Migrant Workers from the Eastern-Mediterranean Region and Occupational Injuries: A Retrospective Database-Based Analysis from North-Eastern Italy




Abstract
:1. Background
2. Material and Methods
2.1. Setting
2.2. Occupational Injuries
2.3. Metereological Data
2.4. Statistical Analysis
2.5. Ethical Approval
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Giraudo, M.; Bena, A.; Costa, G. Migrant workers in Italy: An analysis of injury risk taking into account occupational characteristics and job tenure. BMC Public Health 2017, 17, 351. [Google Scholar] [CrossRef] [PubMed]
- Kassar, H.; Marzouk, D.; Anwar, W.A.; Lakhoua, C.; Hemminki, K.; Khyatti, M. Emigration flows from North Africa to Europe. Eur. J. Publ. Health 2014, 24, 2–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sweileh, W.M. Global output of research on the health of international migrant workers from 2000 to 2017. Glob. Health 2018, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Schmahl, F.W.; Metzler, B. The health risks of occupational stress in islamic industrial workers during the Ramadan fasting period. Pol. J. Occup. Med. Environ. Health 1991, 4, 219–228. [Google Scholar] [PubMed]
- Mertens, A.; Schouteden, M.; Godderis, L. Influence of Ramadan on neuroperformance in healthy workers. Med. Res. Arch. 2015, 3, 1–11. [Google Scholar] [CrossRef]
- Ovayolu, O.; Ovayolu, N.; Tasan, E. Does Ramadan Fasting Affect Fatigue in Nurses? Holist. Nurs. Pract. 2016, 30, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Khalfallah, T.; Chaari, N.; Henchi, M.A.; Abdallah, B.; Chikh, R.B.; Saafi, M.A.; Akrout, M. Evaluation of the impact of Ramadan fasting on the physical workload. Arch. Mal. Prof. Env. 2004, 65, 564–570. [Google Scholar]
- Laraqui, S.; Manar, N.; Laraqui, O.; Caubet, A.; Verger, C.; Laraqui, C.H. Influence of Ramadan observance on wakefulness at work among health care workers in Morocco. Arch. Mal. Prof. Env. 2012, 73, 743–749. [Google Scholar]
- Al-Balhan, E.; Khabbache, H.; Laaziz, A.; Watfa, A.; Mhamdi, A.; Del Puente, G.; Bragazzi, N.L. To fast or not to fast during the month of Ramadan? A comprehensive survey on religious beliefs and practices among Moroccan diabetic patients. Diabetes Metab. Syndr. Obes. 2018, 11, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Bragazzi, N.L. Ramadan fasting and chronic kidney disease: A systematic review. J. Res. Med. Sci. 2014, 19, 665–676. [Google Scholar] [PubMed]
