Artificial Stone Associated Silicosis: A Systematic Review




Abstract
:1. Introduction
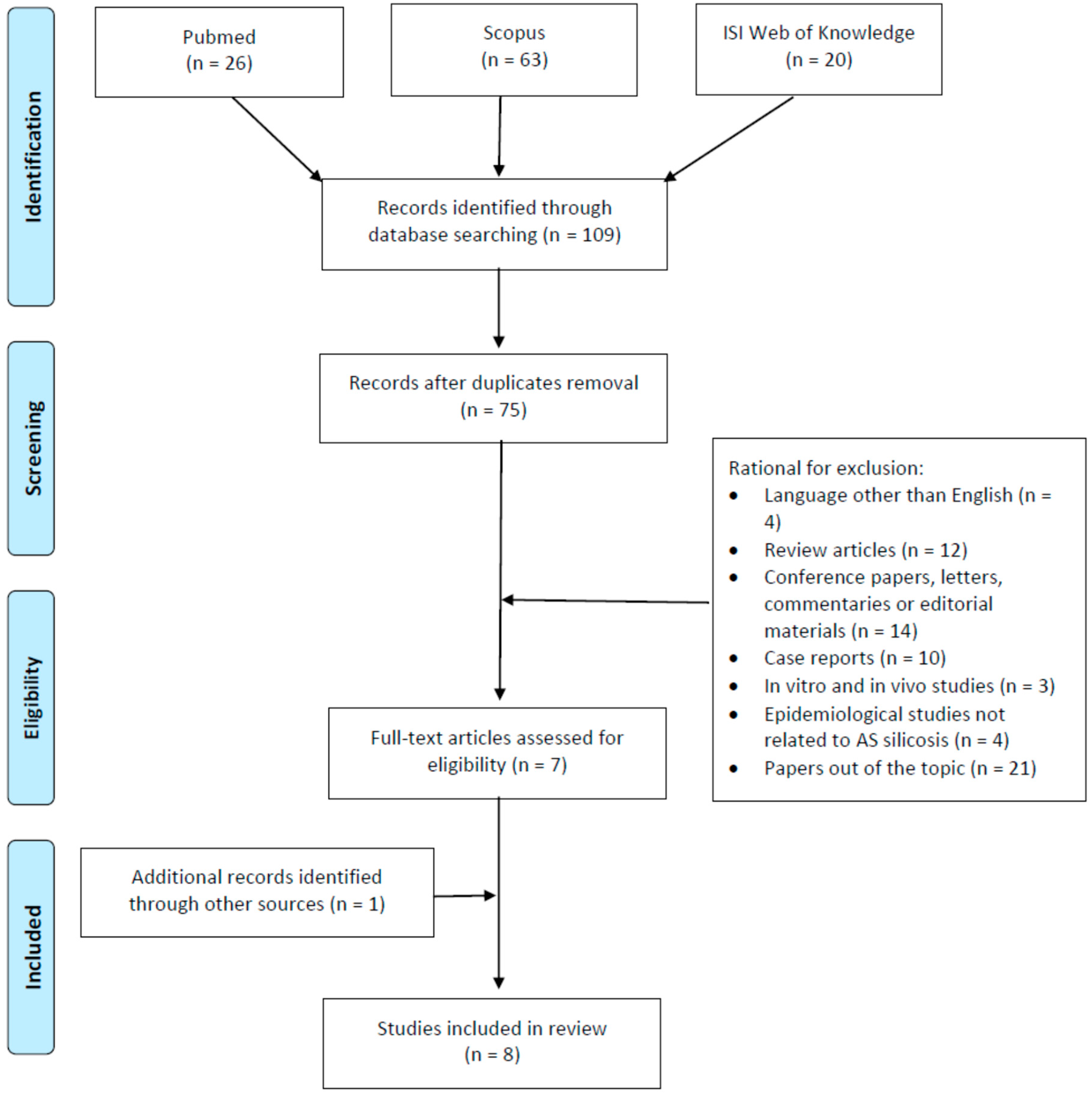
2. Materials and Methods
3. Results
3.1. Identification of Cases
3.2. Symptoms, Pulmonary Function Tests, Radiological Diagnosis
3.3. Histopathological Examination
3.4. Post-Lung Transplantation Outcomes
3.5. Silica Exposure Risk Assessment and Management
3.5.1. Exposure Assessment
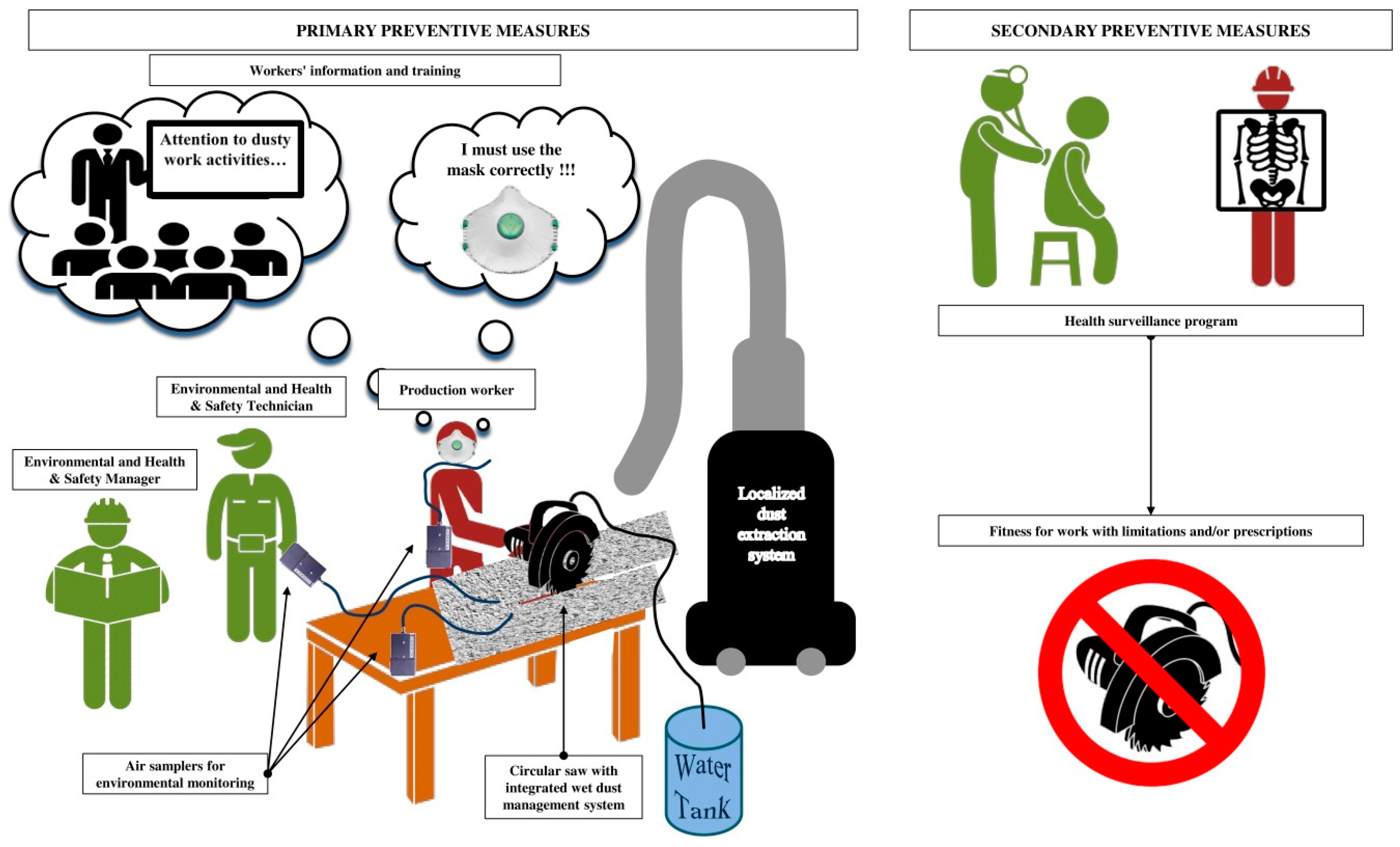
3.5.2. Collective Protective Measures
3.5.3. Personal Protective Equipment
3.5.4. Occupational Health Surveillance
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Leung, C.C.; Yu, I.T.; Chen, W. Silicosis. Lancet 2012, 379, 2008–2018. [Google Scholar] [CrossRef]
- National Institute for Occupational Safety and Health. Health Effects of Occupational Exposure to Respirable Crystalline Silica. Available online: https://www.cdc.gov/niosh/docs/2002-129/default.html (accessed on 20 December 2018).
