Virtual Reality Games as an Adjunct in Improving Upper Limb Function and General Health among Stroke Survivors

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
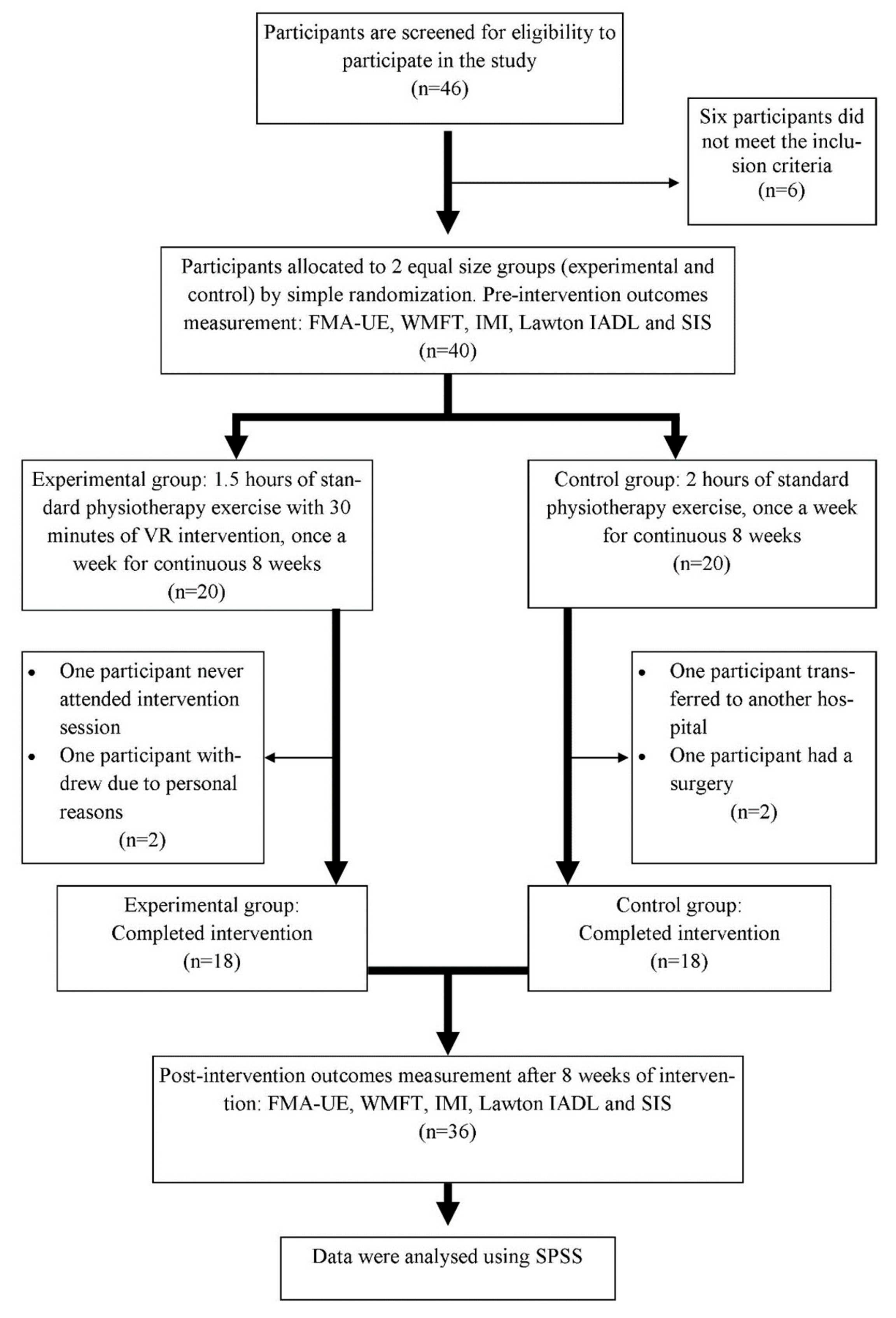
2.1. Participants
2.2. Procedures
2.3. Virtual Reality Games
2.4. Outcome Measures
2.5. Statistical Analysis
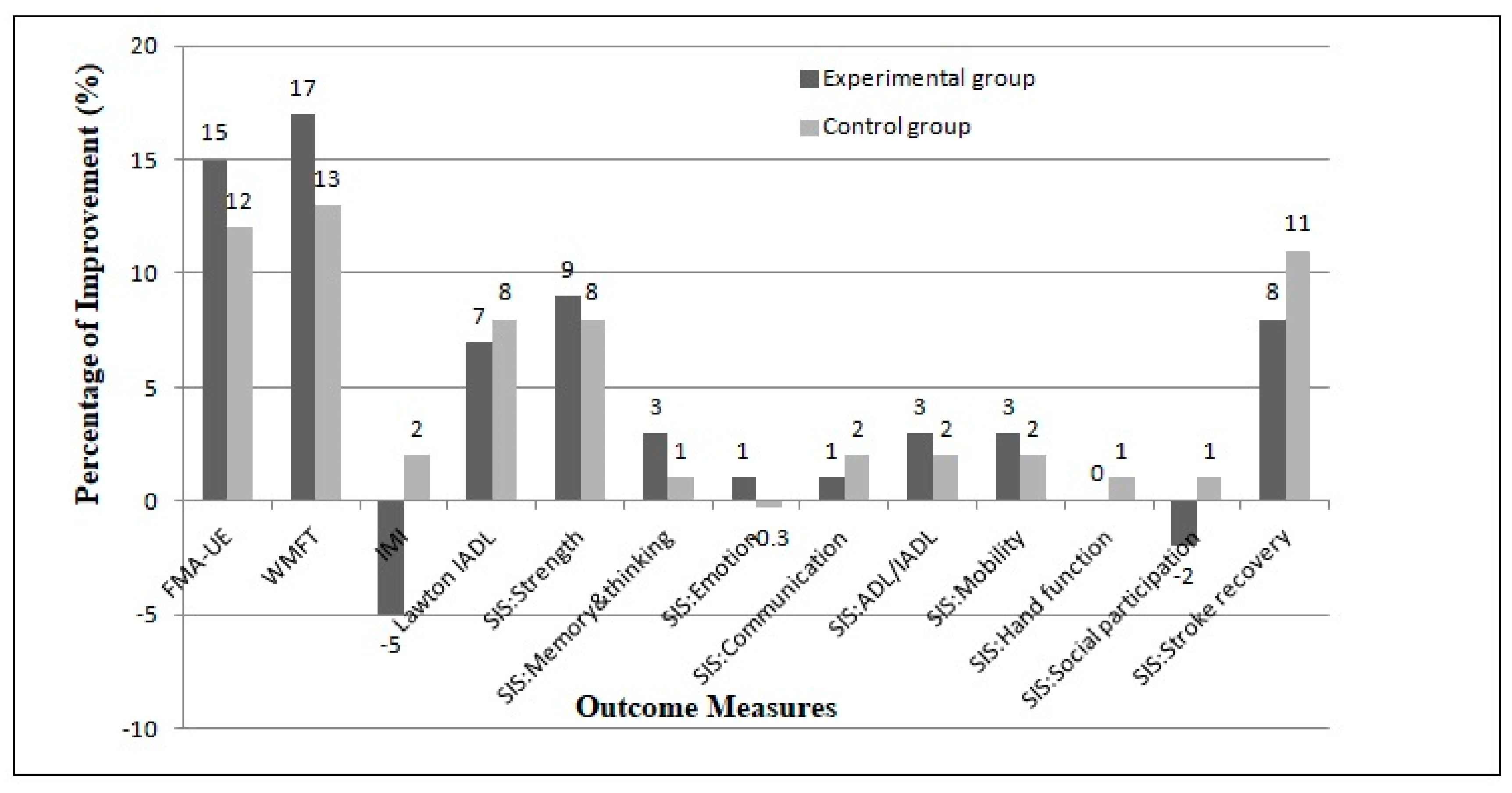
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global burden of stroke. Circ. Res. 2017, 3, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Ostwald, S.K.; Davis, S.; Hersch, G.; Kelley, C.; Godwin, K.M. Evidence-based educational guidelines for stroke survivors after discharge home. J. Neurosci. Nurs. 2008, 40, 173–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordin, N.A.M.; Aziz, N.A.; Aziz, A.F.A.; Singh, D.K.A.; Othman, N.A.O.; Sulong, S.; Aljinid, S.M. Exploring views on long term rehabilitation for people with stroke in a developing country: Findings from focus group discussions. BMC Health Serv. Res. 2014, 14, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, N.S.; Kelly, K.; Brander, F. The future of stroke rehabilitation: Upper limb recovery. Adv. Clin. Neurosci. Rehabil. 2015, 15, 6–9. [Google Scholar]
- Akinladejo, F.O. Virtual environments in physical therapy. In Virtual Reality and Environments, 1st ed.; Cecilia, S.L., Ed.; InTechOpen: London, UK, 2012; Volume 1, pp. 1–20. ISBN 978-953-51-0579-4. Available online: https://www.intechopen.com/books/virtual-reality-and-environments/virtual-environments-in-physical-therapy (accessed on 12 March 2019). [CrossRef] [Green Version]
- Sveistrup, H. Motor rehabilitation using virtual reality. J. Neuroeng. Rehabil. 2004, 1, 10–17. [Google Scholar] [CrossRef] [Green Version]
- International Society on Virtual Rehabilitation (ISVR). Virtual Reality Rehabilitation Newsletter 2014. Available online: http://isvr.org/news/isvr-newsletter/ (accessed on 15 July 2018).
