Evaluation of “Healthy Learning. Together”, an Easily Applicable Mental Health Promotion Tool for Students Aged 9 to 18 Years

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
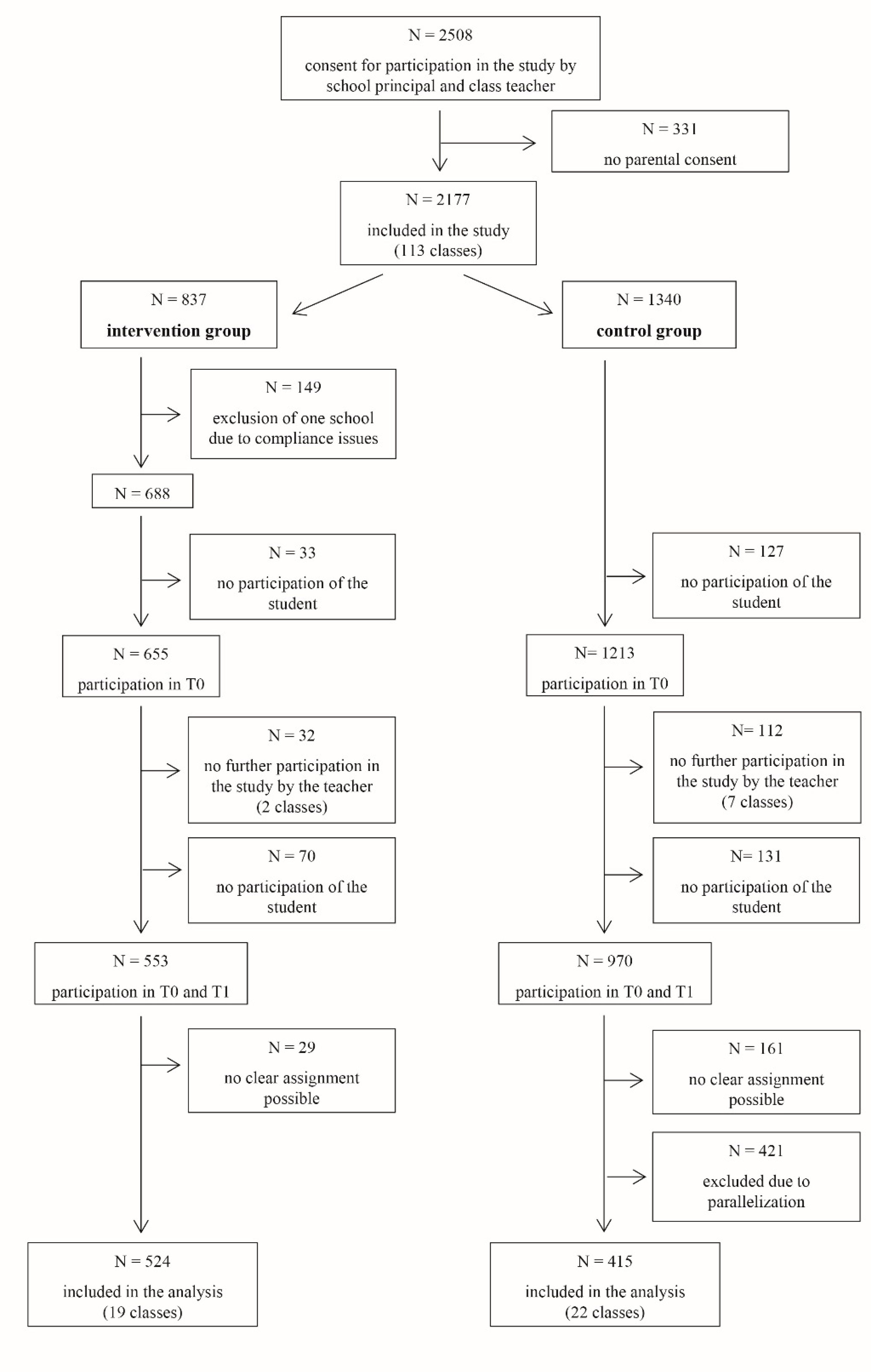
2.2. Participants
2.3. Health Promotion Tool
2.4. Measures
2.4.1. Implementation Outcomes
2.4.2. Primary and Secondary Outcomes
2.5. Statistical Procedure
3. Results
3.1. Evaluation Regarding Implementation Outcomes
3.2. Effects on Primary and Secondary Outcome Measures
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Georgiades, K.; Swendsen, J. Lifetime prevalence of mental disorders in U.S. Adolescents: Results from the national comorbidity survey replication-adolescent supplement (ncs-a). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar]
- Klasen, F.; Meyrose, A.K.; Otto, C.; Reiss, F.; Ravens-Sieberer, U. Mental problems of children and adolescents in germany results of the bella study. Mon. Schr. Kinderheilkd. 2017, 165, 402–407. [Google Scholar] [CrossRef]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Masse, L.C.; Tilert, T.; McDowell, M. Physical activity in the united states measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Daniels, S.R.; Arnett, D.K.; Eckel, R.H.; Gidding, S.S.; Hayman, L.L.; Kumanyika, S.; Robinson, T.N.; Scott, B.J.; St Jeor, S.; Williams, C.L. Overweight in children and adolescents—Pathophysiology, consequences, prevention, and treatment. Circulation 2005, 111, 1999–2012. [Google Scholar] [CrossRef] [PubMed]
- Van Geelen, S.M.; Rydelius, P.A.; Hagquist, C. Somatic symptoms and psychological concerns in a general adolescent population: Exploring the relevance of dsm-5 somatic symptom disorder. J. Psychosom. Res. 2015, 79, 251–258. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, M.; Obrosky, S.; George, C. The course of major depressive disorder from childhood to young adulthood: Recovery and recurrence in a longitudinal observational study. J. Affect. Disord. 2016, 203, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Baumeister, R.F.; Leary, M.R. The need to belong—Desire for interpersonal attachments as a fundamental human-motivation. Psychol. Bull. 1995, 117, 497–529. [Google Scholar] [CrossRef]
- Berkman, L.F.; Glass, T.; Brissette, I.; Seeman, T.E. From social integration to health: Durkheim in the new millennium. Soc. Sci. Med. 2000, 51, 843–857. [Google Scholar] [CrossRef]
- Hall-Lande, J.A.; Eisenberg, M.E.; Christenson, S.L.; Neumark-Sztainer, D. Social isolation, psychological health, and protective factors in adolescence. Adolescence 2007, 42, 265–286. [Google Scholar]
- Thoits, P.A. Mechanisms linking social ties and support to physical and mental health. J. Health Soc. Behav. 2011, 52, 145–161. [Google Scholar] [CrossRef]
- Umberson, D.; Montez, J.K. Social relationships and health: A flashpoint for health policy. J. Health Soc. Behav. 2010, 51, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Parker, J.G.; Rubin, K.H.; Erath, S.A.; Wojslawowicz, J.C.; Buskirk, A.A. Peer relationships, child development, and adjustment: A developmental psychopathology perspective. In Developmental Psychopathology: Theory and Method, Volume 1, 2nd ed.; Cicchetti, D., Cohen, D.J., Eds.; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2006. [Google Scholar]
- Lereya, S.T.; Copeland, W.E.; Costello, E.J.; Wolke, D. Adult mental health consequences of peer bullying and maltreatment in childhood: Two cohorts in two countries. Lancet Psychiatry 2015, 2, 524–531. [Google Scholar] [CrossRef]
