Prevalence of Pressure Injuries Nationwide from 2009 to 2015: Results from the National Inpatient Sample Database in Korea



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Operational Definition of Study Population
2.3. Statistical Analysis
2.4. Ethical Statement
3. Results
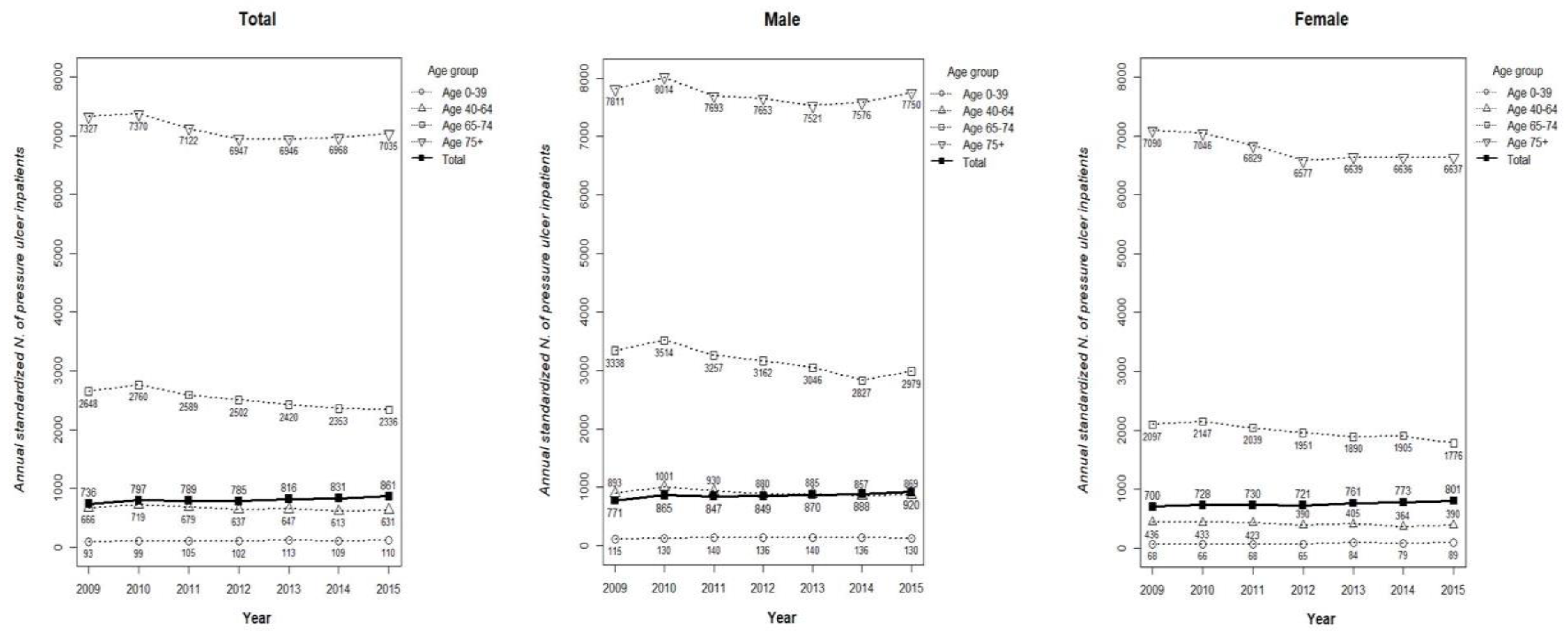
3.1. Number of Inpatients with PI and Its Standardized Prevalence from 2009 to 2015
3.2. Number of PI Inpatients by SES Including the Type of Health Insurance, Regional Location, and Level of Medical Institution
3.3. Average CCI of PI Inpatients and the Number of PI Inpatients with Special Comorbidities
3.4. Logistic Regression Analysis between PI Diagnosis and Socio-Demographic Factors among the Overall Population that Used Medical Services between 2009 and 2015 in Korea
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- National Pressure Ulcer Advisory Panel; European Pressure Ulcer Advisory Panel; Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Quick Reference Guide; Cambridge Media: Osborne Park, Western Australia, 2014; pp. 12–13. ISBN 978-0-9579343-6-8. [Google Scholar]
- Reuler, J.B.; Cooney, T.G. The pressure sore: Pathophysiology and principles of management. Ann. Intern. Med. 1981, 94, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Cushing, C.A.; Phillips, L.G. Evidence-based medicine: Pressure sores. Plast. Reconstr. Surg. 2013, 132, 1720–1732. [Google Scholar] [CrossRef] [PubMed]
- Edlich, R.F.; Winters, K.L. Pressure ulcer prevention. J. Long Term Eff. Med. Implants 2014, 14, 285–304. [Google Scholar] [CrossRef]
- Padula, W.V.; Makic, M.B. Comparative effectiveness of quality improvement interventions for pressure ulcer prevention in academic medical centers in the United States. Joint Comm. J. Qual. Patient Saf. 2015, 41, 246–256. [Google Scholar] [CrossRef]
- VanGilder, C.; Lachenbruch, C. The international pressure ulcer prevalence survey: 2006–2015: A 10-year pressure injury prevalence and demographic trend analysis by care setting. J. Wound Ostomy Cont. Nurs. 2017, 44, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Tannen, A.; Dassen, T.; Halfens, R. Differences in prevalence of pressure ulcers between the Netherlands and Germany—Associations between risk, prevention and occurrence of pressure ulcers in hospitals and nursing homes. J. Clin. Nurs. 2008, 17, 1237–1244. [Google Scholar] [CrossRef] [PubMed]
