Fathers’ Views and Experiences of Creating a Smoke-Free Home: A Scoping Review

 ,
,  ,
, 

Abstract
:1. Introduction
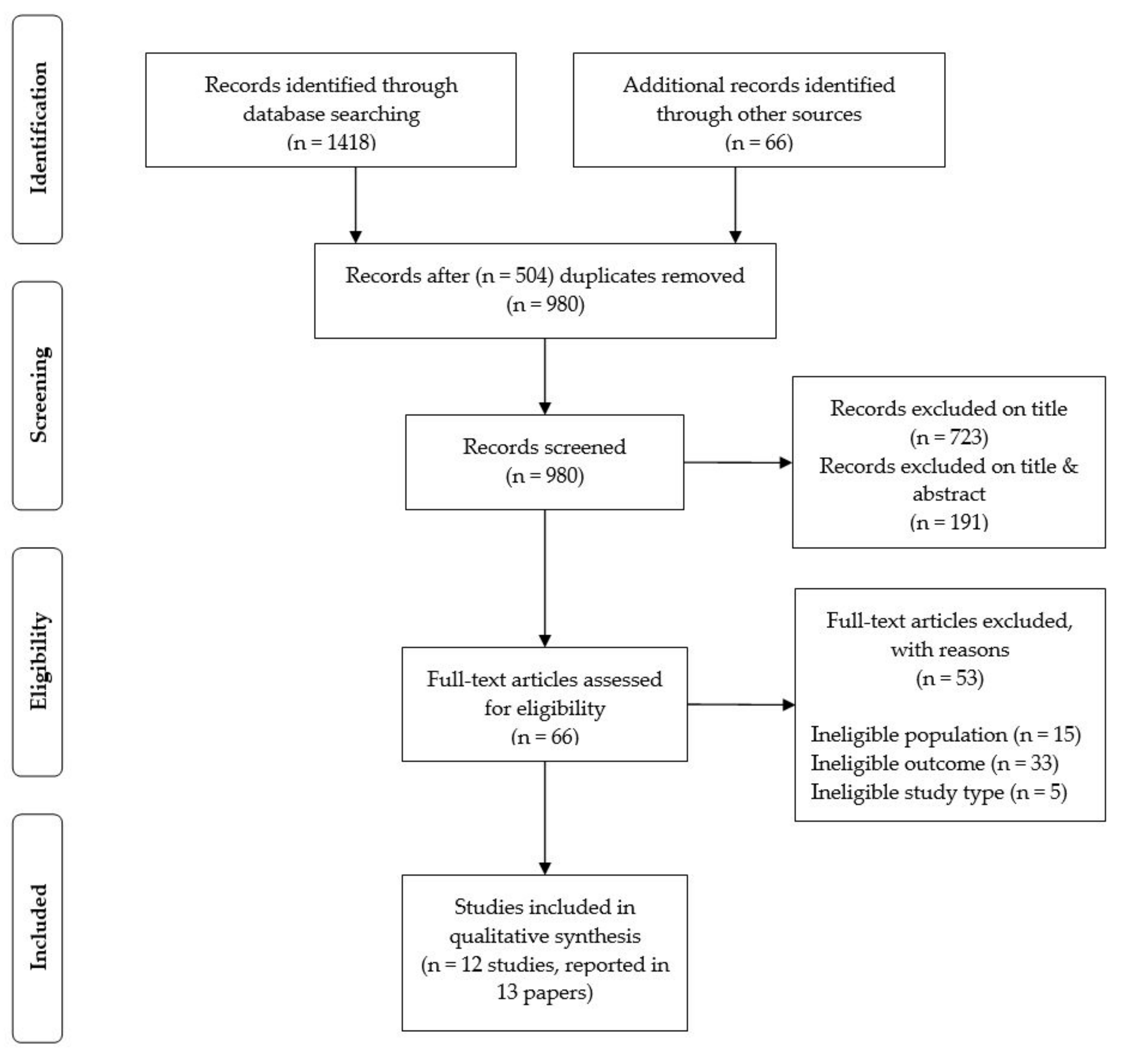
2. Materials and Methods
- Populations: the study’s sample comprised fathers, step-fathers, or male partners who smoked and lived in a home where a wife/partner and/or children also either lived or spent time there as their home, herein referred to as fathers.
- Interventions and Comparisons: the study could include none or any intervention and none or any comparison.
