Multimorbidity Development in Working People


Abstract
:1. Introduction
2. Methods
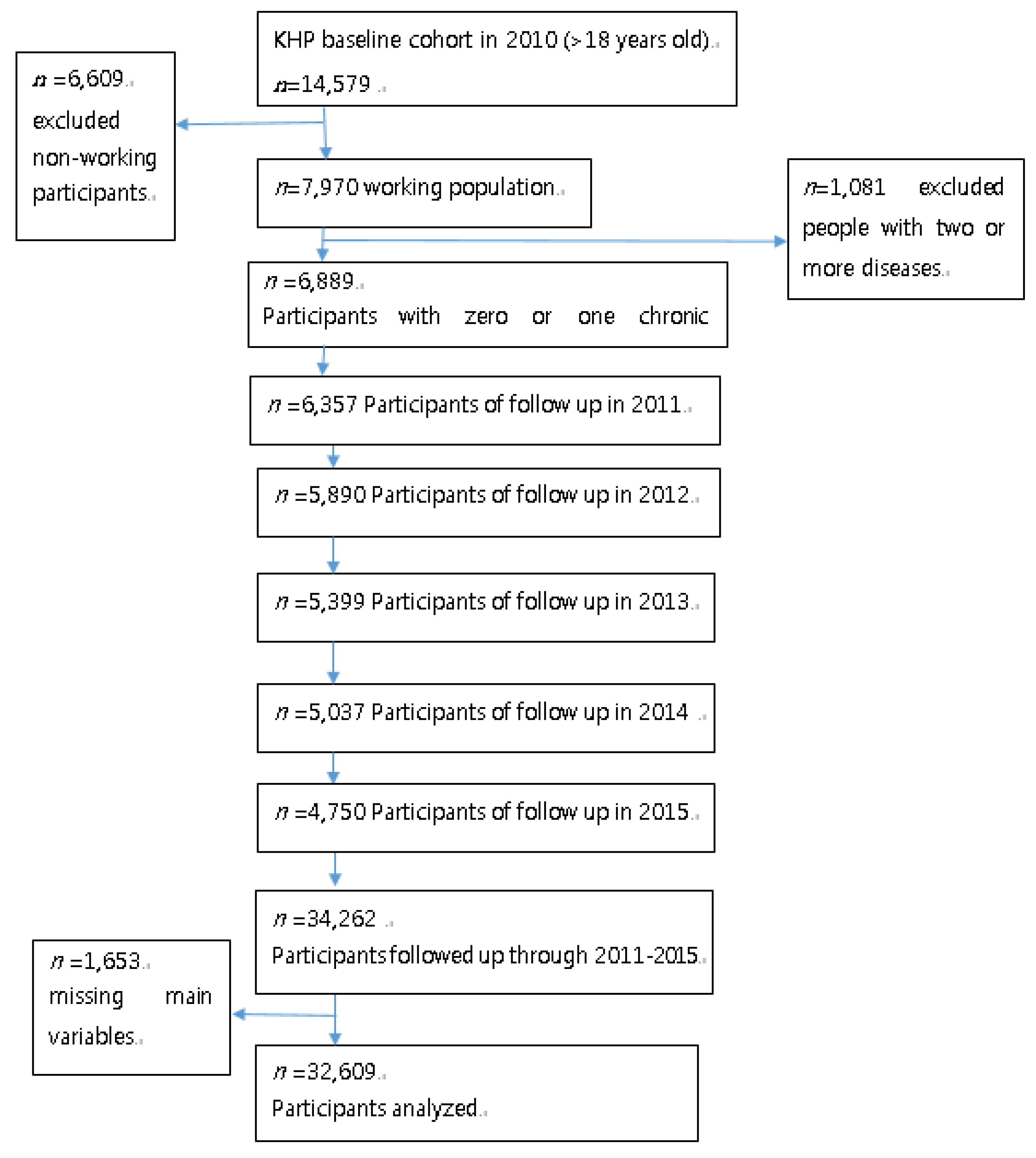
2.1. Data
2.2. Variables and Measurement
2.3. Statistical Analysis
3. Results
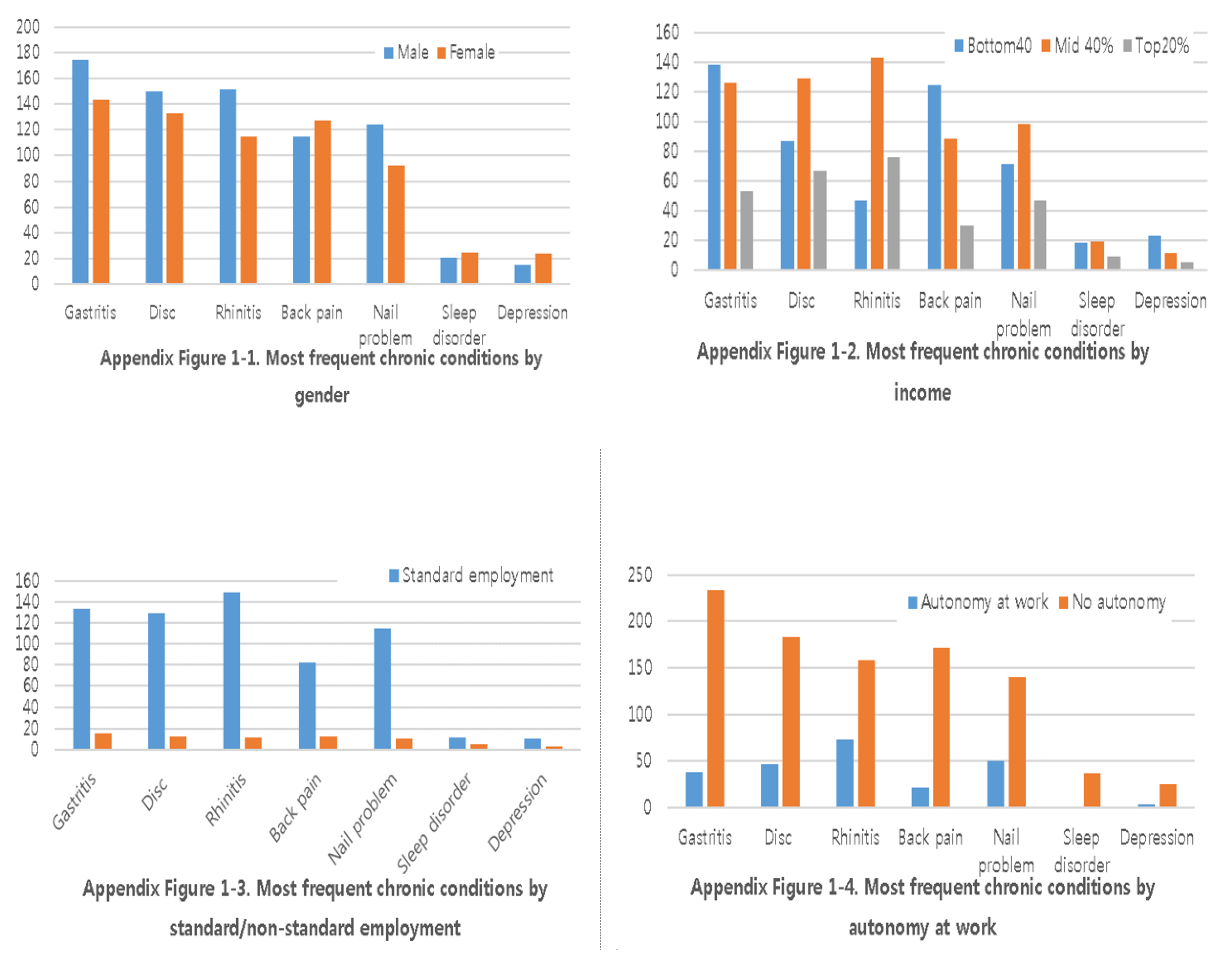
3.1. Sample Description
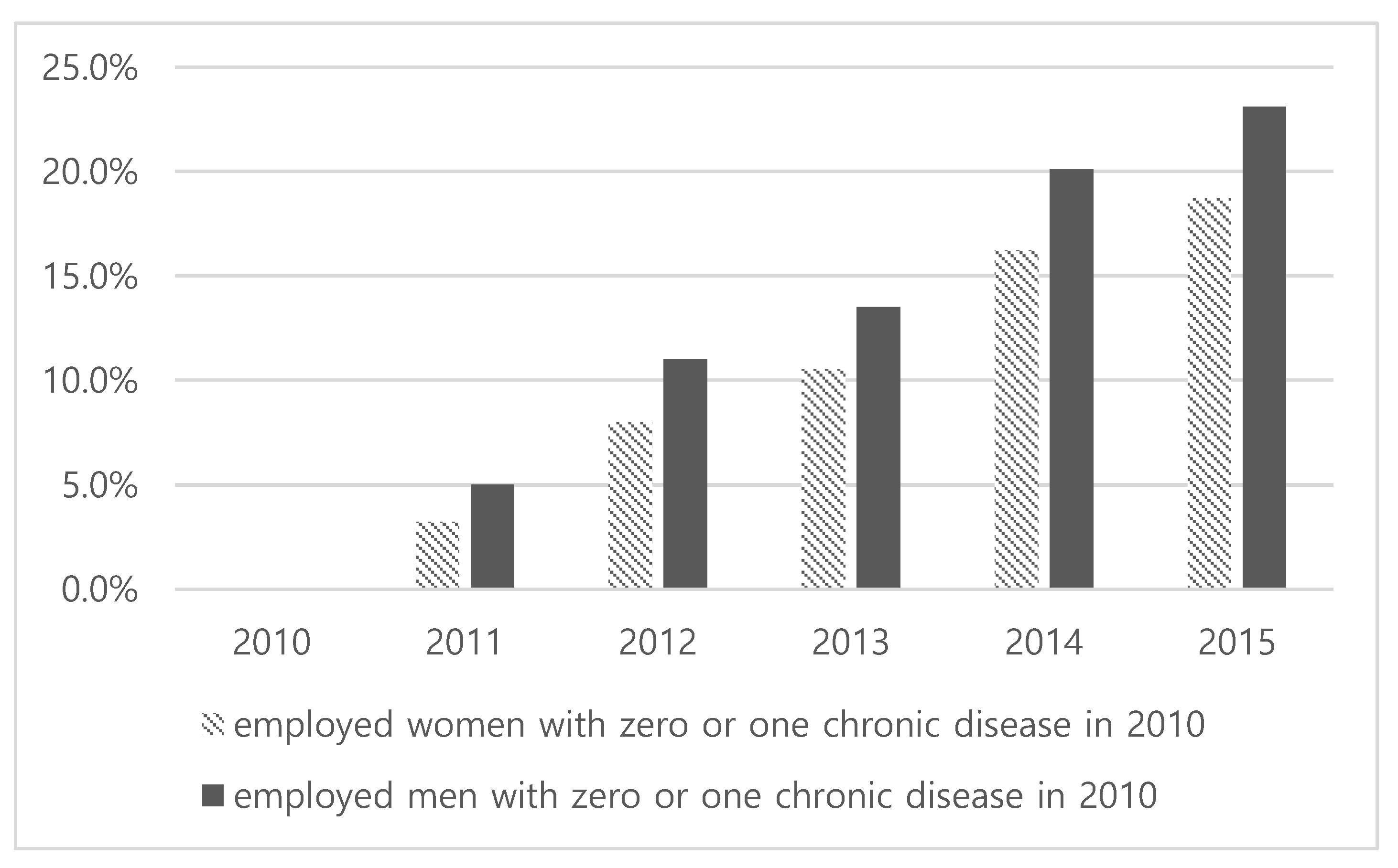
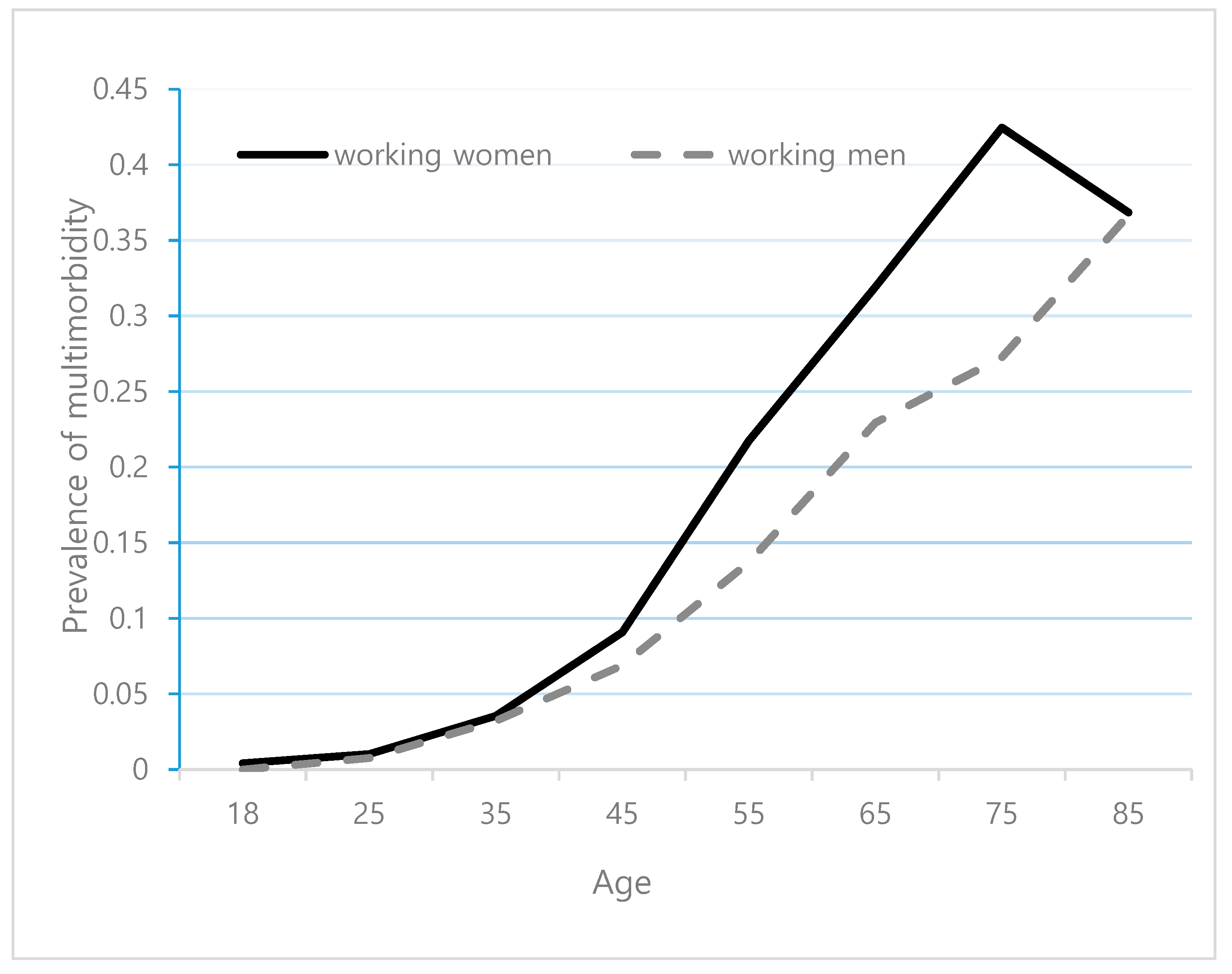
3.2. Prevalence of Multimorbidity
3.3. Regression Results
4. Discussion
5. Conclusions and Policy Implications
Author Contributions
Funding
Availability of Data and Materials
Conflicts of Interest
Abbreviations
| SES | Socioeconomic status |
| KHP | Korea Health Panel |
| KIHASA | Korea Institute for Health and Social Affairs |
| BMI | Body mass index |
| OR | Odds ratio |
| CI | Confidence interval |
| FFS | Fee-for-services |
Appendix A

Appendix B



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2010–2011 | 2012–2015 | ||||||
|---|---|---|---|---|---|---|---|
| No | Chronic Disease | KCD-6 | Freq (%) | No | Chronic Disease | ICD-10 | Freq (%) |
| 1 | Hypertension | 19,031 | 4893 (14.3) | 1 | Hypertension | I10 | 12,141 (12.22) |
| 2 | Arthritis | 23,021 | 2482 (7.17) | 2 | Hyperlipidemia | E78 | 5246 (5.28) |
| 3 | Gastritis | 21,051 | 1819 (5.25) | 3 | Diabetes | E14 | 4811 (4.84) |
| 4 | Diabetes | 14,021 | 1809 (5.22) | 4 | Gastritis | K29 | 4531 (4.56) |
