Decreased Vertical Trunk Inclination Angle and Pelvic Inclination as the Result of Mid-High-Heeled Footwear on Static Posture Parameters in Asymptomatic Young Adult Women

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Design
2.2. Subjects
2.3. Data Acquisition
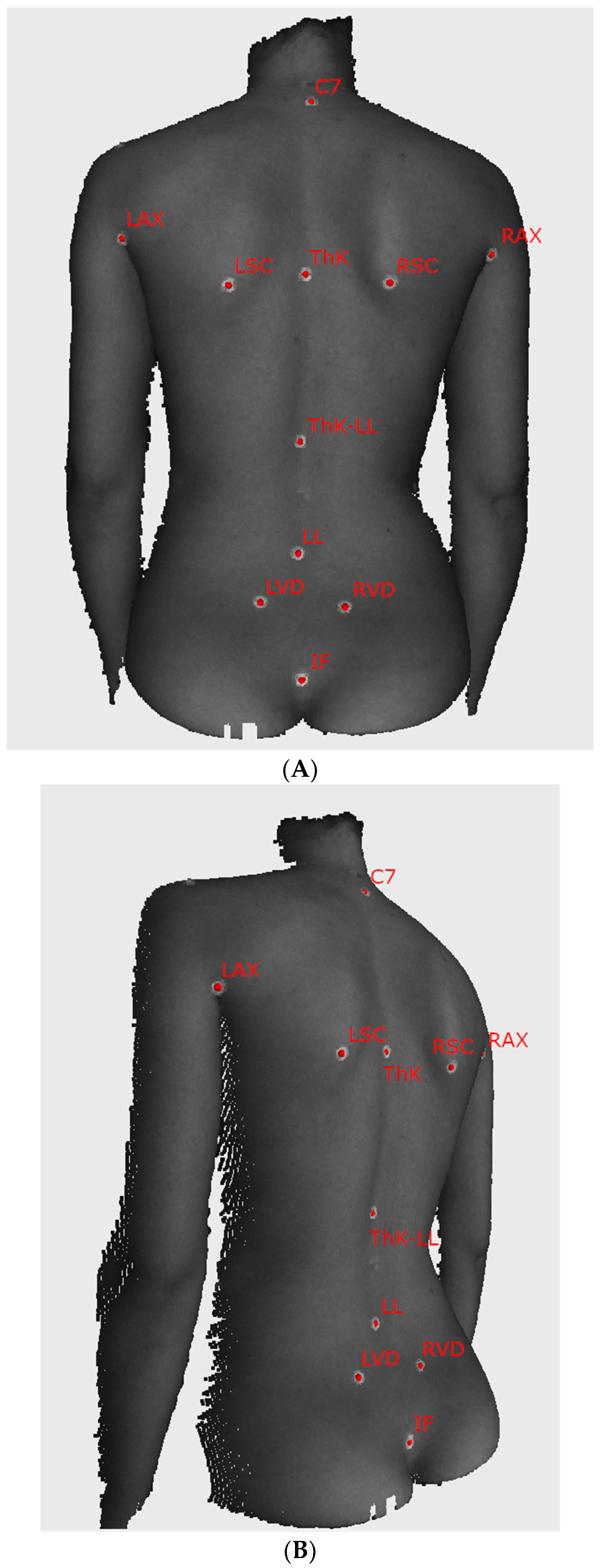
2.4. Application of Fiducial Markers
- -
- C7—the spinous process of the vertebra prominens,
- -
- LAX/RAX—left and right axilla,
- -
- LSC/RSC—the inferior angle of the left and right scapula,
- -
- ThK—the apex of thoracic kyphosis,
- -
- ThK-LL—point of transition from thoracic kyphosis to lumbar lordosis,
- -
- LL—the apex of lumbar lordosis,
- -
- LVD/RVD—left and right Venus dimple,
- -
- IF—top of the intergluteal cleft.
2.5. Barefoot Measurements
2.6. High-Heeled Measurements
2.7. Data Analysis
- filtering measurement noise using FRAMES built-in algorithms,
- using a custom algorithm for automatic detection of the circular markers on the surface of the skin developed for this experiment, and
- methods for estimating parameters connected with posture.
2.8. Postural Parameters Extraction
- -
- vertical balance angle (vertical trunk inclination in the sagittal plane)(VBA), which is the angle between the vertical axis and the line connecting C7 and IF, the positive value corresponds to the subject leaning forward,
- -
- thoracic kyphosis angle (TKA), which is the angle between normal vectors of planes fitted in the area around points C7 and ThK-LL, with an additional offset to C7 equal to 5 mm in the direction of ThK-LL,
- -
- lumbar lordosis angle (LLA), which is the angle between normal vectors of planes fitted in the area around points IF and ThK-LL, with an additional offset to IF equal to 15 mm in the direction of ThK-LL,
- -
- pelvic inclination angle (PIA), which is the angle between the normal vector of the plane fitted to the area between LVD and RVD and the horizontal axis.
