Implementation of the Healthy Workplace Participatory Program in a Retail Setting: A Feasibility Study and Framework for Evaluation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview and Employer Context
2.2. Program Description
2.2.1. HWPP Model and IDEAS Tool
2.2.2. Planning & Roles
2.2.3. Experience Map
2.2.4. Design Team and Steering Committee Recruitment
2.3. Process Evaluation
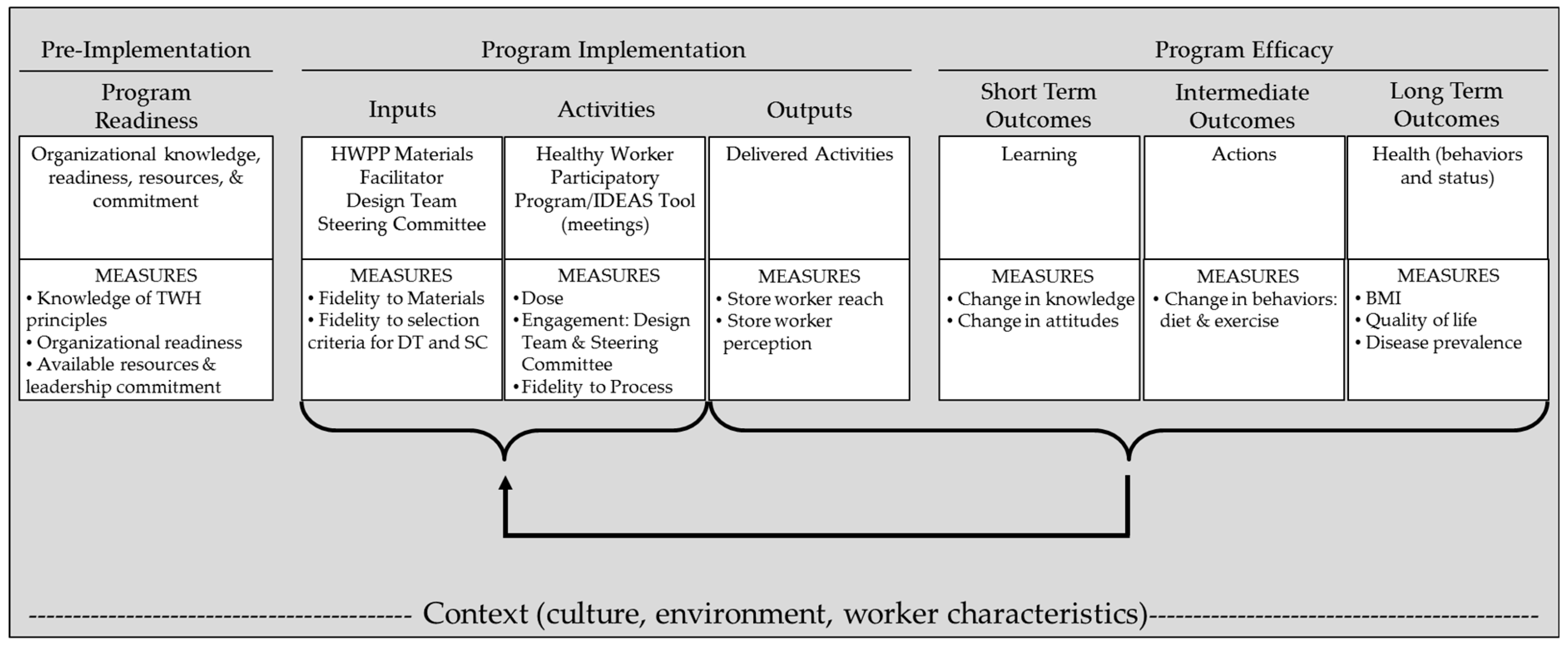
2.3.1. Logic Model
2.3.2. Data Collection
2.3.3. Data Analysis
3. Results
3.1. Model Context
3.2. Model Inputs
3.3. Model Activities
3.4. Model Outputs
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dale, A.M.; Enke, C.; Buckner-Petty, S.; Hipp, J.A.; Marx, C.; Strickland, J.; Evanoff, B. Availability and Use of Workplace Supports for Health Promotion Among Employees of Small and Large Businesses. Am. J. Health Promot. 2018, 33, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Lerner, D.; Allaire, S.H.; Reisine, S.T. Work disability resulting from chronic health conditions. J. Occup. Environ. Med. 2005, 47, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Meraya, A.M.; Sambamoorthi, U. Chronic Condition Combinations and Productivity Loss Among Employed Nonelderly Adults (18 to 64 Years). J. Occup. Environ. Med. 2016, 58, 974–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuong, T.D.; Wei, F.; Beverly, C.J. Absenteeism due to Functional Limitations Caused by Seven Common Chronic Diseases in US Workers. J. Occup. Environ. Med. 2015, 57, 779–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asay, G.R.B.; Roy, K.; Lang, J.E.; Payne, R.L.; Howard, D.H. Absenteeism and Employer Costs Associated With Chronic Diseases and Health Risk Factors in the US Workforce. Prev. Chronic Dis. 2016, 13, E141. [Google Scholar] [CrossRef]
- National Center for Chronic Disease Prevention and Health Promotion. Using the Workplace to Improve the Nation’s Health: At a Glance 2016. Available online: https://www.cdc.gov/chronicdisease/resources/publications/aag/workplace-health.htm (accessed on 21 December 2018).
- Froehlich-Grobe, K.; Jones, D.; Businelle, M.S.; Kendzor, D.E.; Balasubramanian, B.A. Impact of disability and chronic conditions on health. Disabil. Health J. 2016, 9, 600–608. [Google Scholar] [CrossRef]
- Schopp, L.H.; Bike, D.H.; Clark, M.J.; Minor, M.A. Act Healthy: Promoting health behaviors and self-efficacy in the workplace. Health Educ. Res. 2015, 30, 542–553. [Google Scholar] [CrossRef] [PubMed]