| 5 | Allergic rhinitis | 20,081 | 1290 (3.72) | 5 | Allergic rhinitis | J30 | 4518 (4.55) |
| 6 | Osteoporosis | 23,091 | 1105 (3.19) | 6 | Arthritis | M14 | 4400 (4.43) |
| 7 | Back pain | 23,072 | 1054 (3.04) | 7 | Osteoporosis | M81 | 3200 (3.22) |
| 8 | Hyperlipidaemia | 14,081 | 1042 (3.01) | 8 | Disc disorder | M54 | 3178 (3.20) |
| 9 | Disc disorder | 23,061 | 1039 (3.00) | 9 | Arthritis | M19 | 3119 (3.14) |
| 10 | Cataract disease | 17,041 | 887 (2.25) | 10 | Cataract disease | H26 | 2876 (2.89) |
| 11 | Gingivitis | 21,022 | 780 (2.25) | 11 | Gingivitis | K05 | 2427 (2.44) |
| 12 | Nail diseases | 11,282 | 613 (1.77) | 12 | Disc disorder | M51 | 2148 (2.16) |
| 13 | Atopic dermatitis | 22,022 | 530 (1.53) | 13 | Nail disease | B35 | 1880 (1.89) |
| 14 | Dry eye | 17,101 | 528 (1.52) | 14 | Spondylopathesis | M48 | 1650 (1.66) |
| 15 | Rhinitis | 20,082 | 517 (1.49) | 15 | Prostate problem | N40 | 1620 (1.63) |
| 16 | Prostate problem | 24,081 | 456 (1.32) | 16 | Eye disease | H18 | 1537 (1.55) |
| 17 | Asthma | 20,121 | 441 (1.27) | 17 | Atopic dermatitis | L20 | 1388 (1.40) |
| 18 | Allergy | 22,020 | 425 (1.23) | 18 | Muscular disease | M79 | 1260 (1.27) |
| 19 | Dental caries | 21,011 | 413 (1.19) | 19 | Dental caries | K02 | 1105 (1.11) |