- -
2.9. Influence of Marker Placement Accuracy
- for each subject, for each landmark, draw a random displacement vector from the N(0, 10) distribution, each vector component was drawn independently,
- after applying the displacement vector to each landmark, the point was projected to the cloud to find a real point on the surface.
2.10. Statistical Analysis
3. Results
4. Discussion
4.1. The Biomechanical Aspect of Results/Observations
4.2. Influence of Precision of Fiducial Marker Placement
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Lewis, D.M.G.; Russell, E.M.; Al-Shawaf, L.; Ta, V.; Senveli, Z.; Ickes, W.; Buss, D.M. Why Women Wear High Heels: Evolution, Lumbar Curvature, and Attractiveness. Front. Psychol. 2017, 8, 1875. [Google Scholar] [CrossRef] [PubMed]
- Guéguen, N.; Stefan, J.; Renault, Q. Judgments toward women wearing high heels: A forced-choice evaluation. Fash. Text. 2016, 3, 173. [Google Scholar] [CrossRef]
- Frey, C.; Thompson, F.; Smith, J.; Sanders, M.; Horstman, H. American Orthopaedic Foot and Ankle Society women’s shoe survey. Foot Ankle 1993, 14, 78–81. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, J.; Hollander, K. Effects of high-heeled footwear on static and dynamic pelvis position and lumbar lordosis in experienced younger and middle-aged women. Gait Posture 2018, 59, 53–57. [Google Scholar] [CrossRef]
- Di Sipio, E.; Piccinini, G.; Pecchioli, C.; Germanotta, M.; Iacovelli, C.; Simbolotti, C.; Cruciani, A.; Padua, L. Walking variations in healthy women wearing high-heeled shoes: Shoe size and heel height effects. Gait Posture 2018, 63, 195–201. [Google Scholar] [CrossRef]
- Baaklini, E.; Angst, M.; Schellenberg, F.; Hitz, M.; Schmid, S.; Tal, A.; Taylor, W.R.; Lorenzetti, S. High-heeled walking decreases lumbar lordosis. Gait Posture 2017, 55, 12–14. [Google Scholar] [CrossRef]
- Barnish, M.S.; Barnish, J. High-heeled shoes and musculoskeletal injuries: A narrative systematic review. BMJ Open 2016, 6, e010053. [Google Scholar] [CrossRef]
- Weitkunat, T.; Buck, F.M.; Jentzsch, T.; Simmen, H.P.; Werner, C.M.; Osterhoff, G. Influence of high-heeled shoes on the sagittal balance of the spine and the whole body. Eur. Spine J. 2016, 25, 3658–3665. [Google Scholar] [CrossRef]
- Dai, M.; Li, X.; Zhou, X.; Hu, Y.; Luo, Q.; Zhou, S. High-heeled-related alterations in the static sagittal profile of the spino-pelvic structure in young women. Eur. Spine J. 2015, 24, 1274–1281. [Google Scholar] [CrossRef]
- Silva, A.M.; de Siqueira, G.R.; da Silva, G.A. Implications of high-heeled shoes on body posture of adolescents. Rev. Paul. Pediatr. 2013, 31, 265–271. [Google Scholar] [CrossRef]
- Drzal-Grabiec, J.; Snela, S. Effect of high-heeled shoes on the parameters of body posture. Spine (Phila Pa 1976) 2013, 38, 1785–1789. [Google Scholar] [CrossRef] [PubMed]
- Russell, B.S.; Muhlenkamp, K.A.; Hoiriis, K.T.; Desimone, C.M. Measurement of lumbar lordosis in static standing posture with and without high-heeled shoes. J. Chiropr. Med. 2012, 11, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Wan, F.K.W.; Yick, K.L.; Yu, W.W.M. Effects of heel height and high-heel experience on foot stability during quiet standing. Gait Posture 2019, 68, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Franklin, M.E.; Chenier, T.C.; Brauninger, L.; Cook, H.; Harris, S. Effect of positive heel inclination on posture. J. Orthop. Sports Phys. Ther. 1995, 21, 94–99. [Google Scholar] [CrossRef]
- de Oliveira Pezzan, P.A.; Joao, S.M.; Ribeiro, A.P.; Manfio, E.F. Postural assessment of lumbar lordosis and pelvic alignment angles in adolescent users and nonusers of high-heeled shoes. J. Manip. Physiol. Ther. 2011, 34, 614–621. [Google Scholar] [CrossRef]
- Simonsen, E.B. Contributions to the understanding of gait control. Dan. Med. J. 2014, 61, B4823. [Google Scholar]
- Moore, J.X.; Lambert, B.; Jenkins, G.P.; McGwin, G., Jr. Epidemiology of High-Heel Shoe Injuries in U.S. Women: 2002 to 2012. J. Foot Ankle Surg. 2015, 54, 615–619. [Google Scholar] [CrossRef]