- Carlyle, K.E.; Steinman, K.J. Demographic differences in the prevalence, co-occurrence, and correlates of adolescent bullying at school. J. Sch. Health 2007, 77, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Juvonen, J.; Gross, E.F. Extending the school grounds? Bullying experiences in cyberspace. J. Sch. Health 2008, 78, 496–505. [Google Scholar] [CrossRef]
- Quintana-Orts, C.; Rey, L. Traditional Bullying, Cyberbullying and Mental Health in Early Adolescents: Forgiveness as a Protective Factor of Peer Victimisation. Int. J. Environ. Res. Public Health 2018, 15, 2389. [Google Scholar] [CrossRef] [PubMed]
- Turner, I.; Reynolds, K.J.; Lee, E.; Subasic, E.; Bromhead, D. Well-being, school climate, and the social identity process: A latent growth model study of bullying perpetration and peer victimization. Sch. Psychol. Q. 2014, 29, 320–335. [Google Scholar] [CrossRef]
- Reyes, M.R.; Brackett, M.A.; Rivers, S.E.; White, M.; Salovey, P. Classroom emotional climate, student engagement, and academic achievement. J. Educ. Psychol. 2012, 104, 700–712. [Google Scholar] [CrossRef]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Velicer, W.F. The transtheoretical model of health behavior change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef]
- Schwarzer, R. Modeling health behavior change: How to predict and modify the adoption and maintenance of health behaviors. Appl. Psychol.-Int. Rev.-Psychol. Appl.-Rev. Int. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Van der Horst, K.; Paw, M.; Twisk, J.W.R.; Van Mechelen, W. A brief review on correlates of physical activity and sedentariness in youth. Med. Sci. Sports Exerc. 2007, 39, 1241–1250. [Google Scholar] [CrossRef] [PubMed]
- Roddenberry, A.; Renk, K. Locus of control and self-efficacy: Potential mediators of stress, illness, and utilization of health services in college students. Child Psychiat. Hum. Dev. 2010, 41, 353–370. [Google Scholar] [CrossRef] [PubMed]
- Bursch, B.; Tsao, J.C.I.; Meldrum, M.; Zeltzer, L.K. Preliminary validation of a self-efficacy scale for child functioning despite chronic pain (child and parent versions). Pain 2006, 125, 35–42. [Google Scholar] [CrossRef]
- Luszczynska, A.; Benight, C.C.; Cieslak, R. Self-efficacy and health-related outcomes of collective trauma a systematic review. Eur. Psychol. 2009, 14, 51–62. [Google Scholar] [CrossRef]
- Guerra, C.; Farkas, C.; Moncada, L. Depression, anxiety and ptsd in sexually abused adolescents: Association with self-efficacy, coping and family support. Child Abuse Negl. 2018, 76, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Raknes, S.; Pallesen, S.; Bjaastad, J.F.; Wergeland, G.J.; Hoffart, A.; Dyregrov, K.; Haland, A.T.; Haugland, B.S.M. Negative life events, social support, and self-efficacy in anxious adolescents. Psychol. Rep. 2017, 120, 609–626. [Google Scholar] [CrossRef]
- Otto, C.; Haller, A.C.; Klasen, F.; Holing, H.; Bullinger, M.; Ravens-Sieberer, U.; BELLA Study Group. Risk and protective factors of health-related quality of life in children and adolescents: Results of the longitudinal bella study. PLoS ONE 2017, 12, e0190363. [Google Scholar] [CrossRef]
- Orlando, M.; Ellickson, P.L.; McCaffrey, D.F.; Longshore, D.L. Mediation analysis of a school-based drug prevention program: Effects of project alert. Prev. Sci. 2005, 6, 35–46. [Google Scholar] [CrossRef]
