Promoting Healthcare Sustainability in Developing Countries: Analysis of Knowledge Management Drivers in Public and Private Hospitals of Pakistan


 ,
,
Abstract
:1. Introduction
2. Theoretical Perspective
2.1. Knowledge Management and Healthcare
2.2. Knowledge Management Implementation in Pakisani Healthcare
2.3. Drivers of KM in the Healthcare
3. Research Methodology
3.1. Fuzzy Delphi Method (FDM)
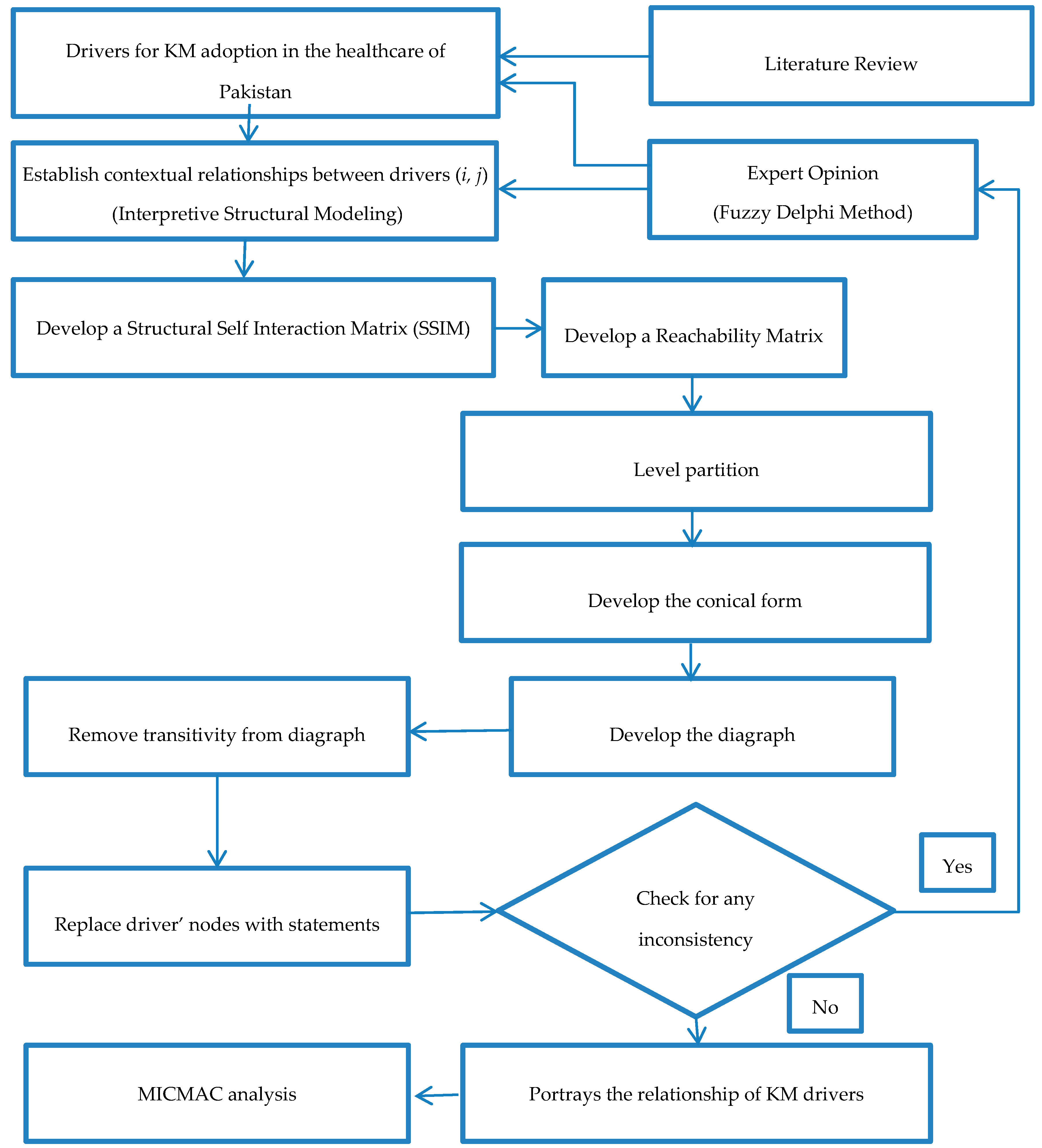
3.2. Interpretive Structural Analysis (ISM)
- Step
- 1: Identifying the drivers of KM for healthcare through literature review.
- Step
- 2: Developing the structural self-interaction matrix (SSIM), which establishes a pair-wise contextual relationship between the drivers.
- Step
- 3: Developing the initial reachability matrix (IRM) by converting the values of SSIM to binary digits (0 and 1).
- Step
- 4: Developing the final reachability matrix (FRM) by removing the transitivity from the IRM.
- Step
- 5: Establishing Level partition to create levels.
- Step
- 6: Convert the level partition into the conical form.
- Step
- 7: Develop the ISM model on the basis of a conical form.
- Step
- 8: Check the model for inconsistency, and to restructure in case of errors.
- Step
- 9: Perform the MICMAC analysis according to the driving and dependence power of each driver.