- Tannen, A.; Dietz, E.; Dassen, T.; Halfens, R. Explaining the national differences in pressure ulcer prevalence between the Netherlands and Germany—Adjusted for personal risk factors and institutional quality indicators. J. Eval. Clin. Pract. 2009, 15, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Barrois, B.; Labalette, C.; Rousseau, P.; Corbin, A.; Colin, D.; Allaert, F.; Saumet, J.L. A national prevalence study of pressure ulcers in French hospital inpatients. J. Wound Care 2008, 17, 373–376, 378–379. [Google Scholar] [CrossRef] [PubMed]
- Gunningberg, L.; Hommel, A.; Baath, C.; Idvall, E. The first national pressure ulcer prevalence survey in county council and municipality settings in Sweden. J. Eval. Clin. Pract. 2013, 19, 862–867. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.; Li, X.; Qu, X.; Liu, Y.; Zhang, L. The incidence, risk factors and characteristics of pressure ulcers in hospitalized patients in China. Int. J. Clin. Exp. Pathol. 2014, 15, 2587–2594. [Google Scholar]
- Amir, Y.; Lohrmann, C.; Halfens, R.J.; Schols, J.M. Pressure ulcers in four Indonesian hospitals: Prevalence, patient characteristics, ulcer characteristics, prevention and treatment. Int. Wound J. 2017, 14, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Jo, A.R. Prevalence, Incidence and Affecting Factors of Pressure Ulcer for Elderly Patients Admitted through Emergency Department of One Tertiary Hospital. Master’s Thesis, Seoul National University Graduate School, Seoul, Korea, 2017. [Google Scholar]
- Rawshani, A.; Svensson, A.M.; Rosengren, A.; Eliasson, B.; Gudbjörnsdottir, S. Impact of socioeconomic status on cardiovascular disease and mortality in 24,947 individuals with type 1 diabetes. Diabetes Care 2015, 38, 1518–1527. [Google Scholar] [CrossRef] [PubMed]
- Leng, B.; Jin, Y.; Li, G.; Chen, L.; Jin, N. Socioeconomic status and hypertension: A meta-analysis. J. Hypertens. 2013, 33, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Jaffiol, C.; Thomas, K.; Bean, K.; Jégo, B.; Danchin, N. Impact of socioeconomic status on diabetes and cardiovascular risk factors: Results of a large French survey. Diabetes Metab. 2013, 39, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Yin, P.; Zhang, M.; Li, Y.; Jiang, Y.; Zhao, W. Prevalence of COPD and its association with socioeconomic status in China: Findings from China Chronic Disease Risk Factor Surveillance 2007. BMC Public Health 2011, 11, 586. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.; Kim, J.A.; Kim, S. A guide for the utilization of health insurance review and assessment service national patient samples. Epidemiol. Health 2014, 36, e2014008. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Jo, M.W.; Yoo, W.S.; Kim, H.J.; Eun, S.J. Evidence of a broken healthcare delivery system in Korea: Unnecessary hospital outpatient utilization among patients with a single chronic disease without complications. J. Korean Med. Sci. 2014, 29, 1590–1596. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.H.; Kim, E.S.; Ham, O.K.; Kim, S.H.; Hwang, S.S. Factors associated with the overuse or underuse of health care services among medical aid beneficiaries in Korea. J. Community Health Nurs. 2011, 28, 190–203. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classification of prognostic comorbidity for longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Vanderwee, K.; Clark, M.; Dealey, C.; Gunningberg, L.; Defloor, T. Pressure ulcer prevalence in Europe: A pilot study. J. Eval. Clin. Pract. 2007, 13, 227–235. [Google Scholar] [CrossRef] [PubMed]
- OECD Data: Elderly Population. Available online: https://data.oecd.org/pop/elderly-population.htm (accessed on 17 February 2018).
- OECD Data: Poverty Rate. Available online: https://data.oecd.org/inequality/poverty-rate.htm (accessed on 17 February 2018).
- Vidal, J.; Sarrias, M. An analysis of the diverse factors concerned with the development of pressure sores in spinal cord injured patients. Paraplegia 1991, 29, 261–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, L.L.; Krause, J.S.; Acuna, J. Association of race, socioeconomic status, and health care access with pressure ulcers after spinal cord injury. Arch. Phys. Med. Rehabil. 2012, 93, 972–977. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y. A study on the effects of socioeconomic status on health level and medical service use. Inst. Hum. Soc. Sci. 2015, 16, 329–369. [Google Scholar]
- Kim, S.K. Socioeconomic status and chronic diseases prevalence inequalities in late life. Korean Assoc. Health Med. Sociol. 2004, 16, 155–177. [Google Scholar]
- The Joint Commission: 2018 National Patient Safety Goals. Available online: https://www.jointcommission.org/standards_information/npsgs.aspx (accessed on 17 February 2018).
- Centers for Medicaid & Medicare Services: Newsroom. Available online: http://www.cms.hhs.gov/apps/media/press/release.asp?Counter=1863 (accessed on 17 February 2018).
- American Nurses Association: Nursing Quality. Available online: http://www.nursingworld.org/ncnq (accessed on 17 February 2018).