- Bragazzi, N.L.; Briki, W.; Khabbache, H.; Rammouz, I.; Mnadla, S.; Demaj, T.; Zouhir, M. Ramadan fasting and infectious diseases: A systematic review. J. Infect. Dev. Ctries 2015, 9, 1186–1194. [Google Scholar] [CrossRef] [PubMed]
- Demirci, S.; Dogan, K.H.; Koc, S. Evaluation of forensic deaths during the month of Ramadan in Konya, Turkey, between 2000 and 2009. Am. J. Forensic Med. Pathol. 2013, 34, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Aziz, A.R.; Chia, M.Y.; Low, C.Y.; Slater, G.J.; Png, W.; Teh, K.C. Conducting an acute intense interval exercise session during the Ramadan fasting month: What is the optimal time of the day? Chronobiol. Int. 2012, 29, 1139–1150. [Google Scholar] [CrossRef] [PubMed]
- Kjellstrom, T.; Briggs, D.; Freyberg, C.; Lemke, B.; Otto, M.; Hyatt, O. Heat, Human Performance, and Occupational Health: A Key Issue for the Assessment of Global Climate Change Impacts. Annu. Rev. Public Health 2016, 37, 97–112. [Google Scholar] [CrossRef] [PubMed]
- Kjellstrom, T.; Lemke, B.; Otto, M. Climate conditions, workplace heat and occupational health in South-East Asia in the context of climate change. WHO. South East Asia J. Public Health 2017, 6, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Kjellstrom, T.; Freyberg, C.; Lemke, B.; Otto, M.; Briggs, D. Estimating population heat exposure and impacts on working people in conjunction with climate change. Int. J. Biometeorol. 2018, 62, 291–306. [Google Scholar] [CrossRef] [PubMed]
- Xiang, J.; Hansen, A.; Pisaniello, D.; Bi, P. Workers’ perceptions of climate change related extreme heat exposure in South Australia: A cross-sectional survey. BMC Public Health 2016, 16, 549. [Google Scholar] [CrossRef] [PubMed]
- Xiang, J.; Hansen, A.; Pisaniello, D.; Bi, P. Extreme heat and occupational heat illnesses in South Australia, 2001-2010. Occup. Environ. Med. 2015, 72, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Xiang, J.; Bi, P.; Pisaniello, D.; Hansen, A. The impact of heatwaves on workers' health and safety in Adelaide, South Australia. Environ. Res. 2014, 133, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Otte im Kampe, E.; Kovats, S.; Hajat, S. Impact of high ambient temperature on unintentional injuries in high-income countries: A narrative systematic literature review. BMJ. Open. 2016, 6, e010399. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M. Air temperature exposure and agricultural occupational injuries in the Autonomous Province of Trento (2000–2013, North-Eastern Italy). Int. J. Occup. Med. Environ. Health 2018, 31, 317–331. [Google Scholar] [CrossRef] [PubMed]
