Environmental and Genetic Factors in Autism Spectrum Disorders: Special Emphasis on Data from Arabian Studies

 ,
, 


Abstract
:1. Introduction
2. Diagnosis
3. Public Health Impact
4. Epidemiology
5. Etiology
6. Genetic Factors
6.1. Genetic Studies of ASD
6.2. Cytogenetic Studies
6.3. Copy Number Variation (CNV) Analysis
6.4. Linkage and Association Studies
6.5. Microarray Analysis
6.6. Genome-Wide Association Studies
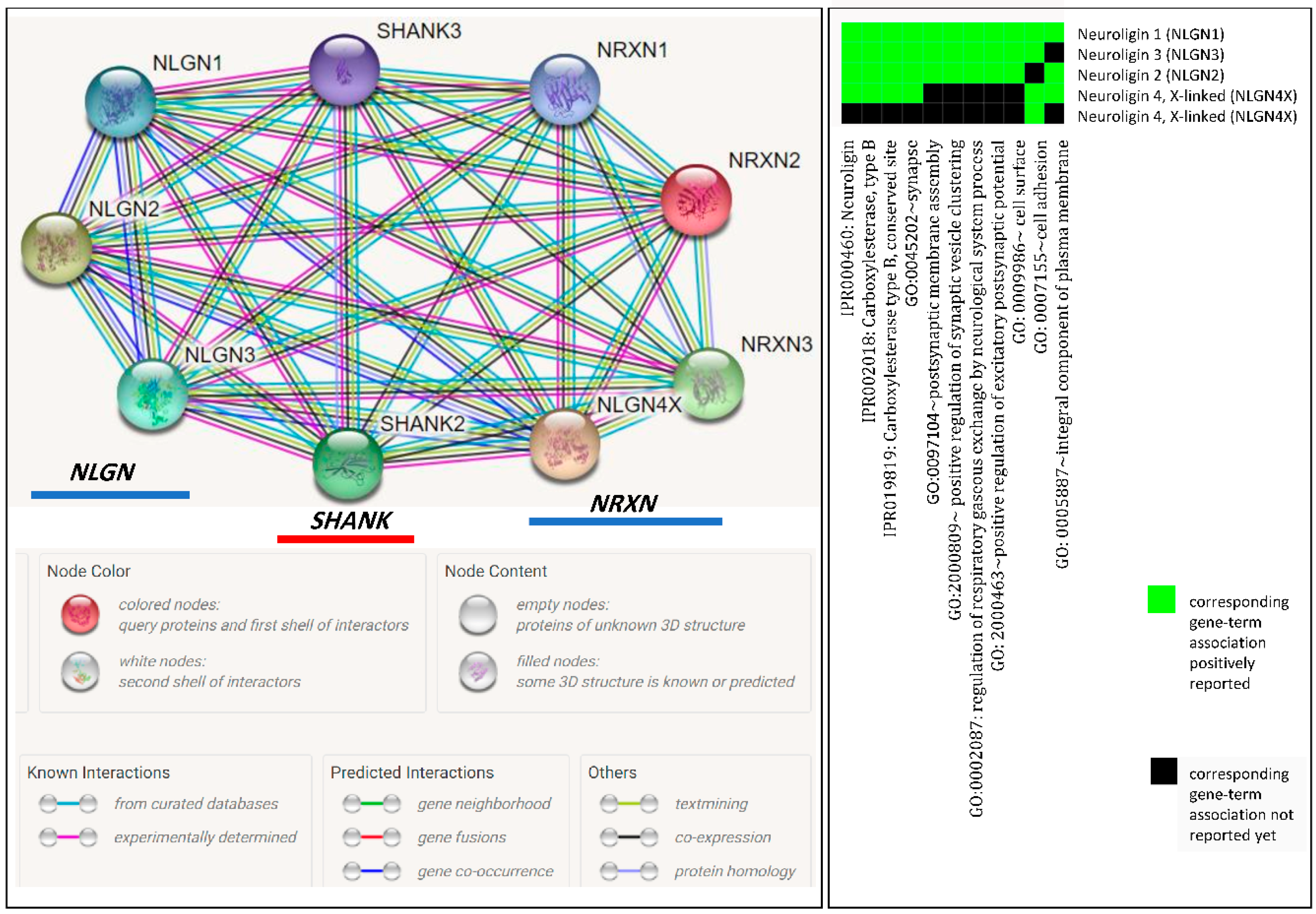
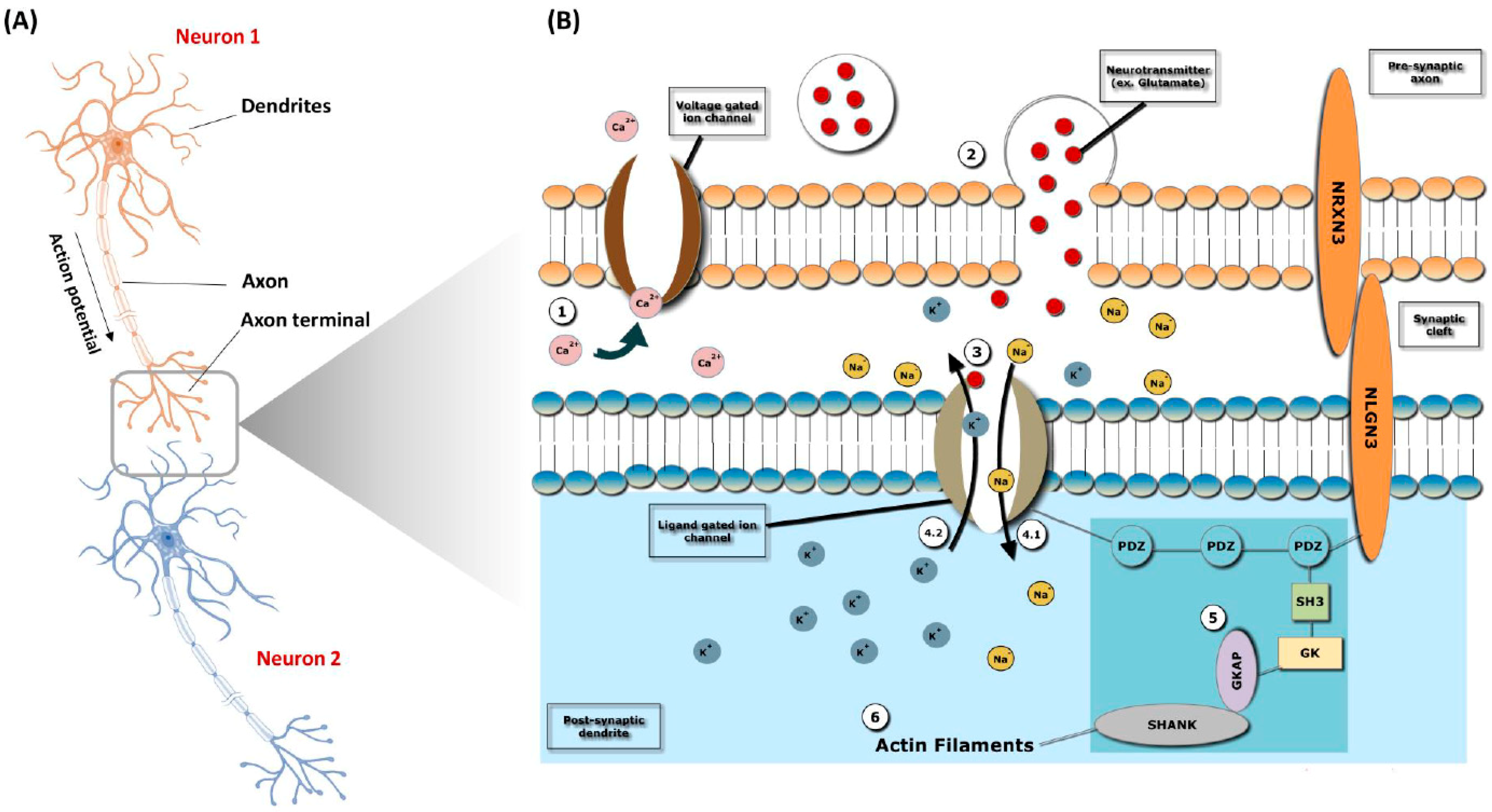
7. Synaptic Genes
Mechanism of Action
8. Environmental Factors
8.1. Parental Age
8.2. Medication Use During Pregnancy
8.3. Maternal Smoking and Alcohol Consumption
8.4. Vaccination
9. Management Strategies
Medications
10. Impact on Families
11. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Faras, H.; AlAteeqi, N.; Tidmarsh, L. Autism spectrum disorders. Ann. Saudi. Med. 2010, 30, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zou, H.; Brown, W.T. Genes associated with autism spectrum disorder. Brain Res. Bull. 2012, 88, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Geschwind, D.H. Genetics of autism spectrum disorders. Trends Cogn. Sci. 2011, 15, 409–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub.: Washington, DC, USA, 22 May 2013. [Google Scholar]
- Lyall, K.; Croen, L.; Daniels, J.; Fallin, M.D.; Ladd-Acosta, C.; Lee, B.K.; Park, B.Y.; Snyder, N.W.; Schendel, D.; Volk, H.; et al. The changing epidemiology of autism spectrum disorders. Annu. Rev. Public Health 2017, 38, 81–102. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.P.; Myers, S.M. Identification and evaluation of children with autism spectrum disorders. Pediatrics 2007, 120, 1183–1215. [Google Scholar] [CrossRef] [PubMed]
- Szatmari, P.; Chawarska, K.; Dawson, G.; Georgiades, S.; Landa, R.; Lord, C.; Messinger, D.S.; Thurm, A.; Halladay, A. Prospective longitudinal studies of infant siblings of children with autism: Lessons learned and future directions. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.B.; Moore, E.L.; Northrup, J.; Brownell, C.A. Developmental changes in empathic concern and self-understanding in toddlers at genetic risk for autism spectrum disorder. J. Autism Dev. Disord. 2017, 7, 2690–2702. [Google Scholar] [CrossRef] [PubMed]
- Al-Zaalah, M.A.; Al-asmari, A.H.; Al-malki, H.H.; Al-shehri, N.M.; Al-moalwi, N.M. Characteristics of Autism Spectrum Disorder among Saudi Children and its Impact on their Families. Neurologist 2015, 31, 13–16. [Google Scholar]
- Baird, G.; Simonoff, E.; Pickles, A.; Chandler, S.; Loucas, T.; Meldrum, D.; Charman, T. Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: The Special Needs and Autism Project (SNAP). Lancet 2006, 368, 210–215. [Google Scholar] [CrossRef]
- Kogan, M.D.; Blumberg, S.J.; Schieve, L.A.; Boyle, C.A.; Perrin, J.M.; Ghandour, R.M.; Singh, G.K.; Strickland, B.B.; Trevathan, E.; van Dyck, P.C. Prevalence of parent-reported diagnosis of autism spectrum disorder among children in the US, 2007. Pediatrics 2009, 124, 1395–1403. [Google Scholar] [CrossRef] [PubMed]
- Lintas, C.; Persico, A.M. Autistic phenotypes and genetic testing: State-of-the-art for the clinical geneticist. J. Med. Genet. 2008, 26, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Salhia, H.O.; Al-Nasser, L.A.; Taher, L.S.; Al-Khathaami, A.M.; El-Metwally, A.A. Systemic review of the epidemiology of autism in Arab Gulf countries. Neurosciences 2014, 19, 291. [Google Scholar] [PubMed]