- Loeppke, R.; Taitel, M.; Haufle, V.; Parry, T.; Kessler, R.C.; Jinnett, K. Health and productivity as a business strategy: A multiemployer study. J. Occup. Environ. Med. 2009, 51, 411–428. [Google Scholar] [CrossRef] [PubMed]
- Bauer, U.E.; Briss, P.A.; Goodman, R.A.; Bowman, B.A. Prevention of chronic disease in the 21st century: Elimination of the leading preventable causes of premature death and disability in the USA. Lancet 2014, 384, 45–52. [Google Scholar] [CrossRef]
- National Institute for Occupational Safety and Health. What is Total Worker Health? Available online: https://www.cdc.gov/niosh/twh/default.html (accessed on 19 December 2018).
- Tamers, S.L.; Chosewood, L.C.; Childress, A.; Hudson, H.; Nigam, J.; Chang, C.-C. Total Worker Health® 2014–2018: The Novel Approach to Worker Safety, Health, and Well-Being Evolves. Int. J. Environ. Res. Public Health 2019, 16, 321. [Google Scholar] [CrossRef] [PubMed]
- Feltner, C.; Peterson, K.; Palmieri Weber, R.; Cluff, L.; Coker-Schwimmer, E.; Viswanathan, M.; Lohr, K.N. The Effectiveness of Total Worker Health Interventions: A Systematic Review for a National Institutes of Health Pathways to Prevention Workshop. Ann. Intern. Med. 2016, 165, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Henning, R.; Warren, N.; Roberston, M.; Faghri, P.; Cherniack, M.; CPH-NEW Research Team. Workplace Health Protection and Promotion through Participatory Ergonomics: An Integrated Approach. Public Health Rep. 2009, 124, 26–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Eerd, D.; Cole, D.; Irvin, E.; Mahood, Q.; Keown, K.; Theberge, N.; Village, J.; St Vincent, M.; Cullen, K. Process and implementation of participatory ergonomic interventions: A systematic review. Ergonomics 2010, 53, 1153–1166. [Google Scholar] [CrossRef] [PubMed]
- Hignett, S.; Wilson, J.R.; Morris, W. Finding ergonomic solutions: Participatory approaches. Occup. Med. Oxf. 2005, 55, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Faridi, Z.; Grunbaum, J.; Gray, B.; Franks, A.; Simoes, E. Community-based Participatory Research: Necessary Next Steps. Prev. Chronic Dis. 2007, 4, A70. [Google Scholar] [PubMed]
- Dugan, A.G.; Farr, D.A.; Namazi, S.; Henning, R.A.; Wallace, K.N.; El Ghaziri, M.; Punnett, L.; Dussetschleger, J.L.; Cherniack, M.G. Process evaluation of two participatory approaches: Implementing total worker health(R) interventions in a correctional workforce. Am. J. Ind. Med. 2016, 59, 897–918. [Google Scholar] [CrossRef] [PubMed]