- Lee, C.M.; Jeong, E.H.; Freivalds, A. Biomechanical effects of wearing high-heeled shoes. Int. J. Ind. Ergon. 2001, 28, 321–326. [Google Scholar] [CrossRef]
- Bendix, T.; Sorensen, S.S.; Klausen, K. Lumbar curve, trunk muscles, and line of gravity with different heel heights. Spine (Phila Pa 1976) 1984, 9, 223–227. [Google Scholar] [CrossRef]
- Opila, K.A.; Wagner, S.S.; Schiowitz, S.; Chen, J. Postural alignment in barefoot and high-heeled stance. Spine (Phila Pa 1976) 1988, 13, 542–547. [Google Scholar] [CrossRef]
- Russell, B.S. The effect of high-heeled shoes on lumbar lordosis: A narrative review and discussion of the disconnect between Internet content and peer-reviewed literature. J. Chiropr. Med. 2010, 9, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Opila-Correia, K.A. Kinematics of high-heeled gait with consideration for age and experience of wearers. Arch. Phys. Med. Rehabil. 1990, 71, 905–909. [Google Scholar] [PubMed]
- Cowley, E.E.; Chevalier, T.L.; Chockalingam, N. The effect of heel height on gait and posture: A review of the literature. J. Am. Podiatr. Med. Assoc. 2009, 99, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.H.; Childress, D.S. Effects of shoe heel height on biologic rollover characteristics during walking. J. Rehabil. Res. Dev. 2004, 41, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Frerich, J.M.; Hertzler, K.; Knott, P.; Mardjetko, S. Comparison of radiographic and surface topography measurements in adolescents with idiopathic scoliosis. Open Orthop. J. 2012, 6, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Pino-Almero, L.; Minguez-Rey, M.F.; Cibrian-Ortiz de Anda, R.M.; Salvador-Palmer, M.R.; Sentamans-Segarra, S. Correlation between Topographic Parameters Obtained by Back Surface Topography Based on Structured Light and Radiographic Variables in the Assessment of Back Morphology in Young Patients with Idiopathic Scoliosis. Asian Spine J. 2017, 11, 219–229. [Google Scholar] [CrossRef]
- Pino-Almero, L.; Minguez-Rey, M.F.; Sentamans-Segarra, S.; Salvador-Palmer, M.R.; Anda, R.M.; La, O.J. Quantification of topographic changes in the surface of back of young patients monitored for idiopathic scoliosis: Correlation with radiographic variables. J. Biomed. Opt. 2016, 21, 116001. [Google Scholar] [CrossRef]
- Larson, A.N.; Schueler, B.A.; Dubousset, J. Radiation in Spine Deformity: State-of-the-Art Reviews. Spine Deform. 2019, 7, 386–394. [Google Scholar] [CrossRef]
- Law, M.; Ma, W.K.; Lau, D.; Cheung, K.; Ip, J.; Yip, L.; Lam, W. Cumulative effective dose and cancer risk for pediatric population in repetitive full spine follow-up imaging: How micro dose is the EOS microdose protocol? Eur. J. Radiol. 2018, 101, 87–91. [Google Scholar] [CrossRef]
- Knott, P.; Sturm, P.; Lonner, B.; Cahill, P.; Betsch, M.; McCarthy, R.; Kelly, M.; Lenke, L.; Betz, R. Multicenter Comparison of 3D Spinal Measurements Using Surface Topography With Those From Conventional Radiography. Spine Deform. 2016, 4, 98–103. [Google Scholar] [CrossRef]
- Simony, A.; Hansen, E.J.; Christensen, S.B.; Carreon, L.Y.; Andersen, M.O. Incidence of cancer in adolescent idiopathic scoliosis patients treated 25 years previously. Eur. Spine J. 2016, 25, 3366–3370. [Google Scholar] [CrossRef]
- Ronckers, C.M.; Land, C.E.; Miller, J.S.; Stovall, M.; Lonstein, J.E.; Doody, M.M. Cancer mortality among women frequently exposed to radiographic examinations for spinal disorders. Radiat. Res. 2010, 174, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Ronckers, C.M.; Doody, M.M.; Lonstein, J.E.; Stovall, M.; Land, C.E. Multiple diagnostic X-rays for spine deformities and risk of breast cancer. Cancer Epidemiol. Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cospons. Am. Soc. Prev. Oncol. 2008, 17, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Doody, M.M.; Lonstein, J.E.; Stovall, M.; Hacker, D.G.; Luckyanov, N.; Land, C.E. Breast cancer mortality after diagnostic radiography: Findings from the U.S. Scoliosis Cohort Study. Spine (Phila Pa 1976) 2000, 25, 2052–2063. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, D.A.; Lonstein, J.E.; Morin, M.M.; Visscher, W.; Harris, B.S., 3rd; Boice, J.D., Jr. Breast cancer in women with scoliosis exposed to multiple diagnostic x rays. J. Natl. Cancer Inst. 1989, 81, 1307–1312. [Google Scholar] [CrossRef] [PubMed]