- Yazbak, F.E. Autism seems to be increasing worldwide, if not in London. BMJ 2004, 328, 226–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aljarallah, A.; Alwaznah, T.; Alnasari, S.; Alhazmi, M. A Study of Autism and Developmental Disorders in Saudi Children; Report; King Abdulaziz City for Science and Technology: Riyadh, Saudi Arabia, 2007. [Google Scholar]
- Al-Zahrani, A. Prevalence and clinical characteristics of autism spectrum disorders in school-age children in Taif-KSA. Int. J. Med. Sci. Public Health 2013, 2, 578–582. [Google Scholar] [CrossRef]
- Al-Farsi, Y.M.; Al-Sharbati, M.M.; Al-Farsi, O.A.; Al-Shafaee, M.S.; Brooks, D.R.; Waly, M.I. Brief report: Prevalence of autistic spectrum disorders in the Sultanate of Oman. J. Autism Dev. Disord. 2011, 41, 821–825. [Google Scholar] [CrossRef] [PubMed]
- Eapen, V.; Mabrouk, A.A.; Zoubeidi, T.; Yunis, F. Prevalence of pervasive developmental disorders in preschool children in the UAE. J. Trop. Pediatr. 2007, 53, 202–205. [Google Scholar] [CrossRef] [PubMed]
- Al-Ansari, A.M.; Ahmed, M.M. Epidemiology of autistic disorder in Bahrain: Prevalence and obstetric and familial characteristics. East. Mediterr. Health J. 2013, 19, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Al-Salehi, S.M.; Al-Hifthy, E.H.; Ghaziuddin, M. Autism in Saudi Arabia: Presentation, clinical correlates and comorbidity. Transcult. Psychiatry 2009, 46, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Caglayan, A.O. Genetic causes of syndromic and non-syndromic autism. Dev. Med. Child. Neurol. 2010, 52, 130–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrahams, B.S.; Geschwind, D.H. Advances in autism genetics: On the threshold of a new neurobiology. Nat. Rev. Genet. 2008, 9, 341. [Google Scholar] [CrossRef] [PubMed]
- Bailey, A.; Le Couteur, A.; Gottesman, I.; Bolton, P.; Simonoff, E.; Yuzda, E.; Rutter, M. Autism as a strongly genetic disorder: Evidence from a British twin study. Psychol. Med. 1995, 25, 63–77. [Google Scholar] [CrossRef] [PubMed]
- Morales, D.R.; Slattery, J.; Evans, S.; Kurz, X. Antidepressant use during pregnancy and risk of autism spectrum disorder and attention deficit hyperactivity disorder: Systematic review of observational studies and methodological considerations. BMC Med. 2018, 16, 6. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, E.J.; State, M.W. Progress in cytogenetics: Implications for child psychopathology. J. Am. Acad. Child. Adolesc. Psychiatry 2010, 49, 736–751. [Google Scholar] [CrossRef] [PubMed]
- Vorstman, J.A.S.; Staal, W.G.; Van Daalen, E.; Van Engeland, H.; Hochstenbach, P.F.R.; Franke, L. Identification of novel autism candidate regions through analysis of reported cytogenetic abnormalities associated with autism. Mol. Psychiatry 2006, 11, 18. [Google Scholar] [CrossRef] [PubMed]