- Qasrawi, S.O.; Pandi-Perumal, S.R.; BaHammam, A.S. The effect of intermittent fasting during Ramadan on sleep, sleepiness, cognitive function, and circadian rhythm. Sleep Breath. 2017, 21, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Nugraha, B.; Ghashang, S.K.; Hamdan, I.; Gutenbrunner, C. Effect of Ramadan fasting on fatigue, mood, sleepiness, and health-related quality of life of healthy young men in summer time in Germany: A prospective controlled study. Appetite 2017, 111, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Ajabnoor, G.M.; Bahijri, S.; Shaik, N.A.; Borai, A.; Alamoudi, A.A.; Al-Aama, J.Y.; Chrousos, G.P. Ramadan fasting in Saudi Arabia is associated with altered expression of CLOCK, DUSP and IL-1alpha genes, as well as changes in cardiometabolic risk factors. PLoS ONE 2017, 12, e0174342. [Google Scholar] [CrossRef] [PubMed]
- Laraqui, C.H.; Tripodi, D.; Laraqui, O.; Rahhali, A.; Caubet, A.; Daoudi, F.; Mounassif, M.; Curtes, J.P.; Verger, C. The effects of fasting and of the quality of sleep on work during the month of Ramadan. Arch. Mal. Prof. Environ. 2001, 62, 115–120. [Google Scholar]
- Varghese, B.M.; Hansen, A.; Nitschke, M.; Nairn, J.; Hanson-Easey, S.; Bi, P.; Pisaniello, D. Heatwave and work-related injuries and illnesses in Adelaide, Australia: A case-crossover analysis using the Excess Heat Factor (EHF) as a universal heatwave index. Int. Arch. Occup. Environ Health. 2019, 92, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Garbarino, S.; Nobili, L.; Beelke, M.; De Carli, F.; Ferrillo, F. The contributing role of sleepiness in highway vehicle accidents. Sleep 2001, 24, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Binazzi, A.; Levi, M.; Bonafede, M.; Bugani, M.; Messeri, A.; Morabito, M.; Marinaccio, A.; Baldasseroni, A. Evaluation of the impact of heat stress on the occurrence of occupational injuries: Meta-analysis of observational studies. Am. J. Ind. Med. 2019, 62, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Vezzosi, L.; Gualerzi, G. Health and safety of pesticide applicators in a high income agricultural setting: A knowledge, attitude, practice, and toxicity study from North-Eastern Italy. J. Prev. Med. Hyg. 2018, 59, E200–E211. [Google Scholar]