- Cherniack, M.; Dussetschleger, J.; Dugan, A.; Farr, D.; Namazi, S.; El Ghaziri, M.; Henning, R. Participatory action research in corrections: The HITEC 2 program. Appl. Ergon. 2016, 53, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Evanoff, B.A.; Bohr, P.C.; Wolf, L.D. Effects of a participatory ergonomics team among hospital orderlies. Am. J. Ind. Med. 1999, 35, 358–365. [Google Scholar] [CrossRef]
- Robertson, M.; Henning, R.; Warren, N.; Nobrega, S.; Dove-Steinkamp, M.; Tibirica, L.; Bizarro, A.; CPH-NEW Research Team. The Intervention Design and Analysis Scorecard: A planning tool for participatory design of integrated health and safety interventions in the workplace. J. Occup. Environ. Med. 2013, 55, S86–S88. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, G.; Stoddard, A.; Ockene, J.K.; Hunt, M.K.; Youngstrom, R. Worker participation in an integrated health promotion health protection program: Results from the WellWorks project. Health Educ. Q. 1996, 23, 191–203. [Google Scholar] [CrossRef]
- Baker, E.A.; Israel, B.A.; Schurman, S.J. A participatory approach to worksite health promotion. J. Ambul. Care Manag. 1994, 17, 68–81. [Google Scholar] [CrossRef]
- Wallerstein, N.; Duran, B. Community-based participatory research contributions to intervention research: The intersection of science and practice to improve health equity. Am. J. Public Health 2010, 100, S40–S46. [Google Scholar] [CrossRef] [PubMed]
- Punnett, L.; Cherniack, M.; Henning, R.; Morse, T.; Faghri, P.; CPH-NEW Research Team. A conceptual framework for integrating workplace health promotion and occupational ergonomics programs. Public Health Rep. 2009, 124, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Kazutaka, K. Roles of Participatory Action-oriented Programs in Promoting Safety and Health at Work. Saf. Health Work 2012, 3, 155–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nobrega, S.; Champagne, N.; Abreu, M.; Goldstein-Gelb, M.; Montano, M.; Lopez, I.; Arevalo, J.; Bruce, S.; Punnett, L. Obesity/Overweight and the Role of Working Conditions: A Qualitative, Participatory Investigation. Health Promot. Pract. 2016, 17, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Nobrega, S.; Kernan, L.; Plaku-Alakbarova, B.; Robertson, M.; Warren, N.; Henning, R. Field tests of a participatory ergonomics toolkit for Total Worker Health. Appl. Ergon. 2017, 60, 366–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Center for the Promotion of Health in the New England Workplace. Evaluate your Program. Available online: https://www.uml.edu/Research/CPH-NEW/Healthy-Work-Participatory-Program/Evaluate-Your-Program/default.aspx (accessed on 31 January 2019).