| 20 | Disc disorder | 23,074 | 350 (1.01) | 20 | Asthma | J45 | 1045 (1.05) |
| 21 | Angina | 19,051 | 349 (1.01) | 21 | Disc disorder | M50 | 1039 (1.05) |
| 22 | Sleep disorder | G47 | 1033 (1.04) | ||||
| 23 | Major depressive disorder | F32 | 996 (1.00) | ||||
References
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef]
- Katikireddi, S.V.; Skivington, K.; Leyland, A.H.; Hunt, K.; Mercer, S.W. The contribution of risk factors to socioeconomic inequalities in multimorbidity across the life course: A longitudinal analysis of the Twenty-07 cohort. BMC Med. 2017, 15, 152. [Google Scholar] [CrossRef] [PubMed]
- Violan, C.; Foguet-Boreu, Q.; Flores-Mateo, G.; Salisbury, C.; Blom, J.; Freitag, M.; Glynn, L.; Muth, C.; Valderas, J.M. Prevalence, determinants and patterns of multimorbidity in primary care: A systematic review of observational studies. PLoS ONE 2014, 9, e102149. [Google Scholar] [CrossRef] [PubMed]
- Bielecky, A.; Chen, C.; Ibrahim, S.; Beaton, D.E.; Mustard, C.A.; Smith, P.M. The impact of co-morbid mental and physical disorders on presenteeism. Scand. J. Work Environ. Health 2015, 41, 554–564. [Google Scholar] [CrossRef]
- Singer, L.; Green, M.; Rowe, F.; Ben-Shlomo, Y.; Morrissey, K. Social determinants of multimorbidity and multiple functional limitations among the ageing population of England, 2002–2015. SSM Popul. Health 2019, 8, 100413. [Google Scholar] [CrossRef]