3.2.1. Structural Self-Interaction Matrix (SSIM)
- V shows that i influences j
- A shows that j influences i
- X shows that i and j both influence each other
- O shows that i and j are unrelated
3.2.2. Initial Reachability Matrix (IRM)
- If (i, j) is represented with V in the SSIM, then the entry for (i, j) in IRM would be 1 and entry for (j, i) would be 0
- If (i, j) is represented with A in the SSIM, then the entry for (i, j) in IRM would be 0 and entry for (j, i) would be 1
- If (i, j) is represented with X in the SSIM, then the entry for both (i, j) and (j, i) in IRM would be 1
- If (i, j) is represented with X in the SSIM, then the entry for both (i, j) and (j, i) in IRM would be 0
3.2.3. Final Reachability Matrix (FRM)
3.2.4. Level Partitions
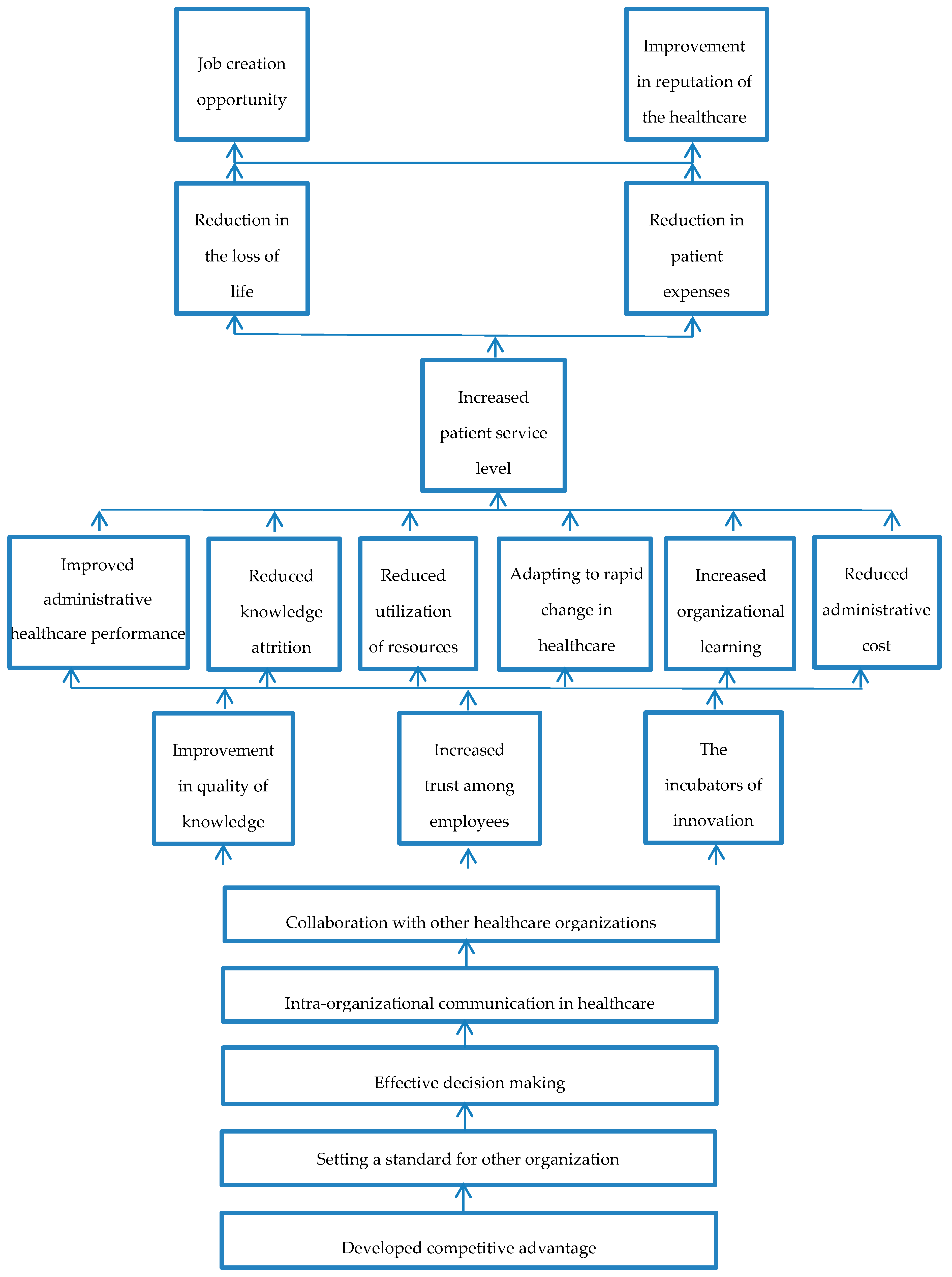
3.2.5. ISM Model
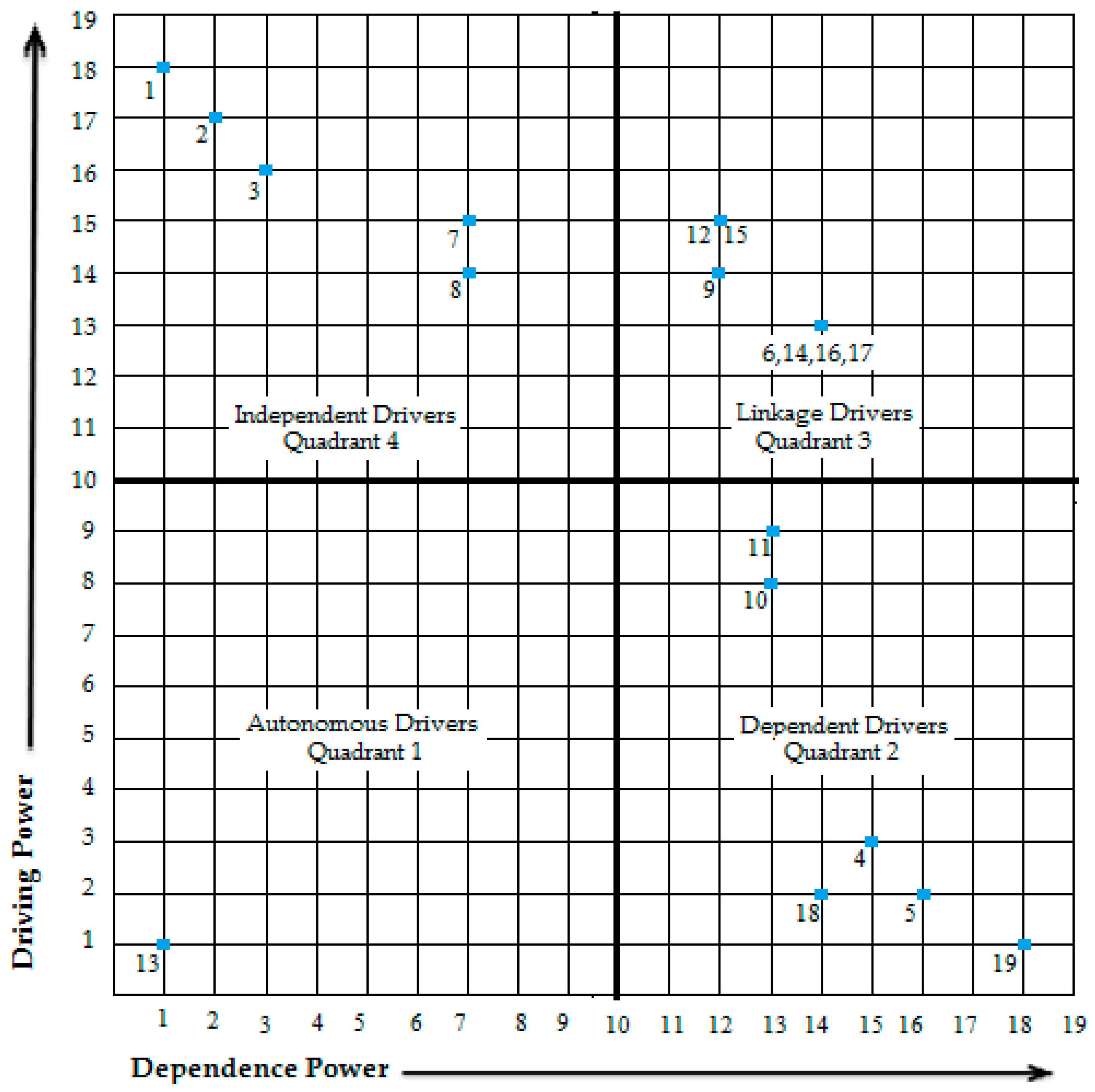
3.3. MICMAC Analysis
- Autonomous Drivers (Quadrant 1): These are the drivers that have weak driving and dependence power. They generally have little to no influence.
- Dependent Drivers (Quadrant 2): These are the drivers that have weak driving but strong dependence power.
- Linkage Drivers (Quadrant 3): These are the drivers that have strong driving and dependence power. These drivers are very active; an action on one will result in a change in the other.