- Outcomes: the study investigated smoking behaviour in the home (evidenced by self-report and/or changes in objective measures of exposure to SHS (air quality, biological markers); and/or changes in SHS attitudes and/or knowledge; and/or any barriers and facilitators to changing smoking behaviour or creating a smoke-free home.
- Study types: the study collected qualitative and/or quantitative primary data, was written in English, and published since January 2008. This time frame was selected to limit the search to contemporary studies, and to acknowledge potential shifts in attitudes to smoking and smoke-free home environments associated with the increased focus on introducing comprehensive smoke-free laws from 2005 since the entry into force of the WHO Framework Convention on Tobacco Control (WHO-FCTC) [24].
- Studies of expectant fathers or female partners were also excluded because pregnancy is a well-documented ‘teachable moment’ where women may be more motivated to stop smoking [25]. Although a smaller number of studies have examined the extent to which pregnancy is a motivator for expectant fathers who quit smoking, it has been suggested that fathers are willing to make changes to their smoking behaviour during this time [26,27,28] and that they may feel differently about their health habits during pregnancy because they are more focused on the family as a whole [29].
- Grey literature and other literature reviews were also excluded.
3. Results
3.1. Facilitators and Barriers
3.1.1. Beliefs and Knowledge
3.1.2. Cultural and Perceived Social Norms
3.1.3. Gender Power Relations
3.1.4. Shifting Perceptions and Responsibilities Related to Fatherhood
3.2. Interventions
3.2.1. Counselling and Education
3.2.2. Education and Objective Assessment of Second-hand Smoke Levels in the Home
3.2.3. Education and Mobile-Health Interventions
3.2.4. Community-Based Interventions
3.2.5. Impact of Smoke-Free Public Places Legislation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| No. | Search String 1 |
|---|---|
| #1 | TS = (smok * OR tobacco OR cigarette * OR indoor * OR passive OR “ETS” OR “SHS” OR secondhand OR second-hand OR “second hand” OR antismoking OR “anti-smoking”) |
| #2 | TS = (home$ OR “at-home” OR hous * OR accommodation$ OR “private” OR “privacy” OR resid * OR cohabit * OR co-habit *) |
| #3 | TS = (father * OR step-father * OR stepfather * OR paternal OR husband * OR “male partner” OR “male partners” OR masculine *) |
| #4 | #3 AND #2 AND #1 |
| #5 | #4 AND LANGUAGE: (English) AND Timespan = 2008–2019 |
References
- Drope, J.; Schluger, N.; Cahn, Z.; Drope, J.; Hamill, S.; Islami, F.; Liber, A.; Nargis, N.; Stoklosa, M. The Tobacco Atlas; American Cancer Society and Vital Strategies: Atlanta, GA, USA, 2018. [Google Scholar]
- Jones, L.L.; Atkinson, O.; Longman, J.; Coleman, T.; McNeill, A.; Lewis, S.A. The motivators and barriers to a smoke-free home among disadvantaged caregivers: Identifying the positive levers for change. Nicotine Tob. Res. 2011, 13, 479–486. [Google Scholar] [CrossRef] [Green Version]
- Oberg, M.; Jaakkola, M.S.; Woodward, A.; Peruga, A.; Prüss-Ustün, A. Worldwide burden of disease from exposure to second-hand smoke: A retrospective analysis of data from 192 countries. Lancet 2011, 337, 139–146. [Google Scholar] [CrossRef]
- Saito, J.; Tabuchi, T.; Shibanuma, A.; Yasuoka, J.; Nakamura, M.; Jimba, M. ‘Only fathers’ smoking’ contributes the most to socioeconomic inequalities: Changes in socioeconomic inequalities in infants’ exposure to second hand smoke over time in Japan. PLoS ONE 2015, 10, e0139512. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Martinez-Donate, A.P.; Kuo, D.; Jones, N.R.; Palmersheim, K.A. Trends in home smoking bans in the U.S.A., 1995–2007: Prevalence, discrepancies and disparities. Tob. Control 2012, 21, 330–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisinger, C.; Hammer-Helmich, L.; Andreasen, A.H.; Jorgensen, T.; Glumer, C. Social disparities in children’s exposure to second hand smoke at home: A repeated cross-sectional survey. Environ. Health 2012, 11, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuntz, B.; Lampert, T. Social disparities in parental smoking and young children’s exposure to secondhand smoke at home: A time-trend analysis of repeated cross-sectional data from the German KiGGS study between 2003–2006 and 2009–2012. BMC Public Health 2016, 16, 485. [Google Scholar] [CrossRef] [Green Version]
- Gartner, C.E.; Hall, W.D. Is the socioeconomic gap in childhood exposure to secondhand smoke widening or narrowing? Tob. Control 2013, 22, 344–348. [Google Scholar] [CrossRef] [Green Version]
- Scottish Government. The Scottish Health Survey 2015: Volume 1: Main Report. 2016. Available online: http://www.gov.scot/Publications/2016/09/2764 (accessed on 22 July 2019).