- Jung, K.W.; Won, Y.J.; Oh, C.M.; Kong, H.J.; Lee, D.H.; Lee, K.H. Community of Population-Based Regional Cancer Registries. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2014. Cancer Res. Treat. 2017, 49, 292–305. [Google Scholar] [CrossRef] [PubMed]
- Schryvers, O.I.; Stranc, M.F.; Nance, P.W. Surgical treatment of pressure ulcers: 20-year experience. Arch. Phys. Med. Rehabil. 2000, 81, 1556–1562. [Google Scholar] [CrossRef] [PubMed]
- Atiyeh, B.S.; Hayek, S.N. Pressure sores with associated spasticity: A clinical challenge. Int. Wound J. 2005, 2, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Motheral, B.R.; Fairman, K.A. The use of claims databases for outcomes research: Rationale, challenges, and strategies. Clin. Ther. 1997, 19, 346–366. [Google Scholar] [CrossRef]


{kind=link}
| Category | Year, n (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | ||
| Study population | Total | 1,116,040 (100.0) | 1,136,688 (100.0) | 1,165,113 (100.0) | 1,169,428 (100.0) | 1,163,117 (100.0) | 1,269,210 (100.0) | 1,293,144 (100.0) |
| Male | 517,123 (46.3) | 522,237 (45.9) | 535,030 (45.9) | 535,455 (45.8) | 535,045 (46.0) | 588,179 (46.3) | 599,093 (46.3) | |
| Female | 598,917 (53.7) | 614,451 (54.1) | 630,083 (54.1) | 633,973 (54.2) | 628,072 (54.0) | 681,031 (53.7) | 694,051 (53.7) | |
| Mean age (SD) | 41.5 (22.5) | 42.8 (22.4) | 43.5 (22.3) | 44.6 (21.8) | 45.7 (21.4) | 43.9 (23.0) | 44.1 (23.2) | |
| N. of PI inpatients | Total | 12,375 (1.1) | 13,681 (1.2) | 13,892 (1.2) | 14,187 (1.2) | 14,765 (1.3) | 15,373 (1.2) | 16,202 (1.3) |
| Male | 5963 (0.5) | 6788 (0.6) | 6805 (0.6) | 6993 (0.6) | 7183 (0.6) | 7421 (0.6) | 7924 (0.6) | |
| Female | 6412 (0.6) | 6893 (0.6) | 7087 (0.6) | 7194 (0.6) | 7582 (0.7) | 7952 (0.6) | 8278 (0.6) | |
| Mean age (SD) | 71.4 (14.8) | 71.6 (16.7) | 71.9 (16.9) | 72.4 (14.6) | 72.5 (14.8) | 72.9 (15.1) | 73.1 (15.1) | |
| Standardized N. of annual PI inpatient1 | 736 | 797 | 789 | 785 | 816 | 831 | 861 | |
| N. of PI inpatients in South Korea2 | 95,192 | 105,238 | 106,861 | 109,129 | 113,576 | 118,253 | 124,629 | |
| Category | Year, n (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | ||
| N. of PI inpatients | 12,375 (100.0) | 13,681 (100.0) | 13,892 (100.0) | 14,187 (100.0 ) | 14,765 (100.0) | 15,373 (100.0) | 16,202 (100.0) | |
| Type of health insurance | NHI | 9650 (78.0) | 10,795 (78.9) | 10,966 (78.9) | 11,283 (79.5) | 11,950 (80.9) | 12,484 (81.2) | 13,285 (82.0) |
| MA | 2725 (28.2) | 2886 (26.7) | 2926 (26.7) | 2904 (25.7) | 2815 (23.6) | 2889 (23.1) | 2917 (22.0) | |
| Region of medical institution | METP | 6189 (45.2) | 6285 (45.2) | 6408 (45.2) | 6721 (45.5) | 7095 (46.2) | 7522 (46.4) | |
| Non-METP | 7492 (54.8) | 7607 (54.8) | 7779 (54.8) | 8044 (54.5) | 8278 (53.8) | 8680 (53.6) | ||