- Bakkaloglu, B.; O’Roak, B.J.; Louvi, A.; Gupta, A.R.; Abelson, J.F.; Morgan, T.M.; Chawarska, K.; Klin, A.; Ercan-Sencicek, A.G.; Stillman, A.A.; et al. Molecular cytogenetic analysis and resequencing of contactin associated protein-like 2 in autism spectrum disorders. Am. J. Hum. Genet. 2008, 82, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Reddy, K.S. Cytogenetic abnormalities and fragile-X syndrome in Autism Spectrum Disorder. BMC Med. Genet. 2005, 6, 3. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.L.; Duvall, J.A.; Ilkin, Y.; Simon, J.S.; Arreaza, M.G.; Wilkes, K.; Alvarez-Retuerto, A.; Whichello, A.; Powell, C.M.; Rao, K.; et al. Cytogenetic and molecular characterization of A2BP1/FOX1 as a candidate gene for autism. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2007, 144, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Lukusa, T.; Vermeesch, J.R.; Holvoet, M.; Fryns, J.P.; Devriendt, K. Deletion 2q37.3 and autism: Molecular cytogenetic mapping of the candidate region for autistic disorder. Genet. Couns. 2004, 15, 293–301. [Google Scholar] [PubMed]
- Piggot, J.; Shirinyan, D.; Shemmassian, S.; Vazirian, S.; Alarcon, M. Neural systems approaches to the neurogenetics of autism spectrum disorders. Neuroscience 2009, 164, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Pinto, D.; Pagnamenta, A.T.; Klei, L.; Anney, R.; Merico, D.; Regan, R.; Conroy, J.; Magalhaes, T.R.; Correia, C.; Abrahams, B.S.; et al. Functional impact of global rare copy number variation in autism spectrum disorders. Nature 2010, 466, 368. [Google Scholar] [CrossRef] [PubMed]
- Glessner, J.T.; Wang, K.; Cai, G.; Korvatska, O.; Kim, C.E.; Wood, S.; Zhang, H.; Estes, A.; Brune, C.W.; Bradfield, J.P.; et al. Autism genome-wide copy number variation reveals ubiquitin and neuronal genes. Nature 2009, 459, 569. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.; Ronemus, M.; Yamrom, B.; Lee, Y.H.; Leotta, A.; Kendall, J.; Marks, S.; Lakshmi, B.; Pai, D.; Ye, K.; et al. Rare de novo and transmitted copy-number variation in autistic spectrum disorders. Neuron 2011, 70, 886–897. [Google Scholar] [CrossRef] [PubMed]
- Sebat, J.; Lakshmi, B.; Malhotra, D.; Troge, J.; Lese-Martin, C.; Walsh, T.; Yamrom, B.; Yoon, S.; Krasnitz, A.; Kendall, J.; et al. Strong association of de novo copy number mutations with autism. Science 2007, 316, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Girirajan, S.; Dennis, M.Y.; Baker, C.; Malig, M.; Coe, B.P.; Campbell, C.D.; Mark, K.; Vu, T.H.; Alkan, C.; Cheng, Z.; et al. Refinement and discovery of new hotspots of copy-number variation associated with autism spectrum disorder. Am. J. Hum. Genet. 2013, 92, 221–237. [Google Scholar] [CrossRef] [PubMed]
- Maestrini, E.; Pagnamenta, A.T.; Lamb, J.A.; Bacchelli, E.; Sykes, N.H.; Sousa, I.; Toma, C.; Barnby, G.; Butler, H.; Winchester, L.; et al. High-density SNP association study and copy number variation analysis of the AUTS1 and AUTS5 loci implicate the IMMP2L–DOCK4 gene region in autism susceptibility. Mol. Psychiatry 2010, 15, 954. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Yu, S.; Fu, Y.; Li, X. Synaptic proteins and receptors defects in autism spectrum disorders. Front. Cell. Neurosci. 2014, 8, 276. [Google Scholar] [CrossRef] [PubMed]