- Gignac, M.A.; Sutton, D.; Badley, E.M. Arthritis symptoms, the work environment, and the future: Measuring perceived job strain among employed persons with arthritis. Arthritis Rheum. 2007, 57, 738–747. [Google Scholar] [CrossRef]
- Wang, H.H.; Wang, J.J.; Lawson, K.D.; Wong, S.Y.; Wong, M.C.; Li, F.J.; Wang, P.X.; Zhou, Z.H.; Zhu, C.Y.; Yeong, Y.Q. Relationships of multimorbidity and income with hospital admissions in 3 health care systems. Ann. Fam. Med. 2015, 13, 164–167. [Google Scholar] [CrossRef]
- Holden, L.; Shuffham, P.A.; Hilton, M.F.; Muspratt, A.; Ng, S.-K.; Whiteford, H.A. Patterns of multimorbidity in working Australians. Popul. Health Metr. 2011, 9, 15. [Google Scholar] [CrossRef]
- Smith, P.; Chen, C.; Mustard, C.; Bielecky, A.; Beaton, D.; Ibrahim, S. Examining the relationship between chronic conditions, multi-morbidity and labour market participation in Canada: 2000–2005. Ageing Soc. 2014, 34, 1730–1748. [Google Scholar] [CrossRef]
- Tetzlaff, J.; Epping, J.; Sperlich, S.; Eberhard, S.; Stahmeyer, J.T.; Geyer, S. Widening inequalities in multimorbidity? Time trends among the working population between 2005 and 2015 based on German health insurance data. Int. J. Equity Health 2018, 17, 103. [Google Scholar] [CrossRef]