- Hedlund, U.; Jonsson, H.; Eriksson, K.; Järvholm, B. Exposure–response of silicosis mortality in Swedish iron ore miners. Ann. Occup. Hyg. 2008, 52, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Mossman, B.T.; Churg, A. Mechanisms in the pathogenesis of asbestosis and silicosis. Am. J. Respir. Crit. Care Med. 1998, 157, 1666–1680. [Google Scholar] [CrossRef] [PubMed]
- Lopes-Pacheco, M.; Bandeira, E.; Morales, M.M. Cell-Based Therapy for Silicosis. Stem. Cells Int. 2016, 2016, 5091838. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, M.I.; Waksman, J.; Curtis, J. Silicosis: A review. Dis. Mon. 2007, 53, 394–416. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.R.; Blanc, P.D.; Fireman, E.; Amital, A.; Guber, A.; Rhahman, N.A.; Shitrit, D. Artificial stone silicosis [corrected]: Disease resurgence among artificial stone workers. Chest 2012, 142, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Poinen-Rughooputh, S.; Rughooputh, M.S.; Guo, Y.; Rong, Y.; Chen, W. Occupational exposure to silica dust and risk of lung cancer: An updated meta-analysis of epidemiological studies. BMC Public Health 2016, 16, 1137. [Google Scholar] [CrossRef]
- Occupational Safety and Health Administration, Department of Labor. Occupational exposure to respirable crystalline silica; final rule. Fed. Regist. 2016, 81, 16285–16890. [Google Scholar]
- World Health Organization. Elimination of Silicosis GOHNET Newsletter. Geneva WHO Global Occupational Health Network. 2007, pp. 1–20. Available online: https://www.who.int/occupational_health/publications/newsletter/gohnet12eref.pdf (accessed on 20 December 2018).
- Kauppinen, T.; Toikkanen, J.; Pedersen, D.; Young, R.; Ahrens, W.; Boffetta, P.; Hansen, J.; Kromhout, H.; Maqueda Blasco, J.; Mirabelli, D.; et al. Occupational exposure to carcinogens in the European Union. Occup. Environ. Med. 2000, 57, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Henneberger, P.K.; Weissman, D.N. Old adversaries in new places. Occup. Environ. Med. 2018, 75, 1–2. [Google Scholar] [CrossRef]
- Maciejewska, A. Occupational exposure assessment for crystalline silica dust: Approach in Poland and worldwide. Int. J. Occup. Med. Environ. Health 2008, 21, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Sato, T.; Shimosato, T.; Klinman, D.M. Silicosis and lung cancer: Current perspectives. Lung Cancer 2018, 9, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Steenland, K.; Ward, E. Silica: A lung carcinogen. CA Cancer J. Clin. 2014, 64, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Rosengarten, D.; Fox, B.D.; Fireman, E.; Blanc, P.D.; Rusanov, V.; Fruchter, O.; Raviv, Y.; Shtraichman, O.; Saute, M.; Kramer, M.R. Survival following lung transplantation for artificial stone silicosis relative to idiopathic pulmonary fibrosis. Am. J. Ind. Med. 2017, 60, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Hoy, R.F.; Baird, T.; Hammerschlag, G.; Hart, D.; Johnson, A.R.; King, P.; Putt, M.; Yates, D.H. Artificial stone-associated silicosis: A rapidly emerging occupational lung disease. Occup. Environ. Med. 2018, 75, 3–5. [Google Scholar] [CrossRef]
- Ophir, N.; Shai, A.B.; Alkalay, Y.; Israeli, S.; Korenstein, R.; Kramer, M.R.; Fireman, E. Artificial stone dust-induced functional and inflammatory abnormalities in exposed workers monitored quantitatively by biometrics. ERJ Open Res. 2016, 2, 0086–2015. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, D.; Miller, B.G.; Soutar, C.A. Quantitative relations between exposure to respirable quartz and risk of silicosis. Occup. Environ. Med. 2003, 60, 159–164. [Google Scholar] [CrossRef] [Green Version]
- Cooper, J.H.; Johnson, D.L.; Phillips, M.L. Respirable silica dust suppression during artificial stone countertop cutting. Ann. Occup. Hyg. 2015, 59, 122–126. [Google Scholar] [CrossRef]
- Meldrum, M.; Howden, P. Crystalline silica: Variability in fibrogenic potency. Ann. Occup. Hyg. 2002, 46, 27–30. [Google Scholar]
- Guarnieri, G.; Bizzotto, R.; Gottardo, O.; Velo, E.; Cassaro, M.; Vio, S.; Putzu, M.G.; Rossi, F.; Zuliani, P.; Liviero, F.; et al. Multiorgan accelerated silicosis misdiagnosed as sarcoidosis in two workers exposed to quartz conglomerate dust. Occup. Environ. Med. 2018, 2018–105462. [Google Scholar] [CrossRef]
- Occupation Safety Health Administration. Worker Exposure to Silica during Countertop Manufacturing, Finishing and Installation. Available online: https://www.osha.gov/Publications/OSHA3768.pdf (accessed on 20 December 2018).
