol Affordability and Availability. Twenty Years of Transitions in Eastern Europe; National Institute for Health and Welfare: Helsinki, Finland, 2016. [Google Scholar]
- Sierosławski, J. Spożycie alkoholu i polityka wobec alkoholu w ocenie społecznej. In Raport z Badań Ankietowych; Instytut Psychiatrii i Neurologii: Warszawa, Poland, 1992. (In Polish) [Google Scholar]
- Moskalewicz, J.; Simpura, J. Alcohohol and alcohol policy in eastern European transitions. J. Subst. Use 2000, 5, 30–38. [Google Scholar] [CrossRef]
- Štelemėkas, M.; Galkus, L.; Gumarov, V.L.; Midttun, N.G.; Miščikienė, L. Holding policy makers to account: Monitoring voting patterns on alcohol and tobacco policy in the Lithuanian Parliament. Drug Alcohol Rev. (in press).
- Rehm, J.; Manthey, J.; Lange, S.; Badaras, R.; Zurlyte, I.; Passmore, J.; Breda, J.; Ferreira-Borges, C.; Štelemėkas, M. Alcohol control policy and changes in alcohol-related traffic harm. Addiction. (in press). [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Population-Based Alcohol Control Policies | Education and Individual-Based Alcohol Policies | Laissez-Faire Alcohol Policies |
|---|---|---|
| Public authorities have the responsibility to protect people from being harmed by their own drinking | Alcohol education and information should be the most important policy to reduce alcohol-related harm | Alcohol is a commodity as any other and does not require any special restrictions |
| The number of places selling alcohol should be kept low in order to reduce alcohol-related harm | Police should be allowed to check randomly if a driver is sober or not even without any indication of drunken driving | Adult people are responsible enough to protect themselves from harm caused by their drinking |
| Prices of alcoholic beverages should be kept high in order to reduce alcohol-related harm | Printed warnings about alcohol-related harm should be displayed on alcoholic beverages | Parents, and no legal authorities, should decide at what age their child is allowed to drink alcoholic beverages |
| Advertising of alcoholic beverages should be banned | ||
| There should be limits on how late in the evening you can buy alcohol |
| Location | Sample Size a | Response Rate (%) | Gender (% women) | Mean Age (SD) | Educational Achievement b (%) | National Alcohol Policy Score (ranking) c | |
|---|---|---|---|---|---|---|---|
| Secondary Education | High Education | ||||||
| Austria | 3406 | 32.1 | 50.1 | 41.28 (0.23) | 70.8 | 15.4 | liberal |
| Bulgaria | 3000 | 75.0 | 50.7 | 41.53 (0.24) | 58.3 | 29.9 | liberal |
| Croatia | 1500 | 50.6 | 50.1 | 41.52 (0.36) | 40.9 | 17.7 | medium |
| Denmark | 1575 | 52.5 | 51.9 | 40.93 (0.28) | 48.7 | 37.5 | medium |
| Estonia | 2153 | 60.4 | 49.4 | 42.11 (0.38) | 63.8 | 29.4 | medium |
| Finland | 1500 | 11.5 | 51.0 | 41.81 (0.36) | 58.7 | 29.9 | strict |
| France | 1701 | 44.5 | 53.5 | 43.53 (0.35) | 59.3 | 30.2 | medium |
| Greece | 1519 | 27.0 | 50.2 | 41.73 (0.34) | 51.1 | 34.8 | liberal |
| Hungary | 2005 | 43.0 | 50.2 | 41.68 (0.33) | 42.1 | 9.5 | liberal |
