The Association between Osteoporosis and Grip Strength and Skeletal Muscle Mass in Community-Dwelling Older Women


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
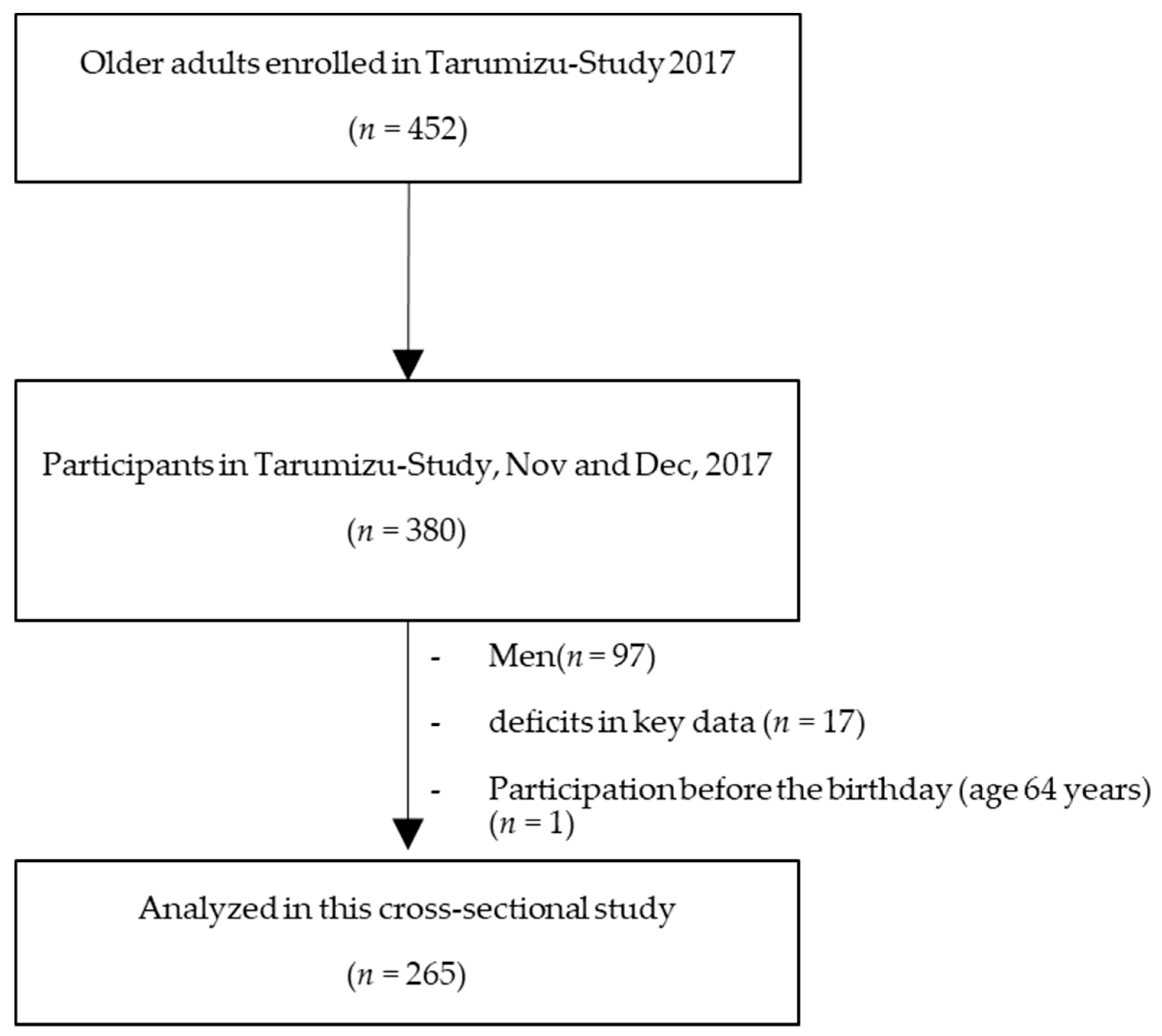
2.1. Participants
2.2. Loss of Skeletal Muscle Mass and Muscle Weakness
2.3. Interviewer-Administered Questionnaire
2.4. Walking Speed
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Participants
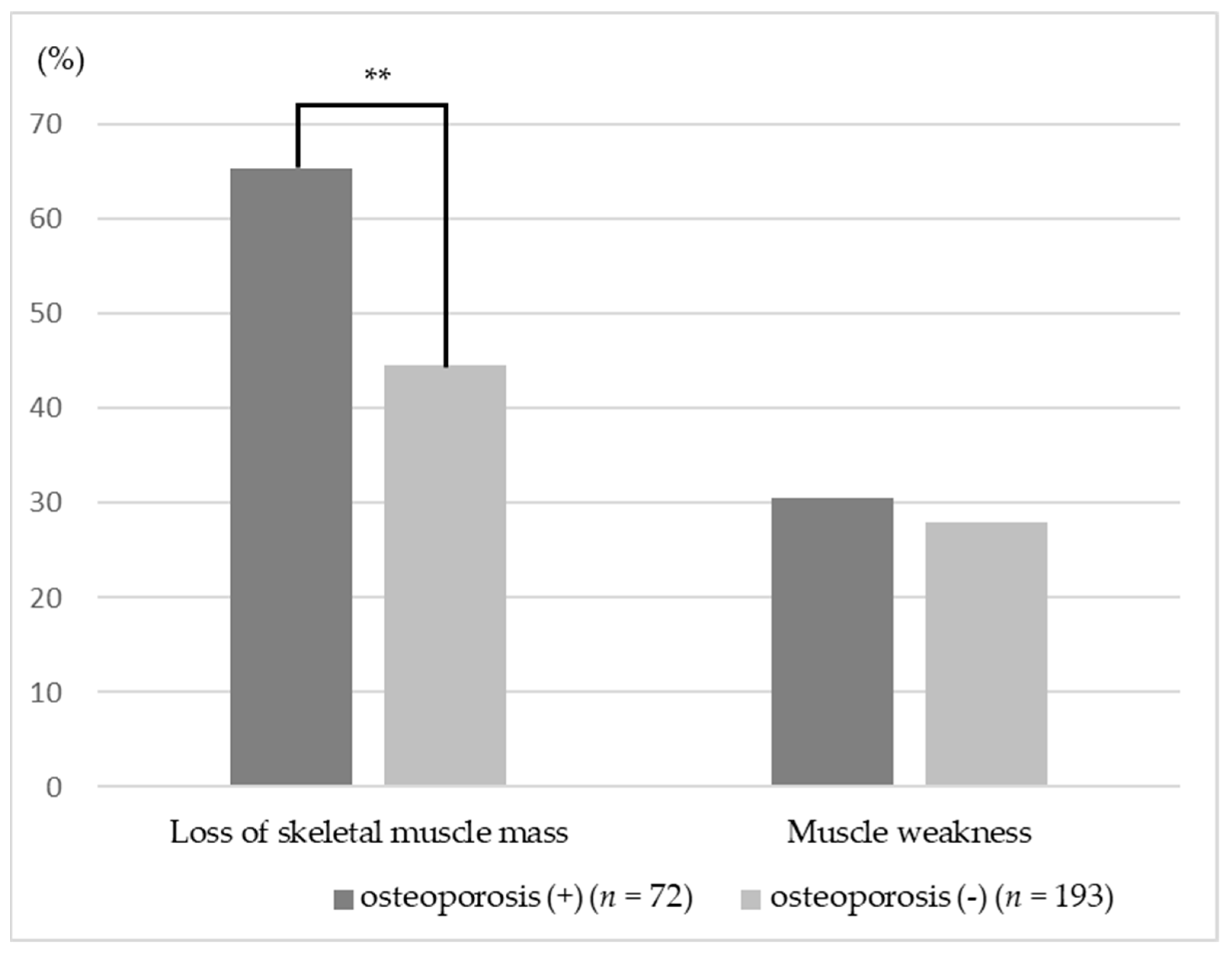
3.2. Association between Osteoporosis and Muscle Mass and Muscle Strength
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO Scientific Group. Prevention and management of osteoporosis. World Health Organ. Tech. Rep. Ser. 2003, 921, 1–164. [Google Scholar]
- Ministry of Health, Labour and Welfare. The Outline of the Results of the National Livelihood Survey. Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2018/html/zenbun/s1_2_2.html (accessed on 4 April 2019).
