Geographical Differences and the National Meeting Effect in Patients with Out-of-Hospital Cardiac Arrests: A JCS–ReSS Study Report

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Sources
2.2. EMS System in Japan
2.3. Choice of Hospital and Post-Arrest Care after OHCA
2.4. Data Collection and Quality Control
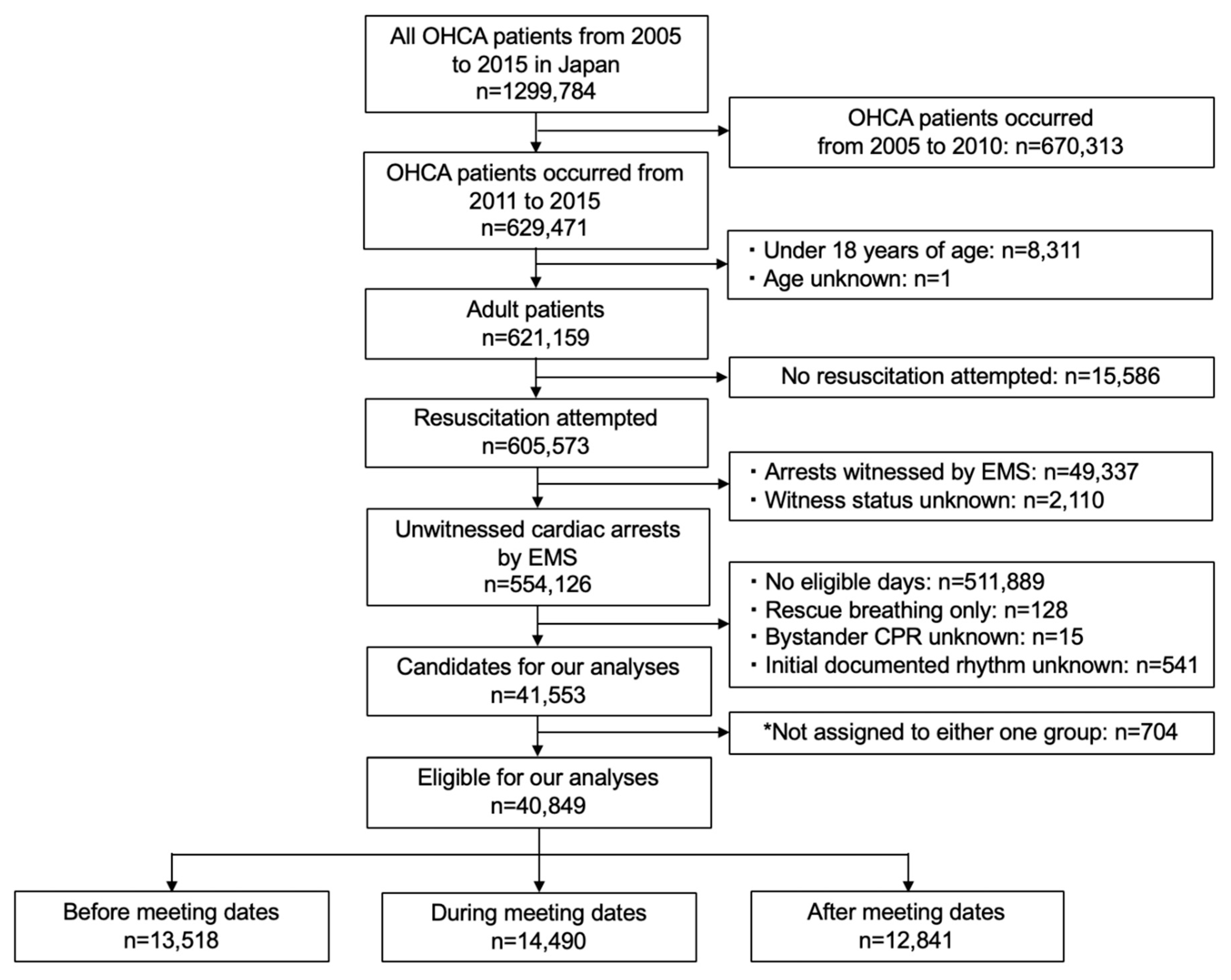
2.5. Study Sample
2.6. Outcome Measures
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Comparison of Outcomes between the Three Groups
3.3. Subgroup Analysis
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Berdowski, J.; Berg, R.A.; Tijssen, J.G.; Koster, R.W. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies. Resuscitation 2010, 81, 1479–1487. [Google Scholar] [CrossRef] [PubMed]
- Ambulance Service Planning Office of Fire and Disaster Management Agency of Japan. Effect of First Aid for Cardiopulmonary Arrest. 2018. Available online: http://www.fdma.go.jp/neuter/topics/kyukyukyujo_genkyo/h30/01_kyukyu.pdf (accessed on 15 November 2019).