- Rine, C.M. Is Social Work Prepared for Diversity in Hospice and Palliative Care? Health Soc. Work 2018, 43, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Bahammam, A.S.; Almushailhi, K.; Pandi-Perumal, S.R.; Sharif, M.M. Intermittent fasting during Ramadan: Does it affect sleep? J. Sleep Res. 2014, 23, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Msaad, S.; Kotti, N.; Abid, S.; Hajjaji, M.; Sellami, S.; Kammoun, S.; Yangui, J.; Masmoudi, A. Influence of Ramadan Observance on Sleep Pattern and Wakefulness at Work among Medical Trainer in Tunisia. J. Sleep Disord. Ther. 2016, 5, 243. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Classification | All Retrieved OIs | |
|---|---|---|
| Number | Percentage | |
| Total | 147,024 | 100.0% |
| Gender | ||
| Male | 114,470 | 77.8% |
| Female | 32,557 | 22.1% |
| WHO Region of Origin | ||
| EURO | 135,982 | 92.5% |
| EMRO | 6203 | 4.2% |
| PAHO | 2653 | 1.8% |
| SEARO | 352 | 0.2% |
| WPRO | 332 | 0.2% |
| AFRO | 1502 | 1.0% |
| Age Group | ||
| ≤24 | 26,619 | 18.1% |
| 25–34 | 36,330 | 24.7% |
| 35–44 | 40,114 | 27.3% |
| 45–54 | 30,802 | 20.9% |
| ≥55 | 13,131 | 9.0% |
| Industrial settings | ||
| Manufacturing | 27,524 | 18.7% |
| Finance, Property and Business Services | 25,576 | 17.4% |
| Wholesale and Retail Trade | 6099 | 4.1% |
| Transport. Storage and Post | 5223 | 3.6% |
| Agriculture | 6726 | 4.6% |
| Construction | 22,346 | 15.2% |
| Services, including Health Services | 5196 | 3.5% |
| Other and undetermined | 48,256 | 32.8% |
| Kind of injury | ||
| Falls to a lower level | 8543 | 5.8% |
| Fall to same level | 23,448 | 15.9% |
| Manual handling | 20,050 | 13.6% |
| Use of tools/machinery | 28,558 | 19.4% |
| Other | 66,457 | 45.2% |
| Prognosis | ||
| <40 days | 128,627 | 87.5% |
| ≥40 days | 18,299 | 12.4% |
| Death | 130 | 0.1% |
| EURO (REF) | EMRO | |||||
|---|---|---|---|---|---|---|
| TOTAL | IH Cold Season | IH Warm Season | TOTAL | IH Cold Season | IH Warm Season | |
| No. (%) | No. (%) | No. (%) | No. (%) | No. (%) | No. (%) | |
| Total | 135,982 (100.0%) | 7948 (100.0%) | 4113 (100.0%) | 6203 (100.0%) | 407 (100.0%) | 210 (100.0%) |
| Gender | ||||||
| Male | 105,218 (77.4%) | 6309 (79.4%) | 3085 (75.0%) | 5622 (90.6%) | 374 (91.9%) | 191 (91.0%) |
| Female | 30,735 (22.6%) | 1637 (20.6%) | 1028 (25.0%) | 581 (9.4%) | 33 (8.1%) | 19 (9.0%) |
| Age Group | ||||||
| ≤24 | 25,221 (18.5%) | 1616 (20.3%) | 619 (15.0%) | 768 (12.4%) | 52 (12.8%) | 24 (11.4%) |
| 25–34 | 32,676 (24.0%) | 2054 (25.8%) | 870 (21.2%) | 2128 (34.3%) | 155 (38.1%) | 61 (29.8%) |
| 35–44 | 36,170 (26.6%) | 2134 (26.8%) | 1119 (27.2%) | 2267 (36.5%) | 148 (36.0%) | 65 (31.0%) |
| 45–54 | 29,008 (21.3%) | 1468 (18.5%) | 1012 (24.6%) | 935 (15.1%) | 50 (12.3%) | 53 (25.2%) |