- Possel, P.; Baldus, C.; Horn, A.B.; Groen, G.; Hautzinger, M. Influence of general self-efficacy on the effects of a school-based universal primary prevention program of depressive symptoms in adolescents: A randomized and controlled follow-up study. J. Child Psychol. Psychiatry 2005, 46, 982–994. [Google Scholar] [CrossRef]
- McAllister, M.; Knight, B.A.; Hasking, P.; Withyman, C.; Dawkins, J. Building resilience in regional youth: Impacts of a universal mental health promotion programme. Int. J. Ment. Health Nurs. 2018, 27, 1044–1054. [Google Scholar] [CrossRef]
- Barry, M.M.; Clarke, A.M.; Jenkins, R.; Patel, V. A systematic review of the effectiveness of mental health promotion interventions for young people in low and middle income countries. BMC Public Health 2013, 13, 19. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, M.; Svirydzenka, N.; Adams, S.; Dogra, N. Review of mental health promotion interventions in schools. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 647–662. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, C.A.; Dyson, J.; Cowdell, F.; Watson, R. Do universal school-based mental health promotion programmes improve the mental health and emotional wellbeing of young people? A literature review. J. Clin. Nurs. 2018, 27, e412–e426. [Google Scholar] [CrossRef] [PubMed]
- Chilton, R.; Pearson, M.; Anderson, R. Health promotion in schools: A scoping review of systematic reviews. Health Educ. 2015, 115, 357–376. [Google Scholar] [CrossRef]
- Wenzel, V.; Weichold, K.; Silbereisen, R.K. The life skills program ipsy: Positive influences on school bonding and prevention of substance misuse. J. Adolesc. 2009, 32, 1391–1401. [Google Scholar] [CrossRef] [PubMed]
- Eisen, M.; Zellman, G.L.; Murray, D.M. Evaluating the lions-quest “skills for adolescence” drug education program—Second-year behavior outcomes. Addict. Behav. 2003, 28, 883–897. [Google Scholar] [CrossRef]
- Dishman, R.K.; Motl, R.W.; Saunders, R.; Felton, G.; Ward, D.S.; Dowda, M.; Pate, R.R. Self-efficacy partially mediates the effect of a school-based physical-activity intervention among adolescent girls. Prev. Med. 2004, 38, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Vreeman, R.C.; Carroll, A.E. A systematic review of school-based interventions to prevent bullying. Arch. Pediatr. Adolesc. Med. 2007, 161, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Gol-Guven, M. The effectiveness of the lions quest program: Skills for growing on school climate, students’ behaviors, perceptions of school, and conflict resolution skills. Eur. Early Child. Educ. 2017, 25, 575–594. [Google Scholar] [CrossRef]
- Franze, M.; Paulus, P. Mindmatters—A programme for the promotion of mental health in primary and secondary schools: Results of an evaluation of the german language adaptation. Health Educ. 2009, 109, 369–379. [Google Scholar] [CrossRef]
- Nielsen, L.; Meilstrup, C.; Nelausen, M.K.; Koushede, V.; Holstein, B.E. Promotion of social and emotional competence experiences from a mental health intervention applying a whole school approach. Health Educ. 2015, 115, 339–356. [Google Scholar] [CrossRef]
- Barry, M.M.; Clarke, A.M.; Dowling, K. Promoting social and emotional well-being in schools. Health Educ. 2017, 117, 434–451. [Google Scholar] [CrossRef]
