Toward an Expanded Focus for Occupational Safety and Health: A Commentary



Abstract
:1. Introduction
2. Changes in the World of Work and Worker Well-Being
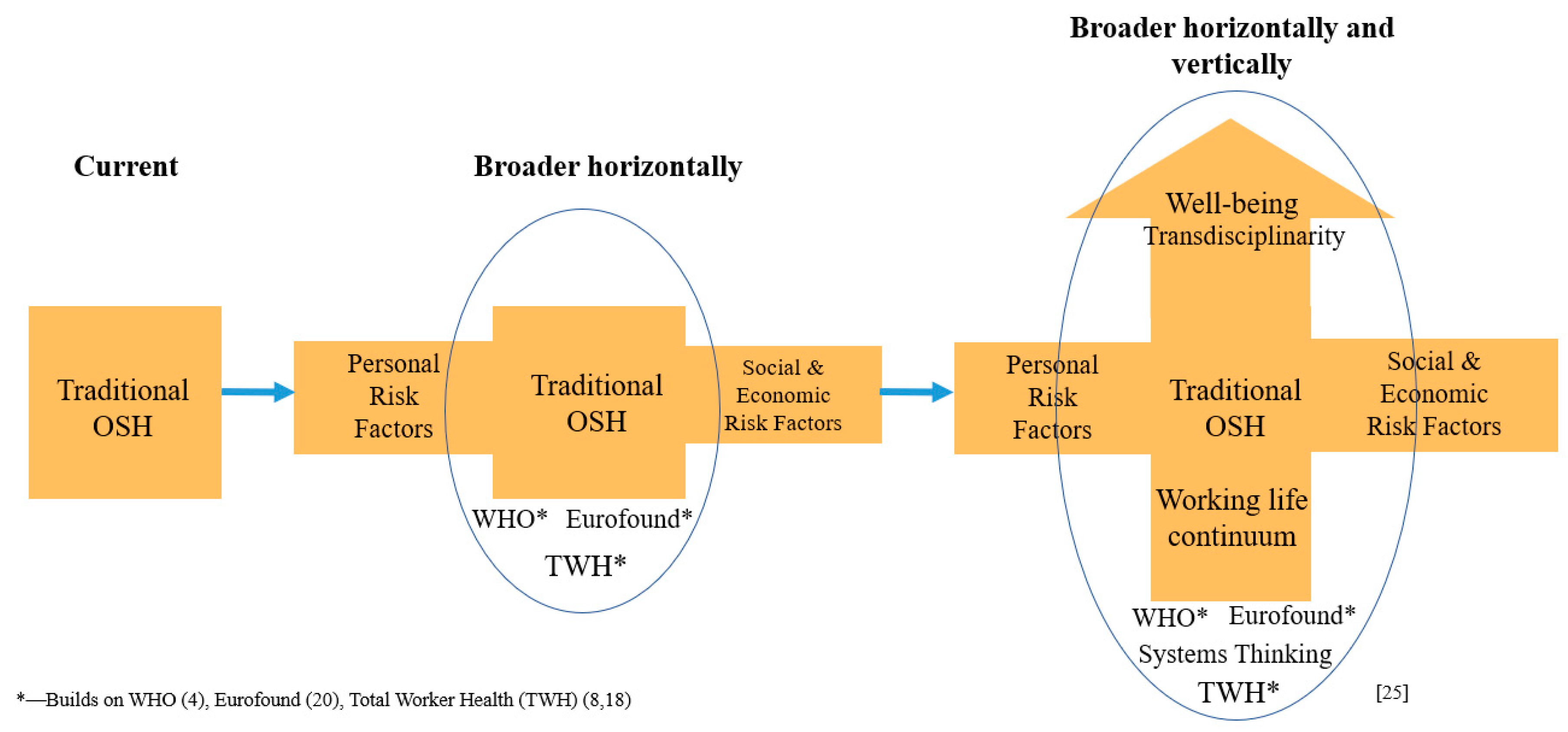
2.1. Horizontal Thinking
2.2. Vertical Thinking
3. Operationalizing the Concept of Worker Well-Being
4. Traditional and New OSH Skill Sets
5. Efforts in Developing an Expanded Focus for OSH
5.1. Systems Approach to OSH
5.2. Future of the OSH Professions
5.3. Active Marketing of OSH
6. Concerns and Issues about an Expanded Focus of OSH
- Employer/managers may emphasize individual approaches such as vitality/fitness and coping behavior, instead of primary stress prevention such as job autonomy, skill discretion, collaborative organizational leadership, or reducing physical workload.