| ≥55 | 12,907 (9.5%) | 676 (8.5%) | 493 (12.0%) | 105 (1.7%) | 2 (0.5%) | 7 (3.3%) |
| Industrial settings | ||||||
| Manufacturing | 24317, 17.9% | 1438, 18.1% | 611, 14.9% | 1928, 31.1% | 114, 28.1% | 55, 26.2% |
| Finance, property and business services | 23,524 (17.3%) | 229 (3.2%) | 118 (2.9%) | 1038 (16.7%) | 26 (17.0%) | 44 (21.0%) |
| Wholesame and retail trade | 5746 (4.2%) | 311 (3.9%) | 171 (4.2%) | 165 (2.7%) | 18 (4.4%) | 2 (1.0%) |
| Transport, storage and post | 4743 (3.5%) | 258 (3.2%) | 118 (2.9%) | 268 (4.3%) | 13 (3.2%) | 9 (4.3%) |
| Agriculture | 6554 (4.8%) | 63 (0.8%) | 597 (14.5%) | 80 (1.3%) | 0 (-) | 6 (2.9%) |
| Construction | 20,947 (15.4%) | 1,326 (16.7%) | 628 (15.3%) | 946 (15.3%) | 72, 17.7% | 32 (15.2%) |
| Services, including health services | 4969 (3.7%) | 229 (2.9%) | 223 (5.4%) | 34 (0.5%) | 0, - | 1 (0.5%) |
| Other and undetermined | 45,075 (33.2%) | 3016 (37.9%) | 983 (23.9%) | 1742 (28.1%) | 120 (29.9%) | 61 (29.0%) |
| Kind of injury | ||||||
| Falls to a lower level | 7906 (5.8%) | 610 (7.7%) | 101 (2.5%) | 355 (5.7%) | 30 (7.7%) | 3 (1.4%) |
| Fall to same level | 21,914 (16.1%) | 1406 (17.7%) | 599 (14.6%) | 844 (13.6%) | 65 (16.0%) | 24 (11.4%) |
| Use of tools/machineries | 23,648 (19.1%) | 2063 (26.0%) | 495 (12.0%) | 1330 (21.4%) | 118 (29.0%) | 22 (10.5%) |
| Manual handling | 16,612 (13.4%) | 1055 (13.3%) | 680 (16.5%) | 961 (15.5%) | 66, 16.2% | 24 (11.4%) |
| Others | 56,557 (45.6%) | 2814 (35.4%) | 2238 (54.4%) | 2713 (43.7%) | 128 (31.4%) | 137 (65.2%) |
| Prognosis | ||||||
| <40 days | 118,723 (87.3%) | 7002 (88.1%) | 3524 (85.7%) | 5510 (88.8%) | 365 (89.7%) | 180 (85.7%) |
| ≥40 days | 17,136 (12.6%) | 936 (11.8%) | 586 (14.2%) | 690 (11.1%) | 42 (10.3%) | 30 (14.3%) |
| Deaths | 130 (0.1%) | 10 (0.1%) | 3 (0.1%) | 3 (0.0%) | 0 (-) | 0 (-) |
| EMRO | EURO (REF) | Statistical Significance (p-Value) | OR (95%CI) | adjOR (95%CI) | |
|---|---|---|---|---|---|
| IH (total) | 617, 9.9% | 12,061, 8.9% | 0.004 | 1.135 (1.042–1.236) | 1.131 (1.038–1.231) |
| IH cold season | 407, 6.6% | 7948, 5.8% | 0.015 | 1.136 (1.025–1.259) | 1.114 (1.005–1.235) |
| IH warm season | 210, 3.4% | 4113, 3.0% | 0.084 | 1.133 (0.984–1.340) | 1.182 (1.026–1.362) |
| IH SeasonNo. (%) | Rest of Calendar Year No. (%) | p-Value | adjOR | 95%CI | ||
|---|---|---|---|---|---|---|
| Industrial settings | ||||||
| Manufacturing | 169 (27.4%) | 1759 (31.5%) | 0.603 | 0.781 | 0.603 | 1.010 |