- Independent Drivers (Quadrant 4): These are the drivers that have strong driving but weak dependence power.
4. Results and Discussion
- Autonomous Drivers: There is only one driver in this quadrant, which is driver 13 (job creation). This driver has weak driving and dependence power, showing that it is relatively less important. The presence of only one enabler in this quadrant proves that the other 18 drivers have more contribution in influencing the system.
- Dependent Driver: There are six drivers in this quadrant, drivers 4 (increased patient service level), 5 (reduction in the loss of life), 10 (reduced knowledge attrition), 11 (reduced utilization of resources), 18 (reduction in patient expenses), and 19 (improvement in reputation of the healthcare). These drivers have a weak driving but strong dependence power; they cannot influence other drivers.
- Linkage Drivers: There are seven drivers in this quadrant, drivers 6 (improved administrative healthcare performance), 9 (improvement in quality of knowledge), 12 (increased trust among employees), 14 (adapting to rapid change in healthcare globally), 15 (the incubators of innovation), 16 (increased organizational learning), and 17 (reduced administrative cost). These drivers have strong driving and dependence power. These are amongst the main drivers, the pursuance of one driver will automatically activate the other drivers to help and show benefits.
- Independent Drivers: These are the key drivers, there are five drivers in this quadrant, drivers 1 (developed competitive advantage), 2 (setting a standard for other organizations), 3 (effective decision making), 7 (intra-organizational communication in healthcare), and 8 (collaboration with other healthcare organizations). These drivers have strong driving but weak dependence power. These are the main reason for Pakistan implementing KM in its health sector.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Karamat, J.; Shurong, T.; Ahmad, N.; Afridi, S.; Khan, S.; Mahmood, K. Enablers Supporting the Implementation of Knowledge Management in the Healthcare of Pakistan. Int. J. Environ. Res. Public Health 2018, 15, 2816. [Google Scholar] [CrossRef] [PubMed]
- Fineberg, H.V. A successful and sustainable health system—How to get there from here. N. Engl. J. Med. 2012, 366, 1020–1027. [Google Scholar] [CrossRef] [PubMed]
- Coulson-Thomas, C. Transforming Knowledge Management: A Quicker and Affordable Route to High Performance Organisations; Policy Publications: Peterborough, UK, 2013. [Google Scholar]
- Yahya, S.; Goh, W.K. Managing human resources toward achieving knowledge management. J. Knowl. Manag. 2002, 6, 457–468. [Google Scholar] [CrossRef]
- Andreeva, T.; Kianto, A. Does knowledge management really matter? Linking knowledge management practices, competitiveness and economic performance. J. Knowl. Manag. 2012, 16, 617–636. [Google Scholar] [CrossRef] [Green Version]
- Rastogi, P.N. Knowledge management and intellectual capital—The new virtuous reality of competitiveness. Hum. Syst. Manag. 2000, 19, 39–48. [Google Scholar]
- Mao, H.; Liu, S.; Zhang, J.; Deng, Z. Information technology resource, knowledge management capability, and competitive advantage: The moderating role of resource commitment. Int. J. Inf. Manag. 2016, 36, 1062–1074. [Google Scholar] [CrossRef]
- El Morr, C.; Subercaze, J. Knowledge management in healthcare. In Handbook of Research on Developments in E-Health and Telemedicine: Technological and Social Perspectives; IGI Global: Hershey, PA, USA, 2010; pp. 490–510. [Google Scholar]
- Havens, C.; Knapp, E. Easing into knowledge management. Strategy Leadership 1999, 27, 4–9. [Google Scholar] [CrossRef]
- Guptill, J. Knowledge management in health care. J. Health Care Financ. 2005, 31, 10–14. [Google Scholar]
- Wenger, E. Communities of Practice, a Brief Introduction. 2006. Available online: http://www.leader-values.com/content/detail.asp?contentdetailid=991 (accessed on 25 December 2018).
- Sharma, S.K.; Wickramasinghe, N.; Gupta, J.N. Knowledge management in healthcare. In Creating Knowledge-Based Healthcare Organizations; IGI Global: Hershey, PA, USA, 2005; pp. 1–13. [Google Scholar]
- Tricco, A.C.; Ashoor, H.M.; Cardoso, R.; MacDonald, H.; Cogo, E.; Kastner, M.; Perrier, L.; McKibbon, A.; Grimshaw, J.M.; Straus, S.E. Sustainability of knowledge translation interventions in healthcare decision-making: A scoping review. Implement. Sci. 2016, 11, 55. [Google Scholar] [CrossRef]
- Sackett, D.L.; Rosenberg, W.M.; Gray, J.M.; Haynes, R.B.; Richardson, W.S. Evidence Based Medicine: What It Is and What It Isn’t; British Medical Journal Publishing Group: Oxford, UK, 1996; pp. 71–72. [Google Scholar]
- Goldsmith, J.C. Digital Medicine: Implications for Healthcare Leaders, 1st ed.; Health Administration Press: Chicago, IL, USA, 2003. [Google Scholar]
- Bose, R. Knowledge management-enabled health care management systems: Capabilities, infrastructure, and decision-support. Expert Syst. Appl. 2003, 24, 59–71. [Google Scholar] [CrossRef]
- Yaghoubi, M.; Karimi, S.; Javadi, M.; Nikbakht, A. A correlation study on organization learning and knowledge management in staffs in selected hospitals of Isfahan University of Medical Sciences. J. Health Admin. 2011, 13, 65–74. [Google Scholar]
- Hojabri, R.; Eftekhar, F.; Sharifi, M.; Hatamian, A. Knowledge Management in an Iranian Health organization: Investigation of Critical Success Factors. J. Ind. Distrib. Bus. 2014, 5, 31–42. [Google Scholar] [CrossRef]
- Karami, M.; Piri, Z. From clinical coding to knowledge management in healthcare organizations. Health Inf. Manag. 2007, 4, 239–247. [Google Scholar]
- WHO. Country Cooperation Strategy at a Glance, Pakistan. 2017. Available online: http://apps.who.int/iris/bitstream/handle/10665/136607/ccsbrief_pak_en.pdf?sequence=1 (accessed on 25 August 2018).
- World Fact Book. 2016. Available online: https://www.cia.gov/library/publications/download/download-2016/index.html (accessed on 25 August 2018).
- Akram, M.; Khan, F.J. Health Care Services and Government Spending in Pakistan. 2007. Available online: www.pide.org.pk/pdf/Working%20Paper/WorkingPaper-32.pdf (accessed on 1 September 2018).