- Sakib, M.N.; Shooshtari, S.; John, P.S.; Menec, V. The prevalence of multimorbidity and associations with lifestyle factors among middle-aged Canadians: An analysis of Canadian Longitudinal Study on Aging data. BMC Public Health 2019, 19, 243. [Google Scholar] [CrossRef] [PubMed]
- Melis, R.; Marengoni, A.; Angleman, S.; Fratiglioni, L. Incidence and predictors of multimorbidity in the elderly: A population-based longitudinal study. PLoS ONE 2014, 9, e103120. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Patel, S.A.; Biswas, S.; Shivashankar, R.; Kondal, D.; Ajay, V.S.; Anjana, R.M.; Fatmi, Z.; Ali, M.K.; Kadir, M.M. Multimorbidity in south asian adults. J. Public Health 2018, 41, 1–10. [Google Scholar]
- Shultz, K.S.; Wang, M.; Crimmins, E.M.; Fisher, G.G. Age differences in the demand–control model of work stress: An examination of data from European countries. J. Appl. Gerontol. 2010, 29, 21–47. [Google Scholar] [CrossRef] [PubMed]
- Standard Chartered. Standard Chartered State of Work-Life Balance in Seoul 2010 Survey. A Summary of Research Findings [Internet]. Community Bus; 2010 [Cited 2016 Jan 15]. 52p. Available online: http://www.communitybusiness.org/images/cb/publications/2010/WLB KR.pdf (accessed on 7 February 2019).
