Can Financial Support Reduce Suicide Mortality Rates?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Summary of Emergency Fund to Enhance Community-Based Suicide Countermeasures
2.3. Standardisation of Suicide Mortality Rates
2.4. Statistical Analysis
3. Results
3.1. 2009–2018 EBSMR Trends for Regional Suicide Mortality Ratios
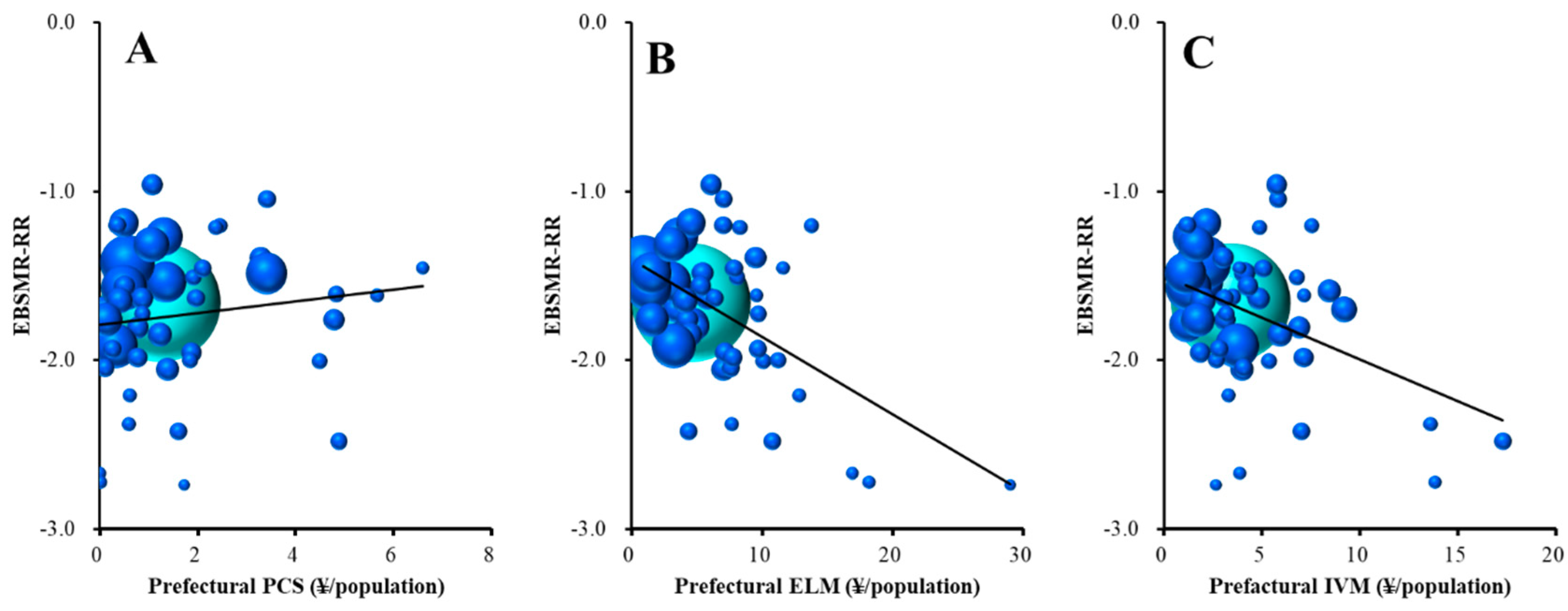
3.2. Relationship between Suicide Mortality Trends (EBSMR-RR) and REA in 47 Prefectures
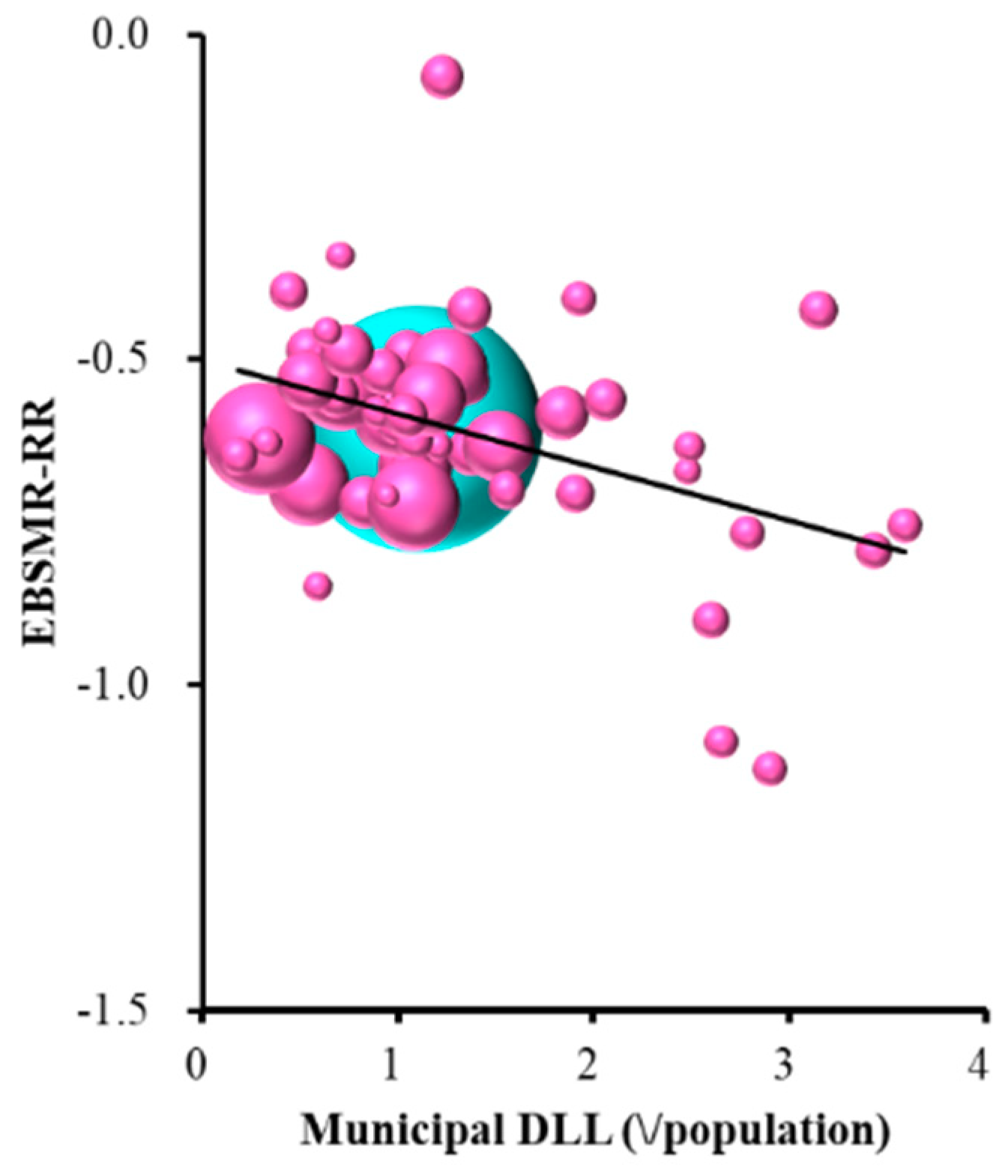
3.3. Relationship between EBSMR-RR and 10 REA Subgroups
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- OECD. Suicide Rates (Indicator). Available online: https://data.oecd.org/healthstat/suicide-rates.htm (accessed on 12 November 2019).
- Kino, S.; Jang, S.N.; Gero, K.; Kato, S.; Kawachi, I. Age, period, cohort trends of suicide in Japan and Korea (1986–2015): A tale of two countries. Soc. Sci. Med. 2019, 235, 112385. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labor and Welfare. Basic Data on Suicide in the Region. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000140901.html (accessed on 12 November 2019).
- Ministry of Health, Labor and Welfare.National Plan for Prevention of Suicide. Available online: https://www.mhlw.go.jp/kokoro/nation/about.html (accessed on 12 November 2019).
- Ministry of Health, Labor and Welfare.Bugets for Suicide Prevention Programmes. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000133838.html (accessed on 12 November 2019).
- Ministry of Health, Labor and Welfare. Regional Suicide Countermeasures Emergency Enhancement Fund. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000134741.html (accessed on 12 November 2019).