- Bartoli, D.; Banchi, B.; di Benedetto, F.; Farina, G.A.; Iaia, T.E.; Poli, C.; Romanelli, M.; Scancarello, G.; Tarchi, M. Silicosis in employees in the processing of kitchen, bar and shop countertops made from quartz resin composite. Provisional results of the environmental and health survey conducted within the territory of USL 11 of Empoli in Tuscany among employees in the processing of quartz resin composite materials and review of the literature. Ital. J. Occup. Environ. Hyg. 2012, 3, 138–143. [Google Scholar]
- Friedman, G.K.; Harrison, R.; Bojes, H.; Worthington, K.; Filios, M. Centers for Disease Control and Prevention (CDC). Notes from the field: Silicosis in a countertop fabricator—Texas, 2014. MMWR Morb. Mortal Wkly. Rep. 2015, 64, 129–130. [Google Scholar] [PubMed]
- Frankel, A.; Blake, L.; Yates, D. Complicated silicosis in an Australian worker from cutting engineered stone countertops: An embarrassing first for Australia. Eur. Resp. J. 2015, 46, PA1144. [Google Scholar] [CrossRef]
- García Vadillo, C.; Gómez, J.S.; Morillo, J.R. Silicosis in quartz conglomerate workers. Arch. Bronconeumol. 2011, 47, 53. [Google Scholar] [CrossRef] [PubMed]
- Hoy, R. Artificial stone associated silicosis with rapid lung function decline. Eur. Resp. J. 2017, 50, OA484. [Google Scholar] [CrossRef]
- Jimenez, A.L.; Hidalgo Molina, A.; Morales Morales, J.; Conde Sanchez, M.A.; Sanchez Romero, I.; Perez Alonso, A.; Cordoba Doña, J.A. Rapid clinical progression of silicosis in quartz conglomerate workers in Southern Spain. Eur. Resp. J. 2017, 50, OA483. [Google Scholar] [CrossRef]
- Martínez, C.; Prieto, A.; García, L.; Quero, A.; González, S.; Casan, P. Silicosis: A disease with an active present. Arch. Bronconeumol. 2010, 46, 97–100. [Google Scholar] [CrossRef]
- Matar, E.; Frankel, A.; McCowan Blake, L.K.; Silverstone, E.J.; Johnson, A.R.; Yates, D.H. Complicated silicosis resulting from occupational exposure to engineered stone products. Med. J. Aust. 2017, 206, 385–386. [Google Scholar] [CrossRef]
- Paolucci, V.; Romeo, R.; Sisinni, A.G.; Bartoli, D.; Mazzei, M.A.; Sartorelli, P. Silicosis in Workers Exposed to Artificial Quartz Conglomerates: Does It Differ From Chronic Simple Silicosis? Arch. Bronconeumol. 2015, 51, e57–e60. [Google Scholar] [CrossRef]
- Pérez-Alonso, A.; Córdoba-Doña, J.A.; García-Vadillo, C. Silicosis: Relevant differences between marble workers and miners. Arch. Bronconeumol. 2015, 51, 53–54. [Google Scholar] [CrossRef]
- Ronsmans, S.; Decoster, L.; Keirsbilck, S.; Verbeken, E.K.; Nemery, B. Artificial stone-associated silicosis in Belgium. Occup. Environ. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Shtraichman, O.; Kramer, M.R. Artificial stone silicosis: The Israel epidemic, current view. Harefuah 2017, 156, 517–521. [Google Scholar] [PubMed]
- Shtraichman, O.; Blanc, P.; Ollech, J.; Fridel, L.; Fuks, L.; Fireman, E.; Shitrit, D.; Kramer, M. Outbreak of autoimmune disease in a silicosis cluster linked to high-silica content artificial stone. Eur. Res. J. 2014, 44, P4545. [Google Scholar]