| Finance, property and business services | 113 (18.6%) | 925(16.6%) | 0.725 | 1.055 | 0.784 | 1.419 |
| Wholesale and retail trade | 20 (3.2%) | 145(2.6%) | 0.644 | 1.128 | 0.677 | 1.879 |
| Transport. storage and post | 22 (3.6%) | 246(4.4%) | 0.189 | 0.724 | 0.448 | 1.172 |
| Agriculture | 6 (1.0%) | 74(1.3%) | 0.307 | 0.638 | 0.269 | 1.510 |
| Construction | 104 (16.9%) | 842(15.1%) | 1.000 | REF | - | - |
| Services. including health services | 1 (0.2%) | 33 (0.6%) | 0.221 | 0.285 | 0.038 | 2.131 |
| Other and undetermined | 181(29.4%) | 1561 (27.9%) | 0.745 | 0.958 | 0.741 | 1.239 |
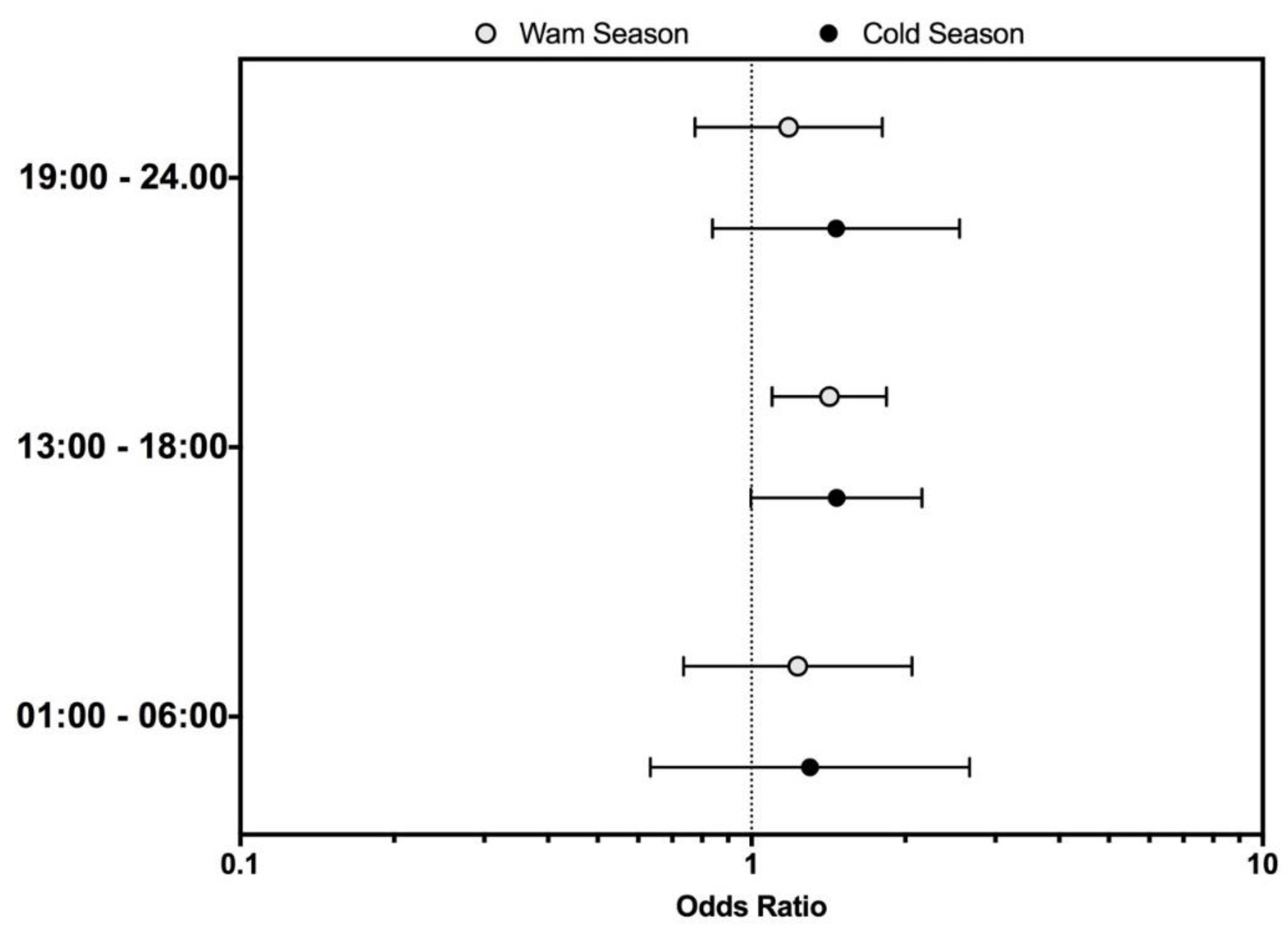
| Hour of the day | ||||||
| 7.00–12.00 | 165 (37.3%) | 1907 (45.2%) | 1.000 | REF | - | - |
| 1.00–6.00 | 27 (6.1%) | 249 (5.9%) | 0.527 | 1.154 | 0.740 | 1.799 |
| 13.00–18.00 | 204 (46.2%) | 1644 (39.0%) | 0.004 | 1.385 | 1.112 | 1.726 |
| 19.00–24.00 | 46 (10.4%) | 418 (9.9%) | 0.295 | 1.208 | 0.848 | 1.722 |
| Unknown | 203 (32.9%) | 1815 (32.5%) | - | - | - | - |
| Kind of injury | ||||||
| Falls to a lower level | 33 (5.3%) | 322 (5.8%) | 0.521 | 0.877 | 0.589 | 1.308 |
| Fall to same level | 89 (14.4%) | 755 (13.5%) | 0.935 | 1.012 | 0.763 | 1.342 |
| Manual handling | 90 (14.6%) | 871 (15.6%) | 0.377 | 0.883 | 0.667 | 1.166 |
| Use of tools/machineries | 140 (22.7%) | 1190 (21.3%) | 1.000 | REF | - | - |
| Others | 265 (42.9%) | 2448 (43.8%) | 0.468 | 0.923 | 0.743 | 1.146 |
| Prognosis | ||||||
| <40 days | 545 (88.3%) | 4965 (88.9%) | REF | 1.000 | - | - |
| ≥40 days | 72(11.7%) | 618 (11.1%) | 0.652 | 1.062 | 0.818 | 1.377 |
| Death | 0(-) | 3 (0.1%) | - | - | - | - |
| Meteorological Measure (unit) | Min. | Max. | Mean | Percentiles | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 5% | 10% | 25% | Median | 75% | 90% | 95% | ||||
| Maximum daily temperature (°C) | 0.1 | 41.2 | 20.5 | 5.7 | 7.5 | 12.1 | 21.4 | 28.6 | 32.3 | 33.9 |
| Minimum daily temperature (°C) | −10.5 | 21.0 | 6.5 | −5.6 | −3.6 | −0.4 | 6.8 | 13.1 | 16.7 | 17.9 |
| Average daily temperature (°C) | −6.2 | 29.9 | 12.7 | −0.6 | 1.2 | 4.9 | 13.1 | 20.1 | 24.0 | 25.3 |
| Relative humidity (%) | 14.8 | 100 | 65.5 | 38.4 | 44.8 | 55.1 | 64.6 | 73.3 | 83.1 | 88.4 |
| Solar radiation (kJ/m2) | 60 | 245,443 | 13,867 | 1,179 | 2,064 | 3,373 | 7,177 | 12,506 | 19,854 | 23,789 |
| Atmospheric pressure (hPa) | 911.2 | 1021.7 | 985.1 | 967.6 | 974.1 | 981.8 | 987.1 | 992.3 | 998.5 | 1002.9 |
| Wind Speed (m*s−1) | 0.1 | 7.6 | 1.5 | 0.6 | 0.7 | 0.9 | 1.4 | 1.9 | 2.3 | 2.6 |
| Exposure Percentiles | ||||||||