- Kitamura, T.; Iwami, T.; Kawamura, T.; Nitta, M.; Nagao, K.; Nonogi, H.; Yonemoto, N.; Kimura, T.; Japanese Circulation Society Resuscitation Science Study Group. Nationwide improvements in survival from out-of-hospital cardiac arrest in Japan. Circulation 2012, 126, 2834–2843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassager, C.; Nagao, K.; Hildick-Smith, D. Out-of-hospital cardiac arrest: In-hospital intervention strategies. Lancet 2018, 391, 989–998. [Google Scholar] [CrossRef]
- Soar, J.; Donnino, M.W.; Maconochie, I.; Aickin, R.; Atkins, D.L.; Andersen, L.W.; Berg, K.M.; Bingham, R.; Böttiger, B.W.; Callaway, C.W.; et al. 2018 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations Summary. Circulation 2018, 138, e714–e730. [Google Scholar] [CrossRef] [Green Version]
- Koike, S.; Tanabe, S.; Ogawa, T.; Akahane, M.; Yasunaga, H.; Horiguchi, H.; Matsumoto, S.; Imamura, T. Effect of time and day of admission on 1-month survival and neurologically favourable 1-month survival in out-of-hospital cardiopulmonary arrest patients. Resuscitation 2011, 82, 863–868. [Google Scholar] [CrossRef]
- Matsumura, Y.; Nakada, T.A.; Shinozaki, K.; Tagami, T.; Nomura, T.; Tahara, Y.; Sakurai, A.; Yonemoto, N.; Nagao, K.; Yaguchi, A.; et al. Nighttime is associated with decreased survival and resuscitation efforts for out-of-hospital cardiac arrests: A prospective observational study. Crit. Care 2016, 20, 141. [Google Scholar] [CrossRef] [Green Version]
- Sorita, A.; Ahmed, A.; Starr, S.R.; Thompson, K.M.; Reed, D.A.; Prokop, L.; Shah, N.D.; Murad, M.H.; Ting, H.H. Off-hour presentation and outcomes in patients with acute myocardial infarction: Systematic review and meta-analysis. BMJ 2014, 348, f7393. [Google Scholar] [CrossRef] [Green Version]
- Galloway, M.; Hegarty, A.; McGill, S.; Arulkumaran, N.; Brett, S.J.; Harrison, D. The Effect of ICU Out-of-Hours Admission on Mortality: A Systematic Review and Meta-Analysis. Crit. Care Med. 2018, 46, 290–299. [Google Scholar] [CrossRef]
- Jena, A.B.; Prasad, V.; Goldman, D.P.; Romley, J. Mortality and treatment patterns among patients hospitalized with acute cardiovascular conditions during dates of national cardiology meetings. JAMA Intern. Med. 2015, 175, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Kitamura, T.; Kiyohara, K.; Matsuyama, T.; Hatakeyama, T.; Shimamoto, T.; Izawa, J.; Nishiyama, C.; Iwami, T. Is Survival After Out-of-Hospital Cardiac Arrests Worse During Days of National Academic Meetings in Japan? A Population-Based Study. J. Epidemiol. 2016, 26, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Jena, A.B.; Olenski, A.; Blumenthal, D.M.; Yeh, R.W.; Goldman, D.P.; Romley, J. Acute Myocardial Infarction Mortality During Dates of National Interventional Cardiology Meetings. J. Am. Heart Assoc. 