- Robertson, M.M.; Henning, R.A.; Warren, N.; Nobrega, S.; Dove-Steinkamp, M.; Tibiriçá, L.; Bizarro, A. Participatory design of integrated safety and health interventions in the workplace: A case study using the Intervention Design and Analysis Scorecard (IDEAS) Tool. Int. J. Hum. Factors Ergon. 2015, 3, 303–326. [Google Scholar] [CrossRef]
- Tamers, S.L.; Goetzel, R.; Kelly, K.M.; Luckhaupt, S.; Nigam, J.; Pronk, N.P.; Rohlman, D.S.; Baron, S.; Brosseau, L.M.; Bushnell, T.; et al. Research Methodologies for Total Worker Health(R): Proceedings From a Workshop. J. Occup. Environ. Med. 2018, 60, 968–978. [Google Scholar] [CrossRef]
- Zhang, Y.; Flum, M.; Kotejoshyer, R.; Fleishman, J.; Henning, R.; Punnett, L. Workplace Participatory Occupational Health/Health Promotion Program: Facilitators and Barriers Observed in Three Nursing Homes. J. Gerontol. Nurs. 2016, 42, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Strickland, J.R.; Eyer, A.A.; Purnell, J.Q.; Kinghorn, A.M.; Herrick, C.; Evanoff, B.A. Enhancing Workplace Wellness Efforts to Reduce Obesity: A Qualitative Study of Low-Wage Workers in St Louis, Missouri, 2013–2014. Prev. Chronic Dis. 2015, 12, E67. [Google Scholar] [CrossRef]
- Strickland, J.R.; Pizzorno, G.; Kinghorn, A.M.; Evanoff, B. Worksite Influences on Obesogenic Behaviors in Low-Wage Workers in Saint Louis, Missouri, 2013–2014. Prev. Chronic Dis. 2015, 12, E66. [Google Scholar] [CrossRef] [PubMed]
- Center for the Promotion of Health in the New England Workplace. Intervention Design and Analysis Scorecard (IDEAS): CPH-NEW Intervention Planning Tool and Facilitator’s Guide. Available online: http://www.uml.edu/docs/FGuide_Mar3_Website_tcm18-102071.pdf (accessed on 31 January 2019).
- Center for the Promotion of Health in the New England Workplace. CPH-NEW Healthy Workplace Participatory Program. Available online: http://www.uml.edu/Research/Centers/CPH-NEW/Healthy-Work-Participatory-Program/default.aspx (accessed on 10 October 2016).
- Kristensen, T.S. Job stress and cardiovascular disease: A theoretic critical review. J. Occup. Health Psychol. 1996, 1, 246–260. [Google Scholar] [CrossRef] [PubMed]
- Gilbody, S.; Richards, D.; Brealey, S.; Hewitt, C. Screening for depression in medical settings with the Patient Health Questionnaire (PHQ): A diagnostic meta-analysis. J. Gen. Intern. Med. 2007, 22, 1596–1602. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. CDC National Healthy Worksite Program (NHWP) Employee Health Assessment (CAPTURE); Centers for Disease Control and Prevention: Atlanta, GA, USA, 2005. [Google Scholar]
- Fassi, M.E.; Bocquet, V.; Majery, N.; Lair, M.L.; Couffignal, S.; Mairiaux, P. Work ability assessment in a worker population: Comparison and determinants of Work Ability Index and Work Ability score. BMC Public Health 2013, 13, 305. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.Y.; Van Der Ploeg, H.P.; Dunn, S.; Kurko, J.; Bauman, A.E. Validity of the occupational sitting and physical activity questionnaire. Med. Sci. Sports Exerc. 2012, 44, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Segal-Isaacson, C.; Wylie-Rosett, J.; Gans, K. Validation of a short dietary assessment questionnaire: The Rapid Eating and Activity Assessment for Participants Short Version (REAP-S). Diabetes Educ. 2004, 30, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S.; Giles, W.H.; Dietz, W.H. Prevalence of the Metabolic Syndrome Among US AdultsFindings From the Third National Health and Nutrition Examination Survey. JAMA 2002, 287, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Zweber, Z.M. A Practical Scale for Multi-faceted Organizational Health Climate Assessment. Master’s Thesis, University of Conneticut, Storrs, CT, USA, 2012. [Google Scholar]
- Strickland, J.; Kinghorn, A.; Evanoff, B.; Dale, A. Experience Mapping to Convey Complex Data and Aid in the Design of Workplace Interventions. In Proceedings of the 12th International Conference on Occupational Stress and Health, Minneapolis, MN, USA, 7–10 June 2017. [Google Scholar]
- Center for the Promotion of Health in the New England Workplace. CPH-NEW Healthy Workplace Participatory Program: Select the Design Team. Available online: http://www.uml.edu/Research/Centers/CPH-NEW/Healthy-Work-Participatory-Program/form-design-team/select-team.aspx (accessed on 31 January 2019).
