A Systematic Review of Methods, Study Quality, and Results of Economic Evaluation for Childhood and Adolescent Obesity Intervention


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
- Types of study: Primary full economic evaluations were included (studies in which both the costs and outcomes of the alternatives are examined and in which a comparison of two or more interventions or case alternatives are undertaken) including trial-based and model-based (using trial data) evaluations. Partial economic evaluations; qualitative studies; conference abstracts; and study protocols were excluded.
- Participants/population: Children and adolescents aged 0–19 years at the start of the intervention and/or their parents/guardians were included. Family based interventions were also included when the target participants were the children. Economic evaluations undertaken within any country context were included. Interventions to tackle obesity due to a secondary cause (e.g., Prader–Willi syndrome) were excluded.
- Intervention(s), exposure(s): All behavioural (focused on individual behaviour change techniques), environmental (focused on modifying the local environment), or policy (focused on population-wide legislative or fiscal action) interventions for the treatment or prevention of overweight/obesity in children and/or adolescents were included. Pharmacological or surgical interventions were excluded.
- Comparator(s)/control: Only studies with a clearly defined comparator were included with no restrictions on the types of comparator(s).
- Outcome(s): No restrictions on outcomes measures. Potentially relevant outcomes were: disability-adjusted life years (DALYs); quality-adjusted life years (QALYs); effectiveness outcomes such as kilogramme weight loss; % body fat; body mass index (BMI) z-score; waist circumference; overweight and obesity cases avoided; additional minute of moderate to vigorous physical activity (MVPA); increase in overall physical activity level and metabolic equivalent (MET) hour gained.
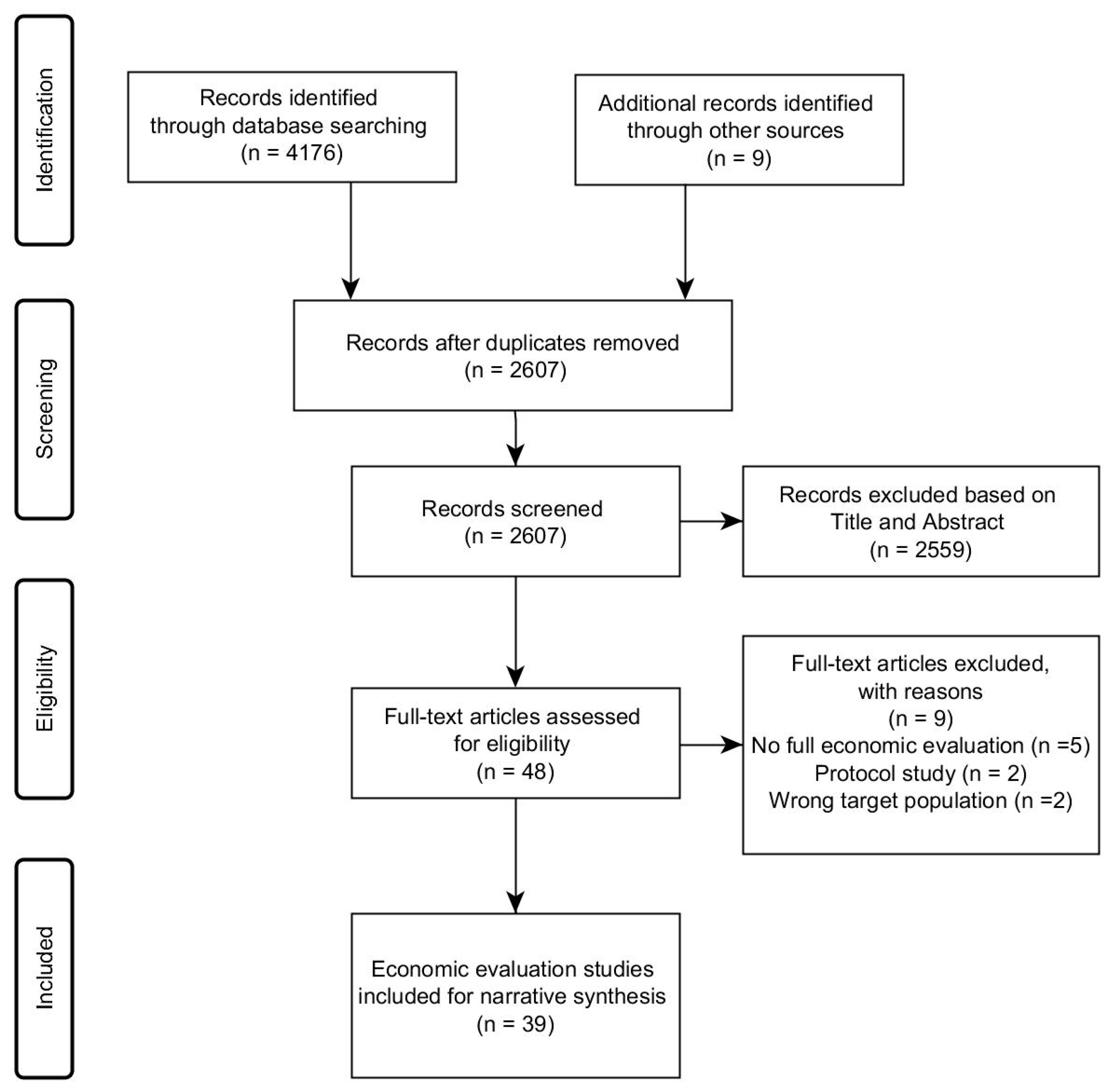
2.3. Study Selection Procedure
2.4. Data Extraction
2.5. Quality Assessment of Included Studies
3. Results
3.1. Details about Study Context
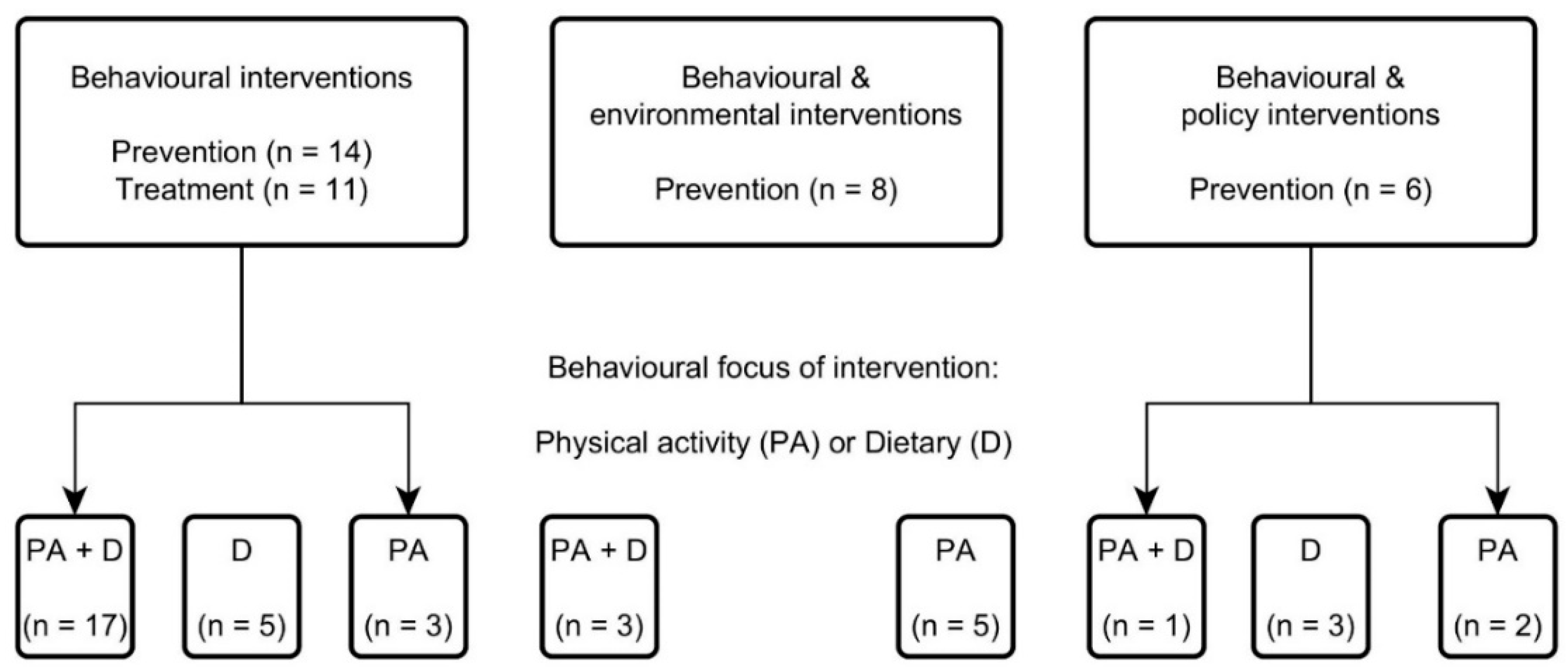
3.1.1. Intervention and Comparator
3.1.2. Country and Setting
3.2. Review of Economic Evaluation Methods
3.2.1. Type of Economic Evaluation and Measures of Effectiveness
3.2.2. Evaluation Perspective Taken
3.2.3. Time Horizon Considered and Type of Modelling Approach Taken
3.2.4. Choice of Discount Rate
3.2.5. Methods for Collecting and Estimating Resource Use/Costs
3.2.6. Sensitivity Analysis Undertaken
3.3. Narrative Synthesis of Cost-Effectiveness Evidence
3.4. Quality Assessment of the Included Studies
4. Discussion
4.1. Comparison with Previous Systematic Reviews
4.2. Strengths and Limitations of this Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Au, N. The health care cost implications of overweight and obesity during childhood. Health Serv. Res. 2012, 47, 655–676. [Google Scholar] [CrossRef] [PubMed]
- Neovius, K.; Johansson, K.; Kark, M.; Neovius, M. Obesity status and sick leave: A systematic review. Obes. Rev. 2009, 10, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Basterfield, L.; Jones, A.R.; Parkinson, K.N.; Reilly, J.; Pearce, M.S.; Reilly, J.J.; Adamson, A.J.; Team, G.M.S.C. Physical activity, diet and BMI in children aged 6–8 years: A cross-sectional analysis. BMJ Open 2014, 4, e005001. [Google Scholar] [CrossRef] [PubMed]