2018, 7, e008230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasegawa, K.; Tsugawa, Y.; Camargo, C.A., Jr.; Hiraide, A.; Brown, D.F. Regional variability in survival outcomes of out-of-hospital cardiac arrest: The All-Japan Utstein Registry. Resuscitation 2013, 84, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- Okubo, M.; Gibo, K.; Wallace, D.J.; Komukai, S.; Izawa, J.; Kiyohara, K.; Callaway, C.W.; Iwami, T.; Kitamura, T. Regional variation in functional outcome after out-of-hospital cardiac arrest across 47 prefectures in Japan. Resuscitation 2018, 124, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, I.; Nadkarni, V.; Bahr, J.; Berg, R.A.; Billi, J.E.; Bossaert, L.; Cassan, P.; Coovadia, A.; D’Este, K.; Finn, J. Cardiac arrest and cardiopulmonary resuscitation outcome reports: Update and simplification of the Utstein templates for resuscitation registries: A statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Councils of Southern Africa). Circulation 2004, 110, 3385–3397. [Google Scholar] [CrossRef] [PubMed]
- Kitamura, T.; Iwami, T.; Kawamura, T.; Nagao, K.; Tanaka, H.; Hiraide, A.; Implementation Working Group for the All-Japan Utstein Registry of the Fire and Disaster Management Agency. Nationwide public-access defibrillation in Japan. N. Engl. J. Med. 2010, 362, 994–1004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Internal Affairs and Communications. Japanese Population Census in 2015. Available online: https://www.stat.go.jp/data/kokusei/2015/kekka/kihon1/pdf/youyaku.pdf (accessed on 15 November 2019).
- Ministry of Internal Affairs and Communications. Promotion of Geographical Expansion of Fire-Fighting and Emergency Medical Services. Available online: http://www.soumu.go.jp/main_content/000427864.pdf (accessed on 15 November 2019).
- Hazinski, M.F.; Nolan, J.P.; Billi, J.E.; Böttiger, B.W.; Bossaert, L.; de Caen, A.R.; Deakin, C.D.; Drajer, S.; Eigel, B.; Hickey, R.W.; et al. Part 1: Executive summary: 2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation 2010, 122, S250–S275. [Google Scholar] [CrossRef] [Green Version]
- Mizuno, S.; Kunisawa, S.; Sasaki, N.; Fushimi, K.; Imanaka, Y. In-hospital mortality and treatment patterns in acute myocardial infarction patients admitted during national cardiology meeting dates. Int. J. Cardiol. 2016, 220, 929–936. [Google Scholar] [CrossRef]
- Abdelwahab Elhamahmi, D.; Chaly, T., Jr.; Wei, G.; Hall, I.E. Kidney Discard Rates in the United States during American Transplant Congress Meetings. Transpl. Direct 2018, 5, e412. [Google Scholar] [CrossRef]
- Linderoth, G.; Hallas, P.; Lippert, F.K.; Wibrandt, I.; Loumann, S.; Møller, T.P.; Østergaard, D. Challenges in out-of-hospital cardiac arrest—A study combining closed-circuit television (CCTV) and medical emergency calls. Resuscitation 2015, 96, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Nallamothu, B.K.; Guetterman, T.C.; Harrod, M.; Kellenberg, J.E.; Lehrich, J.L.; Kronick, S.L.; Krein, S.L.; Iwashyna, T.J.; Saint, S.; Chan, P.S. How Do Resuscitation Teams at Top-Performing Hospitals for In-Hospital Cardiac Arrest Succeed? A Qualitative Study. Circulation 2018, 138, 154–163. [Google Scholar] [CrossRef]
- Yumoto, T.; Naito, H.; Ihoriya, H.; Yorifuji, T.; Nakao, A. Mortality in trauma patients admitted during, before, and after national academic emergency medicine and trauma surgery meeting dates in Japan. PLoS ONE 2019, 14, e0207049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortega-Deballon, I.; Hornby, L.; Shemie, S.D.; Bhanji, F.; Guadagno, E. Extracorporeal resuscitation for refractory out-of-hospital cardiac arrest in adults: A systematic review of international practices and outcomes. Resuscitation 