- Center for the Promotion of Health in the New England Workplace. CPH-NEW Healthy Workplace Participatory Program: Select Steering Committee. Available online: https://www.uml.edu/Research/CPH-NEW/Healthy-Work-Participatory-Program/steering-committee/role.aspx (accessed on 21 December 2018).
- Jaegers, L.; Dale, A.M.; Weaver, N.; Buchholz, B.; Welch, L.; Evanoff, B. Development of a program logic model and evaluation plan for a participatory ergonomics intervention in construction. Am. J. Ind. Med. 2014, 57, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Dale, A.M.; Jaegers, L.; Welch, L.; Gardner, B.T.; Buchholz, B.; Weaver, N.; Evanoff, B.A. Evaluation of a participatory ergonomics intervention in small commercial construction firms. Am. J. Ind. Med. 2016, 59, 465–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haines, H.; Wilson, J.R.; Vink, P.; Koningsveld, E. Validating a framework for participatory ergonomics (the PEF). Ergonomics 2002, 45, 309–327. [Google Scholar] [CrossRef]
- Driessen, M.T.; Proper, K.I.; Anema, J.R.; Bongers, P.M.; van der Beek, A.J. Process evaluation of a participatory ergonomics programme to prevent low back pain and neck pain among workers. Implement. Sci. 2010, 5, 65. [Google Scholar] [CrossRef] [PubMed]
- Pehkonen, I.; Takala, E.P.; Ketola, R.; Viikari-Juntura, E.; Leino-Arjas, P.; Hopsu, L.; Virtanen, T.; Haukka, E.; Holtari-Leino, M.; Nykyri, E.; et al. Evaluation of a participatory ergonomic intervention process in kitchen work. Appl. Ergon. 2009, 40, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Pretty, J.; Guijt, I.; Scoones, I.; Thompson, J. A Trainer’s Guide for Participatory Learning and Action; International Institute for Environment and Development: London, UK, 1995. [Google Scholar]
- Gjessing, C.C.; Schoenborn, T.F.; Cohen, A. Participatory Ergonomic Intervention in Meatpacking Plants; Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health: Washington, DC, USA, 1994.
- Burgess-Limerick, R. Participatory ergonomics: Evidence and implementation lessons. Appl. Ergon. 2018, 68, 289–293. [Google Scholar] [CrossRef]
- Dixon, S.M.; Theberge, N. Contextual factors affecting task distribution in two participatory ergonomic interventions: A qualitative study. Ergonomics 2011, 54, 1005–1016. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, L.; Faghri, P.D.; Henning, R.; Cherniack, M.; Center for the Promotion of Health in the New England Workplace Team. Workplace-based participatory approach to weight loss for correctional employees. J. Occup. Environ. Med. 2013, 55, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Parkinson, M.D. Employer Health and Productivity Roadmap strategy. J. Occup. Environ. Med. 2013, 55, S46–S51. [Google Scholar] [CrossRef] [PubMed]
- Goetzel, R.Z.; Ozminkowski, R.J. The Health and Cost Benefits of Work Site Health-Promotion Programs. Annu. Rev. Public Health 2008, 29, 303–323. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Mean (SD) | |
|---|---|
| Age | 42 (15.1) |
| BMI | 28.21 (6.3) |
| % | |
| Body Mass Index (BMI) Category | |
| Underweight | 1 |
| Normal weight | 37.3 |
| Overweight | 28.4 |
| Obese | 33.3 |
| Gender | |
| Female | 52.4 |
| Race | |
| African American | 37.5 |
| Caucasian | 53.8 |
| Other | 8.6 |
| Hispanic/Latino | 3 |
| Marital Status | |
| Married | 28.6 |
| Member of unmarried couple | 14.3 |
| Never married | 41.9 |
| Widowed | 4.8 |
| Divorced/separated | 10.5 |
| 1 or more children live in household | 40.4 |
| Highest level of education | |
| Less than high school | 1.9 |
| High school graduate or General Education Diploma | 35.6 |
| Postsecondary Education | 62.5 |
| Health Behaviors | |
| Often bring lunch from home | 12.5 |
| Eat the recommend amount of fruits | 34.2 |
| Eat the recommend amount of vegetables | 38.7 |
| Often eat fried foods | 17.5 |
| Drink 16oz or more of regular soda or sugary drinks daily | 24.2 |
| Eats sweets more than 2 times a day | 27.7 |