| NHI | METP | 5009 (46.4) | 5048 (46.1) | 5197 (46.1) | 5521 (46.2) | 5812 (46.6) | 6228 (46.9) | |
| Non-METP | 5786 (53.6) | 5918 (54.0) | 6086 (53.9) | 6429 (53.8) | 6672 (53.5) | 7057 (53.2) | ||
| MA | METP | 1180 (40.9) | 1237 (42.3) | 1211 (41.7) | 1200 (42.6) | 1283 (44.4) | 1294 (44.4) | |
| Non-METP | 1706 (59.1) | 1689 (57.8) | 1693 (58.3) | 1615 (57.4) | 1606 (55.6) | 1623 (55.7) | ||
| Level of medical institution | TTH | 1975 (16.0) | 2347 (17.2) | 2300 (16.6) | 1612 (11.4) | 1750 (11.9) | 2709 (17.6) | 3174 (19.6) |
| GH | 3968 (32.1) | 4523 (33.1) | 4726 (34.0) | 5510 (38.8) | 5667 (38.4) | 5005 (32.6) | 5042 (31.1) | |
| H | 5687 (46.0) | 5987 (43.8) | 5971 (43.0) | 6170 (43.5) | 6428 (43.5) | 6678 (43.5) | 7008 (43.3) | |
| C | 745 (6.0) | 820 (6.0) | 886 (6.4) | 895 (6.3) | 920 (6.2) | 976 (6.4) | 969 (6.0) | |
| NHI | TTH | 1773 (18.4) | 2104 (19.5) | 2057 (18.8) | 1450 (12.9) | 1585 (13.3) | 2441 (19.6) | 2823 (21.3) |
| GH | 3054 (31.6) | 3567 (33.1) | 3691 (33.7) | 4412 (39.1) | 4602 (38.5) | 3986 (31.9) | 4106 (30.9) | |
| H | 4227 (43.8) | 4485 (41.6) | 4518 (41.2) | 4703 (41.7) | 4983 (41.7) | 5239 (42.0) | 5549 (41.8) | |
| C | 596 (6.2) | 636 (5.9) | 694 (6.3) | 718 (6.4) | 780 (6.5) | 814 (6.5) | 799 (6.0) | |
| MA | TTH | 202 (7.4) | 243 (8.4) | 243 (8.3) | 162 (5.6) | 165 (5.9) | 268 (9.3) | 351 (12.0) |
| GH | 914 (33.5) | 956 (33.1) | 1035 (35.4) | 1098 (37.8) | 1065 (37.8) | 1019 (35.3) | 936 (32.1) | |
| H | 1460 (53.6) | 1502 (52.1) | 1453 (49.7) | 1467 (50.5) | 1445 (51.3) | 1439 (49.8) | 1459 (50.0) | |
| C | 149 (5.5) | 184 (6.4) | 192 (6.6) | 177 (6.1) | 140 (5.0) | 162 (5.6) | 170 (5.8) | |
| Variable | Year, n (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | ||
| N. of PI inpatient | 12,375 (100.0) | 13,681 (100.0) | 13,892 (100.0) | 14,187 (100.0) | 14,765 (100.0) | 15,373 (100.0) | 16,202 (100.0) | |
| Average CCI [STD] | 2.3 [2.1] | 2.2 [2.0] | 2.0 [1.9] | 2.2 [2.0] | 2.1 [1.9] | 2.2 [2.0] | 2.1 [1.9] | |
| N. of PI inpatient with special comorbidities | ||||||||
| Plegia | 2141 (17.3) | 2313 (16.9) | 2137 (15.4) | 2037 (14.4) | 2069 (14.0) | 2169 (14.1) | 2203 (13.6) | |
| Quadriplegia | 508 (4.1) | 554 (4.0) | 542 (3.9) | 543 (3.8) | 581 (3.9) | 657 (4.3) | 634 (3.9) | |
| Hemiplegia | 1136 (9.2) | 1282 (9.4) | 1013 (7.3) | 932 (6.6) | 909 (6.2) | 937 (6.1) | 934 (5.8) | |
| Monoplegia | 61 (0.5) | 59 (0.4) | 77 (0.6) | 46 (0.3) | 52 (0.4) | 44 (0.3) | 58 (0.4) | |
| Paraplegia | 169 (1.4) | 218 (1.6) | 227 (1.6) | 226 (1.6) | 214 (1.4) | 257 (1.7) | 246 (1.5) | |
| Flaccid paralysis | 187 (1.5) | 181 (1.3) | 211 (1.5) | 195 (1.4) | 218 (1.5) | 214 (1.4) | 240 (1.5) | |