- Lobstein, T.; Baur, L.; Uauy, R. Obesity in children and young people: A crisis in public health. Obes. Rev. 2004, 5, 4–85. [Google Scholar] [CrossRef] [PubMed]
- Blake-Lamb, T.L.; Locks, L.M.; Perkins, M.E.; Baidal, J.A.W.; Cheng, E.R.; Taveras, E.M. Interventions for childhood obesity in the first 1000 days a systematic review. Am. J. Prev. Med. 2016, 50, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Seburg, E.M.; Olson-Bullis, B.A.; Bredeson, D.M.; Hayes, M.G.; Sherwood, N.E. A review of primary care-based childhood obesity prevention and treatment interventions. Curr. Obes. Rep. 2015, 4, 157–173. [Google Scholar] [CrossRef]
- Wang, Y.; Cai, L.; Wu, Y.; Wilson, R.; Weston, C.; Fawole, O.; Bleich, S.N.; Cheskin, L.J.; Showell, N.N.; Lau, B. What childhood obesity prevention programmes work? A systematic review and meta-analysis. Obes. Rev. 2015, 16, 547–565. [Google Scholar] [CrossRef] [Green Version]
- Palmer, S.; Raftery, J. Economics notes: Opportunity cost. BMJ Br. Med J. 1999, 318, 1551. [Google Scholar] [CrossRef]
- Ananthapavan, J.; Sacks, G.; Moodie, M.; Carter, R. Economics of obesity—Learning from the past to contribute to a better future. Int. J. Environ. Res. Public Health 2014, 11, 4007–4025. [Google Scholar] [CrossRef]
- Frew, E. Economic evaluation of childhood obesity interventions: Reflections and suggestions. PharmacoEconomics 2016, 34, 733–740. [Google Scholar] [CrossRef]
- Johannesson, M.; Jonsson, B.; Jonsson, L.; Kobelt, G.; Zethraeus, N. Why should economic evaluations of medical innovations have a societal perspective? Available online: https://www.ohe.org/publications/why-should-economic-evaluations-medical-innovations-have-societal-perspective (accessed on 17 April 2017).