2016, 101, 12–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jentzer, J.C.; Scutella, M.; Pike, F.; Fitzgibbon, J.; Krehel, N.M.; Kowalski, L.; Callaway, C.W.; Rittenberger, J.C.; Reynolds, J.C.; Barsness, G.W.; et al. Early coronary angiography and percutaneous coronary intervention are associated with improved outcomes after out of hospital cardiac arrest. Resuscitation 2018, 123, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Schenone, A.L.; Cohen, A.; Patarroyo, G.; Harper, L.; Wang, X.; Shishehbor, M.H.; Menon, V.; Duggal, A. Therapeutic hypothermia after cardiac arrest: A systematic review/meta-analysis exploring the impact of expanded criteria and targeted temperature. Resuscitation 2016, 108, 102–110. [Google Scholar] [CrossRef]
- Lee, D.H.; Cho, I.S.; Lee, S.H.; Min, Y.I.; Min, J.H.; Kim, S.H.; Lee, Y.H.; Korean Hypothermia Network Investigators. Correlation between initial serum levels of lactate after return of spontaneous circulation and survival and neurological outcomes in patients who undergo therapeutic hypothermia after cardiac arrest. Resuscitation 2015, 88, 143–149. [Google Scholar] [CrossRef]
- Oddo, M.; Sandroni, C.; Citerio, G.; Miroz, J.P.; Horn, J.; Rundgren, M.; Cariou, A.; Payen, J.F.; Storm, C.; Stammet, P.; et al. Quantitative versus standard pupillary light reflex for early prognostication in comatose cardiac arrest patients: An international prospective multicenter double-blinded study. Intensive Care Med. 2018, 44, 2102–2111. [Google Scholar] [CrossRef] [Green Version]
- Sugiyama, K.; Miyazaki, K.; Ishida, T.; Tanabe, T.; Hamabe, Y. Categorization of post-cardiac arrest patients according to the pattern of amplitude-integrated electroencephalography after return of spontaneous circulation. Crit. Care 2018, 22, 226. [Google Scholar] [CrossRef] [Green Version]
- Caro-Codón, J.; Rey, J.R.; Lopez-de-Sa, E.; González Fernández, Ó.; Rosillo, S.O.; Armada, E.; Iniesta, Á.M.; Fernández de Bobadilla, J.; Ruiz Cantador, J.; Rodríguez Sotelo, L.; et al. Long-term neurological outcomes in out-of-hospital cardiac arrest patients treated with targeted-temperature management. Resuscitation 2018, 133, 33–39. [Google Scholar] [CrossRef]
- Kajino, K.; Iwami, T.; Daya, M.; Nishiuchi, T.; Hayashi, Y.; Kitamura, T.; Irisawa, T.; Sakai, T.; Kuwagata, Y.; Hiraide, A.; et al. Impact of transport to critical care medical centers on outcomes after out-of-hospital cardiac arrest. Resuscitation 2010, 81, 549–554. [Google Scholar] [CrossRef]


{kind=link}
| Before Meeting Dates Group n = 13,518 | During Meeting Dates Group n = 14,490 | After Meeting Dates Group n = 12,841 | p-Value | |
|---|---|---|---|---|
| Age (years), median (IQR) | 79 (68, 86) | 79 (68, 77) | 79 (67, 86) | 0.131 |
| 18–39 (years), n (%) | 478 (3.5) | 533 (3.7) | 472 (3.7) | 0.564 |
| 40–64 (years), n (%) | 2199 (16.3) | 2395 (16.5) | 2177 (17.0) | |
| ≥65 (years), n (%) | 10,841 (80.2) | 11,562 (79.8) | 10,192 (79.4) | |
| Male, n (%) | 7691 (56.9) | 8175 (56.4) | 7240 (56.4) | 0.638 |
| Type of bystander witness | ||||
| None, n (%) | 8807 (65.2) | 9475 (65.4) | 8288 (64.5) | 0.411 |
| Family member, n (%) | 2798 (20.7) | 3044 (21.0) | 2736 (21.3) | |
| Other, n (%) | 1913 (14.1) | 1971 (13.6) | 1817 (14.2) | |