- Employers/managers may reject responsibility because the health problems are related to stress in private life, sports, etc.
- Given all the technologies to monitor their workers, employers/managers might focus on selecting only healthy workers for certain jobs, instead of helping all workers improve their health.
- Employers/managers may reduce “employability” to vitality/fitness instead of creating a learning work environment (Reviewer’s comment. This is a personal communication in a review of the paper).
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rantenen, J. Research challenges arising from changes in work life. Scand. J. Work Environ. Health 1999, 25, 473–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howard, J. Nonstandard work arrangements and worker health and safety. Am. J. Ind. Med. 2017, 60, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peckham, T.T.; Baker, M.G.; Camp, J.E.; Kaufman, J.D.; Sexias, N.S. Creating future for occupational health. Ann. Work Expo. Health 2017, 61, 3–15. [Google Scholar] [PubMed]
- Burton, J. Healthy Workplaces: A Model for Action for Employers, Workers, Policy Makers, and Practitioners; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Benach, J.; Vives, A.; Amable, M.; Vanroelen, C.; Tarafa, G.; Muntaner, C. Precarious employment: Understanding an emerging social determinant of health. Ann. Rev. Public Health 2014, 35, 329–353. [Google Scholar] [CrossRef] [Green Version]
- Rial-Gonzalez, E.; Copsey, S.; Paoli, P.; Schneider, E. Priorities for Occupational Safety and Health Research in the EU-25; European Agency for Safety and Health at Work: Bilbao, Spain, 2005. [Google Scholar]
- Kompier, M.A. New systems of work organization and workers’ health. Scan. J. Work Environ. Health 2006, 32, 421–430. [Google Scholar] [CrossRef] [Green Version]
- Schill, A.L.; Chosewood, L.C. The NIOSH Total Worker Health ® program: An overview. J. Occup. Environ. Med. 2013, 55, S8–S11. [Google Scholar] [CrossRef]
- World Bank. World Development Report 2019: The Changing Nature of Work; World Bank: Washington, DC, USA, 2018. [Google Scholar] [CrossRef]
- Cappelli, P.H.; Keller, J.R. A Study of the Extant and Potential Causes of Alternative Employment Arrangements. Ind. Labor Relat. Rev. 2013, 66, 874–901. [Google Scholar] [CrossRef] [Green Version]
- Cummings, K.J.; Kreiss, K. Contingent workers and contingent health—Risks of a modern economy. JAMA 2008, 299, 448–450. [Google Scholar] [CrossRef]
- Ahonen, E.Q.; Fujishiro, A.; Cunningham, T.; Flynn, M. Work as an inclusive part of populations health inequities research and prevention. Am. J. Public Health 2018, 108, 306–311. [Google Scholar] [CrossRef]
- Dannenberg, A.L.; Frumkin, H.; Jackson, R.J. (Eds.) Making Healthy Places: Designing and Building for Health, Well-Being, and Sustainability; Island Press: Washington, DC, USA, 2001. [Google Scholar]
- Chen, P.Y.; Cooper, G.L. (Eds.) Work and well-being. In Well-Being: A Complete Reference Guide; John Wiley and Sons: West Sussex, UK, 2017; Volume 3. [Google Scholar]
- Schulte, P.A.; Guerin, R.J.; Schill, A.L.; Bhattacharya, A.; Cunningham, T.R.; Pandalai, S.P.; Eggerth, D.; Stephenson, C.M. Considerations for incorporating “Well-being” in public policy for workers and workplaces. Am. J. Public Health 2015, 105, e31–e44. [Google Scholar] [CrossRef]