- Choi, E.; Kim, J. The association between work–life balance and health status among Korean workers. Work 2017, 58, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Korea Health Panel. Available online: http:/kihasa.re.kr (accessed on 17 January 2019).
- van den Bussche, H.K.; Daniela, K.T.; Hansen, H.; Wegscheider, K.; Glaeske, G.; von Leitner, E.; Schäfer, I.; Schön, G. Which chronic diseases and disease combinations are specific to multimorbidity in the elderly? Results of a claims data based cross-sectional study in Germany. BMC Public Health 2011, 11, 101. [Google Scholar] [CrossRef]
- Blossfeld, H.-P. Labor-market entry and the sexual segregation of careers in the Federal Republic of Germany. AJS 1987, 93, 89–118. [Google Scholar] [CrossRef]
- Dhalwani, N.N.; Zaccardi, F.; O’Donovan, G.; Carter, P.; Hamer, M.; Yates, T.; Davies, M.; Khunti, K. Association between lifestyle factors and the incidence of multimorbidity in an older English population. J. Gerontol. 2016, 72, 528–534. [Google Scholar] [CrossRef]
- Hussin, N.M.; Shahar, S.; Din, N.C.; Singh, D.K.; Chin, A.V.; Razali, R.; Omar, M.A. Incidence and predictors of multimorbidity among a multiethnic population in Malaysia: A community-based longitudinal study. Aging Clin. Exp. Res. 2019, 31, 215–224. [Google Scholar] [CrossRef]
- von dem Knesebeck, O.; Bickel, H.; Fuchs, A.; Gensichen, J.; Höfels, S.; Riedel-Heller, S.G.; König, H.-H.; Mergenthal, K.; Schön, G.; Wegscheider, K. Social inequalities in patient-reported outcomes among older multimorbid patients–results of the MultiCare cohort study. Int. J. Equity Health 2015, 14, 17. [Google Scholar] [CrossRef]
- Seo, S.; Kwon, Y.D.; Yoo, K.B.; Lee, Y.; Noh, J.W. Is Transient and persistent poverty harmful to multimorbidity? Int. J. Environ. Res. Public Health 2019, 16, 2395. [Google Scholar] [CrossRef] [PubMed]
- Geyer, S.; Hemström, O.; Peter, R.; Vagerö, D. Education, income, and occupational class cannot be used interchangeably in social epidemiology. Empirical evidence against a common practice. J. Epidemiol. Community Health 2006, 60, 804–810. [Google Scholar]
- Wang, H.H.; Wang, J.J.; Wong, S.Y.; Wong, M.C.; Li, F.J.; Wang, P.X.; Zhou, Z.H.; Zhu, C.Y.; Griffiths, S.M.; Mercer, S.W. Epidemiology of multimorbidity in China and implications for the healthcare system: Cross-sectional survey among 162,464 community household residents in southern China. BMC Med. 2014, 12, 188. [Google Scholar] [CrossRef] [PubMed]
- Contoyannis, P.; Jones, A.M. Socio-economic status, health and lifestyle. J. Health Econ. 2004, 23, 965–995. [Google Scholar] [CrossRef]
- Mercer, S.W.; Guthrie, B.; Furler, J.; Watt, G.C.; Hart, J.T. Multimorbidity and the inverse care law in primary care. Br. Med. J. Publ. Group 2012, 344, e4152. [Google Scholar] [CrossRef]
- An, A.R.; Kim, K.; Lee, J.-H.; Sung, N.-J.; Lee, S.; Hyun, M.K. Having a usual source of care and its associated factors in Korean adults: A cross-sectional study of the 2012 Korea Health Panel Survey. BMC Fam. Pract. 2016, 17, 167. [Google Scholar] [CrossRef] [Green Version]


| Variables n (%) Mean (SD) | Total | Female | Male | t, Chi2 |
|---|---|---|---|---|
| n = 6889 (100.0) | n = 2743 (39.8) | n = 4146 (60.2) | ||
| Age (years) | 45.4 (12.49) | 44.1 (0.25) | 46.3 (0.19) | −7.20 *** |
| Age group | ||||