- Dean, C.; Dresbach, T. Neuroligins and neurexins: Linking cell adhesion, synapse formation and cognitive function. Trends Neurosci. 2006, 29, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Buxbaum, J.D.; Silverman, J.; Keddache, M.; Smith, C.J.; Hollander, E.; Ramoz, N.; Reichert, J.G. Linkage analysis for autism in a subset families with obsessive–compulsive behaviors: Evidence for an autism susceptibility gene on chromosome 1 and further support for susceptibility genes on chromosome 6 and 19. Mol. Psychiatry 2004, 9, 144. [Google Scholar] [CrossRef] [PubMed]
- Szatmari, P.; Paterson, A.D.; Zwaigenbaum, L.; Roberts, W.; Brian, J.; Liu, X.Q.; Vincent, J.B.; Skaug, J.L.; Thompson, A.P.; Senman, L.; et al. Mapping autism risk loci using genetic linkage and chromosomal rearrangements. Nat. Genet. 2007, 39, 319. [Google Scholar] [PubMed]
- Alarcón, M.; Abrahams, B.S.; Stone, J.L.; Duvall, J.A.; Perederiy, J.V.; Bomar, J.M.; Sebat, J.; Wigler, M.; Martin, C.L.; Ledbetter, D.H.; et al. Linkage, association, and gene-expression analyses identify CNTNAP2 as an autism-susceptibility gene. Am. J. Hum. Genet. 2008, 82, 150–159. [Google Scholar] [CrossRef] [PubMed]
- McCauley, J.L.; Olson, L.M.; Dowd, M.; Amin, T.; Steele, A.; Blakely, R.D.; Folstein, S.E.; Haines, J.L.; Sutcliffe, J.S. Linkage and association analysis at the serotonin transporter (SLC6A4) locus in a rigid-compulsive subset of autism. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2004, 127, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Jamain, S.; Betancur, C.; Quach, H.; Philippe, A.; Fellous, M.; Giros, B.; Gillberg, C.; Leboyer, M.; Bourgeron, T. Linkage and association of the glutamate receptor 6 gene with autism. Mol. Psychiatry 2002, 7, 302. [Google Scholar] [CrossRef] [PubMed]
- Tammimies, K.; Marshall, C.R.; Walker, S.; Kaur, G.; Thiruvahindrapuram, B.; Lionel, A.C.; Yuen, R.K.; Uddin, M.; Roberts, W.; Weksberg, R.; et al. Molecular diagnostic yield of chromosomal microarray analysis and whole-exome sequencing in children with autism spectrum disorder. JAMA 2015, 314, 895–903. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, A.; Doccini, V.; Bernardini, L.; Novelli, A.; Loddo, S.; Capalbo, A.; Filippi, T.; Carey, J.C. Confirmation of chromosomal microarray as a first-tier clinical diagnostic test for individuals with developmental delay, intellectual disability, autism spectrum disorders and dysmorphic features. Eur. J. Paediatr. Neurol. 2013, 17, 589–599. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.L.; Hovanes, K.; Dasouki, M.; Manzardo, A.M.; Butler, M.G. Chromosomal microarray analysis of consecutive individuals with autism spectrum disorders or learning disability presenting for genetic services. Gene 2014, 535, 70–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGrew, S.G.; Peters, B.R.; Crittendon, J.A.; Veenstra-VanderWeele, J. Diagnostic yield of chromosomal microarray analysis in an autism primary care practice: Which guidelines to implement? J. Autism Dev. Disord. 2012, 42, 1582–1591. [Google Scholar] [CrossRef] [PubMed]
- Al-Mubarak, B.; Abouelhoda, M.; Omar, A.; AlDhalaan, H.; Aldosari, M.; Nester, M.; Alshamrani, H.A.; El-Kalioby, M.; Goljan, E.; Albar, R.; et al. Whole exome sequencing reveals inherited and de novo variants in autism spectrum disorder: A trio study from Saudi families. Sci. Rep. 2017, 7, 5679. [Google Scholar] [CrossRef] [PubMed]