- Chari, R.; Chang, C.C.; Sauter, S.L.; Sayers, E.L.P.; Cerully, J.L.; Schulte, P.; Schill, A.L.; Uscher-Pines, L. Expanding the paradigm of occupational safety and health. J. Occup. Environ. Med. 2018, 60, 589–593. [Google Scholar] [CrossRef] [PubMed]
- Moore, P.V. The Quantified Self in Precarity: Work, Technology and What Counts; Routledge: London, UK, 2018. [Google Scholar]
- Hudson, H.L.; Nigam, J.A.S.; Sauter, S.L.; Chosewood, L.C.; Schill, A.L.; Howard, J. (Eds.) Total Worker Health ®; American Psychological Association: Washington, DC, USA, 2019. [Google Scholar]
- Schulte, P.A.; Bhattacharya, A.; Butler, C.R.; Chun, H.K.; Jacklitsch, B.; Kiefer, M.; Lincoln, J.; Pendergrass, S.; Shire, J.; Watson, J.; et al. Advancing the framework for considering the effects of climate change on worker safety and health. J. Occup. Environ. Hyg. 2016, 13, 847–865. [Google Scholar] [CrossRef] [Green Version]
- Joint Action on Mental Health and Well-being: Mental Health at the Workplace. Available online: https://ec.europa.eu/health/sites/health/files/mental_health/docs/2017_mh_workplace_annex_en.pdf (accessed on 2 December 2019).
- Ministry of Social Affairs and Health. Policy for the Work Environment and Well-Being at Work 2020 Helsinki; Ministry of Social Affairs and Health: Helsinki, Finland, 2011.
- Eurofound. Sustainable Work throughout the Life Course: National Policies and Strategies; Publication of European Union: Luxembourg, 2016. [Google Scholar]
- Tamers, S.L.; Chosewood, L.C.; Childress, H.; Hudson, H.; Nigam, J.; Chang, C.C. Total Worker Health® 2014–2018: The novel approach to worker, safety, health and well-being evolves. Int. J. Environ. Res. Public Health 2019, 10, 321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, J.; Dawson, L. Occupational health: Meeting the challenges of the next 20 years. Saf. Health Work 2016, 7, 143–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulte, P.A. An expanded focus for occupational safety and health. In Proceedings of the 2nd International Symposium to Advance Total Worker Health® and Well-being, Bethesda, MD, USA, 10 May 2018. [Google Scholar]
- Delclos, G. Shaping the Future to Ensure Worker Health and Well-Being: Shifting Paradigm for Research, Training and Policy. Available online: http://grantome.com/grant/NIH/U13-OH011870-01 (accessed on 18 October 2019).
- Bureau of Labor Statistics. Employer-Reported Workplace Injuries and Illnesses, 2017. News Release, US DL-18-1788, 8 November 2018. Available online: https://www.bls.gov/news.release/pdf/osh.pdf (accessed on 7 December 2018).
- Pfeffer, J. The changing nature of work: Expanding the focus of occupation health, while not losing site of old problems. New Solut. 2019, 28, 731–736. [Google Scholar]
- Stacey, N.; Ellwood, P.; Bradbrook, S.; Reynolds, J.; Williams, H.; Lye, D. Foresight on New and Emerging Occupational Safety and Health Risks Associated with Digitalization by 2025; European Agency for Safety and Health at Work, Publications Office of the European Union: Luxembourg, 2018; Available online: https://osha.europa.eu/en/tools-and-publications/publications/foresight-new-and-emerging-occupational-safety-and-health-risks (accessed on 7 December 2018).
- Bureau of Labor Statistics. Contingent and Alternative Employment Arrangements Survey. 2017. Available online: https://www.bls.gov/news.release/conemp.nr0.htm (accessed on 6 December 2018).