- Rivers, S.E.; Brackett, M.A.; Reyes, M.R.; Elbertson, N.A.; Salovey, P. Improving the social and emotional climate of classrooms: A clustered randomized controlled trial testing the ruler approach. Prev. Sci. 2013, 14, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Blank, L.; Baxter, S.K.; Payne, N.; Guillaume, L.R.; Pilgrim, H. Systematic review and narrative synthesis of the effectiveness of contraceptive service interventions for young people, delivered in educational settings. J. Pediatr. Adol. Gynecol. 2010, 23, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Han, S.S.; Weiss, B. Sustainability of teacher implementation of school-based mental health programs. J. Abnorm. Child Psychol. 2005, 33, 665–679. [Google Scholar] [CrossRef]
- Robert Koch-Institut. Gesundheit in Deutschland. Gesundheitsberichterstattung des Bundes. Gemeinsam getragen von RKI und Destatis; RKI: Berlin, Germany, 2016. [Google Scholar]
- Wick, K.; Gläser, A.; Berger, U.; Strauß, B.; Schwager, S. Process evaluation of the card set “Healthy learning. Together”. Prevention tool to improve social integration and self-efficacy in secondary schools. Psychotherapeut 2019, 64, 23–30. [Google Scholar] [CrossRef]
- Schwager, S.; Gläser, A.; Wick, K.; Strauss, B.; Berger, U. Healthy learning. Together. Development of a tool for schools to prevent psychological problems among children and adolescents. Präv. Gesundheitsf. 2018. [Google Scholar] [CrossRef]
- Gottfredson, D.C.; Cook, T.D.; Gardner, F.E.M.; Gorman-Smith, D.; Howe, G.W.; Sandler, I.N.; Zafft, K.M. Standards of evidence for efficacy, effectiveness, and scale-up research in prevention science: Next generation. Prev. Sci. 2015, 16, 893–926. [Google Scholar] [CrossRef]
- Stuart, E.A. Matching methods for causal inference: A review and a look forward. Stat. Sci. 2010, 25, 1–21. [Google Scholar] [CrossRef]
- Dane, A.V.; Schneider, B.H. Program integrity in primary and early secondary prevention: Are implementation effects out of control. Clin. Psychol. Rev. 1998, 18, 23–45. [Google Scholar] [CrossRef]
- Haeberlin, U.; Moser, U.; Bless, G.; Klaghofer, R. Integration in die Schulklasse. Fragebogen zur Erfassung von Dimensionen der Integration von Schülern FDI 4-6; Haupt: Bern, Switzerland, 1989; pp. 4–6. [Google Scholar]
- Eder, F.; Mayr, J. Linzer Fragebogen zum Schul-und Klassenklima für die 4.-8. Klasse:(lfsk 4-8); Hogrefe: Göttingen, Germany, 2000. [Google Scholar]
- Schwarzer, R.; Jerusalem, M. Generalized self-efficacy scale. In Measures in Health Psychology: A User’s Portfolio. Causal and Control Beliefs; Weinman, J., Wright, S., Johnston, M., Eds.; NFER-NELSON: Windsor, UK, 1995; pp. 35–37. [Google Scholar]
- Bullinger, M.; Brutt, A.L.; Erhart, M.; Ravens-Sieberer, U. Psychometric properties of the kindl-r questionnaire: Results of the bella study. Eur. Child Adolesc. Psychiatry 2008, 17, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Little, R.J.; Rubin, D.B. Statistical Analysis with Missing Data, 2nd ed.; Wiley: Hoboken, NJ, USA, 2002; pp. XV, 381S. [Google Scholar]
- Maxwell, S.E.; Delaney, H.D. Designing Experiments and Analyzing Data: A Model Comparison Perspective; Wadsworth: Pacific Grove, CA, USA, 1990. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: Hillsdale, NJ, USA, 1988; p. xxi. 567p. [Google Scholar]
- Olweus, D.; Limber, S.P. Bullying in school: Evaluation and dissemination of the olweus bullying prevention program. Am. J. Orthopsychiatry 2010, 80, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Durlak, J.A.; DuPre, E.P. Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. Am. J. Community Psychol. 2008, 41, 327–350. [Google Scholar] [CrossRef] [PubMed]