- Barber, C.M.; Fishwick, D.; Seed, M.J.; Carder, M.; van Tongeren, M. Artificial stone-associated silicosis in the UK. Occup. Environ. Med. 2018, 75, 541. [Google Scholar] [CrossRef] [PubMed]
- Pavan, C.; Polimeni, M.; Tomatis, M.; Corazzari, I.; Turci, F.; Ghigo, D.; Fubini, B. Editor’s Highlight: Abrasion of Artificial Stones as a New Cause of an Ancient Disease. Physicochemical Features and Cellular Responses. Toxicol. Sci. 2016, 153, 4–17. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Joanna Briggs Institute. Critical Appraisal tools for use in JBI Systematic Reviews Checklist for Case Series. Available online: http://joannabriggs.org/assets/docs/critical-appraisal-tools/JBI_Critical_Appraisal-Checklist_for_Case_Series2017.pdf (accessed on 29 January 2019).
- Shtraichman, O.; Blanc, P.D.; Ollech, J.E.; Fridel, L.; Fuks, L.; Fireman, E.; Kramer, M.R. Outbreak of autoimmune disease in silicosis linked to artificial stone. Occup. Med. 2015, 65, 444–450. [Google Scholar] [CrossRef] [Green Version]
- Grubstein, A.; Osnat Shtraichman, M.D.; Fireman, E.; Bachar, G.N.; Noach-Ophir, N.; Kramer, M.R. Radiological Evaluation of Artificial Stone Silicosis Outbreak: Emphasizing Findings in Lung Transplant Recipients. J. Comput. Assist. Tomogr. 2016, 40, 923–927. [Google Scholar] [CrossRef]
- Pérez-Alonso, A.; Córdoba-Doña, J.A.; Millares-Lorenzo, J.L.; Figueroa-Murillo, E.; García-Vadillo, C.; Romero-Morillos, J. Outbreak of silicosis in Spanish quartz conglomerate workers. Int. J. Occup. Environ. Health 2014, 20, 26–32. [Google Scholar] [CrossRef]
- Pascual, S.; Urrutia, I.; Ballaz, A.; Arrizubieta, I.; Altube, L.; Salinas, C. Prevalence of silicosis in a marble factory after exposure to quartz conglomerates. Arch. Bronconeumol. 2011, 47, 50–51. [Google Scholar] [CrossRef]
- Pascual Del Pobil, Y.; Ferré, M.A.; García Sevila, R.; García Rodenas, M.D.M.; Barroso Medel, E.; Flores Reos, E.; Gil Carbonell, J. Silicosis: A former occupational disease with new occupational exposure scenarios. Rev. Clin. Esp. 2019. [Google Scholar] [CrossRef]
- Rosenman, K.D.; Reilly, M.J.; Gardiner, J. Results of spirometry among individuals in a silicosis registry. J. Occup. Environ. Med. 2010, 52, 1173–1178. [Google Scholar] [CrossRef] [PubMed]
- Di Giuseppe, M.; Gambelli, F.; Hoyle, G.W.; Lungarella, G.; Studer, S.M.; Richards, T.; Yousem, S.; McCurry, K.; Dauber, J.; Kaminski, N.; et al. Systemic inhibition of nf-kappab activation protects from silicosis. PLoS ONE 2009, 4, e5689. [Google Scholar] [CrossRef] [PubMed]
- Enfield, K.B.; Floyd, S.; Barker, B.; Weder, M.; Kozower, B.D.; Jones, D.R.; Lau, C.L. Survival after lung transplant for coal workers’ pneumoconiosis. J. Heart Lung Transplant. 2012, 31, 1315–1318. [Google Scholar] [CrossRef] [PubMed]
- Directive (EU) 2017/2398 Of The European Parliament And Of The Council of 12 December 2017 Amending Directive 2004/37/EC on the Protection of Workers from the Risks Related to Exposure to Carcinogens or Mutagens at Work. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32017L2398&from=EN (accessed on 20 December 2018).