- Serra Saurina, L.; Lopez Gomez, M.A.; Sanchez-Niubio, A.; Delclos, G.L.; Benavides, F.G. Applications of latent growth modeling to identify different working life trajectories: The case of the Spanish WORKs cohort. Scand. J. Work Environ. Health 2017, 43, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Sirviö, A.; Ek, E.; Jokelainen, J.; Koiranen, M.; Jarvikoski, T.; Taanila, A. Precariousness and discontinuous work history in association with health. Scand. J. Public Health 2012, 40, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Friedland, D.S.; Price, R.H. Underemployment: Consequences for the health and well-being of workers. Am. J. Community Psychol. 2003, 32, 33–45. [Google Scholar] [CrossRef]
- Bambra, C. Work, Worklessness, and the Political Economy of Health; Oxford University Press: New York, NY, USA, 2011. [Google Scholar]
- Badri, A.; Boudreau-Trudel, B.; Souissi, A.S. Occupational health and safety in the industry 4.0 era: A cause for major concern? Saf. Sci. 2018, 109, 403–411. [Google Scholar] [CrossRef]
- Leso, V.; Fontana, L.; Iavicoli, I. The occupational health and safety dimension of industry 4.0. Med. Lav. 2018, 109, 327–338. [Google Scholar]
- Marchant, G.E.; Stevens, Y.A.; Hennessy, J.M. Technology, unemployment and policy options: Navigating the transition to a better world. J. Evol. Technol. 2019, 24, 26–44. [Google Scholar]
- Jain, A.; Leka, S.; Zwetsloot, G.I.J.M. Managing Health Safety and Well-Being. Ethics, Responsibility and Sustainability; Springer: Heidelburg, Germany, 2018. [Google Scholar]
- McKinsey Global Inst. Jobs Lost, Jobs Gained: Workforce Transitions in a Time of Automation, 5 McKinsey & Co., Dec 2017. Available online: https://www.mckinsey.com/featured-insights/future-of-work/jobs-lost-jobs-gained-what-the-future-of-work-will-mean-for-jobs-skills-and-wages (accessed on 2 December 2019).
- Acemoglu, D.; Restrepo, P. Artificial Intelligence and Work; NBER Working Paper No. 24196; National Bureau of Economic Research (NBER): Cambridge, MA, USA, 2018.
- Schwabb, K. The Fourth Industrial Revolution General; World Economic Forum: Cologne, Switzerland, 2016. [Google Scholar]
- Rönnblad, J.; Grönhold, E.; Jonsson, J.; Koryanyi, I.; Orellana, C.; Kreshpaj, B.; Chen, L.; Stockflet, L.; Bodin, T. Precarious employment and mental health; a systematic review and meta-analysis of longitudinal studies. Scand. J. Work Environ. Health 2019. [Google Scholar] [CrossRef] [PubMed]
- Idris, M.A.; Dollard, M.F.; Coward, J.; Docmann, C. Psychosocial safety climate: Conceptual distinctions and effect on demands and worker psychological health. Saf. Sci. 2012, 50, 19–28. [Google Scholar] [CrossRef]
- International Labour Organization. Decent work and digitalization in the chemical and pharmaceutical industries. Paper Presented at the Global Dialogue Forum on Challenges for Decent and Productive Work Arising from Digitalization in the Chemical and Pharmaceutical Industries, Geneva, Switzerland, 10–12 December 2018. [Google Scholar]
- Zwetsloot, G.I.J.M.; Van Scheppingen, A.R.; Dijkman, H.; Hendrics, J.; den Besen, H. The organizational benefits of investing in workplace health. Int. J. Workplace Health Manag. 2010, 3, 143–159. [Google Scholar] [CrossRef] [Green Version]
- Iavicoli, S.; Cesana, G.; Dollard, M.; Leka, S.; Sauter, S.L. Psychosocial factors and workers health and safety. BioMed Res. Int. 2015, 628749. [Google Scholar] [CrossRef] [PubMed]
- El Batawi, M.A. Work-related diseases. A new program of the World Health Organization. Scand. J. Work Environ. Health 1984, 10, 341–346. [Google Scholar] [CrossRef]
- Schulte, P.A.; Pana-Cryan, R.; Schnorr, T.M.; Guerin, R.J.; Felknor, S.A.; Wagner, G.R. An approach to assess the burden of work-related injury, disease and distress. Am. J. Public Health 2017, 107, 1051–1057. [Google Scholar] [CrossRef]
- Scanlon, K.; Lloyd, S.; Gray, G.; Francis, R.; LaRuma, P. An approach to integrating occupational safety and health into Life Cycle Assessment. Development and application of work environment characterization factors. J. Ind. Ecol. 2015, 19, 27–37. [Google Scholar] [CrossRef]