- Dhungel, B.; Sugai, M.K.; Gilmour, S. Trends in Suicide Mortality by Method from 1979 to 2016 in Japan. Int. J. Environ. Res. Public Health 2019, 16, 1794. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.S.; Gunnell, D.; Sterne, J.A.; Lu, T.H.; Cheng, A.T. Was the economic crisis 1997–1998 responsible for rising suicide rates in East/Southeast Asia? A time-trend analysis for Japan, Hong Kong, South Korea, Taiwan, Singapore and Thailand. Soc. Sci. Med. 2009, 68, 1322–1331. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, E.; Kashima, S.; Kawachi, I.; Subramanian, S.V. Social and geographical inequalities in suicide in Japan from 1975 through 2005: A census-based longitudinal analysis. PLoS ONE 2013, 8, e63443. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare. National Plan for Prevention of Suicide. Available online: www.mohw.go.kr/react/modules/download.jsp?BOARD_ID=140&CONT (accessed on 12 November 2019).
- Ministry of Health, Labor and Welfare. Law Concerning the Promotion of Research and the Utilization of the Results to Contribute to the Comprehensive and Effective Implementation of Suicide Countermeasures. Available online: https://elaws.e-gov.go.jp/search/elawsSearch/elaws_search/lsg0500/detail?lawId=501AC1000000032_20190912_000000000000000&openerCode=1 (accessed on 12 November 2019).
- Suzuki, E.; Kashima, S.; Kawachi, I.; Subramanian, S.V. Prefecture-level economic conditions and risk of suicide in Japan: A repeated cross-sectional analysis 1975–2010. Eur. J. Public Health 2014, 24, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Tanii, H. The measures of suicidal prevention in Mie Prefecture, Japan. J. Forensic Leg. Med. 2008, 15, 411–412. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K.; Abe, S.; Okazaki, Y.; Fukunaga, T. Underlying factors for the rapid increase of suicide in Mie Prefecture, Japan. Med. Sci. Law 2005, 45, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Statistics Bureau of the Ministry of Internal Affairs and Communications. Population, Demographics and Number of Households Based on Basic Resident Register. Available online: http://www.soumu.go.jp/main_sosiki/jichi_gyousei/daityo/jinkou_jinkoudoutai-setaisuu.html (accessed on 12 November 2019).