- Carter, R.; Moodie, M.; Markwick, A.; Magnus, A.; Vos, T.; Swinburn, B.; Haby, M.M. Assessing Cost-Effectiveness in Obesity (ACE-Obesity): An overview of the ACE approach, economic methods and cost results. BMC Public Health 2009, 9, 419. [Google Scholar] [CrossRef] [PubMed]
- Doring, N.; Mayer, S.; Rasmussen, F.; Sonntag, D. Economic evaluation of obesity prevention in early childhood: Methods, limitations and recommendations. Int. J. Environ. Res. Public Health 2016, 13, 911. [Google Scholar] [CrossRef] [PubMed]
- Erdol, S.; Mazzucco, W.; Boccia, S. Cost effectiveness analysis of childhood obesity primary prevention programmes: A systematic review. Epidemiol. Biostat. Public Health 2014, 11. [Google Scholar] [CrossRef]
- Gortmaker, S.L.; Long, M.W.; Resch, S.C.; Ward, Z.J.; Cradock, A.L.; Barrett, J.L.; Wright, D.R.; Sonneville, K.R.; Giles, C.M.; Carter, R.C.; et al. Cost Effectiveness of Childhood Obesity Interventions Evidence and Methods for CHOICES. Am. J. Prev. Med. 2015, 49, 102–111. [Google Scholar] [CrossRef] [PubMed]
- John, J.; Wolfenstetter, S.B.; Wenig, C.M. An economic perspective on childhood obesity: Recent findings on cost of illness and cost effectiveness of interventions. Nutrition 2012, 28, 829–839. [Google Scholar] [CrossRef] [PubMed]
- Korber, K. Quality assessment of economic evaluations of health promotion programs for children and adolescents-a systematic review using the example of physical activity. Health Econ. Rev. 2015, 5, 35. [Google Scholar] [CrossRef] [PubMed]
- Lobstein, T.; Jackson-Leach, R.; Moodie, M.L.; Hall, K.D.; Gortmaker, S.L.; Swinburn, B.A.; James, W.P.T.; Wang, Y.; McPherson, K. Child and adolescent obesity: Part of a bigger picture. Lancet 2015, 385, 2510–2520. [Google Scholar] [CrossRef]
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Robertson, W.; Fleming, J.; Kamal, A.; Hamborg, T.; Khan, K.A.; Griffiths, F.; Stewart-Brown, S.; Stallard, N.; Petrou, S.; Simkiss, D.; et al. Randomised controlled trial evaluating the effectiveness and cost-effectiveness of ‘families for health’, a family-based childhood obesity treatment intervention delivered in a community setting for ages 6 to 11 years. Health Technol. Assess. 2017, 21. [Google Scholar] [CrossRef]
- Sutherland, R.; Reeves, P.; Campbell, E.; Lubans, D.R.; Morgan, P.J.; Nathan, N.; Wolfenden, L.; Okely, A.D.; Gillham, K.; Davies, L.; et al. Cost effectiveness of a multi-component school-based physical activity intervention targeting adolescents: The ‘Physical Activity 4 Everyone’ cluster randomized trial. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 94. [Google Scholar] [CrossRef]
- Graziose, M.M.; Koch, P.A.; Wang, Y.C.; Lee Gray, H.; Contento, I.R. Cost-effectiveness of a Nutrition Education Curriculum Intervention in Elementary Schools. J. Nutr. Educ. Behav. 2016. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Zanganeh, M.; Adab, P.; Li, B.; Frew, E. Protocol for a systematic review of methods and cost-effectiveness findings of economic evaluations of obesity prevention and/or treatment interventions in children and adolescents. BMC Syst. Rev. 2018, 7, 54. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.L.; Gortmaker, S.L.; Long, M.W.; Ward, Z.J.; Resch, S.C.; Moodie, M.L.; Carter, R.; Sacks, G.; Swinburn, B.A.; Wang, Y.C.; et al. Cost Effectiveness of an Elementary School Active Physical Education Policy. Am. J. Prev. Med. 2015, 49, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Brown, I.H.S.; Perez, A.; Li, Y.P.; Hoelscher, D.M.; Kelder, S.H.; Rivera, R. The cost-effectiveness of a school-based overweight program. Int. J. Behav. Nutr. Phys. Act. 2007, 4, 