- Schulte, P.A. Occupational Safety and Health in the 21st Century: What Lies Ahead. In Proceedings of the Symposium on Occupational Safety and Health: Recognizing Accomplishments and Planning for the Future, University of West Virginia, Morgantown, WV, USA, 10 August 2017. [Google Scholar]
- Samuels, S.W. Philosophic perspectives: Community, communication and occupational disease causation. Int. J. Health Serv. 1998, 28, 153–164. [Google Scholar] [CrossRef]
- Schulte, P.A.; Pandalai, S.; Wulsin, V.; Chun, H.K. Interaction of occupational and personal risk factors in workforce health and safety. Am. J. Public Health 2012, 102, 434–448. [Google Scholar] [CrossRef]
- Anttonen, H.; Räsänen, T. (Eds.) Well-Being at Work: New Innovations and Good Practices; Finish Inst of Occupational Health: Helsinki, Finland, 2008; Available online: https://eurofound.europa.eu/publications/article/2011/well-being-at-work-innovation (accessed on 2 December 2019).
- Pandalai, S.P.; Schulte, P.A.; Miller, D.B. Conceptual heuristic models of the interrelationships between obesity and the occupational environmental. Scand. J. Work Environ. Health 2013, 39, 221–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalski-McGraw, M.; Green-McKenzie, J.; Pandalai, S.P.; Schulte, P.A. Characterizing the relationships of prescription opioid and benzodiazepine medications and worker health and workplace hazards. J. Occup. Environ. Med. 2017, 59, 1114–1126. [Google Scholar] [CrossRef] [PubMed]
- Dembe, A.E. The social consequences of occupational injuries and illnesses. Am. J. Ind. Med. 2001, 40, 43–417. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Tsai, J.; Kao, S. Public health, social determinants and public policy. J. Med. Sci. 2009, 29, 43–59. [Google Scholar]
- Braverman, P.; Ergerter, S.; Williams, D.R. The social determinants of health: Coming of age. Annu. Rev. Public Health 2011, 32, 381–398. [Google Scholar] [CrossRef] [Green Version]
- Garcia, A.M.; Benavides, F.G. Determinants of workplace occupational safety and health practice in Spain. Policy Pract. Health Saf. 2014, 12, 67–87. [Google Scholar] [CrossRef]
- Navarro, V.; Muntaner, C. Political and Economic Determinants of Population Health and Well-Being: Controversies and Developments; Baywood Publishing Co Inc.: Amityville, NY, USA, 2004; p. 575. [Google Scholar]
- Walters, D.; Wadsworth, E.; Quinlan, M. Analysis of Determinants of Workplace Occupational Safety and Health Practice in a Selection of EU Member States; European Agency for Safety and Health at Work: Bilbao, Spain, 2013. [Google Scholar]
- Amick, B.C.; McLeod, C.B.; Bültmann, U. Labor markets and health: An integrated life course perspective. Scand. J. Work Environ. Health 2016, 42, 346–353. [Google Scholar] [CrossRef]
- Felstead, A.; Gallie, D.; Green, F.; Henseke, G. The determinants of skills use and work pressure: A longitudinal analysis. Econ. Ind. Democr. 2019, 40, 730–754. [Google Scholar] [CrossRef] [Green Version]
- Dooley, D. Unemployment, underemployment, and mental health: Conceptualizing employment status as a continuum. Am. J. Community Psychol. 2003, 32, 9–20. [Google Scholar] [CrossRef]
- Janlert, U. Underemployment as disease and diseases of the unemployed. Scand. J. Work Environ. Health 1997, 23, 79–83. [Google Scholar]
- Rappaport, S.M. Implications of exposome for exposure science. J. Expo. Sci. Environ. Epidemiol. 2011, 21, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Faislander, L.; Bonneterre, V.; De Gaudemaris, R.; Bicout, D.J. Occupational exposome: A network-basedapproach for characterizing Occupational Health Problems. J. Biomed. Inform. 2011, 44, 545–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lentz, T.J.; Dotson, G.S.; Williams, P.R.D.; Maier, H.; Gadagbui, B.; Pandalai, S.P.; Lamboy, H.; Hearl, F.; Mumtaz, M. Aggregate exposure and cumulative risk-integrating occupational and non-occupational risk factors. J. Occup. Environ. Hyg. 2015, 12, S112–S126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allin, P. Measuring well-being in modern societies. In Work and Well-Being. Well-Being a Complete Reference Guide; Chen, P.Y., Gooper, G.L., Eds.; John Wiley and Sons: West Sussex, UK, 2017; Volume 3. [Google Scholar]