- Orimo, H.; Nakamura, T.; Iki, M.; Uenishi, K.; Endo, N.; Ohta, H.; Ogawa, S.; Shiraki, M.; Sugimoto, T.; Suzuki, T.; et al. Prevention and treatment guidelines for Osteoporosis 2015; Life Science Publishing Co., Ltd.: Tokyo, Japan, 2015; p. 4. [Google Scholar]
- Yoshida, D.; Suzuki, T.; Shimada, H.; Park, H.; Makizako, H.; Doi, T.; Anan, Y.; Tsutsumimoto, K.; Uemura, K.; Ito, T.; et al. Using two different algorithms to determine the prevalence of sarcopenia. Geriatr. Gerontol. Int. 2014, 14, 46–51. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, N.; Muraki, S.; Oka, H.; Iidaka, T.; Kodama, R.; Kawaguchi, H.; Nakamura, K.; Tanaka, S.; Akune, T. Is osteoporosis a predictor for future sarcopenia or vice versa? Four-year observations between the second and third ROAD study surveys. Osteoporos. Int. 2017, 28, 189–199. [Google Scholar]
- Di Monaco, M.; Vallero, F.; Di Monaco, R.; Tappero, R. Prevalence of sarcopenia and its association with osteoporosis in 313 older women following a hip fracture. Arch. Gerontol. Geriatr. 2011, 52, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Sirola, J.; Kröger, H. Similarities in Acquired Factors Related to Postmenopausal Osteoporosis and Sarcopenia. J. Osteoporos. 2011, 2011, 1–14. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tagliaferri, C.; Wittrant, Y.; Davicco, M.J.; Walrand, S.; Coxam, V. Muscle and bone, two interconnected tissues. Ageing Res. Rev. 2015, 21, 55–70. [Google Scholar] [PubMed]
- Schoenau, E.; Fricke, O. Mechanical influences on bone development in children. Eur. J. Endocrinol. 2008, 159, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Bijlsma, A.Y.; Meskers, M.C.G.; Molendijk, M.; Westendorp, R.G.J.; Sipilä, S.; Stenroth, L.; Sillanpää, E.; McPhee, J.S.; Jones, D.A.; Narici, M.; et al. Diagnostic measures for sarcopenia and bone mineral density. Osteoporos. Int. 2013, 24, 2681–2691. [Google Scholar] [CrossRef] [PubMed]
- Genaro, P.S.; Pereira, G.A.P.; Pinheiro, M.M.; Szejnfeld, V.L.; Martini, L.A. Influence of body composition on bone mass in postmenopausal osteoporotic women. Arch. Gerontol. Geriatr. 2010, 51, 295–298. [Google Scholar] [CrossRef]
- Pluijm, S.M.; Visser, M.; Smit, J.H.; Popp-Snifders, C.; Roos, J.C.; Lips, P. Determinants of bone mineral density in older men and women: Body composition as mediator. J. Bone Miner. Res. 2001, 16, 2142–2151. [Google Scholar] [CrossRef]
- Tachiki, T.; Kouda, K.; Dongmei, N.; Tamaki, J.; Iki, M.; Kitagawa, J.; Takahira, N.; Sato, Y.; Kajita, E.; Fujita, Y.; et al. Muscle strength is associated with bone health independently of muscle mass in postmenopausal women: The Japanese population-based osteoporosis study. J. Bone Miner. Metab. 2019, 37, 53–59. [Google Scholar] [CrossRef]
- Makizako, H.; Kubozono, T.; Kiyama, R.; Takenaka, T.; Kuwahata, S.; Tabira, T.; Kanoya, T.; Horinouchi, K.; Shimada, H.; Ohishi, M. Associations of social frailty with loss of muscle mass and muscle weakness among community-dwelling older adults. Geriatr. Gerontol. Int. 2019, 19, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian working group for sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Miyakoshi, N.; Hongo, M.; Mizutani, Y.; Shimada, Y. Prevalence of sarcopenia in Japanese women with osteopenia and osteoporosis. J. Bone Miner. Metab. 2013, 31, 556–561. [Google Scholar] [CrossRef]
- Schoenau, E.; Fricke, O. Interaction between muscle and bone. Horm. Res. 2007, 66, 73–78. [Google Scholar] [CrossRef]
- Kim, S.; Won, C.W.; Kim, B.S.; Choi, H.R. The association between the low muscle mass and osteoporosis in elderly Korean people. J. Korean Med. Sci. 2014, 29, 995–1000. [Google Scholar] [CrossRef]