- Passey, M.E.; Longman, J.M.; Robinson, J.; Wiggers, J.; Jones, L.L. Smoke-free homes: What are the barriers, motivators and enablers? A qualitative systematic review and thematic synthesis. BMJ Open 2016, 6, e010260. [Google Scholar] [CrossRef] [Green Version]
- Ng, M.; Freeman, M.K.; Fleming, T.D.; Robinson, M.; Dwyer-Lindgren, L.; Thomson, B.; Wollum, A.; Sanman, E.; Wulf, S.; Lopez, A.D.; et al. Smoking prevalence and cigarette consumption in 187 countries, 1980–2012. JAMA 2014, 311, 183–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Health Observatory Data Repository 2019. Available online: https://blogs.worldbank.org/opendata/men-smoke-5-times-more-women (accessed on 22 July 2019).
- Vitali, M.; Protano, C. How relevant are fathers who smoke at home to the passive smoking exposure of their children? Acta Paediatr. 2017, 106, 74. [Google Scholar] [CrossRef]
- Semple, S.; Abidin, E.; Amos, A.; Hashim, Z.; Siddiqi, K.; Ismail, N.; On Behalf of the Participants of the Smoke-Free Homes Workshop (Kuala Lumpur, 7–9 May 2018). The Kuala Lumpur Charter on Smoke-Free Homes. Tobacco Control Weblog. Available online: https://blogs.bmj.com/tc/2018/06/25/the-kuala-lumpur-charter-on-smoke-free-homes (accessed on 22 July 2019).
- Jacobson, B. The Ladykillers: Why Smoking Is a Feminist Issue; Pluto Press: London, UK, 1981. [Google Scholar]
- Greaves, L. Background Paper on Women and Tobacco; Health Canada: Ottawa, ON, Canada, 1990. [Google Scholar]
- Oliffe, J.L.; Bottorff, J.L.; Sarbit, G. Supporting fathers’ efforts to be smoke-free: Program principles. Can. J. Nurs. Res. 2012, 44, 64–82. [Google Scholar] [PubMed]
- Bottorff, J.L.; Oliffe, J.L.; Sarbit, G.; Huisken, A.; Caperchione, C.; Anand, A.; Howay, K. Evaluating the feasibility of a gender-sensitized smoking cessation program for fathers. Psychol. Men Masc. 2019, 20, 194–207. [Google Scholar] [CrossRef]
- Bottorff, J.L.; Haines-Saah, R.; Kelly, M.T.; Oliffe, J.L.; Torchalla, I.; Poole, N.; Greaves, L.; Robinson, C.A.; Ensom, M.H.; Okoli, C.T.; et al. Gender, smoking and tobacco reduction and cessation: A scoping review. Int. J. Equity Health 2014, 12, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greaves, L.; Pederson, A.; Poole, N. (Eds.) Making It Better: Gender-Transformative Health Promotion; Canadian Scholars Press: Toronto, ON, Canada, 2014; p. 22. [Google Scholar]
- Greaves, L. Can tobacco control be transformative? Reducing gender inequity and tobacco use among vulnerable populations. Int. J. Environ. Res. Public Health 2014, 11, 792–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; Ng, C.; Sharpe, J.P.; Wilson, K.; et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res. Methodol. 2016, 16, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Who Report on the Global Tobacco Epidemic. 2009. Implementing Smoke-Free Environments. Available online: https://www.who.int/tobacco/mpower/2009/GTCR_2009-web.pdf (accessed on 22 July 2019).