- Yuen, R.K.; Merico, D.; Bookman, M.; Howe, J.L.; Thiruvahindrapuram, B.; Patel, R.V.; Whitney, J.; Deflaux, N.; Bingham, J.; Wang, Z.; et al. Whole genome sequencing resource identifies 18 new candidate genes for autism spectrum disorder. Nat. Neurosci. 2017, 20, 602. [Google Scholar] [CrossRef] [PubMed]
- Bishop, S.L.; Farmer, C.; Bal, V.; Robinson, E.B.; Willsey, A.J.; Werling, D.M.; Havdahl, K.A.; Sanders, S.J.; Thurm, A. Identification of developmental and behavioral markers associated with genetic abnormalities in autism spectrum disorder. Am. J. Psychiatry 2017, 174, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Zhang, H.; Ma, D.; Bucan, M.; Glessner, J.T.; Abrahams, B.S.; Salyakina, D.; Imielinski, M.; Bradfield, J.P.; Sleiman, P.M.; et al. Common genetic variants on 5p14. 1 associate with autism spectrum disorders. Nature 2009, 459, 528. [Google Scholar] [CrossRef] [PubMed]
- Kerin, T.; Ramanathan, A.; Rivas, K.; Grepo, N.; Coetzee, G.A.; Campbell, D.B. A noncoding RNA antisense to moesin at 5p14. 1 in autism. Sci. Transl. Med. 2012, 4, 128ra40. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.; Salyakina, D.; Jaworski, J.M.; Konidari, I.; Whitehead, P.L.; Andersen, A.N.; Hoffman, J.D.; Slifer, S.H.; Hedges, D.J.; Cukier, H.N.; et al. A genome-wide association study of autism reveals a common novel risk locus at 5p14. 1. Ann. Hum. Genet. 2009, 73, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Weiss, L.A.; Arking, D.E. Gene Discovery Project of Johns Hopkins the Autism Consortium. A genome-wide linkage and association scan reveals novel loci for autism. Nature 2009, 461, 802. [Google Scholar] [CrossRef] [PubMed]
- Anney, R.; Klei, L.; Pinto, D.; Regan, R.; Conroy, J.; Magalhaes, T.R.; Correia, C.; Abrahams, B.S.; Sykes, N.; Pagnamenta, A.T.; et al. A genome-wide scan for common alleles affecting risk for autism. Hum. Mol. Genet. 2010, 19, 4072–4082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, S.C.; Yoo, H.J.; Park, M.; Cho, I.H.; Kim, B.N.; Kim, J.W.; Shin, M.S.; Park, T.W.; Son, J.W.; Chung, U.S.; et al. Genome-wide association scan of korean autism spectrum disorders with language delay: A preliminary study. Psychiatry Investig. 2011, 8, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Connolly, J.J.; Glessner, J.T.; Hakonarson, H. A Genome-Wide Association Study of Autism Incorporating Autism Diagnostic Interview–Revised, Autism Diagnostic Observation Schedule, and Social Responsiveness Scale. Child. Dev. 2013, 84, 17–33. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H. Genetics of autism spectrum disorder: Current status and possible clinical applications. Exp. Neurobiol. 2015, 24, 257–272. [Google Scholar] [CrossRef] [PubMed]
- Meyer, G.; Varoqueaux, F.; Neeb, A.; Oschlies, M.; Brose, N. The complexity of PDZ domain-mediated interactions at glutamatergic synapses: A case study on neuroligin. Neuropharmacology 2004, 47, 724–733. [Google Scholar] [CrossRef] [PubMed]
- Varoqueaux, F.; Aramuni, G.; Rawson, R.L.; Mohrmann, R.; Missler, M.; Gottmann, K.; Zhang, W.; Südhof, T.C.; Brose, N. Neuroligins determine synapse maturation and function. Neuron 2006, 51, 741–754. [Google Scholar] [CrossRef] [PubMed]
- Khadka, S.; Pearlson, G.D.; Calhoun, V.D.; Liu, J.; Gelernter, J.; Bessette, K.L.; Stevens, M.C. Multivariate Imaging Genetics Study of MRI Gray Matter Volume and SNPs Reveals Biological Pathways Correlated with Brain Structural Differences in Attention Deficit Hyperactivity Disorder. Front. Psychiatry 2016, 25, 128. [Google Scholar] [CrossRef] [PubMed]