47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, M.W.; Gortmaker, S.L.; Ward, Z.J.; Resch, S.C.; Moodie, M.L.; Sacks, G.; Swinburn, B.A.; Carter, R.C.; Wang, Y.C. Cost Effectiveness of a Sugar-Sweetened Beverage Excise Tax in the US. Am. J. Prev. Med. 2015, 49, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Magnus, A.; Haby, M.M.; Carter, R.; Swinburn, B. The cost-effectiveness of removing television advertising of high-fat and/or high-sugar food and beverages to Australian children. Int. J. Obes. 2009, 33, 1094–1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moodie, M.; Haby, M.; Galvin, L.; Swinburn, B.; Carter, R. Cost-effectiveness of active transport for primary school children—Walking School Bus program. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 63. [Google Scholar] [CrossRef]
- Moodie, M.L.; Carter, R.C.; Swinburn, B.A.; Haby, M.M. The Cost-effectiveness of Australia′s Active After-school Communities Program. Obesity 2010, 18, 1585–1592. [Google Scholar] [CrossRef]
- Moodie, M.; Haby, M.M.; Swinburn, B.; Carter, R. Assessing cost-effectiveness in obesity: Active transport program for primary school children- TravelSMART Schools Curriculum program. J. Phys. Act. Health 2011, 8, 503–515. [Google Scholar] [CrossRef]
- Moodie, M.L.; Herbert, J.K.; de Silva-Sanigorski, A.M.; Mavoa, H.M.; Keating, C.L.; Carter, R.C.; Waters, E.; Gibbs, L.; Swinburn, B.A. The Cost-Effectiveness of a Successful Community-Based Obesity Prevention Program: The Be Active Eat Well Program. Obesity 2013, 21, 2072–2080. [Google Scholar] [CrossRef]
- Pringle, A.; Cooke, C.; Gilson, N.; Marsh, K.; McKenna, J. Cost-effectiveness of interventions to improve moderate physical activity: A study in nine UK sites. Health Educ. J. 2010, 69, 211–224. [Google Scholar] [CrossRef]
- Rush, E.; Obolonkin, V.; McLennan, S.; Graham, D.; Harris, J.D.; Mernagh, P.; Weston, A.R. Lifetime cost effectiveness of a through-school nutrition and physical programme: Project Energize. Obes. Res. Clin. Pract. 2014, 8, E115–E122. [Google Scholar] [CrossRef] [PubMed]
- Sonneville, K.R.; Long, M.W.; Ward, Z.J.; Resch, S.C.; Wang, Y.C.; Pomeranz, J.L.; Moodie, M.L.; Carter, R.; Sacks, G.; Swinburn, B.A.; et al. BMI and Healthcare Cost Impact of Eliminating Tax Subsidy for Advertising Unhealthy Food to Youth. Am. J. Prev. Med. 2015, 49, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.Y.; Yang, Q.H.; Lowry, R.; Wechsler, H. Economic analysis of a school-based obesity prevention program. Obes. Res. 2003, 11, 1313–1324. [Google Scholar] [CrossRef]
- Wang, L.Y.; Nichols, L.P.; Austin, S.B. The Economic Effect of Planet Health on Preventing Bulimia Nervosa. Arch. Pediatr. Adolesc. Med. 2011, 165, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Wright, D.R.; Kenney, E.L.; Giles, C.M.; Long, M.W.; Ward, Z.J.; Resch, S.C.; Moodie, M.L.; Carter, R.C.; Wang, Y.C.; Sacks, G.; et al. Modeling the Cost Effectiveness of Child Care Policy Changes in the US. Am. J. Prev. Med. 2015, 49, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Hollingworth, W.; Hawkins, J.; Lawlor, D.A.; Brown, M.; Marsh, T.; Kipping, R.R. Economic evaluation of lifestyle interventions to treat overweight or obesity in children. Int. J. Obes. 2012, 36, 559–566. [Google Scholar] [CrossRef]
- Moodie, M.; Haby, M.; Wake, M.; Gold, L.; Carter, R. Cost-effectiveness of a family-based GP-mediated intervention targeting overweight and moderately obese children. Econ. Hum. Biol. 2008, 6, 363–376. [Google Scholar] [CrossRef]
- McAuley, K.A.; Taylor, R.W.; Farmer, V.L.; Hansen, P.; Williams, S.M.; Booker, C.S.; Mann, J.I. Economic Evaluation of a Community-based Obesity Prevention Program in Children: The A. PPLE Project. Obesity 2010, 18, 131–136. [Google Scholar] [CrossRef]