- McBride, C.M.; Emmons, K.M.; Lipkus, I.M. Understanding the potential of teachable moments: The case of smoking cessation. Health Educ. Res. 2003, 18, 156–170. [Google Scholar] [CrossRef]
- Gage, J.D.; Everett, K.D.; Bullock, L. A review of research literature addressing male partners and smoking during pregnancy. J. Obstet. Gynecol. Neonatal Nurs. 2007, 36, 574–580. [Google Scholar] [CrossRef]
- Pollak, K.I.; Denman, S.; Gordon, K.C.; Lyna, P.; Rocha, P.; Brouwer, R.N.; Fish, L.; Baucom, D.H. Is pregnancy a teachable moment for smoking cessation among US Latino expectant fathers? A pilot study. Ethn. Health 2010, 15, 47–59. [Google Scholar] [CrossRef]
- Yin, H.; Chen, X.; Zheng, P.; Kegler, M.; Shen, Q.; Xu, B. A neglected opportunity for China’s tobacco control? Shift in smoking behaviour during and after wives’ pregnancy. Tob. Induc. Dis. 2016, 14, 39. [Google Scholar] [CrossRef] [Green Version]
- Bottorff, J.L.; Oliffe, J.; Kalaw, C.; Carey, J.; Mroz, L. Men’s constructions of smoking in the context of women’s tobacco reduction during pregnancy and postpartum. Soc. Sci. Med. 2006, 62, 3096–3108. [Google Scholar] [CrossRef] [PubMed]
- Flemming, K.; Graham, H.; McCaughan, D.; Angus, K.; Bauld, L. The barriers and facilitators to smoking cessation experienced by women’s partners during pregnancy and the post-partum period: A systematic review of qualitative research. BMC Public Health 2015, 25, 849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA group. Preferred reporting items for systematic reviews and MetaAnalyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nichter, M.; Padmajam, S.; Nichter, M.; Sairu, P.; Aswathy, S.; Mini, G.K.; Bindu, V.C.; Pradeepkumar, A.S.; Thankappan, K.R. Developing a smoke free homes initiative in Kerala, India. BMC Public Health 2015, 15, 480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdullah, A.S.; Hua, F.; Xia, X.; Hurlburt, S.; Ng, P.; MacLeod, W.; Siegel, M.; Griffiths, S.; Zhang, Z. Second-hand smoke exposure and household smoking bans in Chinese families: A qualitative study. Health Soc. Care Community 2012, 20, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Berg, J.C.; Zheng, P.; Kegler, M.C. Perceived benefits of smoke-free homes, the process of establishing them, and enforcement challenges in Shanghai, China: A qualitative study. BMC Public Health 2015, 15, 89. [Google Scholar] [CrossRef] [Green Version]
- Kwon, J.; Oliffe, J.L.; Bottorff, J.L.; Kelly, M.T. Heterosexual gender relations and masculinity in fathers who smoke. Res. Nurs. Health 2014, 37, 391–398. [Google Scholar] [CrossRef] [Green Version]
- Mao, A.; Bottorff, J.L.; Oliffe, J.L.; Sarbit, G.; Kelly, M.T. A qualitative study of Chinese Canadian fathers’ smoking behaviours: Intersecting cultures and masculinities. BMC Public Health 2015, 15, 286. [Google Scholar] [CrossRef] [Green Version]
- Mao, A.; Bottorff, J.L.; Oliffe, J.L.; Sarbit, G.; Kelly, M.T. A qualitative study on Chinese Canadian male immigrants’ perspectives on stopping smoking: Implications for tobacco control in China. Am. J. Men’s Health 2018, 12, 812–818. [Google Scholar] [CrossRef]
- Oliffe, J.L.; Bottorff, J.L.; Johnson, J.L.; Kelly, M.T.; LeBeau, K. Fathers: Locating smoking and masculinity in the postpartum. Qual. Health Res. 2010, 20, 330–339. [Google Scholar] [CrossRef] [PubMed]
- Saito, J.; Shibanuma, A.; Yasuoka, J.; Kondo, N.; Takagim, D.; Jimba, M. Education and indoor smoking among parents who smoke: The mediating role of perceived social norms of smoking. BMC Public Health 2018, 18, 211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baheiraei, A.; Kharaghani, R.; Mohsenifar, A.; Kazemnejad, A.; Alikhani, S.; Sharifi Milani, H.; Mota, A.; Hovell, M.F. Reduction of secondhand smoke exposure among healthy infants in Iran: Randomized controlled trial. Nicotine Tob. Res. 2011, 13, 840–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, S.S.C.; Leung, D.Y.P.; Mak, Y.W.; Leung, G.M.; Leung, S.; Lam, T.H. New anti-smoking legislation on second-hand smoke exposure of children in homes. Hong Kong Med. J. 2011, 17, S38–S42. [Google Scholar]
- Chan, S.S.; Cheung, Y.T.; Leung, D.Y.; Mak, Y.W.; Leung, G.M.; Lam, T.H. Secondhand smoke exposure and maternal action to protect children from secondhand smoke: Pre- and post-smokefree legislation in Hong Kong. PLoS ONE 2014, 9, e15781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, S.; Duan, Z.; Redmon, P.B.; Eriksen, M.P.; Koplan, J.P.; Huang, C. mHealth intervention is effective in creating smoke-free homes for newborns: A randomized controlled trial study in China. Sci. Rep. 2017, 7, 9276. [Google Scholar] [CrossRef] [Green Version]