- Cheiloudaki, E.; Alexopoulos, E.C. Adherence to Treatment in Stroke Patients. Int. J. Environ. Res. Public Health 2019, 16, 196. [Google Scholar] [CrossRef] [Green Version]
- Singh, D.K.A.; Nordin, N.A.; Abd-Aziz, N.A.; Lim, B.K.; Soh, L.C. Effects of substituting a portion of standard physiotherapy time with virtual reality games among community-dwelling stroke survivors. BMC Neurol. 2013, 13, 199–206. [Google Scholar] [CrossRef] [Green Version]
- Singh, D.K.A.; Rajaratnam, B.S.; Palaniswamy, V.; Raman, V.P.; Bong, P.S.; Pearson, H. Effects of balance-focused interactive games compared to therapeutic balance classes for older women. Climacteric 2013, 16, 141–147. [Google Scholar] [CrossRef]
- Singh, D.K.A.; Rajaratnam, B.S.; Palaniswamy, V.; Raman, V.P.; Bong, P.S.; Pearson, H. Participating in a virtual reality balance exercise program can reduce risk and fear of falls. Maturitas 2012, 73, 239–244. [Google Scholar] [CrossRef]
- Singh, D.K.A.; Ab-Rahman, N.N.A.; Rajiman, S.; Chang, S.Y.; Karim, Z.A.; Ruslan, A.S.; Rajwinder, K.H.S. Impact of virtual reality games on psychological well-being and upper limb performance in adults with physical disabilities: A pilot study. Med. J. Malays. 2017, 72, 119–122. [Google Scholar]
- Hale, L.A.; Satherley, J.A.; McMillan, N.J.; Milosavljevic, S.; Hijmans, J.M.; King, M.J. Participant perceptions of use of adapted CyWee Z as adjunct to rehabilitation of upper-limb function following stroke. J. Rehabil. Res. Dev. 2012, 49, 623–635. [Google Scholar] [CrossRef] [PubMed]
- Hijmans, J.M.; Leigh, A.H.; Jessica, A.S.; Nicole, J.M.; Marcus, J.K. Bilateral upper limb rehabilitation after stroke using a movement-based game controller. J. Rehabil. Res. Dev. 2011, 48, 1005–1015. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jaasko, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. A method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–22. [Google Scholar] [PubMed]
- Lin, J.H.; Hsueh, I.P. Psychometric properties of the sensory scale of the Fugl-Meyer Assessment in stroke patients. Clin. Rehabil. 2004, 18, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, K.J.; Tilson, J.K.; Steven, Y.C.; Rose, D.K.; Hershberg, J.; Correa, A.; Gallichio, J.; McLeod, M.; Moore, C.; Wu, S.S.; et al. Fugl-Meyer Assessment of sensor motor function after stroke: Standardized training procedure for clinical practice and clinical trials. J. Am. Heart Assoc. 2011, 42, 427–433. [Google Scholar]
- Wolf, S.L.; Catlin, P.A.; Ellis, M.; Archer, A.L.; Morgan, B.; Piacentino, A. Assessing Wolf Motor Function Test as outcome measure for research in patients after stroke. J. Am. Heart Assoc. 2001, 32, 1632–1639. [Google Scholar] [CrossRef] [Green Version]
- Nijland, R.; Van-Wegen, E.; Verbunt, J.; Van-Wijk, R.; Van-Kordelaar, J.; Kwakkel, G. A comparison of two validated tests for upper limb function after stroke: The Wolf Motor Function Test and the Action Research Arm Test. J. Rehabil. Med. 2010, 42, 694–697. [Google Scholar]