| Iceland | 873 | 47.7 | 49.4 | 40.23 (0.52) | 38.4 | 45.5 | strict |
| Italy | 1468 | 8.7 | 50.3 | 42.52 (0.35) | 55.8 | 17.7 | liberal |
| Lithuania | 1513 | 35.0 | 51.7 | 41.17 (0.36) | 67.9 | 24.8 | medium |
| Norway | 1493 | 12.0 | 48.7 | 40.62 (0.34) | 45.7 | 48.3 | strict |
| Poland | 1555 | 63.6 | 50.2 | 41.32 (0.34) | 40.3 | 19.3 | medium |
| Portugal | 1500 | 61.0 | 51.4 | 41.51 (0.35) | 30.4 | 17.8 | liberal |
| Romania | 1500 | 31.0 | 50.0 | 41.11 (0.34) | 56.9 | 27.1 | medium |
| Spain | 1645 | 50.3 | 49.8 | 40.90 (0.31) | 66.8 | 12.2 | liberal |
| Spain—Catalonia d | 661 | 51.1 | 49.6 | 41.70 (0.48) | 72.3 | 12.6 | liberal |
| Sweden | 1623 | 35.9 | 50.9 | 40.76 (0.35) | 56.9 | 34.8 | strict |
| UK | 1045 | 15.0 | 51.1 | 42.33 (0.58) | 48.9 | 41.8 | medium |
| Variable. | Class 1 | Class 2 | Class 3 | ||||
|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | ||
| Gender (ref. male) | |||||||
| Female | 1.47 ‡ | [1.41; 1.52] | 0.60 ‡ | [0.58; 0.63] | 1.26 ‡ | [1.22; 1.32] | |
| Age (ref. ≤34 years) | |||||||
| 35–49 years | 1.07 † | [1.03; 1.12] | 0.88 ‡ | [0.84; 0.93] | 1.09 ‡ | [1.04; 1.15] | |
| ≥50 years | 1.04 | [0.99; 1.09] | 0.83 ‡ | [0.78; 0.87] | 1.25 ‡ | [1.19; 1.31] | |
| Educational achievement (ref. primary and lower secondary education) | |||||||
| Secondary education | 1.07 * | [1.01; 1.13] | 1.18 ‡ | [1.11; 1.26] | 0.77 ‡ | [0.73; 0.81] | |
| High education | 1.45 ‡ | [1.36; 1.54] | 1.12 † | [1.04; 1.20] | 0.53 ‡ | [0.50; 0.57] | |
| Drinking status (ref. abstainer) | |||||||
| Low-risk drinking | 0.74 ‡ | [0.70; 0.78] | 2.25 ‡ | [2.11; 2.41] | 0.55 ‡ | [0.53; 0.58] | |
| High-risk drinking | 0.62 ‡ | [0.55; 0.70] | 2.33 ‡ | [2.04; 2.67] | 0.65 ‡ | [0.58; 0.73] | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kilian, C.; Manthey, J.; Moskalewicz, J.; Sieroslawski, J.; Rehm, J. How Attitudes toward Alcohol Policies Differ across European Countries: Evidence from the Standardized European Alcohol Survey (SEAS). Int. J. Environ. Res. Public Health 2019, 16, 4461. https://doi.org/10.3390/ijerph16224461
Kilian C, Manthey J, Moskalewicz J, Sieroslawski J, Rehm J. How Attitudes toward Alcohol Policies Differ across European Countries: Evidence from the Standardized European Alcohol Survey (SEAS). International Journal of Environmental Research and Public Health. 2019; 16(22):4461. https://doi.org/10.3390/ijerph16224461
Chicago/Turabian StyleKilian, Carolin, Jakob Manthey, Jacek Moskalewicz, Janusz Sieroslawski, and Jürgen Rehm. 2019. "How Attitudes toward Alcohol Policies Differ across European Countries: Evidence from the Standardized European Alcohol Survey (SEAS)" International Journal of Environmental Research and Public Health 16, no. 22: 4461. https://doi.org/10.3390/ijerph16224461
APA StyleKilian, C., Manthey, J., Moskalewicz, J., Sieroslawski, J., & Rehm, J. (2019). How Attitudes toward Alcohol Policies Differ across European Countries: Evidence from the Standardized European Alcohol Survey (SEAS). International Journal of Environmental Research and Public Health, 16(22), 4461. https://doi.org/10.3390/ijerph16224461