- Nacaroglu, H.T.; Can, D.; Gunay, I.; Karkiner, C.; Gunay, T.; Cimrin, D.; Nalcabasmaz, T. Does raising awareness in families reduce environmental tobacco smoke exposure in wheezy children? Postepy Dermatol. Alergol. 2017, 34, 350–356. [Google Scholar] [CrossRef] [Green Version]
- Behbod, B.; Sharma, M.; Baxi, R.; Roseby, R.; Webster, P. Family and carer smoking control programmes for reducing children’s exposure to environmental tobacco smoke. Cochrane Database Syst. Rev. 2018, 31, CD001746. [Google Scholar] [CrossRef] [Green Version]
- Rosen, L.J.; Myers, V.; Winickoff, J.P.; Kott, J. Effectiveness of interventions to reduce tobacco smoke pollution in homes: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2015, 12, 16043–16059. [Google Scholar] [CrossRef] [Green Version]
- Mdege, N.; Fairhurst, C.; Ferdous, T.; Hewitt, C.; Huque, R.; Jackson, C.; Kellar, I.; Parrott, S.; Semple, S.; Sheikh, A.; et al. Muslim Communities Learning About Second-hand Smoke in Bangladesh (MCLASS II): Study protocol for a cluster randomised controlled trial of a community-based smoke-free homes intervention, with or without Indoor Air Quality feedback. Trials 2019, 20, 11. [Google Scholar] [CrossRef]
- Shah, S.; Ainsworth, H.; Fairhurst, C.; Tilbrook, H.; Sheikh, A.; Amos, A.; Parrott, S.; Torgerson, D.; Thompson, H.; King, R.; et al. Muslim communities learning about second-hand smoke: A pilot cluster randomised controlled trial and cost-effectiveness analysis. NPJ Prim. Care Respir. Med. 2015, 25, 15052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, R.; Warsi, S.; Amos, A.; Shah, S.; Mir, G.; Sheikh, A.; Siddiqi, K. Involving mosques in health promotion programmes: A qualitative exploration of the MCLASS intervention on smoking in the home. Health Educ. Res. 2017, 32, 293–305. [Google Scholar] [CrossRef] [PubMed]
- Hitchman, S.C.; Fong, G.T. Gender empowerment and female-to-male smoking prevalence ratios. Bull. World Health Organ. 2011, 89, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Dworkin, S.L.; Fleming, P.L.; Colvin, C.J. The promises and limitations of gender-transformative health programming with men: Critical reflections from the field. Cult. Health Sex. 2015, 17, 128–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, G.R.; Parkhurst, J.O.; Ogden, J.A.; Aggleton, P.; Mahal, A. Structural approaches to HIV prevention. Lancet 2008, 372, 764–775. [Google Scholar] [CrossRef]
- Zheng, P.; Berg, C.J.; Kegler, M.C.; Fu, W.; Wang, J.; Zhou, X.; Liu, D.; Fu, H. Smoke-free homes and home exposure to secondhand smoke in Shanghai, China. Int. J. Environ. Res. Public Health 2014, 11, 12015–12028. [Google Scholar] [CrossRef]
- Wang, C.P.; Ma, S.J.; Xu, X.F.; Wang, J.F.; Mei, C.Z.; Yang, G.H. The prevalence of household second-hand smoke exposure and its correlated factors in six counties of China. Tob. Control 2009, 18, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Been, J.V.; Nurmatov, U.V.; Cox, B.; Nawrot, T.S.; van Schayck, C.P.; Sheikh, A. Effect of smoke-free legislation on perinatal and child health: A systematic review and meta-analysis. Lancet 2014, 383, 1549–1560. [Google Scholar] [CrossRef]
- Monson, E.; Arsenault, N. Effects of enactment of legislative (public) smoking bans on voluntary home smoking restrictions: A review. Nicotine Tob. Res. 2017, 19, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Prestwich, A.; Webb, T.; Conner, M. Using theory to develop and test interventions to promote changes in health behaviour: Evidence, issues, and recommendations. Curr. Opin. Psychol. 2015, 5, 1–5. [Google Scholar] [CrossRef]

| Reference | Country | Purpose | Population | Study Design | Key Findings of Relevance to Fathers |
|---|---|---|---|---|---|
| Abdullah et al. 2012 [34] | China (Shanghai) | To explore attitudes to children’s exposure to second-hand smoke in the home in order to inform more effective smoke-free home interventions and policies. | A convenience sample of 31 caregivers (12 fathers, 10 mothers, 9 grandparents) with children aged 5 and under. | Qualitative study; 4 focus groups and 10 in-depth interviews. Thematic analysis. | Facilitators: Most participants said they were willing to protect their child from SHS exposure. Barriers: There was a lack of knowledge about the health risks of SHS exposure. Many families did not openly discuss smoking restrictions at home, and had no rules in place. Other barriers to adopting a smoke-free home included the social acceptability of smoking, hosting social gatherings at home, authoritative attitudes of the father or father-in-law, and difficulties with visitors who smoked. |