- Malik, M.A.; Gul, W.; Abrejo, F. Cost of primary health care in Pakistan. J. Ayub. Med. Coll. Abbottabad 2015, 27, 88. [Google Scholar] [PubMed]
- Weerawardena, J.; McDonald, R.E.; Mort, G.S. Sustainability of nonprofit organizations: An empirical investigation. J. World Bus. 2010, 45, 346–356. [Google Scholar] [CrossRef]
- Talib, F.; Rahman, Z. An interpretive structural modelling for sustainable healthcare quality dimensions in hospital services. Int. J. Qual. Res. Serv. 2015, 2, 28–46. [Google Scholar] [CrossRef]
- Raj, T.; Shankar, R.; Suhaib, M. An ISM approach for modelling the enablers of flexible manufacturing system: The case for India. Int. J. Prod. Res. 2008, 46, 6883–6912. [Google Scholar] [CrossRef]
- Poduval, P.S.; Pramod, V. Interpretive structural modeling (ISM) and its application in analyzing factors inhibiting implementation of total productive maintenance (TPM). Int. J. Qual. Reliab. Manag. 2015, 32, 308–331. [Google Scholar] [CrossRef]
- Mathiyazhagan, K.; Govindan, K.; NoorulHaq, A.; Geng, Y. An ISM approach for the barrier analysis in implementing green supply chain management. J. Clean. Prod. 2013, 47, 283–297. [Google Scholar] [CrossRef]
- Shibin, K.; Gunasekaran, A.; Papadopoulos, T.; Dubey, R.; Singh, M.; Wamba, S.F. Enablers and barriers of flexible green supply chain management: A total interpretive structural modeling approach. Glob. J. Flexib. Syst. Manag. 2016, 17, 171–188. [Google Scholar] [CrossRef]
- Talib, F.; Rahman, Z.; Qureshi, M. An Interpretive Structural Modelling (ISM) Approach for Modelling the Practices of Total Quality Management in Service Sector. Int. J. Model. Oper. Manag. 2011, 1, 223–250. [Google Scholar]
- Khanam, S.; Siddiqui, J.; Talib, F. Modeling the TQM enablers and IT resources in the ICT industry: An ISM-MICMAC approach. Int. J. Inf. Syst. Manag. 2016, 1, 195–218. [Google Scholar]
- Kannan, G.; Pokharel, S.; Kumar, P.S. A hybrid approach using ISM and fuzzy TOPSIS for the selection of reverse logistics provider. Resour. Conserv. Recycl. 2009, 54, 28–36. [Google Scholar] [CrossRef]
- Waqas, M.; Dong, Q.-l.; Ahmad, N.; Zhu, Y.; Nadeem, M. Critical Barriers to Implementation of Reverse Logistics in the Manufacturing Industry: A Case Study of a Developing Country. Sustainability 2018, 10, 4202. [Google Scholar] [CrossRef]
- Lim, M.K.; Tseng, M.-L.; Tan, K.H.; Bui, T.D. Knowledge management in sustainable supply chain management: Improving performance through an interpretive structural modelling approach. J. Clean. Prod. 2017, 162, 806–816. [Google Scholar] [CrossRef]
- Karamat, J.; Shurong, T.; Ahmad, N.; Waheed, A.; Khan, S. Barriers to Knowledge Management in the Health Sector of Pakistan. Sustainability 2018, 10, 4155. [Google Scholar] [CrossRef]
- Shahbandarzadeh, H.; Ghorbanpour, A. The applying ISM/FANP approach for appropriate location selection of health centers. Iranian J. Manag. Stud. 2011, 4, 5–28. [Google Scholar]
- Debata, B.R.; Sree, K.; Patnaik, B.; Mahapatra, S.S. Evaluating medical tourism enablers with interpretive structural modeling. Benchmarking 2013, 20, 716–743. [Google Scholar] [CrossRef]
- Despres, C.; Chauvel, D. Knowledge management(s). J. Knowl. Manag. 1999, 3, 110–123. [Google Scholar] [CrossRef]
- Nonaka, I. A dynamic theory of organizational knowledge creation. Organ. Sci. 1994, 5, 14–37. [Google Scholar] [CrossRef]
- Wathne, K.; Roos, J.; von Krogh, G. Towards a theory of knowledge transfer in a cooperative context. In Managing Knowledge-Perspectives on Cooperation and Competition; 1996; pp. 55–81. [Google Scholar]
- Owen, J.M. Knowledge management and the information professional. Inf. Serv. Use 1999, 19, 7–16. [Google Scholar] [CrossRef]
- Desouza, K.C. Managing Knowledge with Artificial Intelligence: An Introduction with Guidelines for Nonspecialists; Greenwood Publishing Group: Westport, CT, USA, 2002. [Google Scholar]
- Shih, D.-H.; Lu, C.-M.; Lee, C.-H.; Parng, Y.-J.; Wu, K.-J.; Tseng, M.-L. A Strategic Knowledge Management Approach to Circular Agribusiness. Sustainability 2018, 10, 2389. [Google Scholar] [CrossRef]
- Nonaka, I.; Takeuchi, H. The knowledge-creating company. Harv. Bus. Rev. 2007, 85, 162. [Google Scholar]
- Sveiby, K.-E. Transfer of knowledge and the information processing professions. Eur. Manag. J. 1996, 14, 379–388. [Google Scholar] [CrossRef]
- Weed, L.L. New connections between medical knowledge and patient care. BMJ 1997, 315, 231–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pakistan Bureau of Statistics. 6th Population and Housing Census 2017. Available online: www.pbscensus.gov.pk (accessed on 1 November 2018).
- Rana, S. Pakistan Is Now a $300-Billion Economy. The Express Tribune, 18 May 2017. [Google Scholar]
- WHO. The World Health Report. 2000. Available online: https://www.who.int/whr/2000/en/whr00_en.pdf?ua=1 (accessed on 1 November 2018).
- Evaluation. 2017, Pakistan Diseases. Available online: https://vizhub.healthdata.org/gbd-compare/ (accessed on 4 November 2018).
- WHO. World Health Statistics 2016: Monitoring Health for the SDGs. 2016. Available online: https://www.who.int/gho/publications/world_health_statistics/2016/en/ (accessed on 3 November 2018).
- Hersh, W.R.; Lunin, L.F. Perspectives on medical informatics: Information technology in health care. Introduction and overview. J. Am. Soc. Infrastruct. Sci. 1995, 44, 726–727. [Google Scholar]
- Smith, R. What clinical information do doctors need? Br. Med. J. 1996, 313, 1062–1068. [Google Scholar] [CrossRef] [Green Version]
- Rasheed, S.; Butlin, R.; Boots, M. A review of dengue as an emerging disease in Pakistan. Public Health 2013, 127, 11–17. [Google Scholar] [CrossRef]
- Heathfield, H.; Louw, G. New challenges for clinical informatics: Knowledge management tools. Health Inform. J. 1999, 5, 67–73. [Google Scholar] [CrossRef]
- National Health Vision 2016–2025. Available online: http://www.nationalplanningcycles.org/sites/default/files/planning_cycle_repository/pakistan/national_health_vision_2016-25_30-08-2016.pdf (accessed on 25 September 2018).