| <45 | 3513 | 1487 (42.3) | 2023 (57.7) | 19.32 *** |
| 45–55 | 1934 | 729 (37.7) | 1205 (62.3) | |
| >55 | 1442 | 527 (36.5) | 915 (63.5) | |
| Standard employment-based job | ||||
| Standard | 4418 | 1735 (39.3) | 2683 (60.7) | 10.33 *** |
| Non-standard | 373 | 178 (47.7) | 195 (52.3) | |
| Others | 2098 | 830 (39.6) | 1268 (60.4) | |
| Autonomy at work | ||||
| Autonomy | 1418 | 230 (16.2) | 1188 (83.8) | 523.36 *** |
| No autonomy | 4260 | 1928 (45.3) | 2332 (54.7) | |
| Do not know | 550 | 357 (64.9) | 193 (35.1) | |
| Occupation type | ||||
| Highly qualified | 1650 | 613 (37.2) | 1037 (62.8) | 228.98 *** |
| Specialist | 812 | 428 (52.7) | 384 (47.3) | |
| Skilled | 2731 | 847 (31.0) | 1884 (69.0) | |
| Unskilled | 1696 | 855 (50.4) | 841 (49.6) | |
| Income | ||||
| Bottom 40% | 1704 | 695 (40.8) | 1009 (59.2) | 4.32 |
| Mid 40% | 3320 | 1280 (38.5) | 2040 (61.5) | |
| Top 20% | 1865 | 768 (41.2) | 1097 (58.8) | |
| Education | ||||
| Elementary | 1610 | 797 (49.5) | 813 (50.5) | 90.29 *** |
| High school | 2530 | 983 (38.8) | 1547 (61.2) | |
| College+ | 2749 | 963 (35.0) | 1786 (65.0) | |
| Marital status | ||||
| Married | 5274 | 1897 (36.0) | 3377 (64.0) | 139.03 *** |
| Unmarried | 1615 | 846 (52.4) | 769 (47.6) | |
| Having school-age children | ||||
| Yes | 3574 | 1377 (38.5) | 2197 (61.5) | 10.89 *** |
| No | 3142 | 1335 (42.5) | 1807 (57.5) | |
| Unmet health care needs | ||||
| No | 2552 | 1148 (45.0) | 1404 (55.0) | 44.42 *** |
| Yes | 3086 | 1168 (37.8) | 1918 (62.2) | |
| No need | 965 | 333 (34.5) | 632 (65.5) | |
| Currently smoking | ||||
| No smoking | 4671 | 2650 (56.7) | 2021 (43.3) | 170.0 *** |
| Smoking | 2045 | 62(3.0) | 1983(97.0) | |
| Binge drinking | ||||
| Never | 4212 | 2316 (55.0) | 1896 (45.0) | 100.0 *** |
| Sometimes+ | 2504 | 396 (15.8) | 2108 (84.2) | |
| Physical activity | ||||
| No | 2526 | 860 (34.0) | 1666 (66.0) | 67.50 *** |
| Sometimes+ | 4190 | 1852 (44.2 | 2338 (55.8) | |
| Variables | Prevalence Rate Per 100 Person Year (95% CI) | ||||||
|---|---|---|---|---|---|---|---|
| Total | Female Workers | Male Workers | |||||
| Overall | 4.88 | (4.61–5.16) | 5.55 | (5.10–6.03) | 4.44 | (4.12–4.79) | |
| Age group (years) | <45 | 1.60 | (1.38–1.86) | 1.35 | (1.05–1.73) | 1.79 | (1.48–2.16) |
| 45–55 | 4.64 | (4.19–5.14) | 5.72 | (4.92–6.64) | 3.98 | (3.46–4.58) | |
| 55+ | 10.59 | (9.83–11.42) | 13.44 | (12.03–15.00) | 8.96 | (8.09–9.93) | |
| Income | Bottom 40% | 6.91 | (6.28–7.61) | 8.46 | (7.37–9.70) | 5.87 | (5.13–6.72) |
| Mid 40% | 4.42 | (4.06–4.81) | 5.00 | (4.40–5.69) | 4.06 | (3.63–4.54) | |
| Top 20% | 3.91 | (3.47–4.41) | 3.94 | (3.27–4.75) | 3.89 | (3.33–4.55) | |
| Education | Elementary | 9.87 | (9.05–10.76) | 11.31 | (10.08–12.70) | 8.48 | (7.44–9.66) |
| High school | 4.80 | (4.38–5.25) | 5.30 | (4.62–6.08) | 4.48 | (3.97–5.05) | |
| College+ | 2.38 | (2.10–2.71) | 1.63 | (1.26–2.11) | 2.78 | (2.41–3.22) | |
| Marital status | Married | 5.36 | (5.05–5.70) | 5.97 | (5.43–6.57) | 5.02 | (4.64–5.43) |
| Unmarried | 3.18 | (2.74–3.68) | 4.47 | (3.74–5.32) | 1.90 | (1.45–2.49) | |
| Having schoolage children | Yes | 3.93 | (3.61–4.28) | 7.07 | (6.35–7.88) | 3.76 | (3.36–4.20) |
| No | 6.18 | (5.74–6.67) | 4.22 | (6.69–4.82) | 5.54 | (4.99–6.15) | |
| Standard employment | Yes | 3.65 | (3.34–3.98) | 4.32 | (3.78–4.94) | 3.26 | (2.90–3.67) |