- León-del-Barco, B.; Fajardo-Bullón, F.; Mendo-Lázaro, S.; Rasskin-Gutman, I.; Iglesias-Gallego, D. Impact of the Familiar Environment in 11–14-Year-Old Minors’ Mental Health. Int. J. Environ. Res. Public Health 2018, 15, 1314. [Google Scholar] [CrossRef]
- George, D.; Mallery, P. SPSS for Windows Step by Step: A Simple Guide and Reference 11.0 Update, 4th ed.; Allyn & Bacon: Boston, MA, USA, 2003. [Google Scholar]
- Van Genugten, L.; Dusseldorp, E.; Massey, E.K.; van Empelen, P. Effective self-regulation change techniques to promote mental wellbeing among adolescents: A meta-analysis. Health Psychol. Rev. 2017, 11, 53–71. [Google Scholar] [CrossRef] [PubMed]
- Buhler, A. Meta-analysis on the effectiveness of german life skills programs in substance abuse prevention. Kindh. Entwickl. 2016, 25, 175–188. [Google Scholar]
- Weare, K.; Nind, M. Mental health promotion and problem prevention in schools: What does the evidence say? Health Promot. Int. 2011, 26, I29–I69. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy—Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Cummins, R.A.; Li, N.; Wooden, M.; Stokes, M. A demonstration of set-points for subjective wellbeing. J. Happiness Stud. 2014, 15, 183–206. [Google Scholar] [CrossRef]
- Chapman, R.L.; Buckley, L.; Sheehan, M.; Shochet, I. School-based programs for increasing connectedness and reducing risk behavior: A systematic review. Educ. Psychol. Rev. 2013, 25, 95–114. [Google Scholar] [CrossRef]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescent health 2 adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Intervention Group (N = 524) | Control Group (N = 415) | Group Difference |
|---|---|---|---|
| Sociodemographic variables (T1) | |||
| Age (years), M (SD) | 12.52 (1.67) | 12.60 (2.01) | t(936) = 0.67, p = .503 |
| Sex (female) | 57.9% | 58.5% | t(833) = 0.17, p = .862 |
| School type * | Secondary: 13.5% Comprehensive: 55.3% Grammar: 31.1% | Secondary: 17.1% Comprehensive: 53.3% Grammar: 29.6% | χ2(2) = 2.29, p = .318 |
| Baseline scores | |||
| Class climate, M (SD) | 2.03 (0.53) | 2.03 (0.51) | t(929) = 0.18, p = .855 |
| Social integration, M (SD) | 2.42 (0.57) | 2.44 (0.55) | t(931) = 0.39, p = .700 |
| Self-efficacy, M (SD) | 1.90 (0.45) | 1.91 (0.45) | t(926) = 0.32, p = .750 |
| Mental wellbeing, M (SD) | 3.08 (0.60) | 3.09 (0.59) | t(937) = 0.22, p = .830 |
| Physical wellbeing, M (SD) | 2.68 (0.70) | 2.66 (0.71) | t(937) = −0.57, p = .572 |
| Aspect of Implementation | Source | n Positive Evaluations | n Neutral Evaluations | n Negative Evaluations | Example Positive Evaluation | Example Neutral Evaluation | Example Negative Evaluation |
|---|---|---|---|---|---|---|---|
| adherence | teacher interviews | 10 | 2 | 4 | “It was very clear to me (…) and the tool was easy to use.” | “It was difficult to find the right time for the poster exhibition, so I asked students to visit it on their own.” | “I did not use every exercise exactly as instructed as the students were a little too tired for them.” |
| exposure | teacher interviews | 4 | 0 | 6 | “I implemented many games, especially during the first week and until the holidays.” | Not applicable | “Well, I did not manage to do everything (every exercise), because somehow something different always comes up in school.” |