- Hegerl, U.; Hensch, T. The vigilance regulation model of affective disorders and ADHD. Neurosci. Biobehav. Rev. 2014, 44, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Giovedí, S.; Corradi, A.; Fassio, A.; Benfenati, F. Involvement of synaptic genes in the pathogenesis of autism spectrum disorders: The case of synapsins. Front. Pediatrics 2014, 2, 94. [Google Scholar] [CrossRef] [PubMed]
- Harper, C.B.; Mancini, G.M.; van Slegtenhorst, M.; Cousin, M.A. Altered synaptobrevin-II trafficking in neurons expressing a synaptophysin mutation associated with a severe neurodevelopmental disorder. Neurobiol. Dis. 2017, 108, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Gentile, S. Risks of neurobehavioral teratogenicity associated with prenatal exposure to valproate monotherapy: A systematic review with regulatory repercussions. CNS Spectr. 2014, 19, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T.; Matsuyama, T.; Takeuchi, M.; Ito, S. Autism spectrum disorder and prenatal exposure to selective serotonin reuptake inhibitors: A systematic review and meta-analysis. Reprod. Toxicol. 2016, 65, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Modabbernia, A.; Velthorst, E.; Reichenberg, A. Environmental risk factors for autism: An evidence-based review of systematic reviews and meta-analyses. Mol. Autism 2017, 8, 13. [Google Scholar] [CrossRef] [PubMed]
- Jansen, V.A.; Stollenwerk, N.; Jensen, H.J.; Ramsay, M.E.; Edmunds, W.J.; Rhodes, C.J. Measles outbreaks in a population with declining vaccine uptake. Science 2003, 8, 804. [Google Scholar] [CrossRef] [PubMed]
- Madsen, K.M.; Hviid, A.; Vestergaard, M.; Schendel, D.; Wohlfahrt, J.; Thorsen, P.; Olsen, J.; Melbye, M. A population-based study of measles, mumps, and rubella vaccination and autism. N. Engl. J. Med. 2002, 347, 1477–1482. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.E.; Swerdfeger, A.L.; Eslick, G.D. Vaccines are not associated with autism: An evidence-based meta-analysis of case-control and cohort studies. Vaccine 2014, 32, 3623–3629. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.; Chadman, K.K.; McCloskey, D.P.; Sheikh, A.M.; Malik, M.; Brown, W.T.; Li, X. Brain IL-6 elevation causes neuronal circuitry imbalances and mediates autism-like behaviors. Biochim. Biophys. Acta. 2012, 1822, 831–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gherardi, R.K.; Eidi, H.; Crépeaux, G.; Authier, F.J.; Cadusseau, J. Biopersistence and brain translocation of aluminum adjuvants of vaccines. Front. Neurol. 2015, 6, 4. [Google Scholar] [CrossRef] [PubMed]
- Sen, B.; Borle, N.C.; Greiner, R.; Brown, M.R. A general prediction model for the detection of ADHD and Autism using structural and functional MRI. PLoS ONE 2018, 17, e0194856. [Google Scholar] [CrossRef] [PubMed]
- Frodl, T.; Skokauskas, N. Meta-analysis of structural MRI studies in children and adults with attention deficit hyperactivity disorder indicates treatment effects. Acta Psychiatr. Scand. 2012, 125, 114–126. [Google Scholar] [CrossRef] [PubMed]