- Wang, L.Y.; Gutin, B.; Barbeau, P.; Moore, J.B.; Hanes, J., Jr.; Johnson, M.H.; Cavnar, M.; Thornburg, J.; Yin, Z. Cost-effectiveness of a school-based obesity prevention program. J. Sch. Health 2008, 78, 619–624. [Google Scholar] [CrossRef]
- Peterson, M.; Chandlee, M.; Abraham, A. Cost-effectiveness analysis of a statewide media campaign to promote adolescent physical activity. Health Promot. Pr. 2008, 9, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.; Lung, T.; Wen, L.M.; Baur, L.; Rissel, C.; Howard, K. Economic Evaluation of “Healthy Beginnings” an Early Childhood Intervention to Prevent Obesity. Obesity 2014, 22, 1709–1715. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.P.; Xu, H.Q.; Liu, A.L.; van Raaij, J.; Bemelmans, W.; Hu, X.Q.; Zhang, Q.; Du, S.M.; Fang, H.Y.; Ma, J.; et al. The Costs and Cost-Effectiveness of a School-Based Comprehensive Intervention Study on Childhood Obesity in China. PLoS ONE 2013, 8, e77971. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.H.; Paluch, R.A.; Wrotniak, B.H.; Daniel, T.O.; Kilanowski, C.; Wilfley, D.; Finkelstein, E. Cost-Effectiveness of Family-Based Group Treatment for Child and Parental Obesity. Child 2014, 10, 114–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldfield, G.S.; Epstein, L.H.; Kilanowski, C.K.; Paluch, R.A.; Kogut-Bossler, B. Cost-effectiveness of group and mixed family-based treatment for childhood obesity. Int. J. Obes. 2001, 25, 1843–1849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hollinghurst, S.; Hunt, L.P.; Banks, J.; Sharp, D.J.; Shield, J.P. Cost and effectiveness of treatment options for childhood obesity. Pediatr. Obes. 2014, 9, E26–E34. [Google Scholar] [CrossRef]
- Janicke, D.M.; Sallinen, B.J.; Perri, M.G.; Lutes, L.D.; Silverstein, J.H.; Brumback, B. Comparison of Program Costs for Parent-Only and Family-Based Interventions for Pediatric Obesity in Medically Underserved Rural Settings. J. Rural. Health 2009, 25, 326–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wake, M.; Gold, L.; McCallum, Z.; Gerner, B.; Waters, E. Economic evaluation of a primary care trial to reduce weight gain in overweight/obese children: The LEAP trial. Ambul. Pediatr. 2008, 8, 336–341. [Google Scholar] [CrossRef]
- Kesztyus, D.; Schreiber, A.; Wirt, T.; Wiedom, M.; Dreyhaupt, J.; Brandstetter, S.; Koch, B.; Wartha, O.; Muche, R.; Wabitsch, M.; et al. Economic evaluation of URMEL-ICE, a school-based overweight prevention programme comprising metabolism, exercise and lifestyle intervention in children. Eur. J. Health Econ. 2013, 14, 185–195. [Google Scholar] [CrossRef]
- Krauth, C.; Liersch, S.; Sterdt, E.; Henze, V.; Robl, M.; Walter, U. Health economic evaluation of health promotion - the example “fit for pisa”. Gesundheitswesen 2013, 75, 742–746. [Google Scholar]
- Martinez, P.M.; Lopez, M.S.; Bastida, J.L.; Sotos, F.E.; Pacheco, B.N.; Aguilar, F.S.; Vizcaino, V.M. Cost-effectiveness of an intervention to reduce overweight and obesity in 9–10-year-olds. The Cuenca study. Gac. Sanit. 2011, 25, 198–204. [Google Scholar]
- Kalavainen, M.; Karjalainen, S.; Martikainen, J.; Korppi, M.; Linnosmaa, I.; Nuutinen, O. Cost-effectiveness of routine and group programs for treatment of obese children. Pediatr. Int. 2009, 51, 606–611. [Google Scholar] [CrossRef] [PubMed]
- PHARMAC Pharmaceutical Management Agency. Prescription for Pharmacoeconomic Analysis: Methods for Cost-utility Analysis; Version 2.2; PHARMAC Pharmaceutical Management Agency: Wellington, New Zealand, 2015. [Google Scholar]
- Pharmaceutical Benefits Advisory Committee (PBAC). Guidelines for Preparing Submissions to the Pharmaceutical Benefits Advisory Committee; Version 4.3; Australian Government Department of Health and Ageing: Canberra, Australia, 2008.