| quality of delivery | teacher interviews | 25 | 4 | 7 | “(I liked) that it had different exercises and that the students actually slowly opened up.” | “Well a few (exercises) were questionable, where I needed more space in my class room. And I have a room, where the tables are fixed, so I was limited regarding the exercises from the beginning.” | “I think for the teenagers it was really cool, but for the younger ones it (the poster exhibition) was a bit scary sometimes.” |
| participant responsive-ness | student interviews | 145 | 44 | 14 | “Yeah, I mean, that kind of project brought the class closer together somehow.” | “Some (exercises) were not bad, but I think they did not do that much for us now.” | “Many classmates did not take it seriously.” |
| Outcome Measure | Mean Change Score Control Group (SD in Parentheses) | Mean Change Score Intervention Group (SD in Parentheses) | F-Value | df | p-Value (One-Tailed) | Effect Size η2partial |
|---|---|---|---|---|---|---|
| Results for the whole sample | ||||||
| Primary outcomes | ||||||
| Class climate | −0.056 (0.423) | −0.002 (0.422) | 3.857 | 1, 920 | .025 * | .004 |
| Social integration | −0.014 (0.617) | 0.033 (0.600) | 0.936 | 1, 849 | .167 | .001 |
| Self-efficacy | −0.003 (0.455) | 0.042 (0.538) | 1.520 | 1, 520 | .109 | .002 |
| Secondary outcomes | ||||||
| Physical wellbeing | −0.133 (0.721) | −0.097 (0.746) | 1.426 | 1, 934 | .117 | .002 |
| Mental wellbeing | −0.006 (0.530) | −0.008 (0.557) | 0.000 | 1, 933 | .495 | .000 |
| Results for the sub-sample with a minimum of 15 exercises. | ||||||
| Primary outcomes | ||||||
| Class climate | −0.056 (0.423) | 0.026 (0.419) | 4.702 | 1, 598 | .016 * | .008 |
| Social integration | −0.014 (0.617) | 0.061 (0.609) | 3.626 | 1, 547 | .029 * | .007 |
| Self-efficacy | −0.003 (0.455) | 0.071 (0.502) | 2.906 | 1, 558 | .045 * | .005 |
| Secondary outcomes | ||||||
| Physical wellbeing | −0.133 (0.721) | −0.028 (0.725) | 2.256 | 1, 606 | .067 | .004 |
| Mental wellbeing | −0.006 (0.530) | .051 (0.561) | 2.592 | 1, 607 | .054 | 0.004 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwager, S.; Berger, U.; Glaeser, A.; Strauss, B.; Wick, K. Evaluation of “Healthy Learning. Together”, an Easily Applicable Mental Health Promotion Tool for Students Aged 9 to 18 Years. Int. J. Environ. Res. Public Health 2019, 16, 487. https://doi.org/10.3390/ijerph16030487
Schwager S, Berger U, Glaeser A, Strauss B, Wick K. Evaluation of “Healthy Learning. Together”, an Easily Applicable Mental Health Promotion Tool for Students Aged 9 to 18 Years. International Journal of Environmental Research and Public Health. 2019; 16(3):487. https://doi.org/10.3390/ijerph16030487
Chicago/Turabian StyleSchwager, Susanne, Uwe Berger, Anni Glaeser, Bernhard Strauss, and Katharina Wick. 2019. "Evaluation of “Healthy Learning. Together”, an Easily Applicable Mental Health Promotion Tool for Students Aged 9 to 18 Years" International Journal of Environmental Research and Public Health 16, no. 3: 487. https://doi.org/10.3390/ijerph16030487
APA StyleSchwager, S., Berger, U., Glaeser, A., Strauss, B., & Wick, K. (2019). Evaluation of “Healthy Learning. Together”, an Easily Applicable Mental Health Promotion Tool for Students Aged 9 to 18 Years. International Journal of Environmental Research and Public Health, 16(3), 487. https://doi.org/10.3390/ijerph16030487