| Berg et al. 2011 [35] | China (Shanghai) | To examine the reasons, processes and challenges associated with establishing smoke-free homes policies. | 13 fathers who were current smokers and 17 mothers who were non-smokers living with at least one child. | Qualitative study; 30 face to face semi-structured interviews. Thematic analysis. | Facilitators: Mothers were credited with initiating discussion regarding creating a smoke-free home more often and were reported to have decision making authority. Barriers: Common responses to their request to establish a smoke-free home among fathers were agreement, ignoring it, temporarily acquiescing, insisting on smoking in the home anyway, and devaluing the benefits of creating smoke-free homes. Challenges to enforcement included weather, social situations, the smoker being home alone, ineffective harm reduction behaviours such as smoking near windows, and addiction. |
| Kwon et al. 2014 [36] | Canada | To explore the role of masculinity in new and expectant fathers’ explanations of their continued smoking. | 20 fathers (10 of European descent, and 10 of either Asian or Middle Eastern descent) from a previous study with a sample of 29 fathers. | Qualitative study; secondary analysis of interview data from a larger programme of research. | Facilitators: Most fathers reported reconciling with their partners to maintain a smoke-free home. In order to be responsible fathers and spousal partners, they accepted that their smoking routines needed to change. For some, new routines of parenting reduced their opportunities to smoke in the home. Domestic duties such as mowing the lawn and walking the dog provided them with opportunities to smoke outside. Fathers drew on masculine ideas such as protector and risk-taker, which influenced their smoking behaviour change efforts in the home. |
| Mao et al. 2015 [37], 2018 [38] | Canada (Ontario, Quebec, British Columbia) | To explore (1) the smoking-related experiences of immigrant Chinese fathers, and (2) the influence of denormalization in Canada on male Chinese immigrant smoking after migration. | 22 fathers of Chinese origin who were currently smoking or had quit smoking in the past 5 years. | Qualitative study; semi-structured telephone interviews. Interpretive thematic analysis. | Facilitators: The message that exposure to SHS is harmful to pregnant women and young children was well understood. Fathers’ changes in smoking were constructed as voluntary behaviour modifications, rather than forced practices. The Chinese fathers were willing to conform to Canadian smoking norms and extended the ban on indoor smoking in the public sphere into homes. Becoming a father strengthened efforts to maintain a smoke-free home, even during the cold Canadian winter months. Involvement in childcare also increased the Chinese fathers’ determination to restrict their home smoking. |
| Nichter et al. 2015 [33] (see also Table 2) | India (Kerala) | To develop, refine and promote a community-based smoke-free homes intervention to reduce SHS exposure among women and children at home. | Survey: 140 husband wife pairs, where the husband was a smoker Focus Groups/Intervention development: 3 focus groups of 8 wives, whose husbands smoked. | Quantitative survey measuring attitudes re: SHS exposure.Qualitative; Focus groups discussing household gender relations and the ability of women to encourage a smoke-free home. | Barriers: Most women felt powerless to change their husband’s behaviour, as (typically in this region of India) husbands do not listen to advice from their wives about their personal habits. Men and women underestimated the risks of SHS exposure to child health, but men more so–65% of women thought it could cause serious illness, compared to only 32% of men. 28% of women believed it could cause minor illness or was harmless, compared to 42% of men. |
| Oliffe et al. 2010 [39] | Canada (Vancouver) | To investigate smoking and masculinities by detailing the highly gendered nature of the everyday places where fathers smoke. | 20 new fathers who cohabited with their female partner and smoked during the pregnancy and postpartum period. | Ethnographic study–fathers took part in a semi-structured interview in the first month postpartum, were given a camera and encouraged to take pictures of the places that they smoked in during their partner’s pregnancy and afterwards. A second interview was then conducted to discuss photographs taken. | Facilitators: Most fathers understood the dangers of SHS exposure in the home. Fathers spoke of their preference to smoke at work rather than at home, as this gave them freedom to smoke without the surveillance from or risk to their child or partner. Some fathers linked the discussion of their outdoor smoking to notions of good fathering. |