- Monteiro, V.; Mata, L.; Peixoto, F. Intrinsic Motivation Inventory: Psychometric properties in the context of first language and mathematics learning. Psicol. Reflex. Crit. 2015, 28, 434–444. [Google Scholar] [CrossRef] [Green Version]
- Eow, Y.L.; Wan-Zah, W.A.; Roselan, B.; Rosnaini, M. Stability of the Intrinsic Motivation Inventory (IMI) for the use of Malaysian form one students in ICT literacy class. Eurasia J. Math. Sci. Technol.Educ. 2010, 6, 215–227. [Google Scholar]
- Graf, C. The Lawton Instrumental Activities Daily Living scale. Am. J. Nurs. 2008, 108, 52–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muldera, M.; Nijland, R. Stroke Impact Scale. J. Physiother. 2016, 62, 117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saposnik, G.; Teasell, R.; Muhammad, M.; Hall, J.; McLlroy, W.; Cheung, D.; Thorpe, K.E.; Cohen, L.G.; Bayley, M. Effectiveness of virtual reality using Wii gaming technology in stroke rehabilitation: A pilot randomized clinical trial and proof of principle. J. Am. Heart Assoc. 2010, 41, 1477–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levin, M.F.; Osnat, S.; Dario, G.L.; Harold, W.; Patrice, L.W. Virtual reality versus conventional treatment of reaching ability in chronic stroke: Clinical feasibility study. Neurol. Ther. 2012, 1, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rand, D.; Weiss, P.L.; Katz, N. Training multitasking in a virtual supermarket: A novel intervention after stroke. Am. J. Occup. Ther. 2009, 63, 535–543. [Google Scholar] [CrossRef] [Green Version]
- Schuck, S.O.; Whetstone, A.; Hill, V.; Levine, P.; Page, S.J. Game-based, portable, upper extremity rehabilitation in chronic stroke. Top. Stroke Rehabil. 2011, 18, 720–728. [Google Scholar] [CrossRef]
- Cameirao, M.S.; Bermudez, I.B.S.; Duartec, E.; Verschure, P.F.M.J. Virtual reality based rehabilitation speeds up functional recovery of the upper extremities after stroke: A randomized controlled pilot study in the acute phase of stroke using the rehabilitation gaming system. Restor. Neurol. Neurosci. 2011, 29, 287–299. [Google Scholar]



{kind=link}
{kind=link}
| Variable | Experimental (n = 18) | Control (n = 18) | Analysis of Covariance |
|---|---|---|---|
| Mean (SD) | Mean (SD) | p-Values | |
| Gender (male/female) | 17/1 | 14/4 | |
| Age (years) | 57.00 (8.203) | 62.94 (10.54) | 0.07 |
| Post stroke duration (months) | 10.56 (5.26) | 10.72 (6.03) | 0.93 |
| Affected side (left/right) | 11/7 | 9/9 | 0.50 |
| Parameters | Study Group | Analysis of Covariance (p-Values) | |||
|---|---|---|---|---|---|
| Experimental Mean (SD) | Control Mean (SD) | Time (ηp2) | Group (ηp2) | Interaction (ηp2) | |
| FMA-UE | |||||
| Week 0 | 57.44 (10.17) | 56.50 (8.18) | 0.001 * (0.76) | 0.50 (0.01) | 0.23 (0.04) |
| Week 8 | 65.94 (7.57) | 63.22 (6.98) | |||
| WMFT | |||||
| Week 0 | 46.00 (10.99) | 44.11 (7.64) | 0.001 * (0.79) | 0.38 (0.02) | 0.17 (0.05) |
| Week 8 | 53.61 (10.35) | 50.05 (7.55) | |||
| IMI | |||||