- Wood, J.J.; Ehrenreich-May, J.; Alessandri, M.; Fujii, C.; Renno, P.; Laugeson, E.; Murphy, T.K. Cognitive behavioral therapy for early adolescents with autism spectrum disorders and clinical anxiety: A randomized, controlled trial. Behav. Therapy 2015, 46, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Di Martino, A.; Tuchman, R.F. Antiepileptic drugs: Affective use in autism spectrum disorders. Pediatr. Neurol. 2001, 25, 199–207. [Google Scholar] [CrossRef]
- LeClerc, S.; Easley, D. Pharmacological therapies for autism spectrum disorder: A review. Pharm. Ther. 2015, 40, 389. [Google Scholar]
- Zhang, Y.; Hodgson, N.W.; Trivedi, M.S.; Abdolmaleky, H.M.; Fournier, M.; Cuenod, M.; Do, K.Q.; Deth, RC. Decreased brain levels of vitamin B12 in aging, autism and schizophrenia. PLoS ONE 2016, 11, e0146797. [Google Scholar] [CrossRef] [PubMed]
- Hendren, R.L.; James, S.J.; Widjaja, F.; Lawton, B.; Rosenblatt, A.; Bent, S. Randomized, placebo-controlled trial of methyl B12 for children with autism. J. Child. Adolesc. Psychopharmacol. 2016, 26, 774–783. [Google Scholar] [CrossRef] [PubMed]
- Damore, J.; Stine, J.; Brody, L. Medication-induced Hypomania in—Asperger’s Disorder. J. Am. Acad. Child. Adolesc. Psychiatry 1998, 37, 248–249. [Google Scholar] [CrossRef] [PubMed]
- Childs, J.A.; Blair, J.L. Valproic acid treatment of epilepsy in autistic twins. J. Neurosci. Nurs. 1997, 29, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Plioplys, A.V. Autism: Electroencephalogram abnormalities and clinical improvement with valproic acid. Arch. Pediatr. Adolesc. Med. 1994, 148, 220–222. [Google Scholar] [CrossRef] [PubMed]
- Nass, R.; Petrucha, D. Acquired aphasia with convulsive disorder: A pervasive developmental disorder variant. J. Child. Neurol 1990, 5, 327–328. [Google Scholar] [CrossRef] [PubMed]
- Gillberg, C.; Schaumann, H. Epilepsy Presenting as Infantile Autism-Two Case Studies. Neuropediatrics 1983, 14, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Sovner, R. The use of valproate in the treatment of mentally retarded persons with typical and atypical bipolar disorders. J. Clin. Psychiatry 1989, 50, 40–43. [Google Scholar] [PubMed]
- Rittey, C.D. Case summary: Benjamin. Seizure 1994, 3, 25–27. [Google Scholar] [PubMed]
- Deonna, T.; Ziegler, A.L.; Moura-Serra, J.; Innocenti, G. Autistic regression in relation to limbic pathology and epilepsy: Report of two cases. Dev. Med. Child. Neurol 1993, 35, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Komoto, J.; Usui, S.; Hirata, J. Infantile autism and affective disorder. J. Autism Dev. Disord. 1984, 14, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Uvebrant, P.; Bauzienè, R. Intractable epilepsy in children. The efficacy of lamotrigine treatment, including non-seizure-related benefits. Neuropediatrics 1994, 25, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Banach, M.; Iudice, J.; Conway, L.; Couse, L.J. Family support and empowerment: Post autism diagnosis support group for parents. Soc. Work Groups 2010, 12, 69–83. [Google Scholar] [CrossRef]
- Dabrowska, A.; Pisula, E. Parenting stress and coping styles in mothers and fathers of pre-school children with autism and Down syndrome. J. Intellect. Disabil. Res. 2010, 54, 266–280. [Google Scholar] [CrossRef] [PubMed]
- Autism Society. 2011. Available online: http://www.autism-society.org (accessed on 5 June 2018).