| Does not meet exercise recommendations | 45.2 |
| Considered increasing physical activity | 71.2 |
| Health Climate | |
| Believe organization is fully committed to employee wellness | 36.7 |
| Tried to control their weight in the last year | 68.3 |
| Stand in place for more than one hour | 43.5 |
| No energy to exercise | 39.2 |
| No energy for family | 33.3 |
| Exhausted after work | 61.7 |
| Process Measures & Indicators | Results |
|---|---|
| Inputs | |
| Fidelity to HWPP materials | |
| Used IDEAS Tool materials/worksheets as planned | Yes—minor language modifications |
| Design team members understood the materials/program process | Yes—design team members reported that materials were easy to understand, but didn’t always know the best way to move forward through program materials |
| Facilitator | |
| Knowledgeable about the HWPP & IDEAS Tool | Yes—thorough review of facilitator guide prior to program initiation |
| Knowledgeable about the workplace | Partial—external researcher with previous experience in this store |
| Time expenditure met expectations (~20 h) | No—greater than anticipated (57 h over 10 weeks) |
| Design Team | |
| Recruited 6–8 design team members | Yes—6 design team members |
| Met recruitment criteria | Yes—met all criteria |
| Design team members scheduled to work on meeting days | No—all design team members scheduled to work on only 2 of 9 meeting days |
| Steering Committee | |
| Steering committee represented various levels of authority | Partial—corporate, store supervisor, unions; store manager not involved |
| Activities | |
| Fidelity to the IDEAS Tool | |
| Design team completed IDEAS Steps 1–5A | Yes—completed Steps 1–5A; also partially completed Step 6 |
| Steering committee completed IDEAS Steps 5B–6 | Partiall—completed Step 5B; partially completed Step 6 |
| Dose | |
| Number/duration/frequency of design team meetings | 16 meetings; 50–60 min each; met weekly for 10 weeks, then as needed |
| Number/duration/frequency of steering committee meetings | 2 meetings; 60–90 min each; 7 months between meetings |
| Engagement | |
| Design team meeting attendance | All present at six of 16 scheduled meetings; one member absent at seven meetings; two or more members absent at three meetings |
| Steering committee meeting attendance | All present at 1 of 2 scheduled meetings; 2 members present at second meeting |
| Design team engagement (Facilitator mean rating for each design team members across all meetings; Scale: 0 = No, 0.5 = some/somewhat, 1 = Yes) | Offered new ideas during meetings = 0.86 |
| Actively participated in meeting = 0.88 | |
| Completed homework = 0.50 | |
| Discussed projects with co-workers = 0.81 | |
| Design team required significant facilitation to further develop and implement activities; facilitator took on a lot of activity development responsibility; team members reported they were not motivated to take initiative, however they often made a point to attend team meetings even when not scheduled to work (15 out of 20 instances) | |
| Design team perception of the process | Team members reported feeling positively impacted by the program and thought the program was innovative and important, but they did not know how to implement activities without help. |
| Design team perception of support | The team did not feel they received logistical support from store management to implement solutions and response time was slow. They also felt that the steering committee did not follow through on promises and took too long to respond to the team. |
| Steering committee perception of program | 1 of 6 steering committee members continued with the program until completion; one member was vocal about not believing in the program/process. |
| Activities generated | The design team generated 3 objectives with 15 distinct activities; the steering committee approved 7 activities |
| Outputs | |
| Store Worker Reach | |