| Saito et al. 2018 [40] | Japan | To test the potential mediating role of perceived smoking norms on the associations between education and indoor smoking among parents who smoke. | A convenience sample of 1645 parents (822 mothers, 823 fathers) from an online survey panel. | Quantitative; cross-sectional study. | Facilitators: Perceived smoking norms mediated the association between education and indoor smoking. Household smoking status and a worksite smoking ban also mediated this association via perceived norms, but only for fathers. Barriers: For both fathers and mothers who smoked, years of education was significantly negatively associated with indoor smoking behaviours. |
| Reference | Country | Purpose | Population | Study Design | Key Findings of Relevance to Fathers |
|---|---|---|---|---|---|
| Baheiraei et al. 2011 [41] | Iran (Tehran) | To investigate whether counselling both mothers and fathers reduces their infants’ exposure to SHS. | N = 130 (convenience sample of families with children less than 1 year old, exposed to SHS. In 97% of households only the father smoked. Families were recruited whilst attending a health centre for routine infant health checks). | Randomised controlled trial. Mothers in the intervention group each received 3 counselling sessions, one of which was face to face (location not specified) and two of which were by telephone, and fathers in the intervention group received 3 counselling sessions by telephone. The control group received usual care. | In the intervention group, the number of smoke-free homes increased significantly from 15% at baseline to 33.3% at the 3-month follow-up. The differences between the two groups were statistically significant (p < 0.05). The intervention was effective in reducing infant urinary cotinine levels (p < 0.05). |
| Chan et al. 2011 [42] | China (Hong Kong) | To study whether smoking fathers would smoke inside their homes owing to smoke-free legislation in public places. | Pre-legislation group (2005) comprised of 186 families and the 2006 group of 114 families Post legislation group (2007a) comprised of 742 non-smoking mothers and 608 fathers and the 2007b group of 189 mothers, 174 fathers. | Prospective survey of two cohorts of families recruited before legislation and a cross-sectional survey of families after legislation. | Significantly more fathers in the 2007a group than the 2006 group never smoked at home (26.7% vs. 14.0%, p < 0.001), and never smoked around their children (59.7% vs. 30.7%, p < 0.001). The differences remained significant after adjusting for the father’s educational level and age. Regarding 60.6% of fathers who smoked at home and 45.3% of fathers who smoked around children in the 2007a group, they only smoked one to four cigarettes daily at home and around children, respectively. |
| Chan et al. 2014 [43] | China (Hong Kong) | To investigate the effect of maternal action to protect children from SHS and a 2007 public smoking ban, on children’s exposure to SHS in the home. | 333 families participated in surveys prior to the smoking ban and 742 families participated in surveys post smoking ban. | Quantitative study, comparing survey data and direct measurement of SHS exposure levels from previous studies conducted prior to a public smoking ban, with that from survey data and SHS exposure levels collected for the present study post smoking ban. | Fathers’ smoking in the home decreased post-legislation. 29.3% of children post-legislation were exposed to SHS in the home, compared with 87.2% pre-legislation (p < 0.01). Hair nicotine level in mothers and children post-legislation was lower than pre-legislation. Over 90% of mothers pre-and post-legislation advised the fathers to reduce smoking, avoid smoking at home or avoid smoking near the children. This suggests that specific interventions for families should be expanded together with smoke-free legislation. |