- Minehiro, K.; Demura, S.; Ichikawa, K.; Sasagawa, T.; Takahashi, N.; Minami, S.; Murakami, H.; Tsuchiya, H. Dose Reduction Protocol for Full Spine X-ray Examination Using Copper Filters in Patients With Adolescent Idiopathic Scoliosis. Spine (Phila Pa 1976) 2019, 44, 203–210. [Google Scholar] [CrossRef]
- Law, M.; Ma, W.K.; Chan, E.; Lau, D.; Mui, C.; Cheung, K.; Yip, L.; Lam, W. Evaluation of cumulative effective dose and cancer risk from repetitive full spine imaging using EOS system: Impact to adolescent patients of different populations. Eur. J. Radiol. 2017, 96, 1–5. [Google Scholar] [CrossRef]
- Melhem, E.; Assi, A.; El Rachkidi, R.; Ghanem, I. EOS((R)) biplanar X-ray imaging: Concept, developments, benefits, and limitations. J. Child. Orthop. 2016, 10, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Newton, P.O.; Khandwala, Y.; Bartley, C.E.; Reighard, F.G.; Bastrom, T.P.; Yaszay, B. New EOS Imaging Protocol Allows a Substantial Reduction in Radiation Exposure for Scoliosis Patients. Spine Deform. 2016, 4, 138–144. [Google Scholar] [CrossRef]
- Ilharreborde, B.; Ferrero, E.; Alison, M.; Mazda, K. EOS microdose protocol for the radiological follow-up of adolescent idiopathic scoliosis. Eur. Spine J. 2016, 25, 526–531. [Google Scholar] [CrossRef]
- Levy, A.R.; Goldberg, M.S.; Hanley, J.A.; Mayo, N.E.; Poitras, B. Projecting the lifetime risk of cancer from exposure to diagnostic ionizing radiation for adolescent idiopathic scoliosis. Health Phys. 1994, 66, 621–633. [Google Scholar] [CrossRef] [PubMed]
- Glinkowski, W.; Michonski, J.; Glinkowska, B.; Zukowska, A.; Sitnik, R.; Gorecki, A. Telediagnostic 3D school screening of back curvatures and posture using structured light method-pilot study. Stud. Health Technol. Inform. 2012, 176, 291–294. [Google Scholar] [PubMed]
- Glinkowski, W.; Sitnik, R.; Witkowski, M.; Kocon, H.; Bolewicki, P.; Gorecki, A. Method of pectus excavatum measurement based on structured light technique. J. Biomed. Opt. 2009, 14, 044041. [Google Scholar] [CrossRef] [PubMed]
- Hill, D.L.; Berg, D.C.; Raso, V.J.; Lou, E.; Durdle, N.G.; Mahood, J.K.; Moreau, M.J. Evaluation of a laser scanner for surface topography. Stud. Health Technol. Inform. 2002, 88, 90–94. [Google Scholar] [PubMed]
- Bassani, T.; Stucovitz, E.; Galbusera, F.; Brayda-Bruno, M. Is rasterstereography a valid noninvasive method for the screening of juvenile and adolescent idiopathic scoliosis? Eur. Spine J. 2019, 28, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Tabard-Fougere, A.; Bonnefoy-Mazure, A.; Dhouib, A.; Valaikaite, R.; Armand, S.; Dayer, R. Radiation-free measurement tools to evaluate sagittal parameters in AIS patients: A reliability and validity study. Eur. Spine J. 2019, 28, 536–543. [Google Scholar] [CrossRef]
- Degenhardt, B.; Starks, Z.; Bhatia, S.; Franklin, G.A. Appraisal of the DIERS method for calculating postural measurements: An observational study. Scoliosis Spinal Disord. 2017, 12, 28. [Google Scholar] [CrossRef] [Green Version]
- Mohokum, M.; Schulein, S.; Skwara, A. The Validity of Rasterstereography: A Systematic Review. Orthop. Rev. (Pavia) 2015, 7, 5899. [Google Scholar] [CrossRef] [Green Version]
- Drerup, B. Rasterstereographic measurement of scoliotic deformity. Scoliosis 2014, 9, 22. [Google Scholar] [CrossRef] [Green Version]
- Furian, T.C.; Rapp, W.; Eckert, S.; Wild, M.; Betsch, M. Spinal posture and pelvic position in three hundred forty-five elementary school children: A rasterstereographic pilot study. Orthop. Rev. (Pavia) 2013, 5, e7. [Google Scholar] [CrossRef] [Green Version]