- National Institute of Occupational Safety and Health (NIOSH). National Occupational Research Agenda (NORA)/National Total Worker Health ® Agenda (2016–2026): A National Agenda to Advance Total Worker Health® Research, Practice, Policy, and Capacity; DHHS (NIOSH) Publication 2016-114; Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health: Cincinnati, OH, USA, 2016.
- Peters, D.H. The application of systems thinking in health: Why use systems thinking? Health Res. Policy Syst. 2014, 12, 51. [Google Scholar] [CrossRef] [Green Version]
- Foldspang, A.; Birt, C.A.; Otok, R. ASPHER’s European List of Core Competences for the Public Health Professional, 5th ed.; Association of Schools of Public Health in the European Region (ASPHER): Brussels, Belgium, 2018. [Google Scholar]
- Council on Education for Public Health. Accreditation Criteria Schools of Public Health Public Health Programs; Council on Education for Public Health: Silver Spring, MD, USA, 2016; Available online: https://ceph.org/about/org-info/criteria-procedures-documents/criteria-procedures (accessed on 7 December 2018).
- DeSalvo, K.B.; Wang, Y.C.; Harris, A.; Auerbach, J.; Koo, D.; O’Carroll, P. Public Health 3.0: A call to act for public health to meet the challenges of the 21 Century. Prev. Chronic Dis. 2017, 14, E78. [Google Scholar] [CrossRef] [Green Version]
- Hale, A. Occupational Safety and Health (OSH) Professions: Who Are They and Why Do We Need Them? Available online: https://www.ilo.org/global/topics/safety-and-health-at-work/events-training/events-meetings/world-day-for-safety/33thinkpieces/WCMS_678734/lang--en/index.htm (accessed on 2 December 2019).
- Warr, P. Well-being and the workplace. In Well-Being: Foundations of Hedonic Psychology; Kahneman, D., Diener, E., Schwartz, N., Eds.; Russell Sage Foundation: New York, NY, USA, 1999; pp. 392–412. [Google Scholar]
- Schulte, P.; Vainio, H. Well-being at work—Overview and perspective. Scand. J. Work Environ. Health 2010, 36, 422–429. [Google Scholar] [CrossRef] [Green Version]
- Illarinen, J.; Tuomi, K.; Seitsamo, J. New Dimensions in Work Ability, Health and Well-Being of Ageing Workers; Elsevier: Amsterdam, The Netherlands, 2005; pp. 3–7. [Google Scholar]
- Oeij, P.R.A.; Rus, D.; Pot, F.D. (Eds.) Workplace Innovation: Theory Research and Practice; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Stroh, D.P. Systems Thinking in Social Change; Chelsea Green Publishing: White River Junction, VT, USA, 2015. [Google Scholar]
- Leischow, S.J.; Bost, A.; Trochin, W.M.; Clark, P.I.; Gallagher, R.S.; Marcus, S.E.; Matthews, E. Systems thinking to improve the public’s health. Am. J. Prev. Med. 2008, 35, S196–S203. [Google Scholar] [CrossRef] [Green Version]
- Best, A.; Moor, G.; Holmes, B.; Clark, P.I.; Bruce, T.; Leischow, S.; Krajnak, J. Health promotion dissemination and systems thinking: Towards an integrative model. Am. J. Health Behav. 2003, 27, 5206–5216. [Google Scholar] [CrossRef]
- Dammann, O.; Smart, R. Causation in Population Health Informatics and Data Science; Springer Nature: Cham, Switzerland, 2019. [Google Scholar]
- Stokols, D.; Hall, L.; Taylor, B.K.; Moser, R.P. The science of team science: Overview of the field and introduction to the supplement. Am. J. Prev. Med. 2008, 25, 579–589. [Google Scholar]
- Susskind, R.; Susskind, P. The Future of the Professions; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Meltzer, T. Robot Doctors, Online Lawyers and Automated Architects: The Future of the Professions? Available online: https://www.theguardian.com/technology/2014/jun/15/robot-doctors-online-lawyers-automated-architects-future-professions-jobs-technology (accessed on 2 December 2019).