- Crane, L.; Chester, J.W.; Goddard, L.; Henry, L.A.; Hill, E. Experiences of autism diagnosis: A survey of over 1000 parents in the United Kingdom. Autism 2016, 20, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Qoronfleh, M.W.; Essa, M.M.; Alharahsheh, S.T.; Al-Farsi, Y.M.; Al-Adawi, S. Autism in the Gulf States: A regional overview. Front. Biosci. (Landmark Ed.) 2019, 24, 334–346. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Country | Prevalence | Reference |
|---|---|---|
| Oman | 1.4 per 10,000 | [17] |
| UAE | 29 per 10,000 | [18] |
| Bahrain | 4.3 per 10,000 | [19] |
| Saudi Arabia | No proper prevalence to date, but several studies mentioned the number of autistic patients | [14,20] |
| Kuwait | None | None |
| Qatar | None | None |
| EEG Findings * | AED Used | Behavioral Improvement | Reference |
|---|---|---|---|
| Normal | Valproic acid | Present | [81] |
| Abnormal | Valproic acid | Present | [82] |
| Abnormal | Valproic acid | Present | [83] |
| Abnormal | Valproic acid | Present | [84] |
| Abnormal | Valproic acid | Present | [85] |
| Normal | Valproic acid | Present | [86] |
| Abnormal | Carbamazepine | Not present | [87] |
| Abnormal | Carbamazepine | Present | [88] |
| Abnormal | Carbamazepine | Present | [89] |
| Abnormal | Lamotrigine | Present | [90] |
| Condition | Drugs |
|---|---|
| Irritability and aggression | Risperidone, aripiprazole, clozapine, haloperidol, sertraline |
| Aberrant social behavior | Oxytocin, secretin |
| Hyperactivity and inattention | Methylphenidate, venlafaxine |
| Repetitive behaviors | Fluoxetine, citalopram, bumetanide |
| Cognitive disorders | Memantine, rivastigmine |
| Insomnia | Mirtazapine, melatonin |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almandil, N.B.; Alkuroud, D.N.; AbdulAzeez, S.; AlSulaiman, A.; Elaissari, A.; Borgio, J.F. Environmental and Genetic Factors in Autism Spectrum Disorders: Special Emphasis on Data from Arabian Studies. Int. J. Environ. Res. Public Health 2019, 16, 658. https://doi.org/10.3390/ijerph16040658
Almandil NB, Alkuroud DN, AbdulAzeez S, AlSulaiman A, Elaissari A, Borgio JF. Environmental and Genetic Factors in Autism Spectrum Disorders: Special Emphasis on Data from Arabian Studies. International Journal of Environmental Research and Public Health. 2019; 16(4):658. https://doi.org/10.3390/ijerph16040658
Chicago/Turabian StyleAlmandil, Noor B., Deem N. Alkuroud, Sayed AbdulAzeez, Abdulla AlSulaiman, Abdelhamid Elaissari, and J. Francis Borgio. 2019. "Environmental and Genetic Factors in Autism Spectrum Disorders: Special Emphasis on Data from Arabian Studies" International Journal of Environmental Research and Public Health 16, no. 4: 658. https://doi.org/10.3390/ijerph16040658
APA StyleAlmandil, N. B., Alkuroud, D. N., AbdulAzeez, S., AlSulaiman, A., Elaissari, A., & Borgio, J. F. (2019). Environmental and Genetic Factors in Autism Spectrum Disorders: Special Emphasis on Data from Arabian Studies. International Journal of Environmental Research and Public Health, 16(4), 658. https://doi.org/10.3390/ijerph16040658