- Phillips, M.L.; Johnson, D.L.; Johnson, A.C. Determinants of respirable silica exposure in stone countertop fabrication: A preliminary study. J. Occup. Environ. Hyg. 2013, 10, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.L.; Phillips, M.L.; Qi, C.; Van, A.T.; Hawley, D.A. Experimental Evaluation of Respirable Dust and Crystalline Silica Controls During Simulated Performance of Stone Countertop Fabrication Tasks With Powered Hand Tools. Ann. Work Expo. Health 2017, 61, 711–723. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Country | Study Period | Type of Study | Working Activities Investigated and Correlated Cases of Silicosis (n.) | Age of Workers (Years) | Exposure Time (Years) | Quality Rating by JBI | Reference |
|---|---|---|---|---|---|---|---|
| Australia | 2011–2016 | Epidemiological study investigating the prevalence of artificial stone associated silicosis | Dry cutting and polishing of artificial stone for fabrication of small kitchen and bathroom benchtop (7) | 44 (median) | 7.3 (median) | Fair | Hoy et al. [17] |
| Israel | 1997–2010 | Retrospective analysis of patients (with a diagnosis of silicosis) candidates to lung transplantation | Dry cutting of synthetic stone material (Caesar Stone containing ˃85% crystalline silica) for kitchens and other countertop applications (25) | 52 (median) | 17 ± 9–22 ± 7 (mean ± SD) | Good | Kramer et al. [7] |
| Israel | 1997–2012 | Retrospective analysis of patients (with a diagnosis of silicosis) candidates to lung transplantation | Dry cutting and polishing synthetic stone material (with high content of crystalline silica) for kitchens and other countertop applications (40 whom 9 with autoimmune disease) |
| 6–26 (9 with autoimmune disease) | Good | Shtraichman et al. [41] |
| Israel | 1997–2015 | Evaluation of patients with diagnosis of silicosis visited in a pulmonary outpatient clinic | Dry cutting and polishing artificial decorative stone products (˃93–94% crystalline silica) for kitchens and other countertop applications (82) | 47.26 (mean) | 19.8 ± 9.4 (mean ± SD) | Fair | Grubstein et al. [42] |
| Israel | 2006–2013 | Retrospective analysis of patients who underwent lung transplantation for silicosis | Occupations carrying out job tasks consistent with over-exposure to silica through handling artificial stone (17) | 50 (median) | Not reported | Good | Rosengarten et al. [16] |
| Spain | 2008–2011 | Prospective observational study investigating the prevalence of silicosis in subjects who worked quartz conglomerates | Cutting, polishing and assembling quartz conglomerates composed of at least 90% natural quartz (crystallized silicon dioxide [SiO2] and silica) (6) | 39.81 (mean) | 12.54 (mean) | Poor | Pascual et al. [44] |
| Spain | 2009–2012 | Epidemiological study investigating the prevalence of artificial stone associated silicosis and the correlated working conditions in workers exposed to quartz conglomerates | Working activities (cutting, shaping and finishing) in which agglomerated quartz was used in the manufacturing of countertops for kitchens (46) | 33 (median) | 12.8 (mean) | Good | Perez-Alonso et al. [43] |
| Spain | 2009–2016 | Descriptive epidemiological study assessing the prevalence of artificial stone associated silicosis among the silicosis cases reported to the Healthcare Information System for Occupational Epidemiological Surveillance of the Community of Valencia | Cutting, sanding and assembling artificial quartz aggregates (with a high content of crystalline silica: 70–90%) for kitchen and bath countertops (13) | 46.62 ± 13.33 (mean ± SD) | 11.00 ± 3.58 (mean ± SD) | Poor | Pascual et al. [45] |
| Country | Cases (n.) | Respiratory Function Tests | Radiological Assessment | Diagnosis | Reference |
|---|---|---|---|---|---|
| Australia | 7 |
| High-resolution computerized tomographic: semiconfluent nodules in the mid and upper zones, ground glass nodules, bilateral upper lobe fibrosis and volume loss with reticulonodular and large confluent mass-like densities |
| Hoy et al. [17] |
| Israel | 25 | Moderate to severe restrictive lung disease | Diffuse micronodular pattern and progressive massive fibrosis |