|---|---|---|---|---|---|---|---|---|
| <5% | 5–9% | 10–24% | 25–74% | 75–89% | 90–94% | >95% | p Value | |
| Air Humidity—No. (%) | ||||||||
| EMRO | 217 (3.5%) | 242 (3.9%) | 841 (13.6%) | 2667 (43.0%) | 1162 (18.7%) | 458 (7.4%) | 616 (9.9%) | 0.067 |
| EURO | 5711 (4.2%) | 5439 (4.0%) | 18766 (13.8%) | 58,608 (43.1%) | 25,021 (18.4%) | 9655 (7.1%) | 12,646 (9.3%) | |
| Atmospheric Pressure—No. (%) | ||||||||
| EMRO | 314 (5.1%) | 262 (4.2%) | 1115 (18.0%) | 3008 (48.5%) | 842 (13.6%) | 342 (5.5%) | 319 (5.2%) | 0.003 |
| EURO | 7751 (5.7%) | 6255 (4.6%) | 25,429 (18.7%) | 65,543 (48.2%) | 18,222 (13.4%) | 6663 (4.9%) | 5983 (4.4%) | |
| Wind Speed—No. (%) | ||||||||
| EMRO | 437 (7.0%) | 263 (4.2%) | 711 (11.5%) | 3333 (53.7%) | 866 (14.0%) | 296 (4.8%) | 297 (4.8%) | 0.047 |
| EURO | 8567 (6.3%) | 5575 (4.1%) | 15,094 (11.1%) | 72,478 (53.3%) | 20,125 (14.8%) | 6799 (5.0%) | 7207 (5.3%) | |
| Solar Radiation—No. (%) | ||||||||
| EMRO | 398 (6.4%) | 359 (5.8%) | 793 (12.8%) | 1706 (27.5%) | 1419 (22.9%) | 958 (15.4%) | 514 (8.3%) | 0.020 |
| EURO | 8567 (6.3%) | 8159 (6.0%) | 16,590 (12.2%) | 38,211 (28.1%) | 32,364 (23.8%) | 19,037 (14.0%) | 11,830 (8.7%) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riccò, M.; Garbarino, S.; Bragazzi, N.L. Migrant Workers from the Eastern-Mediterranean Region and Occupational Injuries: A Retrospective Database-Based Analysis from North-Eastern Italy. Int. J. Environ. Res. Public Health 2019, 16, 673. https://doi.org/10.3390/ijerph16040673
Riccò M, Garbarino S, Bragazzi NL. Migrant Workers from the Eastern-Mediterranean Region and Occupational Injuries: A Retrospective Database-Based Analysis from North-Eastern Italy. International Journal of Environmental Research and Public Health. 2019; 16(4):673. https://doi.org/10.3390/ijerph16040673
Chicago/Turabian StyleRiccò, Matteo, Sergio Garbarino, and Nicola Luigi Bragazzi. 2019. "Migrant Workers from the Eastern-Mediterranean Region and Occupational Injuries: A Retrospective Database-Based Analysis from North-Eastern Italy" International Journal of Environmental Research and Public Health 16, no. 4: 673. https://doi.org/10.3390/ijerph16040673
APA StyleRiccò, M., Garbarino, S., & Bragazzi, N. L. (2019). Migrant Workers from the Eastern-Mediterranean Region and Occupational Injuries: A Retrospective Database-Based Analysis from North-Eastern Italy. International Journal of Environmental Research and Public Health, 16(4), 673. https://doi.org/10.3390/ijerph16040673