- Brownson, R.C.; Samet, J.M.; Chavez, G.F.; Davies, M.M.; Galea, S.; Hiah, R.A.; Hernung, C.A.; Khoury, M.J.; Kov, P.; Mays, V.M.; et al. Characteristics a future for epidemiologic training. Ann. Epidemiol. 2015, 25, 458–465. [Google Scholar] [CrossRef] [Green Version]
- Senge, P. The Fifth Discipline: The Art and Practice of the Learning Organization; Doubleday/Currency: New York, NY, USA, 2006. [Google Scholar]
- International Labour Office. Safety and Health at the Heart of the Future of Work; International Labour Office: Geneva, Switzerland, 2019. [Google Scholar]
- Rosenfeld, P.L. The potential of transdisciplinary research for sustaining and extending linkage between the health and social sciences. Soc. Sci. Med. 1992, 35, 1343–1357. [Google Scholar] [CrossRef]
- Sorensen, G.; McLellan, D.L.; Sabbath, E.L.; Dennerlein, J.T.; Nagler, E.M.; Hurtado, D.A.; Pronk, N.P.; Wagner, G.R. Integrating worksite health protection and health promotion a conceptual model for intervention and research. Prev. Med. 2016, 9, 188–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sauter, S.L. Integrative approaches to safeguarding the health and safety of workers. Ind. Health. 2013, 51, 559–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillemin, M. Lesser Known Aspects of Occupational Health; L’Harmattan: Paris, France, 2011. (In French) [Google Scholar]
- Birkner, L.R.; McIntyre-Birkner, R.K. Anticpating and evaluating trends influencing occupational hygiene. In The Occupational Environment—Its Evaluation and Control; DiNardi, S.R., Ed.; AIHA Progs: Fairfax, VA, USA, 1977; pp. 1253–1262. [Google Scholar]
- Smith, S. The Federal Budget: What it Could Mean for Occupational Safety, Health and the Environment. EHS Today. Available online: https://www.ehstoday.com/training/federal-budget-what-it-could-mean-occupational-safety-health-and-environment (accessed on 28 November 2019).
- Dingwall, R.; Frost, S. (Eds.) Health and Safety in a Changing World; Routledge: London, UK, 2016. [Google Scholar]
- APPG. All-Party Parliamentary Group on Occupational Safety and Health. Available online: http://www.ucu.org.uk/.../pdf/hsecuts_allpartygroupreport.pdf (accessed on 2 December 2019).