| Type of bystander-initiated CPR | ||||
| None, n (%) | 6983 (51.7) | 7487 (51.7) | 6566 (51.1) | 0.825 |
| Chest compression-only CPR, n (%) | 5529 (40.9) | 5956 (41.1) | 5325 (41.5) | |
| Conventional CPR, n (%) | 1006 (7.4) | 1047 (7.2) | 950 (7.4) | |
| Initial documented rhythm | ||||
| VF/pVT, n (%) | 947 (7.0) | 1026 (7.1) | 998 (7.8) | 0.031 |
| PEA/Asystole, n (%) | 12,571 (93.0) | 13,464 (92.9) | 11,843 (92.2) | |
| Etiology | ||||
| Cardiac, n (%) | 8135 (60.2) | 8718 (60.2) | 7812 (60.8) | 0.444 |
| Other, n (%) | 5383 (39.8) | 5772 (39.8) | 5029 (39.2) | |
| Shocks by public access-AED use, n (%) | 142 (1.1) | 148 (1.0) | 151 (1.2) | 0.431 |
| Intravenous fluid, n (%) | 4344 (32.1) | 4687 (32.3) | 4119 (32.1) | 0.880 |
| Epinephrine administration, n (%) | 2193 (16.2) | 2275 (15.7) | 2058 (16.0) | 0.443 |
| Advanced airway management, n (%) | 7196 (53.2) | 7699 (53.1) | 6967 (54.3) | 0.128 |
| Time interval from call to hospital arrival (in one-minute increments), median (IQR) | 31 (26, 39) | 32 (26, 39) | 31 (26, 39) | 0.131 |
| Better outcome areas, n (%) | 6509 (48.2) | 6990 (48.2) | 6255 (48.7) | 0.620 |
| Worse outcome areas, n (%) | 7009 (51.8) | 7500 (51.8) | 6.586 (51.3) | |
| National academic meeting place | ||||
| Tokyo metropolitan area, n (%) | 7236 (53.5) | 7142 (49.3) | 6980 (54.4) | <0.001 |
| Other area, n (%) | 6282 (46.5) | 7348 (50.7) | 5861 (45.6) |
| Before-Meeting-Dates Group | During-Meeting-Dates Group | After-Meeting-Dates Group | |
|---|---|---|---|
| Favorable neurological outcome, % (n/N) | 1.6 (211/13,518) | 1.7 (243/14,490) | 1.8 (232/12,841) |
| Crude OR (95% CI) | 0.93 (0.77–1.11) | Reference | 0.87 (0.72–1.05) |
| Adjusted OR (95% CI) | 0.95 (0.78–1.15) | Reference | 1.06 (0.88–1.28) |
| One-month survival, % (n/N) | 3.8 (516/13,518) | 3.8 (555/14,490) | 3.8 (493/12,841) |
| Crude OR (95% CI) | 1.00 (0.88–1.13) | Reference | 0.99 (0.88–1.13) |
| Adjusted OR (95% CI) | 1.00 (0.88–1.14) | Reference | 0.98 (0.86–1.11) |
| Overall | ||||
| Meeting Location | Before-Meeting-Dates Group | During-Meeting-Dates Group | After-Meeting-Dates Group | |
| Favorable neurological outcome, % (n/N) | Overall | 1.6 (211/13,518) | 1.7 (243/14,490) | 1.8 (232/12,841) |
| Tokyo metropolitan area | 1.6 (112/7236) | 1.6 (115/7142) | 1.7 (121/6980) | |
| Others | 1.6 (99/6282) | 1.7 (128/7348) | 1.9 (111/5861) | |
| Adjusted OR for favorable neurological outcome | Overall | 0.95 (0.78–1.15) | Reference | 1.06 (0.88–1.28) |
| Tokyo metropolitan area | 1.05 (0.74–1.48) | Reference | 0.88 (0.62–1.25) | |
| Others | 0.97 (0.68–1.39) | Reference | 1.13 (0.80–1.60) | |
| Better Outcome Areas | ||||
| Meeting Location | Before-Meeting-Dates Group | During-Meeting-Dates Group | After-Meeting-Dates Group | |
| Favorable neurological outcome, % (n/N) | Overall | 2.0 (132/6509) | 2.1 (145/6990) | 2.1 (133/6255) |
| Tokyo metropolitan area | 2.1 (74/3491) | 2.0 (71/3512) | 2.0 (67/3392) | |
| Others | 1.9 (58/3018) | 2.1 (74/3478) | 2.3 (66/2863) | |
| Adjusted OR for favorable neurological outcome | Overall | 1.00 (0.78–1.28) | Reference | 1.01 (0.83–1.25) |
| Tokyo metropolitan area | 1.05 (0.74–1.48) | Reference | 0.88 (0.62–1.25) | |
| Others | 0.97 (0.68–1.39) | Reference | 1.13 (0.80–1.60) | |