- Drerup, B.; Hierholzer, E. Back shape measurement using video rasterstereography and three-dimensional reconstruction of spinal shape. Clin. Biomech. 1994, 9, 28–36. [Google Scholar] [CrossRef]
- Drerup, B.; Hierholzer, E. Objective determination of anatomical landmarks on the body surface: Measurement of the vertebra prominens from surface curvature. J. Biomech. 1985, 18, 467–474. [Google Scholar] [CrossRef]
- Liu, X.C.; Tassone, J.C.; Thometz, J.G.; Paulsen, L.C.; Lyon, R.M.; Marquez-Barrientos, C.; Tarima, S.; Johnson, P.R. Development of a 3-Dimensional Back Contour Imaging System for Monitoring Scoliosis Progression in Children. Spine Deform. 2013, 1, 102–107. [Google Scholar] [CrossRef] [PubMed]
- McKenna, C.; Wade, R.; Faria, R.; Yang, H.; Stirk, L.; Gummerson, N.; Sculpher, M.; Woolacott, N. EOS 2D/3D X-ray imaging system: A systematic review and economic evaluation. Health Technol. Assess. 2012, 16, 1–188. [Google Scholar] [CrossRef] [Green Version]
- Knott, P.; Mardjetko, S.; Tager, D.; Hund, R.; Thompson, S. The influence of body mass index (BMI) on the reproducibility of surface topography measurements. Scoliosis 2012, 7, O18. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, J.; Schaar, H.; Mattes, K. Spinal alignment in low back pain patients and age-related side effects: A multivariate cross-sectional analysis of video rasterstereography back shape reconstruction data. Eur. Spine J. 2013, 22, 1979–1985. [Google Scholar] [CrossRef] [Green Version]
- Michonski, J.; Glinkowski, W.; Witkowski, M.; Sitnik, R. Automatic recognition of surface landmarks of anatomical structures of back and posture. J. Biomed. Opt. 2012, 17, 056015. [Google Scholar] [CrossRef] [Green Version]
- Sitnik, R. New Method of Structure Light Measurement System Calibration Based on Adaptive and Effective Evaluation of 3D-Phase Distribution; SPIE: Bellingham, WA, USA, 2005; Volume 5856. [Google Scholar]
- Research, E. Public Opinion Research on Foot Health and Care, Findings from a Survey of 1000 US Adults; American Podiatric Medical Association: Bethesda, MD, USA, 2014; p. 30. [Google Scholar]
- Patias, P.; Grivas, T.B.; Kaspiris, A.; Aggouris, C.; Drakoutos, E. A review of the trunk surface metrics used as Scoliosis and other deformities evaluation indices. Scoliosis 2010, 5, 12. [Google Scholar] [CrossRef] [Green Version]
- Wolanski, N. Typology and Formation of Body Posture in Town and Rural Children and Youth. Acta Anat. (Basel) 1964, 56, 157–183. [Google Scholar] [CrossRef]
- Pearsall, D.J.; Reid, J.G.; Hedden, D.M. Comparison of three noninvasive methods for measuring scoliosis. Phys. Ther. 1992, 72, 648–657. [Google Scholar] [CrossRef]
- Liberadzki, P.; Markiewicz, Ł.; Witkowski, M.; Sitnik, R. Novel 4D Whole Body Scanning Solution and its Medical Application. In Proceedings of the 9th International Conference and Exhibition on 3D Body Scanning and Processing Technologies, Lugano, Switzerland, 16–17 October 2018; pp. 47–56. [Google Scholar]
- Parent, E.C.; Damaraju, S.; Hill, D.L.; Lou, E.; Smetaniuk, D. Identifying the best surface topography parameters for detecting idiopathic scoliosis curve progression. Stud. Health Technol. Inform. 2010, 158, 78–82. [Google Scholar] [PubMed]
- Asher, M.; Lai, S.M.; Burton, D.; Manna, B. Spine deformity correlates better than trunk deformity with idiopathic scoliosis patients’ quality of life questionnaire responses. Stud. Health Technol. Inform. 2002, 91, 462–464. [Google Scholar] [PubMed]
- Ono, T. Trunk deformity in scoliosis studied by surface measurement. Nihon Seikeigeka Gakkai Zasshi 1995, 69, 915–926. [Google Scholar] [PubMed]
- Pino-Almero, L.; Minguez-Rey, M.F.; Rodriguez-Martinez, D.; Cibrian-Ortiz de Anda, R.M.; Salvador-Palmer, M.R.; Sentamans-Segarra, S. Clinical application of back surface topography by means of structured light in the screening of idiopathic scoliosis. J. Pediatr. Orthop. B 2017, 26, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Matlega, A.; Stepowska, J.; Wisniewski, A.; Gajewski, J. Assessment of the coronal plane trunk symmetry in children. Physiother. Theory Pract. 2019, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Janusz, P.; Tyrakowski, M.; Kotwicki, T.; Siemionow, K. Cervical Sagittal Alignment in Scheuermann Disease. Spine (Phila Pa 1976) 2015, 40, E1226–E1232. [Google Scholar] [CrossRef] [PubMed]