- Spieler, E.A.; Wagner, G.R. Counting matters: Implications of undercounting in BLS survey of occupational injuries and illness. Am. J. Ind. Med. 2014, 57, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Rosenman, K.D.; Kalush, A.; Reilly, M.J.; Gardiner, J.C.; Reeves, M.; Luo, Z. How much work-related injury and illness is missed by the current national surveillance system? J. Occup. Environ. Med. 2006, 48, 357–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulte, P.A.; Grosch, J.; Scholl, J.C.; Tamers, S.L. Framework for considering productive aging at work. J. Occup. Environ. Med. 2018, 60, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Dobbs, R.; Manyika, J.; Woetzel, J. No Ordinary Disruption: The Four Global Forces Breaking All the Trends; Public Affairs, PBG Publishing, LLC: New York, NY, USA, 2015. [Google Scholar]
- Adler, S.; Lagakos, D.; Ohanian, L. Competitive Pressure and the Decline of the Rust Belt: A Macroeconomic Analysis; NBER Working Paper Series No. 20538; NBER: Cambridge, MA, USA, 2014. [Google Scholar]
- Project Working Group. Planning for the Future: Delivering a Vision of Occupational Health and Its Workforce for the UK for the Next 20 Years; The Council for Work Health: London, UK, 2014. [Google Scholar]
- Lax, M.B. The perils of integration wellness and safety and health. New Solut. 2016, 26, 11–39. [Google Scholar] [CrossRef]
- Howard, J.; Chosewood, L.C.; Hudson, H.L. The perils of integrating wellness and safety and health and the possibility of a worker oriented alterative letter to the editor. New Solut. 2016, 26, 345–348. [Google Scholar] [CrossRef]
- Anger, W.K.; Elliot, D.L.; Bodner, T.; Olson, R.; Rohlman, D.S.; Truxillo, D.M.; Montgomery, D.; Kuehl, K.S.; Hammer, L.B. Effectiveness of Total Worker Health Interventions. J. Occup Health Psychol. 2015, 20, 226–247. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Activity/Output Goals |
|---|
| 4.1.1: Survey key stakeholders to identify TWH training needs for existing and future workplace and allied professionals (that is, occupational safety and health, worksite health promotion, human resources, business, academic, policy, and other occupational and health professionals). |
| 4.1.2: Identify existing educational programs and curricula where TWH education is currently offered and where TWH principles can be incorporated. |
| 4.1.3: Assess the need for creating specialized TWH degrees, certificates, and continuing education programs. |
| 4.1.4: Develop standard TWH core competencies to be used across programs. |
| 4.1.5: Develop guidance in consultation with educators and academic professional societies and organizations for incorporating TWH core competencies into the curricula of existing and new degree, certificate, and continuing education programs. |
| 4.1.6: Offer TWH seminars, workshops, and courses for undergraduate and graduate students, across various disciplines, e.g., Occupational Health, Public Health, Health Promotion, Health Sciences, Psychology and other Social Sciences, Business, Human Relations, and Engineering. |
| 4.1.7: Evaluate mechanisms by which federal, state, and local agencies can support and fund TWH educational activities. |
| 4.1.8: Publish accessible works in theory, research, and practice on integrative prevention strategies for worker safety, health, and well-being to train both existing and new TWH professionals. |
| 4.2.3: Create a TWH professional organization or align with an existing professional organization to develop standards accreditation, and evaluation guidelines for TWH professionals to enhance their development and build capacity. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulte, P.A.; Delclos, G.; Felknor, S.A.; Chosewood, L.C. Toward an Expanded Focus for Occupational Safety and Health: A Commentary. Int. J. Environ. Res. Public Health 2019, 16, 4946. https://doi.org/10.3390/ijerph16244946
Schulte PA, Delclos G, Felknor SA, Chosewood LC. Toward an Expanded Focus for Occupational Safety and Health: A Commentary. International Journal of Environmental Research and Public Health. 2019; 16(24):4946. https://doi.org/10.3390/ijerph16244946
Chicago/Turabian StyleSchulte, Paul A., George Delclos, Sarah A. Felknor, and L. Casey Chosewood. 2019. "Toward an Expanded Focus for Occupational Safety and Health: A Commentary" International Journal of Environmental Research and Public Health 16, no. 24: 4946. https://doi.org/10.3390/ijerph16244946
APA StyleSchulte, P. A., Delclos, G., Felknor, S. A., & Chosewood, L. C. (2019). Toward an Expanded Focus for Occupational Safety and Health: A Commentary. International Journal of Environmental Research and Public Health, 16(24), 4946. https://doi.org/10.3390/ijerph16244946