| Spastic paralysis | 580 (4.7) | 643 (4.7) | 563 (4.1) | 543 (3.8) | 510 (3.5) | 522 (3.4) | 489 (3.0) | |
| Diabetes | 1275 (10.3) | 1432 (10.5) | 1586 (11.4) | 1697 (12.0) | 1706 (11.6) | 1917 (12.5) | 2055 (12.7) | |
| Sepsis | 1467 (11.9) | 1596 (11.7) | 1531 (11.0) | 1637 (11.5) | 1787 (12.1) | 1892 (12.3) | 1960 (12.1) | |
| Variable | Category | Year, Odds Ratio (95% Confidence Interval) | |||
|---|---|---|---|---|---|
| 2009 | 2011 | 2013 | 2015 | ||
| Total study population | 1,116,040 | 1,165,113 | 1,163,117 | 1,293,144 | |
| N. of PI inpatients | 12,375 | 13,892 | 14,765 | 16,202 | |
| Sex | Male | 1.00 | 1.00 | 1.00 | 1.00 |
| Female | 0.84 (0.82–0.85) | 0.84 (0.83–0.86) | 0.85 (0.83–0.86) | 0.85 (0.83–0.86) | |
| Age | 0–39 | 1.00 | 1.00 | 1.00 | 1.00 |
| 40–64 | 0.66 (0.64–0.69) | 0.66 (0.64–0.69) | 0.65 (0.62–0.67) | 0.65 (0.63–0.67) | |
| 65–74 | 1.98 (1.91–2.06) | 1.90 (1.83–1.97) | 1.79 (1.72–1.86) | 1.78 (1.72–1.84) | |
| 75+ | 5.58 (5.39–5.77) | 5.29 (5.12–5.47) | 5.15 (4.98–5.32) | 5.29 (5.13–5.46) | |
| Type of health insurance | NHI | 1.00 | 1.00 | 1.00 | 1.00 |
| MA | 1.45 (1.41–1.48) | 1.49 (1.46–1.52) | 1.45 (1.42–1.49) | 1.46 (1.43–1.49) | |
| CCI | 0 | 1.00 | 1.00 | 1.00 | 1.00 |
| 1-2 | 1.11 (1.08–1.14) | 1.05 (1.03–1.08) | 1.13 (1.10–1.15) | 1.10 (1.07–1.12) | |
| 3+ | 1.96 (1.91–2.02) | 2.07 (2.02–2.13) | 1.99 (1.94–2.05) | 1.99 (1.94–2.04) | |
| Plegia comorbidity | NO | 1.00 | 1.00 | 1.00 | 1.00 |
| YES | 2.48 (2.39–2.58) | 2.17 (2.09–2.26) | 2.05 (1.98–2.13) | 1.88 (1.81–1.95) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, G.H.; Lee, J.Y.; Kim, J.; Kim, H.J.; Park, J.-U. Prevalence of Pressure Injuries Nationwide from 2009 to 2015: Results from the National Inpatient Sample Database in Korea. Int. J. Environ. Res. Public Health 2019, 16, 704. https://doi.org/10.3390/ijerph16050704
Kim GH, Lee JY, Kim J, Kim HJ, Park J-U. Prevalence of Pressure Injuries Nationwide from 2009 to 2015: Results from the National Inpatient Sample Database in Korea. International Journal of Environmental Research and Public Health. 2019; 16(5):704. https://doi.org/10.3390/ijerph16050704
Chicago/Turabian StyleKim, Gyeong Hoe, Jin Yong Lee, Jayeun Kim, Hyun Joo Kim, and Ji-Ung Park. 2019. "Prevalence of Pressure Injuries Nationwide from 2009 to 2015: Results from the National Inpatient Sample Database in Korea" International Journal of Environmental Research and Public Health 16, no. 5: 704. https://doi.org/10.3390/ijerph16050704
APA StyleKim, G. H., Lee, J. Y., Kim, J., Kim, H. J., & Park, J. -U. (2019). Prevalence of Pressure Injuries Nationwide from 2009 to 2015: Results from the National Inpatient Sample Database in Korea. International Journal of Environmental Research and Public Health, 16(5), 704. https://doi.org/10.3390/ijerph16050704