- Ilharreborde, B.; Sebag, G.; Skalli, W.; Mazda, K. Adolescent idiopathic scoliosis treated with posteromedial translation: Radiologic evaluation with a 3D low-dose system. Eur. Spine J. 2013, 22, 2382–2391. [Google Scholar] [CrossRef] [Green Version]
- Yong, Q.; Zhen, L.; Zezhang, Z.; Bangping, Q.; Feng, Z.; Tao, W.; Jun, J.; Xu, S.; Xusheng, Q.; Weiwei, M.; et al. Comparison of sagittal spinopelvic alignment in Chinese adolescents with and without idiopathic thoracic scoliosis. Spine (Phila Pa 1976) 2012, 37, E714–E720. [Google Scholar] [CrossRef]
- Roussouly, P.; Gollogly, S.; Noseda, O.; Berthonnaud, E.; Dimnet, J. The vertical projection of the sum of the ground reactive forces of a standing patient is not the same as the C7 plumb line: A radiographic study of the sagittal alignment of 153 asymptomatic volunteers. Spine (Phila Pa 1976) 2006, 31, E320–E325. [Google Scholar] [CrossRef]
- Aota, Y.; Saito, T.; Uesugi, M.; Kato, S.; Kuniya, H.; Koh, R. Optimal arm position for evaluation of spinal sagittal balance. J. Spinal Disord. Tech. 2011, 24, 105–109. [Google Scholar] [CrossRef]
- Glinkowski, W.M.; Czyżak, I.; Glinkowska, B.; Zukowska, A.; Michoński, J. The position with fingers on clavicles has no influence on vertical trunk inclination and kyphosis but significantly changes surface topography lordosis angle. Scoliosis 2013, 8. [Google Scholar] [CrossRef] [Green Version]
- Knott, P.T.; Mardjetko, S.M.; Techy, F. The use of the T1 sagittal angle in predicting overall sagittal balance of the spine. Spine J. Off. J. N. Am.n Spine Soc. 2010, 10, 994–998. [Google Scholar] [CrossRef] [PubMed]
- Marks, M.; Stanford, C.; Newton, P. Which lateral radiographic positioning technique provides the most reliable and functional representation of a patient’s sagittal balance? Spine (Phila Pa 1976) 2009, 34, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Tabard-Fougere, A.; Bonnefoy-Mazure, A.; Hanquinet, S.; Lascombes, P.; Armand, S.; Dayer, R. Validity and Reliability of Spine Rasterstereography in Patients With Adolescent Idiopathic Scoliosis. Spine (Phila Pa 1976) 2017, 42, 98–105. [Google Scholar] [CrossRef]
- Guidetti, L.; Bonavolonta, V.; Tito, A.; Reis, V.M.; Gallotta, M.C.; Baldari, C. Intra- and interday reliability of spine rasterstereography. BioMed Res. Int. 2013, 2013. [Google Scholar] [CrossRef]
- Schulein, S.; Mendoza, S.; Malzkorn, R.; Harms, J.; Skwara, A. Rasterstereographic evaluation of interobserver and intraobserver reliability in postsurgical adolescent idiopathic scoliosis patients. J. Spinal Disord. Tech. 2013, 26, E143–E149. [Google Scholar] [CrossRef]
- Mohokum, M.; Mendoza, S.; Udo, W.; Sitter, H.; Paletta, J.R.; Skwara, A. Reproducibility of rasterstereography for kyphotic and lordotic angles, trunk length, and trunk inclination: A reliability study. Spine (Phila Pa 1976) 2010, 35, 1353–1358. [Google Scholar] [CrossRef] [Green Version]
- Glinkowski, W.M.; Kabacyj, M.; Śliwka, A.; Wiącek, P.; Twardowska, K.; Sitnik, R. Reproducibility of Structural Light Assessment 3D Posturę Telediagnostics: Preliminary Reliability Study. Glob. Telemed. eHealth Updat. Knowl. Resour. 2011, 4, 154–157. [Google Scholar]
- Navarro, I.; Rosa, B.N.D.; Candotti, C.T. Anatomical reference marks, evaluation parameters and reproducibility of surface topography for evaluating the adolescent idiopathic scoliosis: A systematic review with meta-analysis. Gait Posture 2019, 69, 112–120. [Google Scholar] [CrossRef]
- Manca, A.; Monticone, M.; Cugusi, L.; Doria, C.; Tranquilli-Leali, P.; Deriu, F. Back surface measurements by rasterstereography for adolescent idiopathic scoliosis: From reproducibility to data reduction analyses. Eur. Spine J. 2018, 27, 2130–2138. [Google Scholar] [CrossRef]