| Kramer et al. [7] |
| Israel | 9 |
|
| Silicosis | Shtraichman et al. [41] |
| Israel | 82 | Reduced FEV1: 68.4±26 (mean±SD) | High-resolution computerized tomographic: centrilobular and perilymphatic nodules, nodal enlargement with or without nodal calcification, emphysema, and conglomerate masses–progressive massive fibrosis |
| Grubstein et al. [42] |
| Israel | 17 | Reduced FEV1 (median: 31; 25th-75th percentile range: 27-38) TLC (median: 47; 25th-75th percentile range: 41-54) | High-resolution computerized tomographic: picture of interstitial lung disease that was consistent withsilicosis in all cases | Silicosis | Rosengarten et al. [16] |
| Spain | 6 |
| Chest X-ray: radiographic patterns of simple chronic silicosis (83.3%) and progressive massive fibrosis (16.66%) |
| Pascual et al. [44] |
| Spain | 46 |
|
|
| Perez-Alonso et al. [43] |
| Spain | 13 | Spirometric data was obtained in 14 silicosis cases. The results of respiratory function tests refer to the total number of cases (findings of patients exposed to artificial quartz aggregates are not specified):
| High-resolution computerized tomographic data were obtained in 14 silicosis cases. The results refer to the total number of cases (findings of patients exposed to artificial quartz aggregates are not specified): micronodular pattern with hilar and mediastinal adenopathies |
| Pascual et al. [45] |
| Country | Cases (n.) | Environmental Monitoring | Collective Protective Measures | Individual Protective Measures | Reference |
|---|---|---|---|---|---|
| Australia | 7 | Environmental monitoring data not known or available |
|
| Hoy et al. [17] |
| Israel | 25 | Environmental monitoring data not known or available | No dust suppression systems or effective local ventilation | The working activities were performed without any personal respiratory protection | Kramer et al. [7] |
| Israel | 9 | Environmental monitoring data not known or available | Not reported | Inadequate respiratory protection (not specified) | Shtraichman et al. [41] |
| Israel | 82 | Environmental monitoring data not known or available | Not reported | Not reported | Grubstein et al. [42] |
| Israel | 17 | Environmental monitoring carried out by the Israel Ministry of Labor has documented that standard working activities (i.e., dry cutting) with artificial stone cause exposure to levels of silica ˃1 mg/m3 | No dust suppression systems | The working activities were performed without any personal respiratory protection | Rosengarten et al. [16] |
| Spain | 6 | Environmental monitoring data not known or available |
| No specific respiratory protection apparatuses were used (at least until 2009) | Pascual et al. [44] |
| Spain | 46 | Environmental monitoring of dust levels was never performed in any workplace |
|
| Perez-Alonso et al. [43] |
| Spain | 13 | Environmental monitoring data not known or available |
| Occasional use of individual protection equipment is reported (not specified what type of protective equipment) | Pascual et al. [45] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leso, V.; Fontana, L.; Romano, R.; Gervetti, P.; Iavicoli, I. Artificial Stone Associated Silicosis: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 568. https://doi.org/10.3390/ijerph16040568
Leso V, Fontana L, Romano R, Gervetti P, Iavicoli I. Artificial Stone Associated Silicosis: A Systematic Review. International Journal of Environmental Research and Public Health. 2019; 16(4):568. https://doi.org/10.3390/ijerph16040568
Chicago/Turabian StyleLeso, Veruscka, Luca Fontana, Rosaria Romano, Paola Gervetti, and Ivo Iavicoli. 2019. "Artificial Stone Associated Silicosis: A Systematic Review" International Journal of Environmental Research and Public Health 16, no. 4: 568. https://doi.org/10.3390/ijerph16040568
APA StyleLeso, V., Fontana, L., Romano, R., Gervetti, P., & Iavicoli, I. (2019). Artificial Stone Associated Silicosis: A Systematic Review. International Journal of Environmental Research and Public Health, 16(4), 568. https://doi.org/10.3390/ijerph16040568