- Du Plessis, M. Drivers of knowledge management in the corporate environment. Int. J. Inf. Manag. 2005, 25, 193–202. [Google Scholar] [CrossRef]
- Du Plessis, M. The strategic drivers and objectives of communities of practice as vehicles for knowledge management in small and medium enterprises. Int. J. Inf. Manag. 2008, 28, 61–67. [Google Scholar] [CrossRef]
- Lee, H.; Choi, B. Knowledge management enablers, processes, and organizational performance: An integrative view and empirical examination. J. Manag. Inf. Syst. 2003, 20, 179–228. [Google Scholar]
- Du Plessis, M. The role of knowledge management in innovation. J. Knowl. Manag. 2007, 11, 20–29. [Google Scholar] [CrossRef] [Green Version]
- Yu, S.-H.; Kim, Y.-G.; Kim, M.-Y. Linking organizational knowledge management drivers to knowledge management performance: An exploratory study. In Proceedings of the 37th Annual Hawaii International Conference on System Sciences, Big Island, HI, USA, 5–8 January 2004; p. 10. [Google Scholar]
- Davenport, T.H.; de Long, D.W.; Beers, M.C. Successful knowledge management projects. Sloan Manag. Rev. 1998, 39, 43–57. [Google Scholar]
- Darko, A.; Chan, A.P.C.; Yang, Y.; Shan, M.; He, B.-J.; Gou, Z. Influences of barriers, drivers, and promotion strategies on green building technologies adoption in developing countries: The Ghanaian case. J. Clean. Prod. 2018, 200, 687–703. [Google Scholar] [CrossRef]
- Yu, D. Building the Knowledge Advantage. 1999. Available online: http://www.pwcglobal.com/extweb/newcolth.nsf/DocID/D68D5EE66EDBFE828525679F0050D362 (accessed on 20 November 2018).
- Parlby, D.; Taylor, R. The Power of Knowledge: A Business Guide to Knowledge Management. 2000. Available online: http://www.kpmgconsulting.com/index.html (accessed on 28 November 2018).
- Bontis, N. There’s a price on your head: Managing intellectual capital strategically. Bus. Q. 1996, 60, 40–78. [Google Scholar]
- Ernst, Y. A Blueprint for Success: How to Put Knowledge to Work in Your Organization. 1999. Available online: http://www.ey.com (accessed on 21 November 2018).
- Shabbir, S.; Kaufmann, H.R.; Shehzad, M. Service quality, word of mouth and trust: Drivers to achieve patient satisfaction. Sci. Res. Essays 2010, 5, 2457–2462. [Google Scholar]
- Andaleeb, S.S. Service quality perceptions and patient satisfaction: A study of hospitals in a developing country. Soc. Sci. Med. 2001, 52, 1359–1370. [Google Scholar] [CrossRef]
- Mudge, A. Knowledge Management: Do we know that we know? Commun. World 1999, 16, 24–27. [Google Scholar]
- Martiny, M. Knowledge management at HP consulting. Organ. Dyn. 1998, 27, 71–78. [Google Scholar] [CrossRef]
- Caldwell, F. Knowledge Management Risk Analysis Framework. 1999. Available online: http://gartner4.gartnerweb.com:80/gg/purchase/0/00/853/52/doc/00085352/ (accessed on 19 November 2018).
- Bjørnson, F.O.; Dingsøyr, T. Knowledge management in software engineering: A systematic review of studied concepts, findings and research methods used. Inf. Softw. Technol. 2008, 50, 1055–1068. [Google Scholar] [CrossRef]
- Zack, M.H. Managing codified knowledge. Sloan Manag. Rev. 1999, 40, 45–58. [Google Scholar]
- Hargadon, A.; Sutton, R.I. Building an innovation factory. Harv. Bus. Rev. 2000, 78, 157–166. [Google Scholar] [PubMed]
- Greco, J. Knowledge Is Power. 1999. Available online: http://web7.infotrac.london.galegroup.com/itw/infomark/482/356/72858976w3/purl=rcl_GBI-M_0_A54293713&dyn=30!xrn_10_0_A54293713?sw_aep=up_itw (accessed on 16 November 2018).
- Luxford, K.; Safran, D.G.; Delbanco, T. Promoting patient-centered care: A qualitative study of facilitators and barriers in healthcare organizations with a reputation for improving the patient experience. Int. J. Qual. Health Care 2011, 23, 510–515. [Google Scholar] [CrossRef]
- Ahmad, N.; Zhu, Y.; Shafait, Z.; Sahibzada, U.F.; Waheed, A. Critical barriers to brownfield redevelopment in developing countries: The case of Pakistan. J. Clean. Prod. 2019, 212, 1193–1209. [Google Scholar] [CrossRef]
- Murray, T.J.; Pipino, L.L.; van Gigch, J.P. A pilot study of fuzzy set modification of Delphi. Hum. Syst. Manag. 1985, 5, 76–80. [Google Scholar]
- Ishikawa, A.; Amagasa, M.; Shiga, T.; Tomizawa, G.; Tatsuta, R.; Mieno, H. The max-min Delphi method and fuzzy Delphi method via fuzzy integration. Fuzzy Sets Syst. 1993, 55, 241–253. [Google Scholar] [CrossRef]
- Hsu, T.; Yang, T. Application of fuzzy analytic hierarchy process in the selection of advertising media. J. Manag. Syst. 2000, 7, 19–39. [Google Scholar]
- Ahmad, N.; Zhu, Y.; Ibrahim, M.; Waqas, M.; Waheed, A. Development of a Standard Brownfield Definition, Guidelines, and Evaluation Index System for Brownfield Redevelopment in Developing Countries: The Case of Pakistan. Sustainability 2018, 10, 4347. [Google Scholar] [CrossRef]
- Warfield, J.N. Toward interpretation of complex structural models. IEEE Trans. Syst. Man Cybern. 1974, 5, 405–417. [Google Scholar] [CrossRef]
- Jharkharia, S.; Shankar, R. IT-enablement of supply chains: Understanding the barriers. J. Enterp. Inf. Manag. 2005, 18, 11–27. [Google Scholar] [CrossRef]
- Singh, M.; Shankar, R.; Narain, R.; Agarwal, A. An interpretive structural modeling of knowledge management in engineering industries. J. Adv. Manag. Res. 2003, 1, 28–40. [Google Scholar] [CrossRef]
- Singh, M.; Kant, R. Knowledge management barriers: An interpretive structural modeling approach. Int. J. Manag. Sci. Eng. Manag. 2008, 3, 141–150. [Google Scholar] [CrossRef]
- Raisinghani, M.S.; Meade, L.L. Strategic decisions in supply-chain intelligence using knowledge management: An analytic-network-process framework. Supply Chain Manag. 2005, 10, 114–121. [Google Scholar] [CrossRef]
- Karamitri, I.; Talias, M.A.; Bellali, T. Knowledge management practices in healthcare settings: A systematic review. Int. J. Health Plan. Manag. 2017, 32, 4–18. [Google Scholar] [CrossRef] [PubMed]
- WHO. Pakistan Statistics Summary (2002–Present). 2015. Available online: http://apps.who.int/gho/data/node.country.country-PAK (accessed on 1 August 2018).
- Layne-Farrar, A. Business Models and the Standard Setting Process. 2010. Available online: http://www.konkurrensverket.se/globalassets/english/publications-and-decisions/the-pros-and-cons-of-standard-setting.pdf (accessed on 30 November 2018).
- Egan, M. Setting standards: Strategic advantages in international trade. Bus. Strategy Rev. 2002, 13, 51–64. [Google Scholar] [CrossRef]
- The Chartered Institute of Management Accountants. Effective Decision Making. 2005. Available online: http://www.cimaglobal.com/documents/importeddocuments/40_effective_decision_making.pdf (accessed on 1 December 2018).