| Nichter et al. 2015 [33] (see also Table 1) | India (Kerala) | To develop, refine and promote a community-based smoke-free homes intervention to reduce SHS exposure among women and children at home. | Proof of concept study: N = 140 Pilot study 1: N = 95 Pilot study 2: N = 157 (husband wife pairs, where husband was a smoker). | Community based intervention including educational meetings, smoke free homes video, healthcare worker household visits, community meetings and community declarations of support for smoke-free homes. | At baseline, across the pilot studies, between 70–80% of men regularly smoked in their home, despite 80% of women having asked their husband not to. Six months post intervention between 34% and 59% of men who smoked no longer smoked in their home. The authors note that this represents a modest, but significant change in community smoking norms. No statistical tests of significance were applied to the data. |
| Yu et al. 2017 [44] | China (Changchun) | To investigate if interventions that incorporate traditional and mobile phone based education help create smoke-free homes for infants and increase quitting among fathers. | N = 342 (families: non-smoking mothers and their newborns currently exposed to SHS in the home by fathers’ smoking). | Randomised controlled trial involving three groups: Intervention Group I-A received counselling on SHS harms to children, education on creating a smoke-free home, and posters to display in the home to encourage fathers and other visitors not to smoke. Intervention Group I-B received the same intervention as I-A, with additional text messages to the mother/father on harms of SHS to the mother and child. The father received additional text messages to quit smoking. Control Group: Received only standard care for their initial postnatal visits, which did not include any tobacco control or cessation counselling service. | Although no reduction of the self-reported exposure rate to SHS among surveyed mothers of newborns was found at 6 months, the rate at 12 months was significantly decreased in I-B compared to the control group. Participants in the I-B group were more likely to report “smoking never permitted inside home” compared to participants in control group at 12 months (1.17 vs. 4.71, p < 0.05). These findings suggest that the addition of an mHealth element to interventions with in-person counselling and provision of educational materials effectively aided in creating smoke-free homes among fathers of newborns. |
| Nacaroglu et al. 2017 [45] | Turkey (Izmir) | To determine whether informing families about their children’s urinary cotinine levels curtailed the exposure of children to SHS. | N = 193 children (Intervention group 97, control group 96). Families of the children recruited via a local hospital. There was no report of the family make-up and gender differences in the sample. | Randomised controlled trial. Urinary cotinine levels were measured in all children. Parents in the intervention group were given education about SHS harms and were advised about their child’s urinary cotinine levels by telephone. The control group were not informed about their child’s urinary cotinine levels until the end of the study. | In the intervention group, significant decreases in the number of cigarettes that fathers smoked both daily (16.8 to 14.5) and at home (7.69 to 3.96) were evident (p = 0.001 and p = 0.001, respectively). Although the number of cigarettes smoked daily by mothers both at home and outside decreased, the decreases were not significant. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Donnell, R.; Angus, K.; McCulloch, P.; Amos, A.; Greaves, L.; Semple, S. Fathers’ Views and Experiences of Creating a Smoke-Free Home: A Scoping Review. Int. J. Environ. Res. Public Health 2019, 16, 5164. https://doi.org/10.3390/ijerph16245164
O’Donnell R, Angus K, McCulloch P, Amos A, Greaves L, Semple S. Fathers’ Views and Experiences of Creating a Smoke-Free Home: A Scoping Review. International Journal of Environmental Research and Public Health. 2019; 16(24):5164. https://doi.org/10.3390/ijerph16245164
Chicago/Turabian StyleO’Donnell, Rachel, Kathryn Angus, Peter McCulloch, Amanda Amos, Lorraine Greaves, and Sean Semple. 2019. "Fathers’ Views and Experiences of Creating a Smoke-Free Home: A Scoping Review" International Journal of Environmental Research and Public Health 16, no. 24: 5164. https://doi.org/10.3390/ijerph16245164
APA StyleO’Donnell, R., Angus, K., McCulloch, P., Amos, A., Greaves, L., & Semple, S. (2019). Fathers’ Views and Experiences of Creating a Smoke-Free Home: A Scoping Review. International Journal of Environmental Research and Public Health, 16(24), 5164. https://doi.org/10.3390/ijerph16245164