- Yoshikawa, H. Japan’s Lost Decade: What Have We Learned and Where Are We Heading? Asian Econ. Policy Rev. 2007, 2, 186–203. [Google Scholar] [CrossRef]
- Ahmad, O.B.; Boschi-Pinto, C.; Lopez, A.D.; Murray, C.J.; Lozano, R.; Inoue, M. Age standardization of rates: A new WHO standard. In GPE Discussion Paper Series: No.31; World Health Organization: Geneva, Switzerland, 2001; Volume 9. [Google Scholar]
- Stuckler, D.; Basu, S.; Suhrcke, M.; Coutts, A.; McKee, M. The public health effect of economic crises and alternative policy responses in Europe: An empirical analysis. Lancet 2009, 374, 315–323. [Google Scholar] [CrossRef]
- Kawaguchi, H.; Koike, S. Association between the Density of Physicians and Suicide Rates in Japan: Nationwide Ecological Study Using a Spatial Bayesian Model. PLoS ONE 2016, 11, e0148288. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Wu, K.C.; Yousuf, S.; Yip, P.S. Suicide in Asia: Opportunities and challenges. Epidemiol. Rev. 2012, 34, 129–144. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Kim, M.H.; Kawachi, I.; Cho, Y. Comparative epidemiology of suicide in South Korea and Japan: Effects of age, gender and suicide methods. Crisis 2011, 32, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.R.; Li, X.; Zhang, Y. Suicide rates in China, 1995–1999. Lancet 2002, 359, 835–840. [Google Scholar] [CrossRef]
- Pearson, V. Goods on which one loses: Women and mental health in China. Soc. Sci. Med. 1995, 41, 1159–1173. [Google Scholar] [CrossRef]
- Ji, J.; Kleinman, A.; Becker, A.E. Suicide in contemporary China: A review of China’s distinctive suicide demographics in their sociocultural context. Harv. Rev. Psychiatry 2001, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Oyama, H.; Koida, J.; Sakashita, T.; Kudo, K. Community-based prevention for suicide in elderly by depression screening and follow-up. Community Ment. Health J. 2004, 40, 249–263. [Google Scholar] [CrossRef] [PubMed]
- Motohashi, Y.; Kaneko, Y.; Sasaki, H.; Yamaji, M. A decrease in suicide rates in Japanese rural towns after community-based intervention by the health promotion approach. Suicide Life Threat. Behav. 2007, 37, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Myles, N.; Large, M.; Myles, H.; Adams, R.; Liu, D.; Galletly, C. Australia’s economic transition, unemployment, suicide and mental health needs. Aust. N. Z. J. Psychiatry 2017, 51, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Agrrawal, P.; Waggle, D.; Sandweiss, D.H. Suicides as a response to adverse market sentiment (1980–2016). PLoS ONE 2017, 12, e0186913. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (Male plus Female) | Male | Female | ||||||
|---|---|---|---|---|---|---|---|---|---|
| β | p | VIF | β | p | VIF | β | p | VIF | |
| Prefecture | |||||||||
| PCS | +0.252 | <0.05 | 1.04 | ||||||
| TCS | |||||||||
| DLL | |||||||||
| ELM | −0.410 | <0.01 | 1.03 | −0.500 | <0.01 | 1.08 | |||
| IVM | −0.312 | <0.05 | 1.08 | ||||||
| Municipality | |||||||||
| PCS | |||||||||
| TCS | |||||||||
| DLL | −0.312 | <0.05 | 1.03 | −0.409 | <0.01 | 1.00 | |||
| ELM | |||||||||
| IVM | |||||||||
| F = 9.806 Adjusted R2 = 0.277 | <0.01 | F = 10.697 Adjusted R2 = 0.389 | <0.01 | F = 9.066 Adjusted R2 = 0.149 | <0.01 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kato, R.; Okada, M. Can Financial Support Reduce Suicide Mortality Rates? Int. J. Environ. Res. Public Health 2019, 16, 4797. https://doi.org/10.3390/ijerph16234797
Kato R, Okada M. Can Financial Support Reduce Suicide Mortality Rates? International Journal of Environmental Research and Public Health. 2019; 16(23):4797. https://doi.org/10.3390/ijerph16234797
Chicago/Turabian StyleKato, Ryo, and Motohiro Okada. 2019. "Can Financial Support Reduce Suicide Mortality Rates?" International Journal of Environmental Research and Public Health 16, no. 23: 4797. https://doi.org/10.3390/ijerph16234797
APA StyleKato, R., & Okada, M. (2019). Can Financial Support Reduce Suicide Mortality Rates? International Journal of Environmental Research and Public Health, 16(23), 4797. https://doi.org/10.3390/ijerph16234797