- Komeili, A.; Westover, L.; Parent, E.C.; El-Rich, M.; Adeeb, S. Correlation Between a Novel Surface Topography Asymmetry Analysis and Radiographic Data in Scoliosis. Spine Deform. 2015, 3, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Glinkowski, W.; Michonski, J.; Zukowska, A.; Glinkowska, B.; Sitnik, R.; Gorecki, A. The time effectiveness of three-dimensional telediagnostic postural screening of back curvatures and scoliosis. Telemed. J. E-Health Off. J. Am. Telemed. Assoc. 2014, 20, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Chowanska, J.; Kotwicki, T.; Rosadzinski, K.; Sliwinski, Z. School screening for scoliosis: Can surface topography replace examination with scoliometer? Scoliosis 2012, 7, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorton, G.E., 3rd; Young, M.L.; Masso, P.D. Accuracy, reliability, and validity of a 3-dimensional scanner for assessing torso shape in idiopathic scoliosis. Spine (Phila Pa 1976) 2012, 37, 957–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zubovic, A.; Davies, N.; Berryman, F.; Pynsent, P.; Quraishi, N.; Lavy, C.; Bowden, G.; Wilson-Macdonald, J.; Fairbank, J. New method of Scoliosis Deformity Assessment: ISIS2 System. Stud. Health Technol. Inform. 2008, 140, 157–160. [Google Scholar] [CrossRef]
- Schumann, K.; Puschel, I.; Maier-Hennes, A.; Weiss, H.R. Postural changes in patients with scoliosis in different postural positions revealed by surface topography. Stud. Health Technol. Inform. 2008, 140, 140–143. [Google Scholar]
- Kotwicki, T. Evaluation of scoliosis today: Examination, X-rays and beyond. Disabil. Rehabil. 2008, 30, 742–751. [Google Scholar] [CrossRef]
- Macdonald, A.M.; Griffiths, C.J.; MacArdle, F.J.; Gibson, M.J. The effect of posture on Quantec measurements. Stud. Health Technol. Inform. 2002, 91, 190–193. [Google Scholar]
- Goldberg, C.J.; Kaliszer, M.; Moore, D.P.; Fogarty, E.E.; Dowling, F.E. Surface topography, Cobb angles, and cosmetic change in scoliosis. Spine (Phila Pa 1976) 2001, 26, E55–E63. [Google Scholar] [CrossRef]
- Oxborrow, N.J. Assessing the child with scoliosis: The role of surface topography. Arch. Dis. Child. 2000, 83, 453–455. [Google Scholar] [CrossRef] [Green Version]
- Wong, H.K.; Balasubramaniam, P.; Rajan, U.; Chng, S.Y. Direct spinal curvature digitization in scoliosis screening—A comparative study with Moire contourgraphy. J. Spinal Disord. 1997, 10, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Pearson, J.D.; Dangerfield, P.H.; Atkinson, J.T.; Gomm, J.B.; Dorgan, J.C.; Hobson, C.A.; Harvey, D.M. Measurement of body surface topography using an automated imaging system. Acta Orthop. Belg. 1992, 58 (Suppl. 1), 73–79. [Google Scholar]
- Stokes, I.A.; Moreland, M.S. Concordance of back surface asymmetry and spine shape in idiopathic scoliosis. Spine (Phila Pa 1976) 1989, 14, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Michonski, J.; Walesiak, K.; Pakula, A.; Glinkowski, W.; Sitnik, R. Monitoring of spine curvatures and posture during pregnancy using surface topography-case study and suggestion of method. Scoliosis Spinal Disord. 2016, 11, 31. [Google Scholar] [CrossRef] [PubMed]
- Weiss, H.R.; Elobeidi, N. Comparison of the kyphosis angle evaluated by video rasterstereography (VRS) with x-ray measurements. Stud. Health Technol. Inform. 2008, 140, 137–139. [Google Scholar] [PubMed]
- Berryman, F.; Pynsent, P.; Fairbank, J. Thoracic kyphosis angle measurements with ISIS2. Stud. Health Technol. Inform. 2008, 140, 68–71. [Google Scholar]
- McArdle, F.J.; Griffiths, C.J.; Macdonald, A.M.; Gibson, M.J. Monitoring the thoracic sagittal curvature in kyphoscoliosis with surface topography: A trend analysis of 57 patients. Stud. Health Technol. Inform. 2002, 91, 199–203. [Google Scholar]
- Grant, C.A.; Johnston, M.; Adam, C.J.; Little, J.P. Accuracy of 3D surface scanners for clinical torso and spinal deformity assessment. Med. Eng. Phys. 2019, 63, 63–71. [Google Scholar] [CrossRef]