- Drucker, P.F. Effective Decisions; Graduate School of Business Administration, Harvard University: Cambridge, MA, USA, 1967. [Google Scholar]
- Blake, W. Hospitals Are Learning from Industry How to Cut Medical Errors. 2018. Available online: https://www.economist.com/international/2018/06/28/hospitals-are-learning-from-industry-how-to-cut-medical-errors (accessed on 19 November 2018).
- WHO. Health System Profile—Pakistan. 2007. Available online: http://www.emro.who.int/human-resources-observatory/countries/country-profile.html (accessed on 15 September 2018).
- Rehmani, R. Emergency section and overcrowding in a university hospital of Karachi, Pakistan. J. Pakistan Med. Assoc. 2004, 54, 233–236. [Google Scholar]
- Pirnejad, H.; Niazkhani, Z.; Berg, M.; Bal, R. Intra-organizational communication in healthcare. Methods Inf. Med. 2008, 47, 336–345. [Google Scholar]
- Punjani, N.S.; Shams, S.; Bhanji, S.M. Analysis of health care delivery systems: Pakistan versus United States. Int. J. Endors. Health Sci. Res. 2014, 2, 38–41. [Google Scholar] [CrossRef]
- Export.gov. Pakistan—Healthcare and Medical Equipment. 2018. Available online: https://www.export.gov/article?id=Pakistan-Healthcare-and-Medical-Equipment (accessed on 1 November 2018).
- Inkpen, A.C. Creating knowledge through collaboration. California Manag. Rev. 1996, 39, 123–140. [Google Scholar] [CrossRef]
- Dyer, J.H. Effective interim collaboration: How firms minimize transaction costs and maximise transaction value. Strateg. Manag. J. 1997, 18, 535–556. [Google Scholar] [CrossRef]
- Grant, R.M.; Baden-Fuller, C. A knowledge-based theory of inter-firm collaboration. In Academy of Management Proceedings; Academy of Management: Briarcliff Manor, NY, USA, 1995; pp. 17–21. [Google Scholar]
- Matusik, S.F.; Hill, C.W. The utilization of contingent work, knowledge creation, and competitive advantage. Acad. Manag. Rev. 1998, 23, 680–697. [Google Scholar] [CrossRef]
- Kimberly, J.R. Managerial innovation. Handb. Organ. Design 1981, 1, 104. [Google Scholar]
- Winkelman, W.J.; Choo, C.W. Provider-sponsored virtual communities for chronic patients: Improving health outcomes through organizational patient-centred knowledge management. Health Expect. 2003, 6, 352–358. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| No | Drivers | References |
|---|---|---|
| 1 | Developed competitive advantage | [57,60,65,66] |
| 2 | Setting a standard for other organizations | [61] |
| 3 | Effective decision making | [57,62,64,67] |
| 4 | Increased patient service level | [62,63,68,69] |
| 5 | Reduction in the loss of life | Recommended by Group of Experts |
| 6 | Improved administrative healthcare performance | [57,62,63] |
| 7 | Intra-organizational communication in healthcare | [57,60,61] |
| 8 | Collaboration with other healthcare organizations | [57,58,59,60,70] |
| 9 | Improvement in quality of knowledge | [57,61,71] |
| 10 | Reduced knowledge attrition | [57,58,72] |
| 11 | Reduced utilization of resources | [63,73] |
| 12 | Increased trust among employees | [59,61,63] |
| 13 | Job creation opportunity | [62,63,73] |
| 14 | Adapting to rapid change in healthcare globally | [58,71,74] |
| 15 | The incubators of innovation | [58,60,62,75] |
| 16 | Increased organizational learning | [59,61,62] |
| 17 | Reduced administrative cost | [62,63,64,76] |
| 18 | Reduction in patient expenses | [62,64,76] |
| 19 | Improvement in the reputation of the healthcare | [63,77] |
| Drivers | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Developed competitive advantage | V | V | V | V | V | V | O | V | V | V | O | O | V | V | V | V | O | V | |
| 2 | Setting a standard for other organizations | V | V | V | V | V | V | V | V | O | O | O | V | V | V | O | O | V | ||
| 3 | Effective decision making | V | V | V | V | O | V | V | V | O | O | O | V | V | V | O | V | |||
| 4 | Increased patient service level | V | A | A | O | O | O | O | O | O | A | A | A | O | O | V | ||||
| 5 | Reduction in the loss of life | A | O | A | O | A | A | O | O | O | A | O | O | O | V | |||||
| 6 | Improved administrative healthcare performance | A | O | V | V | V | A | O | X | V | X | V | O | V | ||||||
| 7 | Intra-organizational communication in healthcare | V | V | V | O | X | O | O | V | O | O | V | O | |||||||
| 8 | Collaboration with other healthcare organizations | V | V | V | O | O | V | V | O | O | V | V | ||||||||
| 9 | Improvement in quality of knowledge | V | V | X | O | V | A | V | O | O | O | |||||||||
| 10 | Reduced knowledge attrition | O | O | O | V | A | V | V | O | O | ||||||||||
| 11 | Reduced utilization of resources | O | O | V | A | O | V | V | O | |||||||||||
| 12 | Increased trust among employees | O | O | X | V | O | O | O | ||||||||||||
| 13 | Job creation opportunity | O | O | O | O | O | O | |||||||||||||
| 14 | Adapting to rapid change in healthcare globally | A | V | A | O | V | ||||||||||||||
| 15 | The incubators of innovation | V | O | V | V | |||||||||||||||
| 16 | Increased organizational learning | V | O | V | ||||||||||||||||
| 17 | Reduced administrative cost | O | O | |||||||||||||||||
| 18 | Reduction in patient expenses | V | ||||||||||||||||||
| 19 | Improvement in the reputation of the healthcare | |||||||||||||||||||
| Structural Self-Interaction Matrix | Initial Reachability Matrix | |
|---|---|---|
| Element (i, j) | Element (i, j) | Element (j, i) |
| V | 1 | 0 |
| A | 0 | 1 |
| X | 1 | 1 |
| O | 0 | 0 |
| No. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 |
| 2 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 1 |
| 3 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 1 |
| 4 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 5 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 6 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 |
| 7 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 0 |
| 8 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 1 |
| 9 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 0 |
| 10 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 0 |