- NICE. Methods for the Development of NICE Public Health Guidance; National Institute for Health and Care Excellence: London, UK, 2012. [Google Scholar]
- Academy of Managed Care Pharmacy. The AMCP Format for Formulary Submissions; Version 4.0; Academy of Managed Care Pharma: Alexandria, VA, USA, 2016. [Google Scholar]
- Anderson, R. Systematic reviews of economic evaluations: Utility or futility? Health Econ. 2010, 19, 350–364. [Google Scholar] [CrossRef] [PubMed]
- Frew, E. Aligning Health Economics Methods to Fit with the Changing World of Public Health. Appl. Health Econ. Health Policy 2017, 15, 287–289. [Google Scholar] [CrossRef] [PubMed]
- Treasury, H. The Green Book, Appraisal and Evaluation in Central Government Treasury Guidance London; The Stationery Office (TSO): London, UK, 2011. [Google Scholar]
- Musgrove, P.; Fox-Rushby, J. Cost-effectiveness analysis for priority setting. In Disease Control Priorities in Developing Countries; The World Bank: Washington, DC, USA, 2006. [Google Scholar]
- NICE. Guide to the Methods of Technology Appraisal 2013; National Institute for Health and Clinical Excellence: London, UK, 2013. [Google Scholar]



{kind=link}
{kind=link}
| Study Characteristics | Number of Studies Identified (%) | |
|---|---|---|
| Year of publication | ||
| 2001–2009 | 17 (44) | |
| 2010–2017 | 22 (56) | |
| Study approach | ||
| Trial-based | Prevention | 9 (23) |
| Treatment | 7 (18) | |
| Model-based | Prevention | 19 (49) |
| Treatment | 4 (10) | |
| Comparator selected | ||
| Usual care | 33 (85) | |
| Another intervention | 6 (15) | |
| Country | ||
| High-income | ||
| Australia | 15 (38.5) | |
| New Zealand | 2 (5) | |
| The USA | 12 (31.5) | |
| Canada | 1 (2.5) | |
| The UK | 4 (10) | |
| Germany | 2 (5) | |
| Finland | 1 (2.5) | |
| Spain | 1 (2.5) | |
| Low and middle-income | ||
| China | 1 (2.5) | |
| Setting | ||
| Prevention | ||
| School | 21 (54) | |
| US/Australian state | 5 (13) | |
| Community | 1 (2.5) | |
| Home | 1 (2.5) | |
| Treatment | ||
| Clinical | 9 (23) | |
| School | 1 (2.5) | |
| Community | 1 (2.5) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanganeh, M.; Adab, P.; Li, B.; Frew, E. A Systematic Review of Methods, Study Quality, and Results of Economic Evaluation for Childhood and Adolescent Obesity Intervention. Int. J. Environ. Res. Public Health 2019, 16, 485. https://doi.org/10.3390/ijerph16030485
Zanganeh M, Adab P, Li B, Frew E. A Systematic Review of Methods, Study Quality, and Results of Economic Evaluation for Childhood and Adolescent Obesity Intervention. International Journal of Environmental Research and Public Health. 2019; 16(3):485. https://doi.org/10.3390/ijerph16030485
Chicago/Turabian StyleZanganeh, Mandana, Peymane Adab, Bai Li, and Emma Frew. 2019. "A Systematic Review of Methods, Study Quality, and Results of Economic Evaluation for Childhood and Adolescent Obesity Intervention" International Journal of Environmental Research and Public Health 16, no. 3: 485. https://doi.org/10.3390/ijerph16030485
APA StyleZanganeh, M., Adab, P., Li, B., & Frew, E. (2019). A Systematic Review of Methods, Study Quality, and Results of Economic Evaluation for Childhood and Adolescent Obesity Intervention. International Journal of Environmental Research and Public Health, 16(3), 485. https://doi.org/10.3390/ijerph16030485