| No | 5.79 | (4.57–7.35) | 7.02 | (5.02–9.83) | 4.93 | (3.52–6.90) | |
| Autonomy at work | Yes | 3.38 | (2.93–3.91) | 2.83 | (1.91–4.19) | 3.49 | (2.98–4.07) |
| No | 5.17 | (4.83–5.52) | 5.80 | (5.27–6.38) | 4.67 | (4.25–5.13) | |
| Occupation type | Highly qualified | 2.83 | (2.42–3.32) | 2.26 | (1.67–3.05) | 3.15 | (2.61–3.80) |
| Specialist | 2.46 | (1.91–3.16) | 1.96 | (1.30–2.95) | 2.91 | (2.12–4.00) | |
| Skilled | 5.57 | (5.11–6.08) | 7.67 | (6.66–8.82) | 4.77 | (4.27–5.32) | |
| Unskilled | 5.90 | (5.27–6.60) | 7.09 | (6.12–8.22-) | 4.78 | (4.02–5.69) | |
| Variables | Female Workers | Male Workers | ||
|---|---|---|---|---|
| Odds Ratio | 95% CI | Odds Ratio | 95% CI | |
| Age group (referenced to 55+) | ||||
| <45 | 0.17 *** | (0.13–0.22) | 0.30 *** | (0.24–0.37) |
| 45–55 | 0.42 *** | (0.34–0.51) | 0.58 *** | (0.49–0.68) |
| Standard employment-based job | 0.79 * | (0.61–1.02) | 1.08 | (0.86–1.38) |
| Non-autonomy at work | 1.05 | (0.79–1.40) | 0.95 | (0.82–1.10) |
| Occupation type (ref. to unskilled) | ||||
| Highly qualified | 1.15 | (0.85–1.55) | 0.99 | (0.78–1.26) |
| Specialist | 0.79 | (0.55–1.15) | 1.17 | (0.85–1.60) |
| Skilled | 0.93 | (0.78–1.11) | 1.04 | (0.87–1.23) |
| Income (ref to. Bottom 40%): | ||||
| Mid 40% | 0.84 ** | (0.74–0.97) | 0.96 | (0.84–1.09) |
| Top 20% | 0.84 * | (0.70–1.01) | 0.88 | (0.74–1.04) |
| Education (ref. to college+): | ||||
| Elementary school | 2.95 *** | (2.12–4.12) | 1.69 *** | (1.35–2.12) |
| High school | 2.53 *** | (1.88–3.43) | 1.48 *** | (1.26–2.38) |
| Married | 0.96 | (0.79–1.16) | 1.85 *** | (1.43–4.11) |
| Having school age children | 0.97 | (0.79–1.19) | 0.85 *** | (0.72–1.00) |
| Unmet health care needs (ref.to non-unmet need) | ||||
| Unmet needs | 1.20 *** | (1.06–1.40) | 0.95 | (0.83–1.09) |
| No health care needs | 0.51 *** | (0.30–0.84) | 0.83 | (0.62–1.09) |
| Currently smoking | 0.92 | (0.58–1.44) | 0.74 *** | (0.65–0.85) |
| Binge drinking | 0.83 | (0.66–1.05) | 0.90 * | (0.79–1.01) |
| Physical inactivity Year (ref.2011) | 0.88 ** | (0.79–0.99) | 0.92 | (0.82–1.02) |
| 2012 | 2.31 *** | (1.93–2.77) | 2.66 *** | (2.22–3.19) |
| 2013 | 2.80 *** | (2.34–3.31) | 3.39 *** | (2.83–4.05) |
| 2014 | 4.65 *** | (3.88–5.57) | 5.62 *** | (4.71–6.70) |
| 2015 | 5.15 *** | (4.30–6.17) | 6.40 *** | (5.36–7.65) |
| N | 13,299 | 19,310 | ||
| Persons | 2509 | 3683 | ||
| GEE correlation option | Exchangeable | |||
| GEE family option | Binomial | |||
| Wald F test | 1065.24 *** | 675.02 *** | ||
© 2019 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, S. Multimorbidity Development in Working People. Int. J. Environ. Res. Public Health 2019, 16, 4749. https://doi.org/10.3390/ijerph16234749
Seo S. Multimorbidity Development in Working People. International Journal of Environmental Research and Public Health. 2019; 16(23):4749. https://doi.org/10.3390/ijerph16234749
Chicago/Turabian StyleSeo, Sukyong. 2019. "Multimorbidity Development in Working People" International Journal of Environmental Research and Public Health 16, no. 23: 4749. https://doi.org/10.3390/ijerph16234749
APA StyleSeo, S. (2019). Multimorbidity Development in Working People. International Journal of Environmental Research and Public Health, 16(23), 4749. https://doi.org/10.3390/ijerph16234749