| 11 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 0 |
| 12 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 |
| 13 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| 14 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 1 |
| 15 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 |
| 16 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 1 |
| 17 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 0 |
| 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| 19 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Drivers | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | Driv. Power |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 * | 1 | 1 | 1 | 1 * | 0 | 1 | 1 | 1 | 1 | 1 * | 1 | 18 |
| 2 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 * | 1 * | 0 | 1 | 1 | 1 | 1 * | 1 * | 1 | 17 |
| 3 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 * | 1 | 1 | 1 | 1 * | 0 | 1 * | 1 | 1 | 1 | 1 * | 1 | 16 |
| 4 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 3 |
| 5 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 2 |
| 6 | 0 | 0 | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 * | 0 | 1 | 1 | 1 | 1 | 1 * | 1 | 13 |
| 7 | 0 | 0 | 0 | 1 | 1 * | 1 | 1 | 1 | 1 | 1 | 1 * | 1 | 0 | 1 * | 1 | 1 * | 1 * | 1 | 1 * | 15 |
| e | 0 | 0 | 0 | 1 * | 1 | 1 * | 0 | 1 | 1 | 1 | 1 | 1 * | 0 | 1 | 1 | 1 * | 1 * | 1 | 1 | 14 |
| 9 | 0 | 0 | 0 | 1 * | 1 * | 1 * | 1 * | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 1 * | 1 | 1 * | 1 * | 1 * | 14 |
| 10 | 0 | 0 | 0 | 1 * | 1 | 1 * | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 1 * | 8 |
| 11 | 0 | 0 | 0 | 1 * | 1 | 1 * | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 1 * | 1 | 1 | 1 * | 9 |
| 12 | 0 | 0 | 0 | 1 * | 1 * | 1 | 1 | 1 * | 1 | 1 * | 1 * | 1 | 0 | 1 * | 1 | 1 | 1 * | 1 * | 1 * | 15 |
| 13 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 14 | 0 | 0 | 0 | 1 | 1 * | 1 | 0 | 0 | 1 * | 1 * | 1 * | 1 * | 0 | 1 | 1 * | 1 | 1 * | 1 * | 1 | 13 |
| 15 | 0 | 0 | 0 | 1 | 1 | 1 * | 1 * | 1 * | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 * | 1 | 1 | 15 |
| 16 | 0 | 0 | 0 | 1 | 1 * | 1 | 0 | 0 | 1 * | 1 * | 1 * | 1 * | 0 | 1 * | 1 * | 1 | 1 | 1 * | 1 | 13 |
| 17 | 0 | 0 | 0 | 1 * | 1 * | 1 * | 0 | 0 | 1 * | 1 * | 1 * | 1 * | 0 | 1 | 1 * | 1 * | 1 | 1 * | 1 * | 13 |
| 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 2 |
| 19 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 |
| Dep. power | 1 | 2 | 3 | 15 | 16 | 14 | 7 | 7 | 12 | 13 | 13 | 12 | 1 | 14 | 12 | 14 | 14 | 14 | 18 | 202 |
| Drivers | Reachability Sets | Antecedent Set | Intersections | Levels |
|---|---|---|---|---|
| 1 | 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18, 19 | 1 | 1 | |
| 2 | 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18, 19 | 1, 2 | 2 | |
| 3 | 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18, 19 | 1, 2, 3 | 3 | |
| 4 | 4, 5, 19 | 1, 2, 3, 4, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 4 | |
| 5 | 5, 19 | 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 5 | |
| 6 | 4, 5, 6, 9, 10, 11, 12, 14, 15, 16, 17, 18, 19 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | |
| 7 | 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18, 19 | 1, 2, 3, 7, 9, 12, 15 | 7, 9, 12, 15 | |
| 8 | 4, 5, 6, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18, 19 | 1, 2, 3, 7, 8, 12, 15 | 8, 12, 15 | |
| 9 | 4, 5, 6, 7, 9, 10, 11, 12, 14, 15, 16, 17, 18, 19 | 1, 2, 3, 6, 7, 8, 9, 12, 14, 15, 16, 17 | 6, 7, 9, 12, 14, 15, 16, 17 | |
| 10 | 4, 5, 6, 10, 14, 16, 17, 19 | 1, 2, 3, 6, 7, 8, 9, 10, 12, 14, 15, 16, 17 | 6, 10, 14, 16, 17 | |
| 11 | 4, 5, 6, 11, 14, 16, 17, 18, 19 | 1, 2, 3, 6, 7, 8, 9, 11, 12, 14, 15, 16, 17 | 6, 11, 14, 16, 17 | |
| 12 | 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18, 19 | 1, 2, 3, 6, 7, 8, 9, 12, 14, 15, 16, 17 | 6, 7, 8, 9, 12, 14, 15, 16, 17 | |
| 13 | 13 | 13 | 13 | 1 |
| 14 | 4, 5, 6, 9, 10, 11, 12, 14, 15, 16, 17, 18, 19 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | |
| 15 | 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18, 19 | 1, 2, 3, 6, 7, 8, 9, 12, 14, 15, 16, 17 | 6, 7, 8, 9, 12, 14, 15, 16, 17 | |
| 16 | 4, 5, 6, 9, 10, 11, 12, 14, 15, 16, 17, 18, 19 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | |
| 17 | 4, 5, 6, 9, 10, 11, 12, 14, 15, 16, 17, 18, 19 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | |
| 18 | 18, 19 | 1, 2, 3, 6, 7, 8, 9, 11, 12, 14, 15, 16, 17, 18 | 18 | |
| 19 | 19 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18, 19 | 19 | 1 |
| Drivers | Reachability Sets | Antecedent Set | Intersections | Levels |
|---|---|---|---|---|
| 1 | 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18 | 1 | 1 | |
| 2 | 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18 | 1, 2 | 2 | |
| 3 | 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18 | 1, 2, 3 | 3 | |
| 4 | 4, 5 | 1, 2, 3, 4, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 4 | |
| 5 | 5 | 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 5 | 2 |
| 6 | 4, 5, 6, 9, 10, 11, 12, 14, 15, 16, 17, 18 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | |
| 7 | 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18 | 1, 2, 3, 7, 9, 12, 15 | 7, 9, 12, 15 | |
| 8 | 4, 5, 6, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18 | 1, 2, 3, 7, 8, 12, 15 | 8, 12, 15 | |
| 9 | 4, 5, 6, 7, 9, 10, 11, 12, 14, 15, 16, 17, 18 | 1, 2, 3, 6, 7, 8, 9, 12, 14, 15, 16, 17 | 6, 7, 9, 12, 14, 15, 16, 17 | |
| 10 | 4, 5, 6, 10, 14, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 10, 12, 14, 15, 16, 17 | 6, 10, 14, 16, 17 | |
| 11 | 4, 5, 6, 11, 14, 16, 17, 18 | 1, 2, 3, 6, 7, 8, 9, 11, 12, 14, 15, 16, 17 | 6, 11, 14, 16, 17 | |
| 12 | 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18 | 1, 2, 3, 6, 7, 8, 9, 12, 14, 15, 16, 17 | 6, 7, 8, 9, 12, 14, 15, 16, 17 | |
| 14 | 4, 5, 6, 9, 10, 11, 12, 14, 15, 16, 17, 18 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | |
| 15 | 4, 5, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17, 18 | 1, 2, 3, 6, 7, 8, 9, 12, 14, 15, 16, 17 | 6, 7, 8, 9, 12, 14, 15, 16, 17 | |