| Week 0 | 126.94 (11.40) | 118.22 (8.35) | 0.16 (0.06) | 0.14 (0.06) | 0.001 * (0.20) |
| Week 8 | 120.50 (10.00) | 120.50 (8.37) | |||
| Lawton IADL | |||||
| Week 0 | 4.28 (2.22) | 2.78 (1.00) | 0.01 * (0.17) | 0.77 (0.00) | 0.01 * (0.19) |
| Week 8 | 4.56 (1.98) | 3.00 (1.03) | |||
| SIS domains | |||||
| Strength | 0.00 * (0.32) | 1.00 (0.00) | 0.16 (0.06) | ||
| Week 0 | 57.29 (15.93) | 63.54 (12.91) | |||
| Week 8 | 62.50 (11.94) | 68.75 (13.89) | |||
| Memory, thinking | 0.05 (0.11) | 0.34 (0.03) | 0.21 (0.05) | ||
| Week 0 | 87.91 (14.24) | 82.94 (11.39) | |||
| Week 8 | 90.96 (11.39) | 84.02 (15.32) | |||
| Emotion | 0.78 (0.00) | 0.57 (0.01) | 0.34 (0.30) | ||
| Week 0 | 83.97 (12.92) | 80.40 (13.46) | |||
| Week 8 | 84.79 (12.29) | 80.13 (13.37) | |||
| Communication | 0.13 (0.07) | 0.51 (0.01) | 0.03 * (0.13) | ||
| Week 0 | 94.84 (8.85) | 84.92 (17.70) | |||
| Week 8 | 95.64 (9.05) | 86.91 (14.13) | |||
| ADL/IADL | |||||
| Week 0 | 84.32 (12.05) | 77.41 (11.11) | 0.001 * (0.24) | 0.67 (0.00) | 0.06 (0.10) |
| Week 8 | 86.68 (10.31) | 79.23 (11.11) | |||
| Mobility | |||||
| Week 0 | 85.34 (10.52) | 80.86 (15.06) | 0.06 (0.10) | 0.82 (0.00) | 0.25 (0.04) |
| Week 8 | 87.50 (6.95) | 82.56 (15.12) | |||
| Hand function | |||||
| Week 0 | 68.61 (27.64) | 66.11 (22.59) | 0.77 (0.00) | 0.77 (0.00) | 0.79 (0.00) |
| Week 8 | 68.61 (27.80) | 66.67 (22.10) | |||
| Social | |||||
| Week 0 | 74.31 (16.31) | 68.58 (18.44) | 0.74 (0.00) | 0.19 (0.05) | 0.45 (0.02) |
| Week 8 | 72.63 (17.95) | 69.59 (16.47) | |||
| Stroke recovery | |||||
| Week 0 | 68.61 (12.70) | 61.67 (9.85) | 0.001 * (0.56) | 0.45 (0.02) | 0.09 (0.08) |
| Week 8 | 73.89 (10.37) | 68.33 (11.38) | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmad, M.A.; Singh, D.K.A.; Mohd Nordin, N.A.; Hooi Nee, K.; Ibrahim, N. Virtual Reality Games as an Adjunct in Improving Upper Limb Function and General Health among Stroke Survivors. Int. J. Environ. Res. Public Health 2019, 16, 5144. https://doi.org/10.3390/ijerph16245144
Ahmad MA, Singh DKA, Mohd Nordin NA, Hooi Nee K, Ibrahim N. Virtual Reality Games as an Adjunct in Improving Upper Limb Function and General Health among Stroke Survivors. International Journal of Environmental Research and Public Health. 2019; 16(24):5144. https://doi.org/10.3390/ijerph16245144
Chicago/Turabian StyleAhmad, Mohd Azzuan, Devinder Kaur Ajit Singh, Nor Azlin Mohd Nordin, Khor Hooi Nee, and Norliza Ibrahim. 2019. "Virtual Reality Games as an Adjunct in Improving Upper Limb Function and General Health among Stroke Survivors" International Journal of Environmental Research and Public Health 16, no. 24: 5144. https://doi.org/10.3390/ijerph16245144
APA StyleAhmad, M. A., Singh, D. K. A., Mohd Nordin, N. A., Hooi Nee, K., & Ibrahim, N. (2019). Virtual Reality Games as an Adjunct in Improving Upper Limb Function and General Health among Stroke Survivors. International Journal of Environmental Research and Public Health, 16(24), 5144. https://doi.org/10.3390/ijerph16245144