- He, H.; Liu, Y.; Tian, Q.; Papasian, C.J.; Hu, T.; Deng, H.W. Relationship of sarcopenia and body composition with osteoporosis. Osteoporos. Int. 2016, 27, 473–482. [Google Scholar] [CrossRef]
- Kawao, N.; Kaji, H. Interactions between muscle tissues and bone metabolism. J. Cell. Biochem. 2015, 116, 687–695. [Google Scholar] [CrossRef] [PubMed]
- De Laet, C.; Kanis, J.A.; Odén, A.; Johanson, H.; Johnell, O.; Delmas, P.; Eisman, J.A.; Kroger, H.; Fujiwara, S.; Garnero, P.; et al. Body mass index as a predictor of fracture risk: A meta-analysis. Osteoporos. Int. 2005, 16, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Joakimsen, R.M.; Fønnebø, V.; Magnus, J.H.; Tollan, A.; Søgaard, A.J. The Tromsø Study: Body Height, Body Mass Index and Fractures. Osteoporos. Int. 1998, 8, 436–442. [Google Scholar] [CrossRef]
- An, J.H.; Yang, J.Y.; Ahn, B.Y.; Cho, S.W.; Jung, J.Y.; Cho, H.Y.; Cho, Y.M.; Kim, S.W.; Park, K.S.; Kim, S.Y.; et al. Enhanced mitochondrial biogenesis contributes to Wnt induced osteoblastic differentiation of C3H10T1/2 cells. Bone 2010, 47, 140–150. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Over All (N = 265) | Participants with Osteoporosis (N = 72, 27.2%) | Participants without Osteoporosis (N = 193, 72.8%) | pa |
|---|---|---|---|---|
| Age, years | 75.5 ± 6.5 | 76.2 ± 6.4 | 75.3 ± 6.5 | 0.297 |
| Height, cm | 149.4 ± 5.5 | 149.1 ± 5.8 | 149.5 ± 5.4 | 0.593 |
| Weight, kg | 52.4 ± 8.8 | 50.3 ± 8.9 | 53.2 ± 8.6 | 0.015 |
| Body mass index, kg/m2 | 23.5 ± 3.9 | 22.6 ± 3.6 | 23.8 ± 3.5 | 0.016 |
| Medications, number/day | 3.7 ± 3.9 | 5.6 ± 4.9 | 3.0 ± 3.2 | <0.001 |
| Grip strength, kg | 20.4 ± 4.2 | 19.8 ± 4.1 | 20.6 ± 4.2 | 0.154 |
| Usual walking speed, m/s | 1.4 ± 0.2 | 1.4 ± 0.2 | 1.4 ± 0.4 | 0.285 |
| ASMI, kg/m2 | 5.7 ± 0.7 | 5.5 ± 0.6 | 5.8 ± 0.7 | 0.004 |
| No exercise habits, n (%) | 42 (15.8%) | 10 (13.9%) | 32 (16.6%) | 0.594 |
| Fall history, n (%) | 43 (16.2%) | 9 (12.5%) | 34 (17.6%) | 0.315 |
| Variable | Dependent Value: Loss of Skeletal Muscle Mass | |
|---|---|---|
| Odds Ratio (95% CI) | p | |
| Osteoporosis | 2.56 (1.33–4.91) | 0.005 |
| Age | 1.03 (0.98–1.09) | 0.257 |
| Grip strength | 0.79 (0.73–0.86) | <0.001 |
| Usual walking speed | 0.60 (0.14–2.57) | 0.494 |
| Medications | 0.94 (0.86–1.03) | 0.172 |
| No exercise habits | 1.46 (0.69–3.10) | 0.327 |
| Fall history | 1.54 (0.72–3.32) | 0.266 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taniguchi, Y.; Makizako, H.; Kiyama, R.; Tomioka, K.; Nakai, Y.; Kubozono, T.; Takenaka, T.; Ohishi, M. The Association between Osteoporosis and Grip Strength and Skeletal Muscle Mass in Community-Dwelling Older Women. Int. J. Environ. Res. Public Health 2019, 16, 1228. https://doi.org/10.3390/ijerph16071228
Taniguchi Y, Makizako H, Kiyama R, Tomioka K, Nakai Y, Kubozono T, Takenaka T, Ohishi M. The Association between Osteoporosis and Grip Strength and Skeletal Muscle Mass in Community-Dwelling Older Women. International Journal of Environmental Research and Public Health. 2019; 16(7):1228. https://doi.org/10.3390/ijerph16071228
Chicago/Turabian StyleTaniguchi, Yoshiaki, Hyuma Makizako, Ryoji Kiyama, Kazutoshi Tomioka, Yuki Nakai, Takuro Kubozono, Toshihiro Takenaka, and Mitsuru Ohishi. 2019. "The Association between Osteoporosis and Grip Strength and Skeletal Muscle Mass in Community-Dwelling Older Women" International Journal of Environmental Research and Public Health 16, no. 7: 1228. https://doi.org/10.3390/ijerph16071228
APA StyleTaniguchi, Y., Makizako, H., Kiyama, R., Tomioka, K., Nakai, Y., Kubozono, T., Takenaka, T., & Ohishi, M. (2019). The Association between Osteoporosis and Grip Strength and Skeletal Muscle Mass in Community-Dwelling Older Women. International Journal of Environmental Research and Public Health, 16(7), 1228. https://doi.org/10.3390/ijerph16071228