| Worse Outcome Areas | ||||
| Meeting Location | Before-Meeting-Dates Group | During-Meeting-Dates Group | After-Meeting-Dates Group | |
| Favorable neurological outcome, % (n/N) | Overall | 1.1 (79/7009) | 1.3 (98/7500) | 1.5 (99/6586) |
| Tokyo metropolitan area | 1.0 (38/3745) | 1.2 (44/3630) | 1.5 (54/3588) | |
| Others | 1.3 (41/3264) | 1.4 (54/3870) | 1.5 (45/2998) | |
| Adjusted OR for favorable neurological outcome | Overall | 1.15 (0.86–1.55) | Reference | 0.93 (0.73–1.20) |
| Tokyo metropolitan area | 0.82 (0.52–1.29) | Reference | 1.25 (0.82–1.89) | |
| Others | 0.90 (0.59–1.37) | Reference | 1.07 (0.71–1.62) | |
| Before Meeting Dates Group | During Meeting Dates Group | After Meeting Dates Group | |
|---|---|---|---|
| ±2 a | |||
| Favorable neurological outcome, % (n/N) | 1.7 (223/12,948) | 1.7 (216/12,537) | 1.8 (226/12,366) |
| Adjusted OR (95% CI) | 0.91 (0.71–1.17) | Reference | 0.96 (0.75–1.23) |
| ±3 b | |||
| Favorable neurological outcome, % (n/N) | 1.5 (196/13,497) | 1.8 (219/12,429) | 1.8 (235/12,820) |
| Adjusted OR (95% CI) | 0.76 (0.60–0.96) | Reference | 0.97 (0.78–1.22) |
| ±4 c | |||
| Favorable neurological outcome, % (n/N) | 1.5 (193/13,106) | 1.7 (234/13,792) | 1.7 (203/12,111) |
| Adjusted OR (95% CI) | 1.01 (0.78–1.30) | Reference | 0.99 (0.88–1.12) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yumoto, T.; Naito, H.; Yorifuji, T.; Tahara, Y.; Yonemoto, N.; Nonogi, H.; Nagao, K.; Ikeda, T.; Sato, N.; Tsutsui, H., on behalf of the Japanese Circulation Society Resuscitation Science Study (JCS-ReSS) Group. Geographical Differences and the National Meeting Effect in Patients with Out-of-Hospital Cardiac Arrests: A JCS–ReSS Study Report. Int. J. Environ. Res. Public Health 2019, 16, 5130. https://doi.org/10.3390/ijerph16245130
Yumoto T, Naito H, Yorifuji T, Tahara Y, Yonemoto N, Nonogi H, Nagao K, Ikeda T, Sato N, Tsutsui H on behalf of the Japanese Circulation Society Resuscitation Science Study (JCS-ReSS) Group. Geographical Differences and the National Meeting Effect in Patients with Out-of-Hospital Cardiac Arrests: A JCS–ReSS Study Report. International Journal of Environmental Research and Public Health. 2019; 16(24):5130. https://doi.org/10.3390/ijerph16245130
Chicago/Turabian StyleYumoto, Tetsuya, Hiromichi Naito, Takashi Yorifuji, Yoshio Tahara, Naohiro Yonemoto, Hiroshi Nonogi, Ken Nagao, Takanori Ikeda, Naoki Sato, and Hiroyuki Tsutsui on behalf of the Japanese Circulation Society Resuscitation Science Study (JCS-ReSS) Group. 2019. "Geographical Differences and the National Meeting Effect in Patients with Out-of-Hospital Cardiac Arrests: A JCS–ReSS Study Report" International Journal of Environmental Research and Public Health 16, no. 24: 5130. https://doi.org/10.3390/ijerph16245130
APA StyleYumoto, T., Naito, H., Yorifuji, T., Tahara, Y., Yonemoto, N., Nonogi, H., Nagao, K., Ikeda, T., Sato, N., & Tsutsui, H., on behalf of the Japanese Circulation Society Resuscitation Science Study (JCS-ReSS) Group. (2019). Geographical Differences and the National Meeting Effect in Patients with Out-of-Hospital Cardiac Arrests: A JCS–ReSS Study Report. International Journal of Environmental Research and Public Health, 16(24), 5130. https://doi.org/10.3390/ijerph16245130