| 16 | 4, 5, 6, 9, 10, 11, 12, 14, 15, 16, 17, 18 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | |
| 17 | 4, 5, 6, 9, 10, 11, 12, 14, 15, 16, 17, 18 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | |
| 18 | 18 | 1, 2, 3, 6, 7, 8, 9, 11, 12, 14, 15, 16, 17, 18 | 18 | 2 |
| Drivers | Reachability Sets | Antecedent Set | Intersections | Levels |
|---|---|---|---|---|
| 1 | 1, 2, 3, 4, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1 | 1 | |
| 2 | 2, 3, 4, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2 | 2 | |
| 3 | 3, 4, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3 | 3 | |
| 4 | 4 | 1, 2, 3, 4, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 4 | 3 |
| 6 | 4, 6, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | |
| 7 | 4, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 7, 9, 12, 15 | 7, 9, 12, 15 | |
| 8 | 4, 6, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 7, 8, 12, 15 | 8, 12, 15 | |
| 9 | 4, 6, 7, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 12, 14, 15, 16, 17 | 6, 7, 9, 12, 14, 15, 16, 17 | |
| 10 | 4, 6, 10, 14, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 10, 12, 14, 15, 16, 17 | 6, 10, 14, 16, 17 | |
| 11 | 4, 6, 11, 14, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 11, 12, 14, 15, 16, 17 | 6, 11, 14, 16, 17 | |
| 12 | 4, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 12, 14, 15, 16, 17 | 6, 7, 8, 9, 12, 14, 15, 16, 17 | |
| 14 | 4, 6, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | |
| 15 | 4, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 12, 14, 15, 16, 17 | 6, 7, 8, 9, 12, 14, 15, 16, 17 | |
| 16 | 4, 6, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | |
| 17 | 4, 6, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 |
| Drivers | Reachability Sets | Antecedent Set | Intersections | Levels |
|---|---|---|---|---|
| 1 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1 | 1 | |
| 2 | 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2 | 2 | |
| 3 | 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3 | 3 | |
| 6 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | 4 |
| 7 | 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 7, 9, 12, 15 | 7, 9, 12, 15 | |
| 8 | 6, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 7, 8, 12, 15 | 8, 12, 15 | |
| 9 | 6, 7, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 12, 14, 15, 16, 17 | 6, 7, 9, 12, 14, 15, 16, 17 | |
| 10 | 6, 10, 14, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 10, 12, 14, 15, 16, 17 | 6, 10, 14, 16, 17 | 4 |
| 11 | 6, 11, 14, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 11, 12, 14, 15, 16, 17 | 6, 11, 14, 16, 17 | 4 |
| 12 | 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 12, 14, 15, 16, 17 | 6, 7, 8, 9, 12, 14, 15, 16, 17 | |
| 14 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | 4 |
| 15 | 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 12, 14, 15, 16, 17 | 6, 7, 8, 9, 12, 14, 15, 16, 17 | |
| 16 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | 4 |
| 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | 1, 2, 3, 6, 7, 8, 9, 10, 11, 12, 14, 15, 16, 17 | 6, 9, 10, 11, 12, 14, 15, 16, 17 | 4 |
| Drivers | Reachability Sets | Antecedent Set | Intersections | Levels |
|---|---|---|---|---|
| 1 | 1, 2, 3, 7, 8, 9, 12, 15 | 1 | 1 | |
| 2 | 2, 3, 7, 8, 9, 12, 15 | 1, 2 | 2 | |
| 3 | 3, 7, 8, 9, 12, 15 | 1, 2, 3 | 3 | |
| 7 | 7, 8, 9, 12, 15 | 1, 2, 3, 7, 9, 12, 15 | 7, 9, 12, 15 | |
| 8 | 8, 9, 12, 15 | 1, 2, 3, 7, 8, 12, 15 | 8, 12, 15 | |
| 9 | 7, 9, 12, 15 | 1, 2, 3, 7, 8, 9, 12, 15 | 7, 9, 12, 15 | 5 |
| 12 | 7, 8, 9, 12, 15 | 1, 2, 3, 7, 8, 9, 12, 15 | 7, 8, 9, 12, 15 | 5 |
| 15 | 7, 8, 9, 12, 15 | 1, 2, 3, 7, 8, 9, 12, 15 | 7, 8, 9, 12, 15 | 5 |
| Drivers | Reachability Sets | Antecedent Set | Intersections | Levels |
|---|---|---|---|---|
| 1 | 1, 2, 3, 7, 8 | 1 | 1 | |
| 2 | 2, 3, 7, 8 | 1, 2 | 2 | |
| 3 | 3, 7, 8 | 1, 2, 3 | 3 | |
| 7 | 7, 8 | 1, 2, 3, 7 | 7 | |
| 8 | 8 | 1, 2, 3, 7, 8, | 8 | 6 |
| Drivers | Reachability Sets | Antecedent Set | Intersections | Levels |
|---|---|---|---|---|
| 1 | 1, 2, 3, 7 | 1 | 1 | |
| 2 | 2, 3, 7 | 1, 2 | 2 | |
| 3 | 3, 7 | 1, 2, 3 | 3 | |
| 7 | 7 | 1, 2, 3, 7 | 7 | 7 |
| Drivers | Reachability Sets | Antecedent Set | Intersections | Levels |
|---|---|---|---|---|
| 1 | 1, 2, 3 | 1 | 1 | |
| 2 | 2, 3 | 1, 2 | 2 | |
| 3 | 3 | 1, 2, 3 | 3 | 8 |
| Drivers | Reachability Sets | Antecedent Set | Intersections | Levels |
|---|---|---|---|---|
| 1 | 1, 2 | 1 | 1 | |
| 2 | 2 | 1, 2 | 2 | 9 |
| Drivers | Reachability Sets | Antecedent Set | Intersections | Levels |
|---|---|---|---|---|
| 1 | 1 | 1 | 1 | 10 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karamat, J.; Shurong, T.; Ahmad, N.; Afridi, S.; Khan, S.; Mahmood, K. Promoting Healthcare Sustainability in Developing Countries: Analysis of Knowledge Management Drivers in Public and Private Hospitals of Pakistan. Int. J. Environ. Res. Public Health 2019, 16, 508. https://doi.org/10.3390/ijerph16030508
Karamat J, Shurong T, Ahmad N, Afridi S, Khan S, Mahmood K. Promoting Healthcare Sustainability in Developing Countries: Analysis of Knowledge Management Drivers in Public and Private Hospitals of Pakistan. International Journal of Environmental Research and Public Health. 2019; 16(3):508. https://doi.org/10.3390/ijerph16030508
Chicago/Turabian StyleKaramat, Jawad, Tong Shurong, Naveed Ahmad, Sana Afridi, Shahbaz Khan, and Kashif Mahmood. 2019. "Promoting Healthcare Sustainability in Developing Countries: Analysis of Knowledge Management Drivers in Public and Private Hospitals of Pakistan" International Journal of Environmental Research and Public Health 16, no. 3: 508. https://doi.org/10.3390/ijerph16030508
APA StyleKaramat, J., Shurong, T., Ahmad, N., Afridi, S., Khan, S., & Mahmood, K. (2019). Promoting Healthcare Sustainability in Developing Countries: Analysis of Knowledge Management Drivers in Public and Private Hospitals of Pakistan. International Journal of Environmental Research and Public Health, 16(3), 508. https://doi.org/10.3390/ijerph16030508