| Activities implemented | 5 activities were implemented |
| Awareness of implemented solutions | Surveys: 99 of 105 workers noticed at least one activity implemented by the design team. Awareness varied by activities; Results shown in Table 3. |
| Utilization of implemented activities | Surveys: Participation in the activities was higher among workers who used the break room, where most of the activities were implemented and communicated to the workforce. Results shown in Table 3. |
| Store Workers’ Perception of Program | Surveys: 39 of 105 workers reported the activities helped them improve their eating and/or exercise habits |
| Worker interviews (n = 5): 4/5 thought the activities were good for store workers in general, but changes in their own health behaviors were made for other reasons, not due to program | |
| Objectives and Activities | Steering Committee Response to Proposal | Implemented (Yes/No)—Responsible Party | Store Workers | |
|---|---|---|---|---|
| Noticed (n = 105) | Used (n = 105) | |||
| Improve Store Communication | ||||
| Utilize email to communicate info | Agreed | No—store mgmt. | - | - |
| Use TV in break room for announcements | Agreed with modifications | No—store mgmt. | - | - |
| Develop better process for tracking and ordering supplies (identified as a stressor) | Not approved (said it was not relevant to the project) | N/A | - | - |
| Improve Diet at Work | ||||
| Get a bigger refrigerator for break room | Agreed | Yes—store mgmt. | 78% | 43% |
| Healthier options near checkout | Agreed | Yes (partial)—store mgmt. | 30% | 16% |
| Bottled water in break room | Agreed | Yes—design team | 81% | 47% |
| “Healthy choices” section | Wanted more details | No—design team | - | - |
| Include healthy options in $5 meals | Wanted more details | No—steering committee | - | - |
| Offer healthier premade meals and offer discount | Not approved (not profitable) | N/A | - | - |
| Add nutrition info and healthy recipes to recipe kiosks | Not approved (kiosks no longer used) | N/A | - | - |
| Reward workers for eating healthy | Wanted more details | No—design team | - | - |
| Increase Health Awareness | ||||
| Walking challenge with incentives | Agreed | Yes (Completed one 12-week challenge) —design team | 50% | 13% |
| Health focused newsletter | Agreed | Yes (2 delivered during study period)—design team | 45% | 25% |
| Gym/ Exercise class discounts | Need details from unions | No—steering committee | - | - |
| Add more health topics to the “Meet the Expert” class schedule & increase the number of classes | Not approved (no longer offer classes) | N/A | - | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strickland, J.R.; Kinghorn, A.M.; Evanoff, B.A.; Dale, A.M. Implementation of the Healthy Workplace Participatory Program in a Retail Setting: A Feasibility Study and Framework for Evaluation. Int. J. Environ. Res. Public Health 2019, 16, 590. https://doi.org/10.3390/ijerph16040590
Strickland JR, Kinghorn AM, Evanoff BA, Dale AM. Implementation of the Healthy Workplace Participatory Program in a Retail Setting: A Feasibility Study and Framework for Evaluation. International Journal of Environmental Research and Public Health. 2019; 16(4):590. https://doi.org/10.3390/ijerph16040590
Chicago/Turabian StyleStrickland, Jaime R., Anna M. Kinghorn, Bradley A. Evanoff, and Ann Marie Dale. 2019. "Implementation of the Healthy Workplace Participatory Program in a Retail Setting: A Feasibility Study and Framework for Evaluation" International Journal of Environmental Research and Public Health 16, no. 4: 590. https://doi.org/10.3390/ijerph16040590
APA StyleStrickland, J. R., Kinghorn, A. M., Evanoff, B. A., & Dale, A. M. (2019). Implementation of the Healthy Workplace Participatory Program in a Retail Setting: A Feasibility Study and Framework for Evaluation. International Journal of Environmental Research and Public Health, 16(4), 590. https://doi.org/10.3390/ijerph16040590