- Ghaneei, M.; Komeili, A.; Li, Y.; Parent, E.C.; Adeeb, S. 3D Markerless asymmetry analysis in the management of adolescent idiopathic scoliosis. BMC Musculoskelet. Disord. 2018, 19, 385. [Google Scholar] [CrossRef]
- Cohen, L.; Kobayashi, S.; Simic, M.; Dennis, S.; Refshauge, K.; Pappas, E. Non-radiographic methods of measuring global sagittal balance: A systematic review. Scoliosis Spinal Disord. 2017, 12, 30. [Google Scholar] [CrossRef] [Green Version]
- Snow, R.E.; Williams, K.R. High heeled shoes: Their effect on center of mass position, posture, three-dimensional kinematics, rearfoot motion, and ground reaction forces. Arch. Phys. Med. Rehabil. 1994, 75, 568–576. [Google Scholar] [PubMed]
- Hyun, S.H.; Ryew, C.C. Effect of lower limb kinetic on carrying infant by hip seat carrier during high heel gait. J. Exerc. Rehabil. 2018, 14, 1092–1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, D. Muscle activation of paraspinal muscles in different types of high heels during standing. J. Phys. Ther. Sci. 2015, 27, 67–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Studer, D. Clinical investigation and imaging. J. Child. Orthop. 2013, 7, 29–35. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Distribution | Minimum [°] | Lower-Hinge [°] | Median [°] | Upper-Hinge [°] | Maximum [°] |
|---|---|---|---|---|---|---|
| Thoracic kyphosis angle | Barefoot | 11.5 | 24.8 | 32.5 | 35.5 | 47.0 |
| High Heels | 12.9 | 25.3 | 31.1 | 36.8 | 47.7 | |
| Lumbar lordosis angle | Barefoot | 15.1 | 28.7 | 33.8 | 40.5 | 50.6 |
| High Heels | 14.0 | 26.4 | 32.6 | 39.0 | 50.0 | |
| Pelvic inclination angle | Barefoot | 16.5 | 25.2 | 28.5 | 31.8 | 37.6 |
| High Heels | 15.1 | 23.0 | 26.8 | 31.5 | 36.6 | |
| Vertical balance angle | Barefoot | 0.0 | 2.6 | 3.5 | 5.3 | 10.0 |
| High Heels | −1.1 | 1.2 | 2.4 | 4.0 | 9.7 |
| Parameter | ICC3,3 |
|---|---|
| Thoracic kyphosis angle | 0.94 |
| Lumbar lordosis angle | 0.99 |
| Pelvic inclination angle | 0.96 |
| Vertical balance angle | 0.98 |
| Parameter | Wilcoxon Signed Rank Test (Heels vs. Barefoot, Paired) | Matched Pairs Rank-Biserial Correlation |
|---|---|---|
| Thoracic kyphosis angle | W = 547, p = 0.13 | 0.23 (small) |
| Lumbar lordosis angle | W = 620, p = 0.40 | −0.13 (small) |
| Pelvic inclination angle *** | W = 201, p < 0.001 | −0.72 (medium to large) |
| Vertical balance angle *** | W = 51, p < 0.001 | −0.93 (large) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michoński, J.; Witkowski, M.; Glinkowska, B.; Sitnik, R.; Glinkowski, W. Decreased Vertical Trunk Inclination Angle and Pelvic Inclination as the Result of Mid-High-Heeled Footwear on Static Posture Parameters in Asymptomatic Young Adult Women. Int. J. Environ. Res. Public Health 2019, 16, 4556. https://doi.org/10.3390/ijerph16224556
Michoński J, Witkowski M, Glinkowska B, Sitnik R, Glinkowski W. Decreased Vertical Trunk Inclination Angle and Pelvic Inclination as the Result of Mid-High-Heeled Footwear on Static Posture Parameters in Asymptomatic Young Adult Women. International Journal of Environmental Research and Public Health. 2019; 16(22):4556. https://doi.org/10.3390/ijerph16224556
Chicago/Turabian StyleMichoński, Jakub, Marcin Witkowski, Bożena Glinkowska, Robert Sitnik, and Wojciech Glinkowski. 2019. "Decreased Vertical Trunk Inclination Angle and Pelvic Inclination as the Result of Mid-High-Heeled Footwear on Static Posture Parameters in Asymptomatic Young Adult Women" International Journal of Environmental Research and Public Health 16, no. 22: 4556. https://doi.org/10.3390/ijerph16224556
APA StyleMichoński, J., Witkowski, M., Glinkowska, B., Sitnik, R., & Glinkowski, W. (2019). Decreased Vertical Trunk Inclination Angle and Pelvic Inclination as the Result of Mid-High-Heeled Footwear on Static Posture Parameters in Asymptomatic Young Adult Women. International Journal of Environmental Research and Public Health, 16(22), 4556. https://doi.org/10.3390/ijerph16224556